1. Introduction
For many individuals, driving is an integral activity of day-to-day life. Conversely, for individuals who undergo a stroke and transition into driving retirement, such a change in mobility is associated with poorer health outcomes, higher rates of depression, and lower rates of community integration [
1,
2,
3]. Driving is a skill that requires the coordination of high-level cognitive and motor function to perform safely. When a patient has a stroke, it remains a challenge for the clinician to determine whether it is safe for the patient to return to driving [
4,
5,
6,
7]. There is a myriad of methodologies used to assess the safety of returning to driving after stroke. These include, but are not limited to, road tests and psychometric assessments [
8,
9].
The performance-based road test is often considered a reliable test to assess driving ability after stroke, and it is considered a standard criterion to which other tests with the same goal are often compared [
10,
11]. However, the road test can be costly, and patients’ access to these tests can be limited. Therefore, it has been a topic of interest to develop low-cost, easily accessible models predictive of success on a road test after stroke, which by extension aims to predict a safe return to driving [
8]. Using a battery of clinical assessments and psychometric tests predictive of road test performance is one such approach, and our group has previously published a fitness-to-drive (FTD) calculator to predict the probability of road test failure using two brief psychometric screens that tap into processing speed, visuospatial skill, planning, and foresight [
5].
High-end, research-based driving simulators have emerged as a viable supplement to assessing the safety of returning to driving after stroke [
12]. These traditional research simulators are highly customizable platforms that can assess driving performance in a variety of contexts simulating real-life driving scenarios. While driving simulation is obviously different from real-life driving, evidence supports the use of research-based driving simulators to predict real-life driving performance, and they may be useful prospective predictors of driving performance in neurologically impaired adults [
13,
14,
15,
16,
17,
18]. Research-based driving simulators typically involve a life-size vehicle cab as well as a multiple monitor setup to simulate the wide field of view required in real life driving.
However, there are drawbacks to research simulators that may limit their accessibility. Research simulator units are costly, and higher-fidelity models often require budgets normally only available at the research institution level [
19,
20,
21]. Driving rehabilitation in general, of which use of a research simulator may be included, requires multiple visits with health care professionals and is not typically reimbursed through usual insurance mechanisms.
Whereas research simulators aim to recreate the experience of community-based road driving, consumer-grade racing simulators emphasize fidelity to the experience of a motorsport driver on a competitive racing track [
22,
23]. Such racing simulators, which are targeted to automotive racing professionals and enthusiasts alike, offer enhanced physics models, immersive graphics rendering, and feature-rich telemetry all at very low cost. However, while both road driving and racing share several obvious skills, the two activities have some fundamental differences. Compared to road driving, automotive racing is conducted on wider tracks, with turns designed to physically challenge the driver in both solitary practice and in competitive scenarios where as many as 20 drivers may be competing simultaneously [
24]. Race cars are also configured to perform at velocities and levels of acceleration/deceleration much greater than those seen in road cars [
25]. Differences in cortical activation and eye movements in racers vs. non-racers have also been described, suggesting physiologically different adaptations to the two disciplines [
26,
27]. As such, it should be stressed that racing simulation is not meant to mimic road driving, but to offer a more strenuous driving experience. As a result, most racing simulators are limited in their ability to simulate street traffic and measure driver behavior in real world-based scenarios.
In spite of these differences, low-cost racing simulators possess another compelling feature: they provide feedback on driver performance using the same telemetric data and analysis techniques employed by real-world racing professionals [
22]. Such feedback on performance from these low-cost simulators may have utility for future outpatient or home-based rehabilitation opportunities. For instance, the Assetto Corsa racing simulator can make use of a telemetry plug-in, the Assetto Corsa Telemetry Interface (ACTI), to harness a comprehensive array of sensors in gathering driver performance data [
28]. The collected data may then be analyzed using statistical techniques commonly used in research, similar to the data extraction and reduction methods used for research simulators. Data can also be captured remotely over the internet.
One of the key advantages of the racing simulator is its low cost and flexibility for use at the individual consumer level. Racing simulators can run on desktops configured for computer gaming, on one or more monitors, and accept a number of consumer-grade force feedback steering wheels. Thus, a complete simulator system with only a few portable components can be assembled for under
$1000 USD. A summary comparing custom-built research simulators and low-cost racing simulators is outlined in
Table 1. The feasibility of using low-cost racing simulation has been explored in other clinical contexts, such as attention-deficit hyperactivity disorder [
29]. Given these features, we aim to explore the feasibility of using a low-cost racing simulator as a tool in driving assessment after strokes [
30].
Our aims for this observational-analytic pilot study were threefold. We first sought to determine the feasibility and tolerability (i.e., successfully completing simulator participation with minimal adverse events) of a low-cost racing simulator in a stroke patient cohort. We then sought to determine if parameters of research simulation and racing simulation correlated with clinical and psychometric characteristics in our cohort and, moreover, if parameters of the two simulators correlated between themselves. Finally, using our probability of road test failure calculator, we sought to determine if driving and racing simulator outcomes can each help reliably predict the risk of failure of on-road testing. We hypothesized that impaired driving simulator performance would be associated with performance on psychometric tests of processing speed, executive function, and visuospatial skills in our stroke sample.
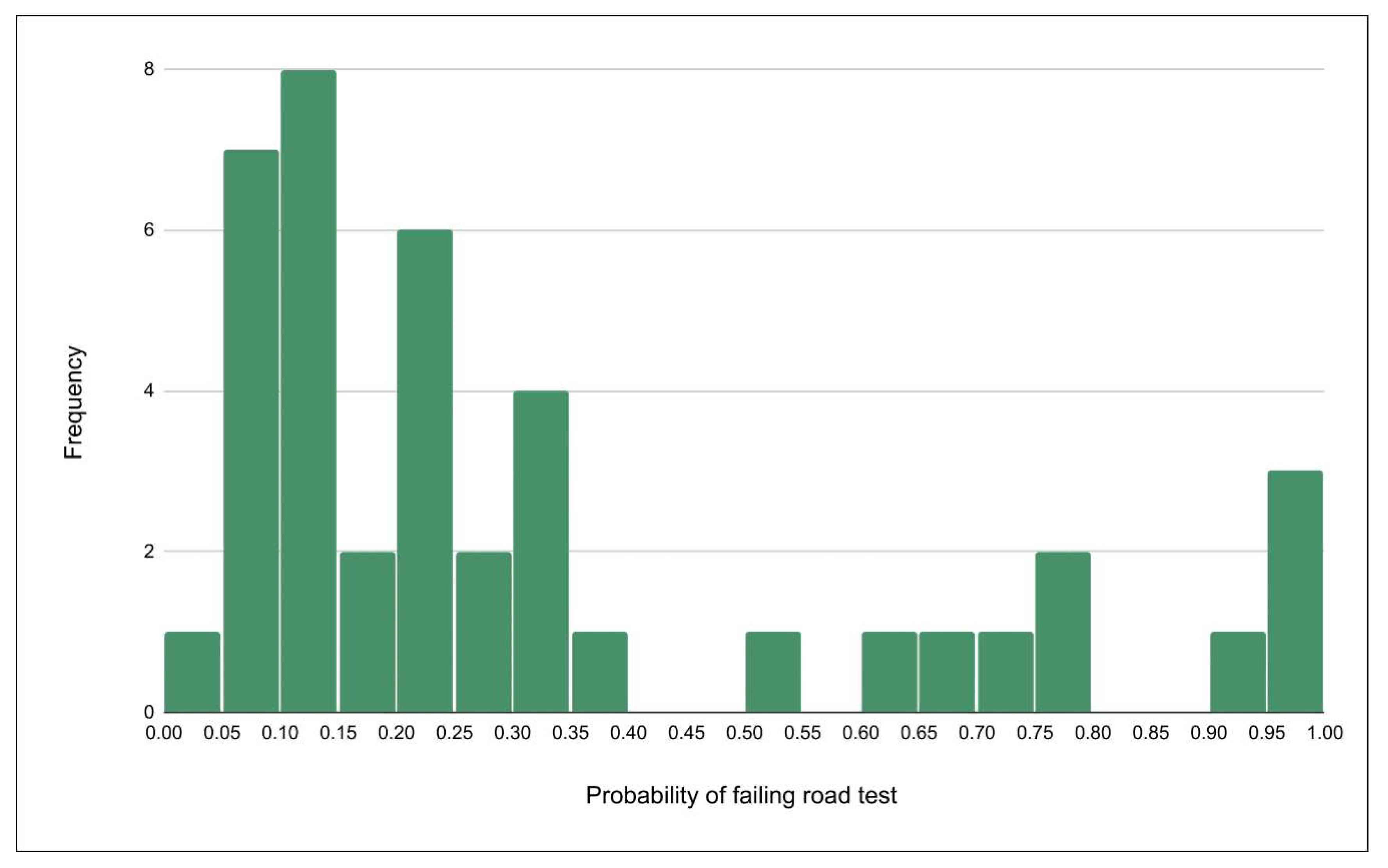
The results of our study demonstrate that the use of consumer-grade racing simulators after minor stroke is well tolerated. Correlates between psychometric and physical (Snellgrove Maze Task [SMT], Trail Making Test Part A [TMT-A]) and Motricity Index [MI] of the right side) clinical assessments and several research and racing simulator outcomes are identified. We also present two models using parameters from either the research or racing simulator to predict a low- (≤25%) or high-risk (≥70%) probability of road test failure.
4. Discussion
Traditional research-based driving simulators aim to mimic realistic and immersive driving environments (e.g., driving cab with bucket seats, multiple screens with wide viewing angles, and real-world traffic scenarios), but their size and cost can be prohibitive in a clinical setting. Racing simulators, on the other hand, are available at the consumer level and are thus cheaper and more accessible. However, little empirical evidence is available to discern the validity, adaptability, and tolerability of these racing simulators to assess or rehabilitate medical driving impairments, including stroke. In this exploratory study, we assessed how well adults with minor stroke tolerated racing simulation, and we also compared driving performance outcomes on the two types of driving simulators. We also determined that simulator performance outcomes could accurately group participants into low or high risk of failing an on-road skills test, as determined by our previously published fitness-to-drive calculator.
The research and racing simulator were both well tolerated overall, with few symptoms of SAS syndrome in this sample (only 1 of 41 patients experienced SAS symptoms). During our investigation, participants were noted to provide spontaneous feedback on the racing simulator. This feedback was not collected in a systematized manner, although it was passively observed that participants found the controls realistic, the graphics attractive and convincing, and vehicle sounds and physical responses reminiscent of real driving. A few participants disagreed with steering feel (e.g., “unrealistic,” “challenging,” and “felt heavy”). This complaint about heavy steering feel may be due to the fact that the participants were unfamiliar with the steering feel of high-performance race cars, which the racing simulator seeks to accurately recreate. Future work can attempt to collect feedback in a systematized way to better understand a participant’s experiences with the racing simulator, which might also serve to refine future racing simulator assessment protocols. Furthermore, our racing simulator did not have a driving cab—such a feature may enhance simulation immersion but is not typically available to the average consumer. While literature on construct validity of research simulators is already established, additional studies will be needed to establish the construct validity of low-cost racing simulators [
43,
54,
55].
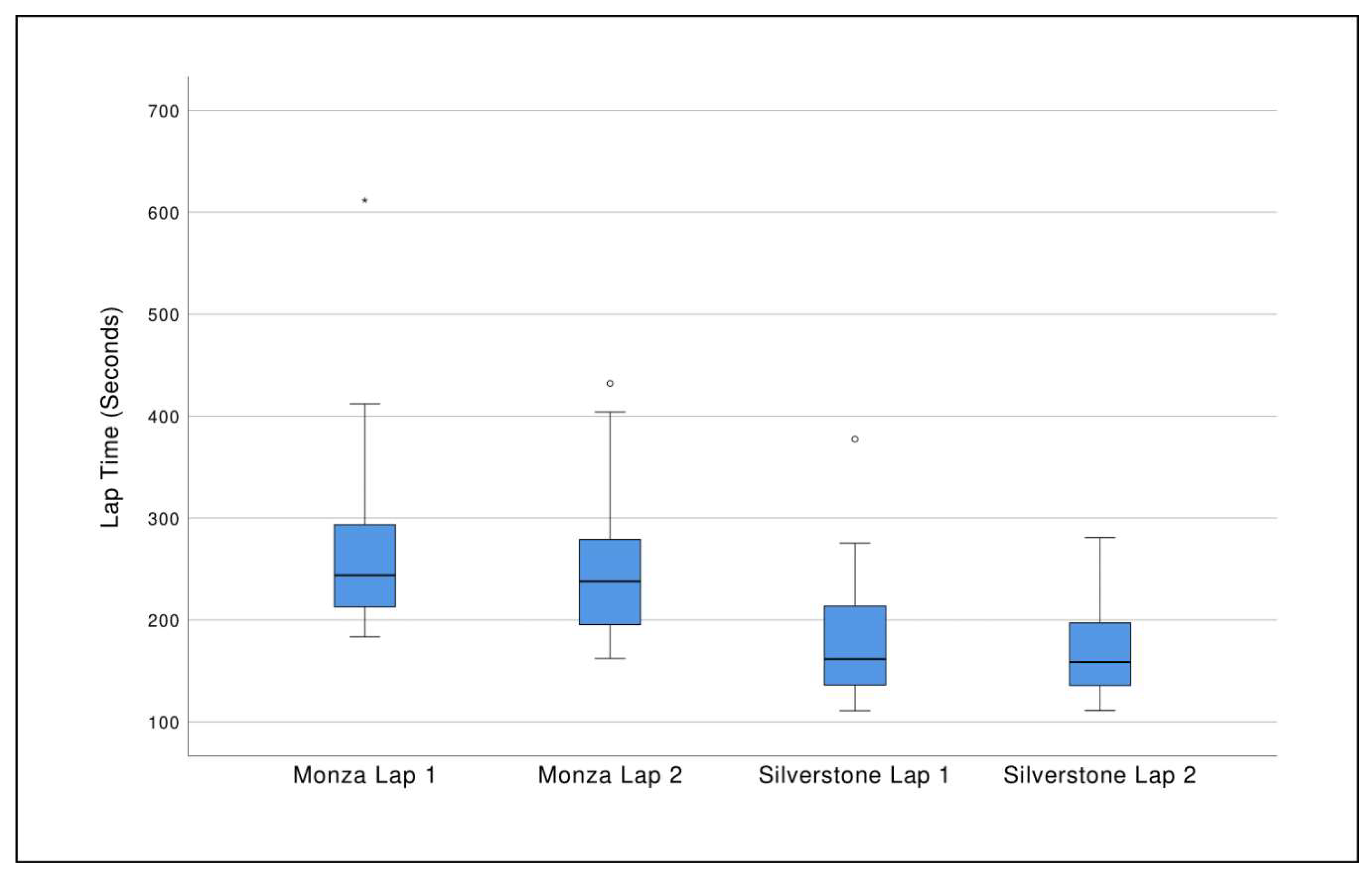
Importantly, performance measures from the racing simulator were significantly related to clinical tests of physical and cognitive function, emphasizing the potential ability of consumer-grade racing simulators to flag stroke patients for driving impairment. In our sample, Trail Making Test A (TMT-A) correlated with lap 2 times on both the Monza and Silverstone racing simulator courses. As a primary component of the fitness-to-drive calculator [
5], which calculates the probability of failing a road-based performance test, TMT-A is one of the best clinical predictors of driving [
56]. This link to an established clinical correlate of driving performance suggests that lap times—which are essentially measures of general racing performance—may have some significance when using the racing simulator as a driving assessment tool. Physical measurements such as limb and grip strength also correlated with racing performance in terms of vehicular control, although not consistently between courses. Larger samples are needed to see if these relationships hold, as well as other racing performance outcomes associated with fitness to drive.
Interestingly, maximum speed in scenario 2 of the research simulator correlated with fast lap times in the racing simulator, as well as measures of vehicular control (max # of tires off track) in both tracks of the racing simulator. It is important to highlight that while maximizing speed is important in the racing simulator, speed limits and safe adherence to traffic regulations were emphasized in the research simulator. With that said, few participants exceeded the speed limit in research simulator scenario 2. It makes sense that being able to navigate the racing simulator courses at high speed with a minimum of technical errors correlates with safe and effective driving on the complex research simulator scenarios. Of note, other than in the drag race scenario in the racing simulator, we did not collect data on use of left or right foot for each pedal in the racing simulator. It is generally noted that most race drivers—even at amateur levels—use “left-foot braking” [
22]. It would be valuable to characterize this behavior during racing in a stroke population as it pertains to lesion side and presence of any hemiparesis.
We were able to create two models—using either the research simulator or the racing simulator alone—for predicting patients at low- and high-risk of road-test failure as determined by our fitness-to-drive calculator. Both of our simulator models reached statistical significance, but individual components of each model did not. Compared to our research simulator model, our racing simulator model was less strongly predictive of road test failure; nonetheless, the racing model was able to detect 3/5 high risk drivers. The strength of both of our models may be an artifact of our small sample size. It may be an area of interest for future larger studies to compare performance on different racetracks and conducting sessions with an increased number of laps.
The findings of our small pilot study bring initial support for the idea that racing simulation may have the potential for clinical use in assessing driving fitness after minor stroke, but more data is needed before this practice can be confidently adopted into the clinical setting. On a practical level, for the patient with minor stroke who does not have ready access to driving simulation or driving rehabilitation resources, clinicians might be able to suggest the installation of a low-cost racing simulator at the patient’s home as a tool for assessing the safety of returning to driving after stroke. However, it ought to be stressed once again that racing is not meant to be a 1:1 analogue to road driving, but rather a modality aimed at providing a strenuous driving environment for which skills may correlate with road driving. Larger future studies are necessary to validate our results, to explore the transfer of skills between racing and research simulation, and most importantly, to determine direct correlations of racing simulation to the actual road. One of the strengths of our study was collecting simulator data previously shown to have significance. There are numerous simulated driving behaviors that are correlated with real-world driving performance such as motor vehicle crashes or performance-based road tests and which have been the subject of previous reviews. Vehicle speed, speed variability (standard deviation of speed), SDLP, brake reaction time, and TTC are frequent outcomes measured in driving simulation [
43,
44,
45,
46,
47,
48]. In our study, we were able to obtain the majority of these measures, or close proxies, during racing simulation.
Another of the strengths of our study was the relative simplicity of our protocol using widely available psychometric and motor tests as well as a popular racing simulator. This helps the reproducibility of our methods for future, related projects. Of note, another advantage of a racing simulation using popular simulator software is the opportunity for user-made modification, which are often freely available for download on enthusiast community websites. Following the completion of this study, there has been development of modifications for Assetto Corsa which add the feature of two-way highway traffic; such modifications may increase the relevance of these racing simulators to driving assessment and rehabilitation [
31].
Our pilot study had a number of limitations. Firstly, we had a mixed sample of drivers and non-drivers. Recent driving experience may influence simulation performance and larger studies may be able to assess subgroup analyses based on whether participants are actively driving. In a related way, while it was not wholly surprising that none of our subjects had racing experience, future work ought to screen for this point. Secondly, our model utilized a fitness-to-drive calculator to indirectly predict road test performance. Future work that directly compares simulator outcomes to road test performance and/or prospective crash data will enhance validity measures. Additionally, we did not control for prior gaming experience. The majority of our sample had never played video games, while 5 (12%) of our subjects played daily. Prior gaming experience and transfer across racing simulators may influence simulator performance, with unclear transfer to real-world driving performance [
57]. Furthermore, our pilot study featured a small sample size. Recruiting a larger sample would improve the accuracy of the predictions and also reduce Type II error.
Finally, we did not emphasize capture of stroke location; however, we were able to use chronic NIHSS as an indirect measure to approximate stroke lesion side. Obviously, stroke locations and sizes are heterogeneous and would impact performance on simulator testing. However, in our study most of our participants had very low NIHSS scores, and were either driving or had an interest in returning to driving. We additionally found a low occurrence of neglect in our sample based on NIHSS, although the sensitivity of the NIHSS for capturing this may not be great [
58]. Future work could explore the impact of racing simulator use in more severe strokes.
In addition, we found nearly no performance difference between those driving with the affected foot compared to those driving with the unaffected foot. The sample’s low NIHSS score average may suggest that stroke severity was unlikely to be a major factor in this sample, thereby limiting left-/right-sided stroke differences in our sample. While this is an intriguing finding, the limitations of the data and sample size do not allow us to draw further implications. Unfortunately, only 8 participants drove with their unimpaired foot (n = 8; 4 right-body-affected participants who used a left foot accelerator, and 4 left-body-affected participants who continued to drive with their right foot), diminishing the statistical estimations. Nonetheless, lesion side is vital information that should be collected in future studies on racing simulation and stroke.
In conclusion, low-cost, high-fidelity racing simulation has matured in recent years, and our data support the rigorous study of this technology as a potential assessment tool to help individuals with minor stroke return to safe and active driving. If installed at participants’ homes, patients could minimize visits or return trips to a health care center, which may serve as an especially valuable shift for those already compromised in safe transportation.

 ,
, 



{kind=link}
{kind=link}