
Physical Activity and Sarcopenia in Community-Dwelling Older Adults with Long-Term Care Insurance

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
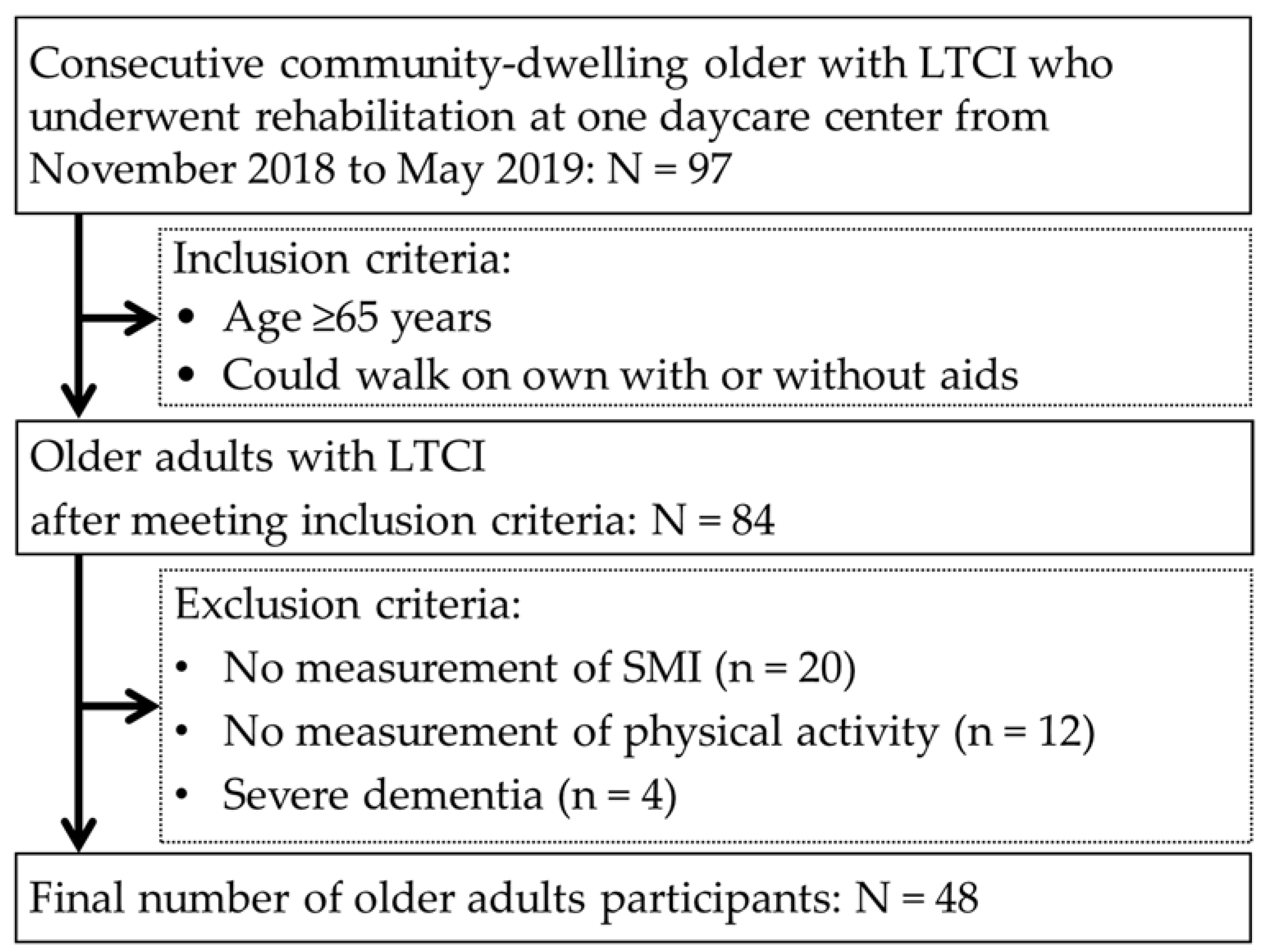
2.1. Design, Setting and Participants Flow
2.2. Measures
2.3. Long-Term Care Insurance
2.4. Physical Activity
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Sarcopenia Group
3.2. Adjusted PA in the Sarcopenia Group
3.3. Cut-Off Value of PA for Sarcopenia
4. Discussion
4.1. Prevalence and PA of Sarcopenia
4.2. Cut-Off Value of PA for Sarcopenia
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. The 2019 Revision of World Population Prospects. Available online: https://esa.un.org/unpd/wpp/ (accessed on 10 May 2021).
- Statistics Bureau, Ministry of Internal Affairs and Communications. Available online: https://www.stat.go.jp/data/topics/topi1135.html (accessed on 10 May 2021).
- Ministry of Health, Labour and Welfare. Long-Term Care, Health and Welfare Services for the Elderly. Available online: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/index.html (accessed on 10 May 2021).
- Inoue, N. The chronological trend of the bedridden status and preventative factors and cumulative survival rate during three years in the Japanese urban elderly dwellers. Bull. Soc. Med. 2012, 30, 1–12. Available online: http://jssm.umin.jp/report/no30-1/30-1-01.pdf (accessed on 10 May 2021). (In Japanese).
- Choi, J.K.; Joung, E. The association between the utilization of long-term care services and mortality in elderly Koreans. Arch. Gerontol. Geriatr. 2016, 65, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Konagaya, Y.; Watanabe, T. Evaluation of multimodal factors for the certification of long-term care insurance among community-dwelling elderly: A four-year follow-up study. Nippon Ronen Igakkai Zasshi Jpn. J. Geriatr. 2014, 51, 170–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990S–991S. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Yoshida, D.; Honda, T.; Hata, J.; Shibata, M.; Hirakawa, Y.; Furuta, Y.; Kishimoto, H.; Ohara, T.; Kitazono, T.; et al. Prevalence and mortality of sarcopenia in a community-dwelling older Japanese population: The Hisayama Study. J. Epidemiol. 2021, 31, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y.; et al. Sarcopenia: Prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J. Cachexia Sarcopenia Muscle 2021, 12, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Nishiguchi, S.; Fukutani, N.; Tanigawa, T.; Yukutake, T.; Kayama, H.; Aoyama, T.; Araiet, H. Prevalence of sarcopenia in community-dwelling Japanese older adults. J. Am. Med. Dir. Assoc. 2013, 14, 911–915. [Google Scholar] [CrossRef] [PubMed]
- Yuki, A.; Ando, F.; Shimokata, H. Aging-related frailty and sarcopenia. Epidemiology of frailty and sarcopenia. Clin. Calcium 2018, 28, 1183–1189. (In Japanese) [Google Scholar]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [PubMed] [Green Version]
- Landi, F.; Abbatecola, A.M.; Provinciali, M.; Corsonello, A.; Bustacchini, S.; Manigrasso, L.; Cherubini, A.; Bernabei, R.; Lattanzio, F. Moving against frailty: Does physical activity matter? Biogerontology 2010, 11, 537–545. [Google Scholar] [CrossRef]
- Landi, F.; Russo, A.; Cesari, M.; Pahor, M.; Liperoti, R.; Danese, P.; Bernabei, R.; Onder, G. Walking one hour or more per day prevented mortality among older persons: Results from ilSIRENTE study. Prev. Med. 2008, 47, 422–426. [Google Scholar] [CrossRef]
- Landi, F.; Marzetti, E.; Martone, A.M.; Bernabei, R.; Onder, G. Exercise as a remedy for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Watanabe, Y.; Ikenaga, M.; Yokoyama, K.; Yoshida, T.; Morimoto, T.; Kimura, M. Comparison of single- or multifrequency bioelectrical impedance analysis and spectroscopy for assessment of appendicular skeletal muscle in the elderly. J. Appl. Physiol. 2013, 115, 812–818. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Tung, H.H.; Liu, C.Y.; Chen, L.K. Physical activity and sarcopenia in the geriatric population: A systematic review. J. Am. Med. Dir. Assoc. 2018, 9, 378–383. [Google Scholar] [CrossRef]
- Oliveira, J.S.; Pinheiro, M.B.; Fairhall, N.; Walsh, S.; Chesterfield Franks, T.; Kwok, W.; Bauman, A.; Sherrington, C. Evidence on physical activity and the prevention of frailty and sarcopenia among older people: A systematic review to inform the World Health Organization Physical Activity Guidelines. J. Phys. Act. Health 2020, 17, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Ida, S.; Kaneko, R.; Murata, K. SARC-F for screening of sarcopenia among older adults: A meta-analysis of screening test accuracy. J. Am. Med. Dir. Assoc. 2018, 19, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Mizuta, C.; Yamada, Y.; Okayama, Y.; Nakamura, E. Constructing an index of physical fitness age for Japanese elderly based on 7-year longitudinal data: Sex differences in estimated physical fitness age. Age (Dordr.) 2012, 34, 203–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, M.; Ikezoe, T.; Ichihashi, N.; Tabara, Y.; Nakayama, T.; Takahashi, Y.; Matsuda, F.; Tsuboyama, T.; Nagahama Study Group. Relationship of low muscle mass and obesity with physical function in community dwelling older adults: Results from the Nagahama study. Arch. Gerontol. Geriatr. 2020, 88, 103987. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Schneider, P.L.; Crouter, S.E.; Lukajic, O.; Bassett, D.R., Jr. Accuracy and reliability of 10 pedometers for measuring steps over a 400-m walk. Med. Sci. Sports Exerc. 2003, 35, 1779–1784. [Google Scholar] [CrossRef]
- Park, H.; Park, S.; Shephard, R.J.; Aoyagi, Y. Yearlong physical activity and sarcopenia in older adults: The Nakanojo Study. Eur. J. Appl. Physiol. 2010, 109, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef]
- Wu, X.; Li, X.; Xu, M.; Zhang, Z.; He, L.; Li, Y. Sarcopenia prevalence and associated factors among older Chinese population: Findings from the China Health and Retirement Longitudinal Study. PLoS ONE 2021, 16, e0247617. [Google Scholar] [CrossRef] [PubMed]
- Sato, R.; Sawaya, Y.; Shiba, T.; Hirose, T. Relationship between depression and sarcopenia in Japanese elderly with mild long-term care or support needs. Rigakuryoho Kagaku 2020, 35, 673–677. (In Japanese) [Google Scholar] [CrossRef]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef] [Green Version]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1772–1774. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Chen, T.; Kishimoto, H.; Yatsugi, H.; Kumagai, S. Associations of objectively measured patterns of sedentary behavior and physical activity with frailty status screened by the Frail Scale in Japanese community-dwelling older adults. J. Sports Sci. Med. 2020, 19, 166–174. [Google Scholar]
- Crouter, S.E.; Schneider, P.L.; Karabulut, M.; Bassett, D.R., Jr. Validity of 10 electronic pedometers for measuring steps, distance, and energy cost. Med. Sci. Sports Exerc. 2003, 35, 1455–1460. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Hillel, I.; Shustak, S.; Del Din, S.; Bekkers, E.M.J.; Pelosin, E.; Nieuwhof, F.; Rochester, L.; Mirelman, A. Everyday stepping quantity and quality among older adult fallers with and without mild cognitive impairment: Initial evidence for new motor markers of cognitive deficits? J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1078–1082. [Google Scholar] [CrossRef]
- Gianfredi, V.; Blandi, L.; Cacitti, S.; Minelli, M.; Signorelli, C.; Amerio, A.; Odone, A. Depression and objectively measured physical activity: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 3738. [Google Scholar] [CrossRef] [PubMed]
- Yoshiuchi, K.; Nakahara, R.; Kumano, H.; Kuboki, T.; Togo, F.; Watanabe, E.; Yasunaga, A.; Park, H.; Shephard, R.J.; Aoyagi, Y. Yearlong physical activity and depressive symptoms in older Japanese adults: Cross-sectional data from the Nakanojo Study. Am. J. Geriatr. Psychiatry 2006, 14, 621–624. [Google Scholar] [CrossRef]
- Izawa, K.P.; Watanabe, S.; Hiraki, K.; Morio, Y.; Kasahara, Y.; Takeichi, N.; Oka, K.; Osada, N.; Omiya, K. Determination of the effectiveness of accelerometer use in the promotion of physical activity in cardiac patients: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2012, 93, 1896–1902. [Google Scholar] [CrossRef] [PubMed]
- Kono, Y.; Yamada, S.; Yamaguchi, J.; Hagiwara, Y.; Iritani, N.; Ishida, S.; Araki, A.; Hasegawa, Y.; Sakakibara, H.; Koike, Y. Secondary prevention of new vascular events with lifestyle intervention in patients with noncardioembolic mild ischemic stroke: A single-center randomized controlled trial. Cerebrovasc. Dis. 2013, 36, 88–97. [Google Scholar] [CrossRef]
- Miyanaga, M.; Fujii, M.; Sakai, H.; Morimoto, K.; Sudo, M.; Niki, Y.; Tokimitsu, I. Effects of a walking program using a physical activity monitoring device on elderly requiring support or low-level care. Jpn. J. Phys. Fitness Sports Med. 2015, 64, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Goto, K.; Yamamoto, T.; Kashiwazaki, M.; Miura, K.; Kubo, A. Longitudinal changes and characteristics of the number of steps of subjects with different levels of care needs. Rigakuryoho Kagaku 2018, 33, 623–629. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Tsukishima, E. Disease requiring severe-level care certification for long-term care insurance. Nihon Koshu Eisei Zasshi Jpn. J. Public Health 2017, 64, 655–663. (In Japanese) [Google Scholar]
- Narazaki, K.; Kumagai, S. Associations of frailty, physical activity, and physical fitness with incident long-term care and support needs in community-dwelling older Japanese adults. Jpn. J. Phys. Fit. Sports Med. 2019, 68, 303–312. [Google Scholar] [CrossRef]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Kasahara, Y.; Morio, Y.; Hiraki, K.; Hirano, Y.; Omori, Y.; Suzuki, N.; Kida, K.; et al. Sarcopenia and physical activity in older male cardiac patients. Int. J. Cardiol. 2016, 222, 457–461. [Google Scholar] [CrossRef]
- Takayanagi, N.; Sudo, M.; Yamashiro, Y.; Chiba, I.; Lee, S.; Niki, Y.; Shimada, H. Screening prefrailty in Japanese community-dwelling older adults with daily gait speed and number of steps via tri-axial accelerometers. Sci. Rep. 2021, 11, 18673. [Google Scholar] [CrossRef]
- Turunen, K.; Aaltonen, L.; Kumpumäki, J.; Portegijs, E.; Keikkala, S.; Kinnunen, M.L.; Finni, T.; Sipilä, S.; Nikander, R. A tailored counseling and home-based rehabilitation program to increase physical activity and improve mobility among community-dwelling older people after hospitalization: Protocol of a randomized controlled trial. BMC Musculoskelet. Disord. 2017, 18, 477. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Sarcopenia | No Sarcopenia | t, Z or χ2 Value | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| n= 20 | n = 28 | |||||||
| Prevalence of sarcopenia, % | 41.7 | 58.3 | ||||||
| Age, years | 78.4 | ± | 7.4 | 77.8 | ± | 6.8 | 0.3 | 0.790 |
| Sex, Male, % | 40.0 | 25.0 | 1.2 a | 0.270 | ||||
| BMI, kg/m2 | 22.7 | ± | 3.3 | 25.8 | ± | 4.5 | 2.2 b | 0.025 |
| SMI, kg/m2 | 5.6 | ± | 0.8 | 6.5 | ± | 1.0 | 3.2 | 0.002 |
| LTCI level, % | ||||||||
| Support level 1 | 63.2 | 53.6 | 3.2 a | 0.530 | ||||
| Support level 2 | 10.5 | 25.0 | ||||||
| Care level 1 | 10.5 | 14.3 | ||||||
| Care level 2 | 10.5 | 7.1 | ||||||
| Care level 3 | 5.3 | 0.0 | ||||||
| Comorbidity, % | ||||||||
| Hypertension | 65.0 | 78.6 | 1.1 a | 0.300 | ||||
| Diabetes | 25.0 | 14.3 | 0.9 a | 0.350 | ||||
| Orthopedic disease | 50.0 | 60.7 | 0.5 a | 0.460 | ||||
| Neurological disease | 40.0 | 39.3 | <0.1 a | 0.960 | ||||
| Heart disease | 80.0 | 78.6 | <0.1 a | 0.900 | ||||
| Cancer disease | 20.0 | 14.3 | 0.3 a | 0.600 | ||||
| Physical function, Physical activity | ||||||||
| Handgrip strength, kg | 19.2 | ± | 7.2 | 21.8 | ± | 8.6 | 1.1 | 0.268 |
| One leg standing time, s | 6.8 | ± | 13.2 | 13.4 | ± | 17.1 | 1.7 b | 0.088 |
| Gait speed, m/s | 0.70 | ± | 0.18 | 0.93 | ± | 0.30 | 3.1 | 0.004 |
| Physical activity, step/day | 1052.4 | ± | 739.2 | 2388.3 | ± | 2044.4 | 2.4 b | 0.014 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitamura, M.; Izawa, K.P.; Ishihara, K.; Matsuda, H.; Okamura, S.; Fujioka, K. Physical Activity and Sarcopenia in Community-Dwelling Older Adults with Long-Term Care Insurance. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1610-1618. https://doi.org/10.3390/ejihpe11040114
Kitamura M, Izawa KP, Ishihara K, Matsuda H, Okamura S, Fujioka K. Physical Activity and Sarcopenia in Community-Dwelling Older Adults with Long-Term Care Insurance. European Journal of Investigation in Health, Psychology and Education. 2021; 11(4):1610-1618. https://doi.org/10.3390/ejihpe11040114
Chicago/Turabian StyleKitamura, Masahiro, Kazuhiro P. Izawa, Kodai Ishihara, Hiroaki Matsuda, Soichiro Okamura, and Koji Fujioka. 2021. "Physical Activity and Sarcopenia in Community-Dwelling Older Adults with Long-Term Care Insurance" European Journal of Investigation in Health, Psychology and Education 11, no. 4: 1610-1618. https://doi.org/10.3390/ejihpe11040114