Comparison of Commercial ELISA Kits, a Prototype Multiplex Electrochemoluminescent Assay, and a Multiplex Bead-Based Immunoassay for Detecting a Urine-Based Bladder-Cancer-Associated Diagnostic Signature

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Initial Performance of Commercial ELISA Assays and Two Multiplex Array Platforms
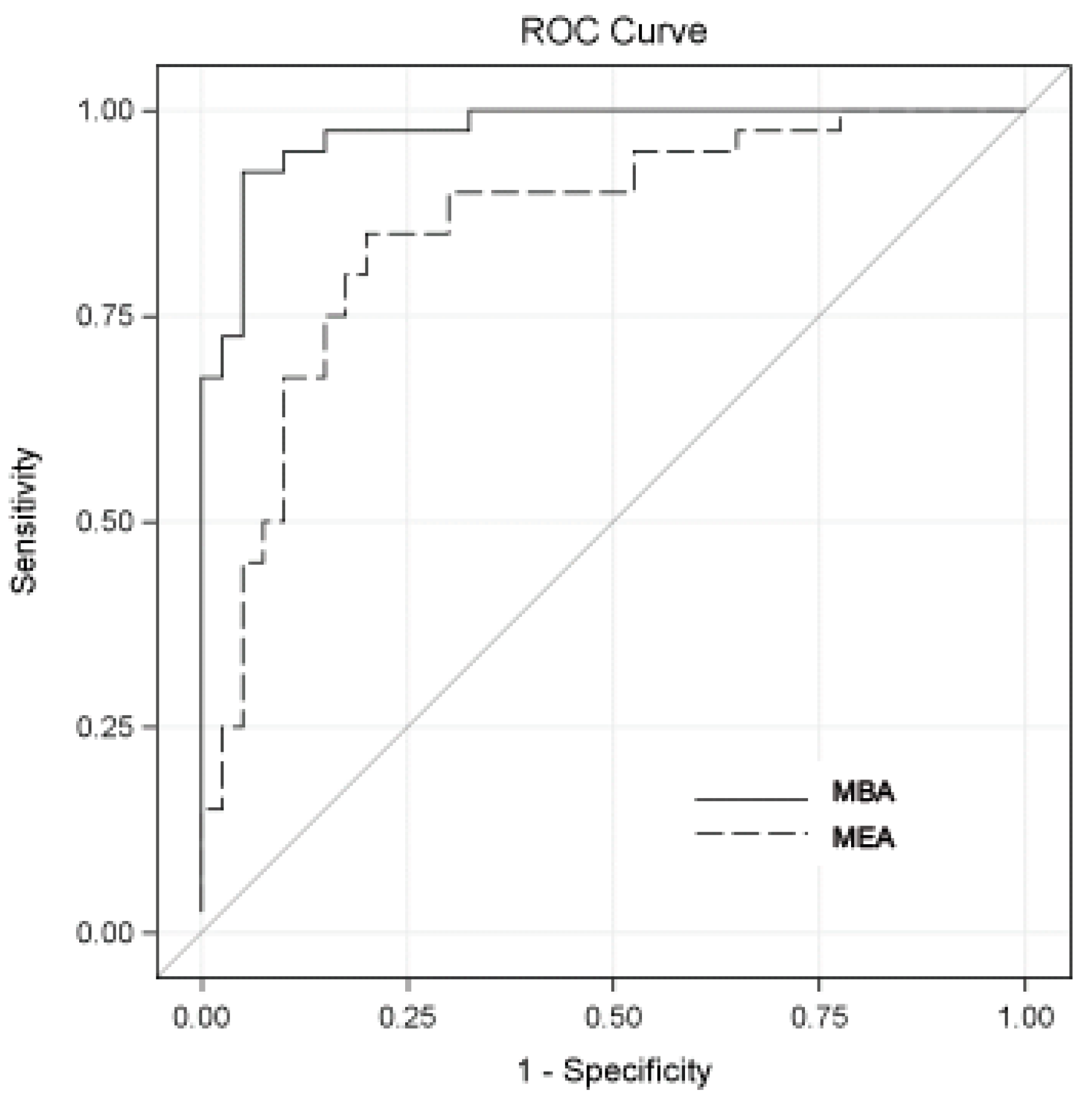
2.2. Initial Diagnostic Accuracy Performance of Multiplex Array Platforms (MEA and MBA)
3. Discussion
4. Materials and Methods
4.1. Patients and Specimen Processing
4.2. Commercial Enzyme-Linked Immunosorbent Assays (ELISA)
4.3. Multiplex Array Platforms
4.4. Data Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nguyen, B.; Cusumano, P.G.; Deck, K.; Kerlin, D.; Garcia, A.A.; Barone, J.L.; Rivera, E.; Yao, K.; de Snoo, F.A.; van den Akker, J.; et al. Comparison of Molecular Subtyping with BluePrint, MammaPrint, and TargetPrint to Local Clinical Subtyping in Breast Cancer Patients. Ann. SurgOncol. 2012, 19, 3257–3263. [Google Scholar] [CrossRef] [PubMed]
- Malo, T.L.; Lipkus, I.; Wilson, T.; Han, H.S.; Acs, G.; Vadaparampil, S.T. Treatment Choices Based on OncotypeDx in the Breast Oncology Care Setting. J. Cancer Epidemiol. 2012, 2012, 941495. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, D.; Goddard, A.D.; Natraj, N.; Cherbavaz, D.B.; Clark-Langone, K.M.; Snable, J.; Watson, D.; Falzarano, S.M.; Magi-Galluzzi, C.; Klein, E.A.; et al. Analytical validation of the Oncotype DX prostate cancer assay - a clinical RT-PCR assay optimized for prostate needle biopsies. BMC Genom. 2013, 14, 690. [Google Scholar] [CrossRef] [PubMed]
- Rosser, C.J.; Ross, S.; Chang, M.; Dai, Y.; Mengual, L.; Zhang, G.; Kim, J.; Urquidi, V.; Alcaraz, A.; Goodison, S. Multiplex protein signature for the detection of bladder cancer in voided urine samples. J. Urol. 2013, 190, 2257–2262. [Google Scholar] [CrossRef]
- Urquidi, V.; Goodison, S.; Kim, J.; Chang, M.; Dai, Y.; Rosser, C.J. Vascular endothelial growth factor, carbonic anhydrase 9, and angiogenin as urinary biomarkers for bladder cancer detection. Urology 2012, 79, 1185.e1–1185.e6. [Google Scholar] [CrossRef]
- Urquidi, V.; Chang, M.; Dai, Y.; Kim, J.; Wolfson, E.D.; Goodison, S.; Rosser, C.J. IL-8 as a urinary biomarker for the detection of bladder cancer. BMC Urol. 2012, 12, 12. [Google Scholar] [CrossRef]
- Urquidi, V.; Goodison, S.; Ross, S.; Chang, M.; Dai, Y.; Rosser, C.J. Diagnostic potential of urinary α1-antitrypsin and apolipoprotein E in the detection of bladder cancer. J. Urol. 2012, 188, 2377–2383. [Google Scholar] [CrossRef]
- Urquidi, V.; Kim, J.; Chang, M.; Dai, Y.; Rosser, C.J.; Goodison, S. CCL18 in a multiplex urine-based assay for the detection of bladder cancer. PLoS ONE 2012, 7, e37797. [Google Scholar] [CrossRef]
- Rosser, C.J.; Liu, L.; Sun, Y.; Villicana, P.; McCullers, M.; Porvasnik, S.; Young, P.R.; Parker, A.S.; Goodison, S. Bladder Cancer-Associated Gene Expression Signatures Identified by Profiling of Exfoliated Urothelia. Cancer Epidemiol. Biomarkers Prev. 2009, 2, 444–453. [Google Scholar] [CrossRef]
- Urquidi, V.; Goodison, S.; Cai, Y.; Sun, Y.; Rosser, C.J. A Candidate Molecular Biomarker Panel for the Detection of Bladder Cancer. Cancer Epidemiol. Biomarkers Prev. 2012, 12, 2149–2158. [Google Scholar] [CrossRef]
- Kreunin, P.; Zhao, J.; Rosser, C.J.; Urquidi, V.; Lubman, D.M.; Goodison, S. Bladder Cancer Associated Glycoprotein Signatures revealed by Urinary Proteomic Profiling. J. Proteome Res. 2007, 6, 2631–2639. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.; Feng, S.; Shedden, K.; Xie, X.; Liu, Y.; Rosser, C.J.; Lubman, D.M.; Goodison, S. Urinary Glycoprotein Biomarker Discovery for Bladder Cancer Detection using LC-MS/MS and Label-free Quantification. Clin. Cancer Res. 2011, 17, 3349–3359. [Google Scholar] [CrossRef] [PubMed]
- Goodison, S.; Chang, M.; Dai, Y.; Urquidi, V.; Rosser, C.J. A multi-analyte assay for the non-invasive detection of bladder cancer. PLoS ONE 2012, 7, e47469. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.M.; Chang, M.; Dai, Y.; Chai, K.X.; Dyrskjøt, L.; Sanchez-Carbayo, M.; Szarvas, T.; Zwarthoff, E.C.; Lokeshwar, V.; Jeronimo, C.; et al. External validation of a multiplex urinary protein panel for the detection of bladder cancer in a multicenter cohort. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1804–1812. [Google Scholar] [CrossRef] [PubMed]
- Rosser, C.J.; Chang, M.; Dai, Y.; Ross, S.; Mengual, L.; Alcaraz, A.; Goodison, S. Urinary protein biomarker panel for the detection of recurrent bladder cancer. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1340–1345. [Google Scholar] [CrossRef]
- Masuda, N.; Ogawa, O.; Park, M.; Liu, A.Y.; Goodison, S.; Dai, Y.; Kozai, L.; Furuya, H.; Lotan, Y.; Rosser, C.J.; et al. Meta-analysis of a 10-plex urine-based biomarker assay for the detection of bladder cancer. Oncotarget 2018, 9, 7101–7111. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.; Liu, J.; Wang, Y.; Wang, L.; Weng, S.; Chen, S.; Yang, G.Y. Cocktail blood biomarkers: Prediction of clinical outcomes in patients with acute ischemic stroke. Eur. Neurol. 2013, 69, 68–75. [Google Scholar] [CrossRef]
- Szarvas, T.; Nyirády, P.; Ogawa, O.; Furuya, H.; Rosser, C.J.; Kobayashi, T. Urinary Protein Markers for the Detection and Prognostication of Urothelial Carcinoma. Methods Mol. Biol. 2018, 1655, 251–273. [Google Scholar] [CrossRef]
- Shimizu, Y.; Furuya, H.; Bryant Greenwood, P.; Chan, O.; Dai, Y.; Thornquist, M.D.; Goodison, S.; Rosser, C.J. A multiplex immunoassay for the non-invasive detection of bladder cancer. J. Transl. Med. 2016, 14, 3110. [Google Scholar] [CrossRef]
- Goodison, S.; Ogawa, O.; Matsui, Y.; Kobayashi, T.; Miyake, M.; Ohnishi, S.; Fujimoto, K.; Dai, Y.; Shimizu, Y.; Tsukikawa, K.; et al. A multiplex urinary immunoassay for bladder cancer detection: Analysis of a Japanese cohort. J. Transl. Med. 2016, 14, 287. [Google Scholar] [CrossRef]
- Motulsky, H.; Christopoulos, H. Fitting Models to Biological Data Using Linear and Nonlinear Regression: A Practical Guide to Curve Fitting; Oxford University Press: New York, NY, USA, 2004; p. 17. [Google Scholar]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Commercial ELISA Kits | MEA | MBA | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Analyte | CV | LLOQ (pg/mL) | ULOQ (pg/mL) | CV | LLOQ (pg/mL) | ULOQ (pg/mL) | CV | LLOQ (pg/mL) | ULOQ (pg/mL) |
| IL8 | 2.85 | 0.5 | 2033 | 3.65 | 1.23 | 3169 | 3.58 | 2.01 | 1397 |
| MMP9 | 1.69 | 0.1 | 9.0 | 3.14 | 23.9 | 9337 | 3.37 | 14.76 | 7164 |
| MMP10 | 0.00 | 4.13 | 4.13 | 3.01 | 8.94 | 816 | 0.77 | 1.71 | 90.33 |
| VEGFA | 0.91 | 10.0 | 506 | 1.52 | 21.38 | 2587 | 1.61 | 18.24 | 1031 |
| CA9 | 0.00 | 2.28 | 2.28 | 1.47 | 2.06 | 132.32 | 1.04 | 0.48 | 54.07 |
| APOE | 0.31 | 0.03 | 0.087 | 4.32 | 435.81 | 653309 | 2.28 | 78.30 | 1998 |
| PAI1 | 0.38 | 0.05 | 0.168 | 4.46 | 4.47 | 73437 | 2.86 | 0.10 | 426.92 |
| A1AT | 2.63 | 6.0 | 5968 | 3.13 | 4422 | 682690 | 1.55 | 424.31 | 179,724 |
| ANG | 1.74 | 2.9 | 2208 | 2.33 | 18.35 | 19638 | 2.27 | 24.98 | 6557 |
| SDC1 | 1.16 | 9.88 | 474 | 0.84 | 1002 | 38916 | 0.60 | 2608 | 19,051 |
| Cancer Cases (n = 40) | Controls (n = 40) | p | |
|---|---|---|---|
| Age | |||
| 30–65 | 6 (15%) | 12 (30%) | 0.08 |
| 66–70 | 7 (18%) | 12 (30%) | |
| 71–75 | 13 (33%) | 10 (25%) | |
| 76–90 | 14 (35%) | 6 (15%) | |
| Sex | |||
| Male | 36 (90%) | 30 (75%) | 0.14 |
| Female | 4 (10%) | 10 (25%) | |
| Cytology | |||
| Negative | 19 (48%) | ||
| Positive | 13 (33%) | ||
| N/A | 8 (20%) | 40 (100%) | |
| Grade | |||
| Low | 12 (30%) | ||
| High | 21 (53%) | ||
| N/A | 7 (18%) | 40 (100%) | |
| Stage | |||
| Tis | 1 (3%) | ||
| Ta | 21 (53%) | ||
| T1 | 4 (10%) | ||
| T2 | 6 (15%) | ||
| N/A | 8 (20%) | 40 (100%) |
| Biomarker | MEA | MBA | ||||
|---|---|---|---|---|---|---|
| Cancers | Controls | p | Cancers | Controls | p | |
| MMP9 (pg/mL) | 749.0 ± 5949.9 | 439.5 ± 4964.8 | 0.31 | 13.2 ± 355.5 | 36.2 ± 388.8 | 0.13 |
| IL8 (pg/mL) | 13.9 ± 189.4 | 5.8 ± 21.7 | 0.08 | 8.0 ± 66.9 | 5.1 ± 19.5 | 0.31 |
| VEGF (pg/mL) | 205.4 ± 606.8 | 207.2 ± 380.3 | 0.97 | 38.3 ± 121.8 | 41.8 ± 79.0 | 0.76 |
| SCD1 (ng/mL) | 4.9 ± 22.9 | 4.7 ± 7.6 | 0.93 | 5.9 ± 4.8 | 6.2 ± 21.5 | 0.84 |
| ANG(pg/mL) | 140.7 ± 714.8 | 163.2 ± 488.2 | 0.68 | 69.1 ± 321.8 | 93.1 ± 446.9 | 0.45 |
| PA1 (pg/mL) | 32.1 ± 225.9 | 9.9 ± 19.5 | 0.002 | 4.4 ± 28.1 | 1.3 ± 1.3 | 0.001 |
| CA9 (pg/mL) | 7.7 ± 3 4.6 | 5.3 ± 12.3 | 0.26 | 11.2 ± 22.0 | 2.7 ± 6.6 | <.0001 |
| MMP10 (pg/mL) | 15.0 ± 91.9 | 6.5 ± 44.3 | 0.07 | 2.3 ± 9.4 | 4.8 ± 24.7 | 0.06 |
| A1AT (ng/mL) | 18.5 ± 484.0 | 7.1 ± 170.0 | 0.19 | 20.3 ± 82.2 | 25.6 ± 97.6 | 0.52 |
| APOE (ng/mL) | 7.1 ± 18.3 | 2.3 ± 44.6 | 0.03 | 1.1 ± 2.4 | 1.2 ± 2.6 | 0.55 |
| Biomarker | MEA | MBA | Difference | 95% Confidence Interval | p |
|---|---|---|---|---|---|
| MMP9 | 0.48 | 0.64 | 0.16 | (−0.08, 0.39) | 0.19 |
| IL8 | 0.60 | 0.53 | −0.07 | (−0.16, 0.03) | 0.15 |
| VEGF | 0.54 | 0.58 | 0.04 | (−0.07, 0.16) | 0.47 |
| SDC1 | 0.57 | 0.62 | 0.05 | (−0.17, 0.27) | 0.65 |
| ANG | 0.53 | 0.56 | 0.04 | (−0.08, 0.15) | 0.55 |
| PA1 | 0.67 | 0.85 | 0.18 | (0.06, 0.30) | 0.004 |
| CA9 | 0.53 | 0.80 | 0.27 | (0.11, 0.43) | 0.001 |
| MMP10 | 0.59 | 0.62 | 0.03 | (−0.15, 0.21) | 0.75 |
| A1AT | 0.57 | 0.55 | −0.02 | (−0.24, 0.19) | 0.82 |
| APOE | 0.48 | 0.59 | 0.11 | (−0.11, 0.33) | 0.32 |
| Combined | 0.86 | 0.97 | 0.12 | (0.04, 0.19) | 0.003 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furuya, H.; Pagano, I.; Chee, K.; Kobayashi, T.; Wong, R.S.; Lee, R.; Rosser, C.J. Comparison of Commercial ELISA Kits, a Prototype Multiplex Electrochemoluminescent Assay, and a Multiplex Bead-Based Immunoassay for Detecting a Urine-Based Bladder-Cancer-Associated Diagnostic Signature. Diagnostics 2019, 9, 166. https://doi.org/10.3390/diagnostics9040166
Furuya H, Pagano I, Chee K, Kobayashi T, Wong RS, Lee R, Rosser CJ. Comparison of Commercial ELISA Kits, a Prototype Multiplex Electrochemoluminescent Assay, and a Multiplex Bead-Based Immunoassay for Detecting a Urine-Based Bladder-Cancer-Associated Diagnostic Signature. Diagnostics. 2019; 9(4):166. https://doi.org/10.3390/diagnostics9040166
Chicago/Turabian StyleFuruya, Hideki, Ian Pagano, Keanu Chee, Takashi Kobayashi, Regan S. Wong, Riko Lee, and Charles J. Rosser. 2019. "Comparison of Commercial ELISA Kits, a Prototype Multiplex Electrochemoluminescent Assay, and a Multiplex Bead-Based Immunoassay for Detecting a Urine-Based Bladder-Cancer-Associated Diagnostic Signature" Diagnostics 9, no. 4: 166. https://doi.org/10.3390/diagnostics9040166