Liquid Biopsy Potential Biomarkers in Prostate Cancer


Department of Urology, Research Laboratory, University Leipzig, D-04103 Leipzig, Germany
*
Author to whom correspondence should be addressed.
Diagnostics 2018, 8(4), 68; https://doi.org/10.3390/diagnostics8040068
Submission received: 9 August 2018
/
Revised: 12 September 2018
/
Accepted: 14 September 2018
/
Published: 21 September 2018
(This article belongs to the Special Issue Diagnostic Biomarkers in Prostate Cancer)
Abstract
:Prostate cancer (PCa) is the second most common cancer in men worldwide with an incidence of 14.8% and a mortality of 6.6%. Shortcomings in comprehensive medical check-ups in low- and middle-income countries lead to delayed detection of PCa and are causative of high numbers of advanced PCa cases at first diagnosis. The performance of available biomarkers is still insufficient and limited applicability, including logistical and financial burdens, impedes comprehensive implementation into health care systems. There is broad agreement on the need of new biomarkers to improve (i) early detection of PCa, (ii) risk stratification, (iii) prognosis, and (iv) treatment monitoring. This review focuses on liquid biopsy tests distinguishing high-grade significant (Gleason score (GS) ≥ 7) from low-grade indolent PCa. Available biomarkers still lack performance in risk stratification of biopsy naïve patients. However, biomarkers with highly negative predictive values may help to reduce unnecessary biopsies. Risk calculators using integrative scoring systems clearly improve decision-making for invasive prostate biopsy. Emerging biomarkers have the potential to substitute PSA and improve the overall performance of risk calculators. Until then, PSA should be used and may be replaced whenever enough evidence has accumulated for better performance of a new biomarker.
1. Introduction
Prostate cancer (PCa) is the second most common cancer in men worldwide, with an incidence of 14.8% (estimated at 1.1 million in 2012) and a mortality of still 6.6% (an estimated 307,000 deaths in 2012), which is at 5th rank among cancers. The five-year prevalence of 148.6/100,000 is the highest seen in all cancers in adult men [1].
There is a significant variation of incidence, with the highest rates seen in Western and Northern Europe, Australia/New Zealand, and Northern America and the lowest rates in Asian countries, which may be partly due to the comprehensive use of prostate-specific antigen (PSA) testing and close monitoring of the male population in more developed regions. As recently reported in China, the poor coverage of PSA monitoring seems to be the major cause of advanced PCa at first diagnosis, translating into a high mortality of 44% in China compared to 23% in the EU and 14% in the USA [2,3,4].
In this review we will evaluate the performance of available and emerging biomarkers in risk stratification, focusing on liquid biopsies and distinguishing high-risk Gleason score (GS) ≥ 7 tumours from indolent, low-risk tumours, especially in biopsy-naïve patients.
2. Current PCa Diagnostics
At present, the recommendations of the American Urological Association (AUA) and the European Association of Urology (EAU) guidelines for the clinical examination methods of prostate cancer include digital rectal examination (DRE), rectal ultrasound (TRUS) examination, and prostate biopsy [5,6,7].
Biopsy is still the only standard in preoperative diagnosis. This invasive operation causes obvious physical pain to patients and the detection rate was closely related to the number of puncture points and prostate volume, and is likely to cause haematuria, urinary retention or infection, sepsis, and other serious complications leading to distress. At the same time, DRE and TRUS have disadvantages such as poor accuracy and are affected by the skill and experience of the operator and other subjective factors. For instance, 24% of 126 patients with suspected DRE had no PCa on biopsies in a prospective study by Leyten and co-workers [8].
In addition, all three, DRE, TRUS and biopsy, are inevitably faced with an important issue, namely low sensitivity to early cancer, after which the patient has missed the most ideal treatment time [9,10,11].
As proposed by Dr TA Stamey in the early 1980s, PSA diagnostics rapidly developed into comprehensive screening programs in the USA and worldwide [12]. PSA population screening in 6260 Americans showed a significant decrease of high- and intermediate-risk patients from 68.9% to 52.3% and an increase of low-risk disease from 31.2% to 47.7% between 1989 and 2002 [13]. PSA screening caused prostate cancer mortality to fall by 21%, demonstrated in the 13-year follow-up of the European Randomised Study of Screening for Prostate Cancer (ERSPC), indicating that early diagnosis and treatment of prostate cancer were indeed significantly improved by the popularity of serum PSA screening [14,15,16].
However, in the past decade more and more evidence accumulated challenging the benefit of extensive PCa screening programs. Comprehensive PSA screening, in particular, may lead to significant overdiagnosis and overtreatment [17,18,19]. Overdiagnosis and unnecessary prostate biopsies were calculated to occur in 23–42% in PSA screening programs [20]. Thus, there are considerable concerns about the predictive value of PSA levels, PSA density, and even first biopsy in the group of patients eligible for active surveillance following the recommendations of the EAU [21].
One major problem of PSA screening is the different cutoff values used. The threshold of 4.0 ng/mL (commonly used with the Tandem-R, Hybritech test) has to be revised based on the findings of 15.2% PCa in men with PSA ≤ 4 ng/mL in a cohort of 2950 men (aged 62–91 years) by Thompson and co-workers [22]. A considerable 14.9% of those were diagnosed with high-grade (GS ≥ 7) tumours. Even at very low PSA levels of ≤0.5 ng/mL, they found 6.6% PCa, of which 12.5% were high-grade tumours [22]. These findings clearly illustrate the diagnostic shortcomings of PSA.
Age-adjusted PSA cutoffs were tested to improve performance. While age-adjusted PSA cutoffs for total serum PSA (tPSA) and complexed serum PSA (cPSA) were superior to a fixed cutoff in a cohort of 3597 men who underwent routine biopsy, they could not improve the PCa detection rate of approximately 39% within the range of 2.0 ng/mL–20.0 ng/mL [23].
In light of those diagnostic restrictions, there is still an ongoing dispute on PSA testing worldwide. In the USA, PSA screening was evaluated by the U.S. Preventive Services Task Force (USPSTF), leading to amendment of the recommendations on PSA screening in 2008 [24]. The American Urological Association (AUA) stated that PSA screening should apply only to men aged 55 to 69 years and suggested that routine examination be performed once every two years or longer [7,18,25].
However, this diagnostic practice may significantly increase the risk of missing PCa in men <55 years [26] and might increase mortality, which has to be analysed after longer follow-up [27,28]. Nevertheless, recent data analysis shows a continuous increase in the morbidity of biopsies in conjunction with reduction of total biopsies since the 2008 USPSTF recommendations [29]. Amongst the many attempts to solve this diagnostic dilemma, only a few biomarkers are established in clinical practice.
In summary, to date no single serum or urine biomarker or biomarker panel meets the requirements for highly sensitive and specific detection of PCa and differentiation between indolent and significant PCa. Imaging technologies have been greatly improved but still are not sufficiently validated or standardized. Some of the diagnostic tools are already established, such as PSA and its derivatives; others are under critical evaluation and some are exploring the potency of the latest high-end analytics to improve (i) early detection of PCa, (ii) risk stratification, (iii) disease prognosis, and (iv) treatment monitoring.
3. Current PCa Biomarker Tests for Discrimination-Significant and Indolent PCa
The need for better PCa diagnostics has led to a huge number of new strategies for meaningful combinations of established and innovative approaches to open up new biomarker resources. Table 1 gives an overview of commercially available biomarker tests, using liquid biopsy for the detection of high-grade (≥GS 7) PCa and assisting the physician with identifying patients for prostate biopsy and those eligible for active surveillance (for detailed information and more specialized tests, see [30]). Table 1 also demonstrates that PSA cutoff values vary between studies. Age-adjusted use of PSA cutoff values could significantly improve the sensitivity of PSA testing [23].
3.1. Prostate-Specific Antigen (PSA)
PSA, alone or in combination with free/total PSA (f/t PSA) ratio, formerly thought to be of value for distinguishing PCa from BPH, shows only limited sensitivity and insufficient specificity (Table 1; recent meta-analysis by Huang et al. [31]).
Longitudinal PSA screening to determine PSA velocity has been initially described to distinguish PCa from BPH in men aged >60 years at an average rate of change (ng/mL per year) of ≥0.75 with 90% specificity compared to 60% single PSA value ≥4 ng/mL [32]. However, in the following studies these promising results could not be confirmed [31].
3.2. Prostate Health Index and Derivates
The Prostate Health Index (PHI Beckman Coulter, Atlanta, GA, USA) was FDA-approved in 2012. The PHI score combines total, free, and [–2] proPSA in one test and a score is calculated indicating the probability of PCa positive biopsy (phi-score = [−2] proPSA/fPSA) × √tPSA) [46].
In an early meta-analysis, AUCs of %[–2] proPSA and PHI were comparable in patients with PSA values of 2–10 ng/mL, reaching between 0.76 and 0.78 for prediction of PCa-positive biopsies [47]. As recently analysed by White and co-workers, PHI alone impacts the decision-making of physicians and resulted in a significant reduction in biopsies of 40% [48]. However, the PHI score was not very good at predicting high-grade PCa and as such did not help with clinical decision-making in a large study using pT3 stage and/or GS ≥ 7 as outcome measures [49] (see also Table 1 [35]).
3.3. 4KScore® Test
Promising data have also been reported for the 4KScore® Test (OPKO Lab, Nashville, TN, USA) using 4-Kallikrein markers in blood serum after DRE. In a recent study including 496 participants with PSA ≥ 3.0 ng/mL, the accuracy of predicting PCa GS ≥ 7 was AUC 0.738 in the standard model (PSA + age) and AUC 0.820 in the advanced model integrating 4KScore® Test (p < 0.001). In a model with 6% cutoff, the risk calculated by age and 4KScore® would avoid 43% of biopsies, detect 119 of 133 (89.5%) GS ≥ 7 high-risk tumours, and delay diagnosis of 14 (10.5%) of the significant tumours [36].
3.4. Progensa™ (Gen-Probe Inc., San Diego, CA, USA)
The prostate cancer gene 3 (PCA3) test detects long non-coding RNA (lncRNA), which has been shown to be associated with PCa. The Progensa™ PCA3-score calculates the ratio of PCA3 and PSA mRNA of exosomes isolated from post-DRE urine and has been proposed for the identification of patients eligible for active surveillance [50]. It was FDA-approved in 2012 and several studies reported variable performance (sensitivity: 58–78%; specificity: 57–72%) for detection of PCa (Table 1) [39,40,41]. The NPV was reported to be 88% and 90%, respectively, which was regarded as helpful for biopsy decision-making [40,41]. However, as pointed out by Vickers and co-workers, PCA3 was approved by the FDA only to add the decision of repeat biopsy. In biopsy-naïve patients, there is a high risk of missing high-grade PCa with low levels of PCA3 [51].
3.5. Further Non-Commercial and Integrative Tests
Several other tests are already available for risk evaluation in patients with elevated PSA, usually at a threshold of ≥4 ng/mL (Table 1). While their positive predictive value is low (28–36%), those tests showed highly negative predictive values (88–98%), which make them valuable for clinical decision-making on invasive biopsy diagnostics. Tomlins et al. reported avoidance of 35–47% of biopsies using the MiPS test (University of Michigan, MLabs) [43]. Van Neste calculated that 42% of total biopsies and 53% of unnecessary biopsies can be avoided by combining the SelectMDx (MDx Health, Irvine, CA, USA) measuring HOXC6 mRNA and DLX1 mRNA in post-DRE urine with serum PSA, PSA density, DRE status, age, and family history [44].
As summarized in Table 1, more or less critical restrictions regarding the target patients apply to most biomarker test available. Only a few are useful in a broad clinical setting, as required for screening or routine check-up examinations, i.e., for application in biopsy-naïve patients. Especially for the detection of critical high-risk patients (“risk of Gleason score ≥ 7”) who need to undergo prostate biopsy, the specificity of the available tests is poor. For detailed information, the reader is referred to the literature given in Table 1.
4. Do We Need More Biomarkers, or Do We Need a New, Consistent Concept?
In view of the huge number of different biomarkers available and new approaches, one has to ask whether there is a realistic chance that these advanced methods will finally provide a set of biomarkers able to meet all requirements in PCa detection, stratification, and monitoring. Most probably, we will need a combination of specialized biomarkers with good performance within their restricted fields. The primary goal should be to reduce the need for invasive prostate biopsies to improve the benefit‒harm balance.
An ideal biomarker concept should support low-invasive, organ-saving treatments if possible; radical surgery if necessary at the earliest time point to avoid PCa progression to metastatic and androgen-insensitive disease [52].
5. Emerging Biomarkers for Detection of Significant PCa
5.1. Polypeptides
Seminal plasma is a body fluid directly related to the prostate. Therefore, PCa specific analytes are expected to be available at higher concentrations and better accessible than in urine or blood. An in-depth proteome analysis of expressed prostatic secretions (EPS) was conducted in 2010 by Drake and co-workers to provide a resource for the development of biomarkers [53]. In a small cohort of patients with advanced (n = 8) or organ-confined (n = 8) prostate cancer, a total of 624 unique proteins were identified in EPS by mass spectrometry [54]. Fourteen candidates with 133 differently expressed proteins were further analysed for suitability as biomarkers, including PSA and PAP, which were significantly elevated in organ-confined PCa. The authors concluded that EPS-urines are a promising source for new PCa biomarkers [54].
In a multicentre, open-label case/control study our group analysed 125 patients for PCa-specific polypeptides in seminal plasma from fresh ejaculate donation after physiological liquefaction. The idea was to create stable conditions reflecting the enzymatic activity of pathological protease network in PCa, and to analyse the resulting protein fragments, ≤20 kDa polypeptides by capillary-electrophoresis mass spectroscopy (CE-MS). We were able to define a panel of 11 polypeptides from seminal plasma-based CE-MS analysis with 80% sensitivity at 82% specificity in discriminating patients with GS 7 and organ-confined (<pT3a) or advanced disease (≥pT3a) [55].
Proteomic signatures of polypeptides have also been used to detect PCa in the urine of biopsy-naïve patients without known PCa or suspect DRE [56]. The biomarker panel of 12 polypeptides detected PCa with 89% sensitivity and 51% specificity (AUC 0.70). By inclusion of age and fPSA, the performance was augmented to 91% sensitivity and 69% specificity [56]. Unfortunately, the data were not analysed for prediction in high-risk patients.
5.2. Metabolites
Metabolites were shown to closely reflect aggressiveness of PCa [57]. A prospective study including 1122 cases tested the performance of sarcosine to predict the risk of prostate cancer. This study revealed an association of serum sarcosine levels normalized to alanine with low-grade (non-aggressive) PCa but no association with aggressive PCa [58], and a recent study showed that sarcosine is not indicative of PCa in urine [59].
Post-DRE urine pellet is used as a source for metabolites to predict high-grade PCa (GS ≥ 7) in the Polarix® test (Metabolon Inc., Morrisville, NC, USA). In a retrospective study, McDunn and co-workers identified metabolites associated with the aggressiveness of a tumour and constructed a panel of four metabolites (5,6-dihydrouracil, choline phosphate, glycerol, and methylpalmitate) predicting the probability of organ-confined PCa with an accuracy of AUC = 0.62. Using a panel of three metabolites (7-a-hydroxy-3-oxo-4-cholestenoate, pregnen-diol disulfate, and mannosyl tryptophan), they were also able to improve the prediction of progression-free survival to AUC = 0.64 [57]. While these results are promising, the performance of urine metabolites is still not satisfying. However, the study provides the basis for further development of metabolite biomarkers.
Most interestingly, PCa-specific metabolites have been found in urine exosomes, implying potential use as a new biomarker source to address PCa pathogenesis and progression. Out of 248 metabolites identified, 76 were differentially expressed in PCa and BPH [60].
Metabolomics is a hot topic in current biomarker research. However, so far, even large studies did not successfully identify meaningful metabolites [61].
5.3. MicroRNA (miRNA)
MiRNAs have been acknowledged to be important for gene regulation in normal and pathological conditions. Based on tissue analyses, dozens of miRNAs have been shown to be dysregulated in PCa (see [62,63]).
In a comprehensive screening study using radical prostatectomy samples of 34 patients, 34 miRNA were significantly upregulated in the tumour epithelium compared to normal epithelium [64]. The authors also compared GS 6 PCa with high-grade GS ≥ 8 PCa tissue. They found 18 differentially expressed miRNAs (p < 0.005): 11 were up- and seven were downregulated (Table 2).
Schaefer et al. reported five upregulated and 10 downregulated miRNAs during miRNA microarray analysis of 76 radical prostatectomy specimens comparing matched tumour and adjacent normal tissues [65]. The expression of five miRNAs correlated with Gleason score, and upregulated miR-96 predicted biochemical recurrence (Table 2).
However, Stephan et al.’s study of miR-183 (upregulated) and miR-205 (downregulated) failed to detect high-grade PCa in patients with and without PCa (38 each group) using urine sediment, while PCA3 was able to separate those patient groups [66]. In a recent meta-analysis, Song et al. identified from an extensive literature survey 10 upregulated and 14 downregulated miRNAs with potential for separating PCa from BPH or normal controls (Table 2). Furthermore, high expression of miR-32 and let-7c differentiated local from metastatic PCa. The authors also found that the expression profiles of urine, blood serum, and tissue differed considerably [62].
Circulating miRNAs were isolated from various body fluids, including blood plasma and serum being protected against ribonuclease degradation by inclusion in lipid compartments, extracellular vesicles of 40–5000 nm in diameter [67].
In serum, miR-141 levels can distinguish PCa from healthy controls with an AUC of 0.907 with 60% sensitivity at 100% specificity in a cohort of 25 PCa and 25 age-matched healthy control individuals [68]. In a recent study Porzycki et al. found that the combination of miR-141, miR-21, and miR-375 could distinguish PCa (mean PSA of 21.3 ng/mL) from healthy controls with an AUC of 0.864 and a sensitivity of 93% at 63% specificity. However, the group sizes were quite small (20 PCa vs. eight healthy controls), requiring further validation of the findings in larger cohorts [69].
Recently, Tinay et al. found a significant upregulation of miR-9-3p, miR-330-3p-3p, and miR-345-5p in PCa patients (n = 25) compared to healthy controls (n = 20). MiR-345-5p was further analysed due to its direct targeting of CDKN1A encoding the cyclin-dependent kinase inhibitor p21 [70]. Interestingly, the overlap between the miRNAs in serum with tissue miRNAs is limited to miR-21, miR-141, and miR-375 (boldface and labelled “l” in Table 2).
In urine, PCa-specific miRNAs patterns can be detected in exosomes by next-generation sequencing (NGS) and RT-qPCR. For example, miR-196a-5p and miR-501-3p levels were significantly downregulated in a preliminary study of 28 PCa (GS ≥ 7) vs. 19 healthy controls [71]. In a larger study, including 215 PCa patients, 23 BPH patients, and 62 asymptomatic control individuals, Stuopelyte et al. found 100 out of 754 miRNAs scanned deregulated in PCa. MiR-148a and miR-375 were the most abundant miRNAs in urine and showed high sensitivity and specificity (85.31% and 65.22%, respectively), with an AUC of 0.79 in differentiation between PCa (n = 72) and BPH (n = 23). In combination with serum PSA, the AUC was 0.85, with 84.29% sensitivity at 76.19% specificity. Within the grey zone PSA levels of 4–10 ng/mL AUC increased to 0.90 with 83.87% sensitivity at 81.82% sensitivity [72]. Overlapping miRNAs were in boldface and labelled “m” in Table 2.
None of the current miRNA approaches provide high PPV for the detection of high-grade PCa. The largest NPV of 0.939 has been reported to predict the absence of high-grade PCa compared to BPH for a 14-miRNA panel: miR-24, -26b, -30c, -93, -100, -103, -106a, -107, -130b, -223, -146a, -451, -874, and let-7a [73].
The high number of miRNAs found to be dysregulated in PCa and the ability of subsets to either detect PCa, differentiate high-grade from low-grade PCa, or predict recurrence-free/overall survival encourages further attempts to define miRNA biomarker panels. Most interestingly, the overlap between tissue and liquid biopsies is rather limited. This problem has to be investigated more deeply.
5.4. Gene Expression of PCa-Related Genes in Exosomes
Exosomes can be used to measure gene expression of PCa-related genes (among others: SPDEF, ERG and PCA3). Combined into a score (ExoDx Prostate IntelliScore urine exosome assay (Exosome Diagnostics, Inc., Waltham, MA, USA)) with standard of care parameters: prostate-specific antigen level, age, race, and family history [42], this score was able to predict high-risk PCa, defined as GS ≥ 7, with a sensitivity of 92%. However, specificity was low (34%) resulting in a positive predictive value (PPV) of only 36%. In contrast, the negative predicted value (NPV) was high (91%), thereby unnecessary biopsies could have been avoided in 27%, missing only 5% of patients with high-risk PCa (GS 4 + 3) [42], indicating a considerable clinical value of tests providing high NPV, even if the PPV is low (Table 1).
5.5. Long Non-Coding RNA (lncRNA)
Non-coding RNA makes up the vast majority of our genetic information. Only <3% of the human DNA comprises protein-coding gene sequences. LncRNAs are key regulators of the genome and their involvement in several disease states, especially cancer has recently emerged [74,75,76]. Thus, lncRNAs are regarded as promising biomarkers as well as therapeutic targets in urologic cancers [77,78]. Several biomarker tests including lncRNA (PCA3) are already on the market (Table 1).
5.6. Circulating Tumour Cells (CTC)
At the moment circulating tumour cells (CTC) are not used for early detection of high-grade PCa because they are rarely detected in localized PCa [89,90,91,92]. CTCs are being investigated for use as a prognostic biomarker of mCRPC and to predict treatment efficacy [93,94,95,96]. However, the first long-term follow-up studies have questioned the prognostic value of preoperative CTCs for the prediction of early biochemical recurrence. Meyer et al. detected CTCs in only 11% (17/152) of patients before radical prostatectomy. The CTC counts did not correlate with PSA levels, disease status, or biochemical recurrence [97]. Recently, Murray et al. concluded that the biological characteristics of circulating prostate cells (CPCs) may be more important than the number of circulating cells. They found that patients with CD82-negative CPCs had a worse prognosis in a study of 285 men at a follow-up of 10 years. CD82 is a tumour suppressor and the expression on CPCs may indicate high metastatic potential [98].
6. Integrative Scoring Systems/Risk Calculators
The overall goal of all biomarkers is the improvement of the prediction of the individual risk of the patient. To this end, standard null hypothesis significance testing (NHST) methods are not conducive, since they do not report quantitative percent individual risk evaluation. Bayesian data analysis can overcome this weakness and provide direct access to meaningful risk evaluation. Risk calculators such as the online Prostate Cancer Prevention Trial Risk Calculator (PCPTRC) developed in 2006 predicting the likelihood of detecting no versus low-grade (GS < 7) versus high-grade (GS ≥ 7) in a biopsy for an individual patient can be continuously adjusted on the basis of newly available epidemiologic data [99,100,101]. New biomarkers replacing lower-performing ones may be included when available, thus continuously improving the performance of those calculators. Several complex scoring models for risk assessment of PCa GS ≥ 7 have been developed, including population adaption: the Stockholm model 3 (STHLM3) [45], the Rotterdam Prostate Cancer Risk Calculator (RPCRC) [102], the Indonesian prostate cancer risk calculator (IPCRC) [103], a Chinese (Hong Kong) adaptation of the ERSPC risk calculator [104], the Huashan risk calculator [105], and the Chinese Prostate Cancer Consortium Risk Calculator (CPCC-RC) [106].
7. Conclusions
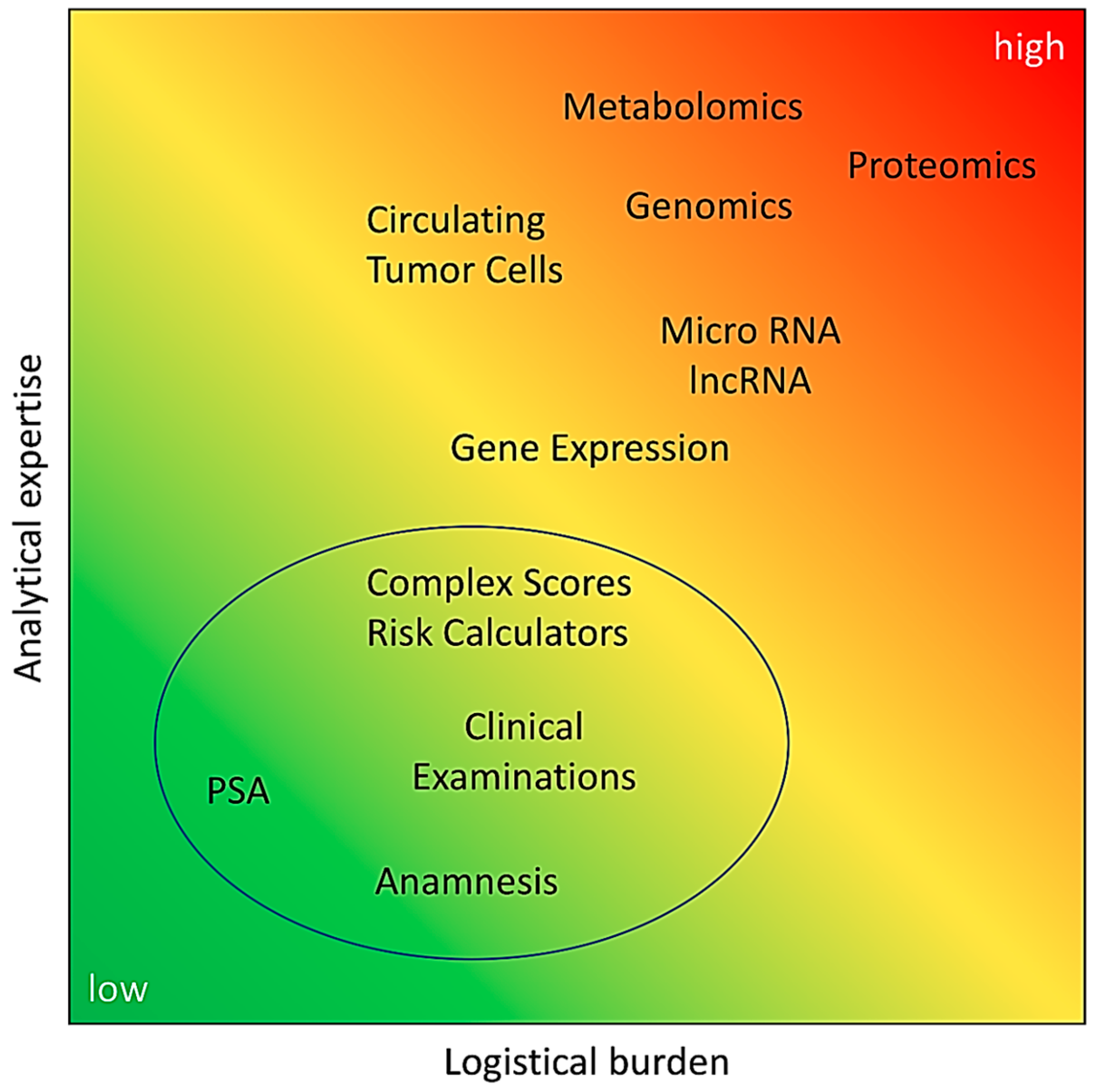
In this review we focused on the liquid biopsy biomarkers currently in use and emerging for distinguishing patients with low, insignificant PCa from patients with high-risk PCa with a Gleason score ≥ 7. Biomarker development faces some common challenges that may limit the usability of biomarkers in clinical routine. The accuracy of transrectal ultrasound (TRUS)-guided needle biopsy is limited by a false negative rate of 23% [107]. Serial biopsies can improve the detection rate of organ-confined PCa from 77% at first biopsy to 99% at fourth biopsy [107]. However, since this initial study in 2002 the number of biopsy cores to be obtained increased from quadrant biopsy (four cores) to sextant biopsies (six cores) and, recently, to a standard of 10–12 cores, as recommended by the guidelines of the EAU. Nevertheless, detection rates are still in the range of 35% [36]. This results in significant uncertainty when using systematic biopsy as a reference standard. In addition, there is a significant upgrading of tumour grade of up to 56.7%, as demonstrated by studies comparing biopsy and final Gleason score after radical prostatectomy [21,108,109]. This causes another serious problem in defining the reference standard in biomarker studies, because whole-gland histopathological evaluation is only available after tumour radical prostatectomy and in rare cases of prostate enucleation due to large volume BPH. Furthermore, in healthy control groups neither biopsy material nor whole-gland tissue is available, reducing the determination of “tumour-free” status to clinical observation and exclusion of other biomarkers (in practice, mostly suspicious PSA levels). Another challenge is the population bias, e.g., shown in metabolomic studies. Special care has to be taken in conception, sampling, and sample processing to account for ethnic and lifestyle differences [110,111]. Population-based adjustment of biomarker panels and cutoffs is required, e.g., for Asian and Western countries [112,113,114,115]. All biomarkers have to compete against PSA and most outperform PSA in certain patient groups. While PSA assays are standardized, comparable, and easy to handle, with a low logistical burden, many of the novel biomarkers make higher demands on clinical staff, organization, laboratory equipment, and data analysis (Figure 1).
In addition, the superiority to PSA has to be validated in large prospective studies, which usually takes at least five years. There are already good data for the biomarkers established in the market (Table 1), but only a few of the novel biomarkers can provide clinical data. Furthermore, distinct restrictions apply to the tests (“targeted patients” in Table 1), which need to be taken into account when comparing the performance of different biomarkers. Currently, histopathological evaluation of needle biopsies is the gold standard and the basis of treatment decisions. Biomarkers should be able to predict the initial biopsy outcome in respect of high-grade disease, i.e., they should have a highly positive predictive value. At present, none of the available biomarkers and tests alone can achieve this goal.
Therefore, because of the low application threshold, PSA monitoring is indispensable at the moment, and should be integrated into routine health examinations of men aged ≥45 years, as recommended in the latest 2018 German S3-guidelines for Prostate Cancer [116]. In case of suspect PSA findings, additional biomarkers should be used to further characterize disease state and safe stratification of patients into treatment groups. Risk calculators should be used for transparent decision-making and to improve the inclusion of the patient.
Author Contributions
Conceptualization, J.N.; Writing—Review & Editing, J.N. and B.Y.
Funding
This research received no external funding.
Acknowledgments
The authors would like to thank Mandy Berndt-Paetz and Vinodh Kumar Adithyaa Arthanareeswaran for critical reading of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Available online: http://globocan.iarc.fr (accessed on 1 July 2018).
- Chen, W.; Zheng, R.; Baade, P.D.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Ervik, M.; Lam, F.; Ferlay, J.; Mery, L.; Soerjomataram, I.; Bray, F. Cancer Today. Lyon, France: International Agency for Research on Cancer; Cancer Today: Lyon, France, 2016; Available online: http://gco.iarc.fr/today (accessed on 28 August 2016).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowrance, W.T.; Murad, M.H.; Oh, W.K.; Jarrard, D.F.; Resnick, M.J.; Cookson, M.S. Castration-Resistant Prostate Cancer: AUA Guideline Amendment 2018. J. Urol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, H.B. American Urological Association (AUA) guideline on prostate cancer detection: Process and rationale. BJU Int. 2013, 112, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Leyten, G.H.; Hessels, D.; Jannink, S.A.; Smit, F.P.; de Jong, H.; Cornel, E.B.; de Reijke, T.M.; Vergunst, H.; Kil, P.; Knipscheer, B.C.; et al. Prospective multicentre evaluation of PCA3 and TMPRSS2-ERG gene fusions as diagnostic and prognostic urinary biomarkers for prostate cancer. Eur. Urol. 2014, 65, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.; Friend, C.; Dreher, A.; Allgar, V.; Macleod, U. The diagnostic test accuracy of rectal examination for prostate cancer diagnosis in symptomatic patients: A systematic review. BMC Fam. Pract. 2018, 19, 79. [Google Scholar] [CrossRef] [PubMed]
- Smeenge, M.; Barentsz, J.; Cosgrove, D.; de la Rosette, J.; de Reijke, T.; Eggener, S.; Frauscher, F.; Kovacs, G.; Matin, S.F.; Mischi, M.; et al. Role of transrectal ultrasonography (TRUS) in focal therapy of prostate cancer: Report from a Consensus Panel. BJU Int. 2012, 110, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Haas, G.P.; Delongchamps, N.B.; Jones, R.F.; Chandan, V.; Serio, A.M.; Vickers, A.J.; Jumbelic, M.; Threatte, G.; Korets, R.; Lilja, H.; et al. Needle biopsies on autopsy prostates: Sensitivity of cancer detection based on true prevalence. J. Natl. Cancer Inst. 2007, 99, 1484–1489. [Google Scholar] [CrossRef] [PubMed]
- Stamey, T.A.; Yang, N.; Hay, A.R.; McNeal, J.E.; Freiha, F.S.; Redwine, E. Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. N. Engl. J. Med. 1987, 317, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.R.; Lubeck, D.P.; Mehta, S.S.; Carroll, P.R. Time trends in clinical risk stratification for prostate cancer: Implications for outcomes (data from CaPSURE). J. Urol. 2003, 170, S21–S27. [Google Scholar] [CrossRef] [PubMed]
- Schröder, F.H.; Hugosson, J.; Roobol, M.J.; Tammela, T.L.; Zappa, M.; Nelen, V.; Kwiatkowski, M.; Lujan, M.; Määttänen, L.; Lilja, H.; et al. Screening and prostate cancer mortality: Results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet 2014, 384, 2027–2035. [Google Scholar] [CrossRef]
- Brawley, O.W. Prostate cancer epidemiology in the United States. World J. Urol. 2012, 30, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Neppl-Huber, C.; Zappa, M.; Coebergh, J.W.; Rapiti, E.; Rachtan, J.; Holleczek, B.; Rosso, S.; Aareleid, T.; Brenner, H.; Gondos, A.; EUNICE Survival Working Group. Changes in incidence, survival and mortality of prostate cancer in Europe and the United States in the PSA era: Additional diagnoses and avoided deaths. Ann. Oncol. 2012, 23, 1325–1334. [Google Scholar] [CrossRef] [PubMed]
- Leidinger, P.; Keller, A.; Milchram, L.; Harz, C.; Hart, M.; Werth, A.; Lenhof, H.P.; Weinhäusel, A.; Keck, B.; Wullich, B.; et al. Combination of Autoantibody Signature with PSA Level Enables a Highly Accurate Blood-Based Differentiation of Prostate Cancer Patients from Patients with Benign Prostatic Hyperplasia. PLoS ONE 2015, 10, e0128235. [Google Scholar] [CrossRef] [PubMed]
- Moyer, V.A.; U.S. Preventive Services Task Force. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2012, 157, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Howrey, B.T.; Kuo, Y.F.; Lin, Y.L.; Goodwin, J.S. The impact of PSA screening on prostate cancer mortality and overdiagnosis of prostate cancer in the United States. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Draisma, G.; Etzioni, R.; Tsodikov, A.; Mariotto, A.; Wever, E.; Gulati, R.; Feuer, E.; de Koning, H. Lead time and overdiagnosis in prostate-specific antigen screening: Importance of methods and context. J. Natl. Cancer Inst. 2009, 101, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Heidegger, I.; Skradski, V.; Steiner, E.; Klocker, H.; Pichler, R.; Pircher, A.; Horninger, W.; Bektic, J. High risk of under-grading and -staging in prostate cancer patients eligible for active surveillance. PLoS ONE 2015, 10, e0115537. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.M.; Pauler, D.K.; Goodman, P.J.; Tangen, C.M.; Lucia, M.S.; Parnes, H.L.; Minasian, L.M.; Ford, L.G.; Lippman, S.M.; Crawford, E.D.; et al. Prevalence of prostate cancer among men with a prostate-specific antigen level < or = 4.0 ng per milliliter. N. Engl. J. Med. 2004, 350, 2239–2246. [Google Scholar] [CrossRef] [PubMed]
- Veltri, R.W.; Miller, M.C.; O’dowd, G.J.; Partin, A.W. Impact of age on total and complexed prostate-specific antigen cutoffs in a contemporary referral series of men with prostate cancer. Urology 2002, 60, 47–52. [Google Scholar] [CrossRef]
- U.S. Preventive Services Task Force. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2008, 149, 185–191. [Google Scholar] [CrossRef]
- Carter, H.B.; Albertsen, P.C.; Barry, M.J.; Etzioni, R.; Freedland, S.J.; Greene, K.L.; Holmberg, L.; Kantoff, P.; Konety, B.R.; Murad, M.H.; et al. Early detection of prostate cancer: AUA Guideline. J. Urol. 2013, 190, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Auffenberg, G.B.; Meeks, J.J. Application of the 2013 American Urological Association early detection of prostate cancer guideline: Who will we miss. World J. Urol. 2014, 32, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Fedewa, S.A.; Ma, J.; Siegel, R.; Lin, C.C.; Brawley, O.; Ward, E.M. Prostate Cancer Incidence and PSA Testing Patterns in Relation to USPSTF Screening Recommendations. JAMA 2015, 314, 2054–2061. [Google Scholar] [CrossRef] [PubMed]
- Vertosick, E.A.; Poon, B.Y.; Vickers, A.J. Relative value of race, family history and prostate specific antigen as indications for early initiation of prostate cancer screening. J. Urol. 2014, 192, 724–728. [Google Scholar] [CrossRef] [PubMed]
- Gershman, B.; Van Houten, H.K.; Herrin, J.; Moreira, D.M.; Kim, S.P.; Shah, N.D.; Karnes, R.J. Impact of Prostate-specific Antigen (PSA) Screening Trials and Revised PSA Screening Guidelines on Rates of Prostate Biopsy and Postbiopsy Complications. Eur. Urol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Alford, A.V.; Brito, J.M.; Yadav, K.K.; Yadav, S.S.; Tewari, A.K.; Renzulli, J. The Use of Biomarkers in Prostate Cancer Screening and Treatment. Rev. Urol. 2017, 19, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Li, Z.Z.; Huang, Y.L.; Song, H.J.; Wang, Y.J. Value of free/total prostate-specific antigen (f/t PSA) ratios for prostate cancer detection in patients with total serum prostate-specific antigen between 4 and 10 ng/mL: A. meta-analysis. Medicine 2018, 97, e0249. [Google Scholar] [CrossRef] [PubMed]
- Carter, H.B.; Pearson, J.D.; Metter, E.J.; Brant, L.J.; Chan, D.W.; Andres, R.; Fozard, J.L.; Walsh, P.C. Longitudinal evaluation of prostate-specific antigen levels in men with and without prostate disease. JAMA 1992, 267, 2215–2220. [Google Scholar] [CrossRef] [PubMed]
- Catalona, W.J.; Smith, D.S.; Ratliff, T.L.; Dodds, K.M.; Coplen, D.E.; Yuan, J.J.; Petros, J.A.; Andriole, G.L. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N. Engl. J. Med. 1991, 324, 1156–1161. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Sanda, M.G.; Broyles, D.L.; Shin, S.S.; Bangma, C.H.; Wei, J.T.; Partin, A.W.; Klee, G.G.; Slawin, K.M.; Marks, L.S.; et al. The prostate health index selectively identifies clinically significant prostate cancer. J. Urol. 2015, 193, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wang, M.; Wang, L.; Adams, T.S.; Tian, Y.; Xu, J. Diagnostic ability of %p2PSA and prostate health index for aggressive prostate cancer: A meta-analysis. Sci. Rep. 2014, 4, 5012. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.J.; Sjoberg, D.D.; Vickers, A.J.; Robinson, M.C.; Kumar, R.; Marsden, L.; Davis, M.; Scardino, P.T.; Donovan, J.; Neal, D.E.; et al. Predicting high-grade cancer at ten-core prostate biopsy using four kallikrein markers measured in blood in the ProtecT study. J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef] [PubMed]
- Schipper, M.; Wang, G.; Giles, N.; Ohrnberger, J. Novel prostate cancer biomarkers derived from autoantibody signatures. Transl. Oncol. 2015, 8, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yu, J.; Sreekumar, A.; Varambally, S.; Shen, R.; Giacherio, D.; Mehra, R.; Montie, J.E.; Pienta, K.J.; Sanda, M.G.; et al. Autoantibody signatures in prostate cancer. N. Engl. J. Med. 2005, 353, 1224–1235. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.S.; Fradet, Y.; Deras, I.L.; Blase, A.; Mathis, J.; Aubin, S.M.; Cancio, A.T.; Desaulniers, M.; Ellis, W.J.; Rittenhouse, H.; et al. PCA3 molecular urine assay for prostate cancer in men undergoing repeat biopsy. Urology 2007, 69, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Gittelman, M.C.; Hertzman, B.; Bailen, J.; Williams, T.; Koziol, I.; Henderson, R.J.; Efros, M.; Bidair, M.; Ward, J.F. PCA3 molecular urine test as a predictor of repeat prostate biopsy outcome in men with previous negative biopsies: A prospective multicenter clinical study. J. Urol. 2013, 190, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.T.; Feng, Z.; Partin, A.W.; Brown, E.; Thompson, I.; Sokoll, L.; Chan, D.W.; Lotan, Y.; Kibel, A.S.; Busby, J.E.; et al. Can urinary PCA3 supplement PSA in the early detection of prostate cancer. J. Clin. Oncol. 2014, 32, 4066–4072. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, J.; Donovan, M.J.; O’Neill, V.; Bentink, S.; Noerholm, M.; Belzer, S.; Skog, J.; Kattan, M.W.; Partin, A.; Andriole, G.; et al. A Novel Urine Exosome Gene Expression Assay to Predict High-grade Prostate Cancer at Initial Biopsy. JAMA Oncol. 2016, 2, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Tomlins, S.A.; Day, J.R.; Lonigro, R.J.; Hovelson, D.H.; Siddiqui, J.; Kunju, L.P.; Dunn, R.L.; Meyer, S.; Hodge, P.; Groskopf, J.; et al. Urine TMPRSS2:ERG Plus PCA3 for Individualized Prostate Cancer Risk Assessment. Eur. Urol. 2016, 70, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Neste, L.; Hendriks, R.J.; Dijkstra, S.; Trooskens, G.; Cornel, E.B.; Jannink, S.A.; de Jong, H.; Hessels, D.; Smit, F.P.; Melchers, W.J.; et al. Detection of High-grade Prostate Cancer Using a Urinary Molecular Biomarker-Based Risk Score. Eur. Urol. 2016, 70, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Grönberg, H.; Adolfsson, J.; Aly, M.; Nordström, T.; Wiklund, P.; Brandberg, Y.; Thompson, J.; Wiklund, F.; Lindberg, J.; Clements, M.; et al. Prostate cancer screening in men aged 50-69 years (STHLM3): A prospective population-based diagnostic study. Lancet Oncol. 2015, 16, 1667–1676. [Google Scholar] [CrossRef]
- Le, B.V.; Griffin, C.R.; Loeb, S.; Carvalhal, G.F.; Kan, D.; Baumann, N.A.; Catalona, W.J. [–2] Proenzyme prostate specific antigen is more accurate than total and free prostate specific antigen in differentiating prostate cancer from benign disease in a prospective prostate cancer screening study. J. Urol. 2010, 183, 1355–1359. [Google Scholar] [CrossRef] [PubMed]
- Filella, X.; Giménez, N. Evaluation of [–2] proPSA and Prostate Health Index (phi) for the detection of prostate cancer: A systematic review and meta-analysis. Clin. Chem. Lab. Med. 2013, 51, 729–739. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Shenoy, B.V.; Tutrone, R.F.; Karsh, L.I.; Saltzstein, D.R.; Harmon, W.J.; Broyles, D.L.; Roddy, T.E.; Lofaro, L.R.; Paoli, C.J.; et al. Clinical utility of the Prostate Health Index (phi) for biopsy decision management in a large group urology practice setting. Prostate Cancer Prostatic Dis. 2018, 21, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Fossati, N.; Buffi, N.M.; Haese, A.; Stephan, C.; Larcher, A.; McNicholas, T.; de la Taille, A.; Freschi, M.; Lughezzani, G.; Abrate, A.; et al. Preoperative Prostate-specific Antigen Isoform p2PSA and Its Derivatives, %p2PSA and Prostate Health Index, Predict Pathologic Outcomes in Patients Undergoing Radical Prostatectomy for Prostate Cancer: Results from a Multicentric European Prospective Study. Eur. Urol. 2015, 68, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Durand, X.; Xylinas, E.; Moutereau, S.; Radulescu, C.; Forgue, A.; Nicolaiew, N.; Terry, S.; Allory, Y.; Loric, S. Prostate cancer antigen 3 score accurately predicts tumour volume and might help in selecting prostate cancer patients for active surveillance. Eur. Urol. 2011, 59, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J. Markers for the early detection of prostate cancer: Some principles for statistical reporting and interpretation. J. Clin. Oncol. 2014, 32, 4033–4034. [Google Scholar] [CrossRef] [PubMed]
- Tilki, D.; Evans, C.P. The changing landscape of advanced and castration resistant prostate cancer: Latest science and revised definitions. Can. J. Urol. 2014, 21, 7–13. [Google Scholar] [PubMed]
- Drake, R.R.; Elschenbroich, S.; Lopez-Perez, O.; Kim, Y.; Ignatchenko, V.; Ignatchenko, A.; Nyalwidhe, J.O.; Basu, G.; Wilkins, C.E.; Gjurich, B.; et al. In-depth proteomic analyses of direct expressed prostatic secretions. J. Proteome Res. 2010, 9, 2109–2116. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Ignatchenko, V.; Yao, C.Q.; Kalatskaya, I.; Nyalwidhe, J.O.; Lance, R.S.; Gramolini, A.O.; Troyer, D.A.; Stein, L.D.; Boutros, P.C.; et al. Identification of differentially expressed proteins in direct expressed prostatic secretions of men with organ-confined versus extracapsular prostate cancer. Mol. Cell. Proteom. 2012, 11, 1870–1884. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, J.; Schiffer, E.; von Wilcke, P.; Bauer, H.W.; Leung, H.; Siwy, J.; Ulrici, W.; Paasch, U.; Horn, L.-C.; Stolzenburg, J.U. Seminal Plasma as a Source of Prostate Cancer Peptide Biomarker Candidates for Detection of Indolent and Advanced Disease. PLoS ONE 2013, 8, e67514. [Google Scholar] [CrossRef] [PubMed]
- Theodorescu, D.; Schiffer, E.; Bauer, H.W.; Douwes, F.; Eichhorn, F.; Polley, R.; Schmidt, T.; Schofer, W.; Zurbig, P.; Good, D.M.; et al. Discovery and validation of urinary biomarkers for prostate cancer. Proteom. Clin. Appl. 2008, 2, 556–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDunn, J.E.; Li, Z.; Adam, K.P.; Neri, B.P.; Wolfert, R.L.; Milburn, M.V.; Lotan, Y.; Wheeler, T.M. Metabolomic signatures of aggressive prostate cancer. Prostate 2013, 73, 1547–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutros, S.; Meyer, T.E.; Fox, S.D.; Issaq, H.J.; Veenstra, T.D.; Huang, W.Y.; Yu, K.; Albanes, D.; Chu, L.W.; Andriole, G.; et al. Prospective evaluation of serum sarcosine and risk of prostate cancer in the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial. Carcinogenesis 2013, 34, 2281–2285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sroka, W.D.; Boughton, B.A.; Reddy, P.; Roessner, U.; Słupski, P.; Jarzemski, P.; Dąbrowska, A.; Markuszewski, M.J.; Marszałł, M.P. Determination of amino acids in urine of patients with prostate cancer and benign prostate growth. Eur. J. Cancer Prev. 2017, 26, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Clos-Garcia, M.; Loizaga-Iriarte, A.; Zuñiga-Garcia, P.; Sánchez-Mosquera, P.; Rosa Cortazar, A.; González, E.; Torrano, V.; Alonso, C.; Pérez-Cormenzana, M.; Ugalde-Olano, A.; et al. Metabolic alterations in urine extracellular vesicles are associated to prostate cancer pathogenesis and progression. J. Extracell. Vesicles 2018, 7, 1470442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, J.A.; Fensom, G.K.; Rinaldi, S.; Scalbert, A.; Appleby, P.N.; Achaintre, D.; Gicquiau, A.; Gunter, M.J.; Ferrari, P.; Kaaks, R.; et al. Pre-diagnostic metabolite concentrations and prostate cancer risk in 1077 cases and 1077 matched controls in the European Prospective Investigation into Cancer and Nutrition. BMC Med. 2017, 15, 122. [Google Scholar] [CrossRef] [PubMed]
- Song, C.J.; Chen, H.; Chen, L.Z.; Ru, G.M.; Guo, J.J.; Ding, Q.N. The potential of microRNAs as human prostate cancer biomarkers: A meta-analysis of related studies. J. Cell. Biochem. 2018, 119, 2763–2786. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.; Baird, A.-M.; Aird, J.; Greene, J.; Kapoor, D.; Gray, S.; McDermott, R.; Finn, S. RNAs as Candidate Diagnostic and Prognostic Markers of Prostate Cancer‚ ÄîFrom Cell Line Models to Liquid Biopsies. Diagnostics 2018, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- Walter, B.A.; Valera, V.A.; Pinto, P.A.; Merino, M.J. Comprehensive microRNA Profiling of Prostate Cancer. J. Cancer 2013, 4, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, A.; Jung, M.; Mollenkopf, H.J.; Wagner, I.; Stephan, C.; Jentzmik, F.; Miller, K.; Lein, M.; Kristiansen, G.; Jung, K. Diagnostic and prognostic implications of microRNA profiling in prostate carcinoma. Int. J. Cancer 2010, 126, 1166–1176. [Google Scholar] [CrossRef] [PubMed]
- Stephan, C.; Jung, M.; Rabenhorst, S.; Kilic, E.; Jung, K. Urinary miR-183 and miR-205 do not surpass PCA3 in urine as predictive markers for prostate biopsy outcome despite their highly dysregulated expression in prostate cancer tissue. Clin. Chem. Lab. Med. 2015, 53, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, N.; Iguchi, H.; Ochiya, T. Circulating microRNA in body fluid: A new potential biomarker for cancer diagnosis and prognosis. Cancer Sci. 2010, 101, 2087–2092. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porzycki, P.; Ciszkowicz, E.; Semik, M.; Tyrka, M. Combination of three miRNA (miR-141, miR-21, and miR-375) as potential diagnostic tool for prostate cancer recognition. Int. Urol. Nephrol. 2018, 50, 1619–1626. [Google Scholar] [CrossRef] [PubMed]
- Tinay, I.; Tan, M.; Gui, B.; Werner, L.; Kibel, A.S.; Jia, L. Functional roles and potential clinical application of miRNA-345-5p in prostate cancer. Prostate 2018, 78, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, M.; Bajo-Santos, C.; Hessvik, N.P.; Lorenz, S.; Fromm, B.; Berge, V.; Sandvig, K.; Linē, A.; Llorente, A. Identification of non-invasive miRNAs biomarkers for prostate cancer by deep sequencing analysis of urinary exosomes. Mol. Cancer 2017, 16, 156. [Google Scholar] [CrossRef] [PubMed]
- Stuopelyte, K.; Daniunaite, K.; Bakavicius, A.; Lazutka, J.R.; Jankevicius, F.; Jarmalaite, S. The utility of urine-circulating miRNAs for detection of prostate cancer. Br. J. Cancer 2016, 115, 707–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihelich, B.L.; Maranville, J.C.; Nolley, R.; Peehl, D.M.; Nonn, L. Elevated serum microRNA levels associate with absence of high-grade prostate cancer in a retrospective cohort. PLoS ONE 2015, 10, e0124245. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.; Hann, S.S. HOTAIR: An Oncogenic Long Non-Coding RNA in Human Cancer. Cell. Physiol. Biochem. 2018, 47, 893–913. [Google Scholar] [CrossRef] [PubMed]
- Huarte, M. The emerging role of lncRNAs in cancer. Nat. Med. 2015, 21, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Rinn, J.L.; Chang, H.Y. Genome regulation by long noncoding RNAs. Annu. Rev. Biochem. 2012, 81, 145–166. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Miao, Z.; Xue, B.; Shan, Y.; Weng, G.; Shen, B. Long Non-coding RNAs in Urologic Malignancies: Functional Roles and Clinical Translation. J. Cancer 2016, 7, 1842–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martens-Uzunova, E.S.; Böttcher, R.; Croce, C.M.; Jenster, G.; Visakorpi, T.; Calin, G.A. Long noncoding RNA in prostate, bladder, and kidney cancer. Eur. Urol. 2014, 65, 1140–1151. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Ding, H.; Li, Y.; Xue, D.; Liu, Y. LncRNA TINCR is associated with clinical progression and serves as tumor suppressive role in prostate cancer. Cancer Manag. Res. 2018, 10, 2799–2807. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ren, S.C.; Shi, X.L.; Liu, Y.W.; Zhu, Y.S.; Jing, T.L.; Wang, F.B.; Chen, R.; Xu, C.L.; Wang, H.Q.; et al. A novel urinary long non-coding RNA transcript improves diagnostic accuracy in patients undergoing prostate biopsy. Prostate 2015, 75, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Mehra, R.; Udager, A.M.; Ahearn, T.U.; Cao, X.; Feng, F.Y.; Loda, M.; Petimar, J.S.; Kantoff, P.; Mucci, L.A.; Chinnaiyan, A.M. Overexpression of the Long Non-coding RNA SChLAP1 Independently Predicts Lethal Prostate Cancer. Eur. Urol. 2016, 70, 549–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Ren, S.; Chen, R.; Lu, J.; Shi, X.; Zhu, Y.; Zhang, W.; Jing, T.; Zhang, C.; Shen, J.; et al. Development and prospective multicenter evaluation of the long noncoding RNA MALAT-1 as a diagnostic urinary biomarker for prostate cancer. Oncotarget 2014, 5, 11091–11102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.; Ding, M.; Xu, K.; Yang, C.; Mao, L.J. Exosomes in diagnosis and therapy of prostate cancer. Oncotarget 2017, 8, 97693–97700. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Yuan, T.; Liang, M.; Du, M.; Xia, S.; Dittmar, R.; Wang, D.; See, W.; Costello, B.A.; Quevedo, F.; et al. Exosomal miR-1290 and miR-375 as prognostic markers in castration-resistant prostate cancer. Eur. Urol. 2015, 67, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Wang, J.; Wang, Y.; Zhu, P.; Liu, X.; Li, N.; Liu, J.; Yu, L.; Wang, W. GRP78 Participates in PCA3-regulated Prostate Cancer Progression. Anticancer Res. 2017, 37, 4303–4310. [Google Scholar] [CrossRef] [PubMed]
- de Kok, J.B.; Verhaegh, G.W.; Roelofs, R.W.; Hessels, D.; Kiemeney, L.A.; Aalders, T.W.; Swinkels, D.W.; Schalken, J.A. DD3(PCA3), a very sensitive and specific marker to detect prostate tumors. Cancer Res. 2002, 62, 2695–2698. [Google Scholar] [PubMed]
- Li, Y.; Luo, H.; Xiao, N.; Duan, J.; Wang, Z.; Wang, S. Long Noncoding RNA SChLAP1 Accelerates the Proliferation and Metastasis of Prostate Cancer via Targeting miR-198 and Promoting the MAPK1 Pathway. Oncol. Res. 2018, 26, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Ding, L.; Wang, L.; Zhao, Y.; Sun, Z.; Karnes, R.J.; Zhang, J.; Huang, H. LncRNA MALAT1 enhances oncogenic activities of EZH2 in castration-resistant prostate cancer. Oncotarget 2015, 6, 41045–41055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorin, M.A.; Verdone, J.E.; van der Toom, E.; Bivalacqua, T.J.; Allaf, M.E.; Pienta, K.J. Circulating tumour cells as biomarkers of prostate, bladder, and kidney cancer. Nat. Rev. Urol. 2016, 14, 90. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Lu, D.; Schreiber, N.A.; Louw, J.; Graf, R.P.; Vargas, H.A.; Johnson, A.; Jendrisak, A.; Bambury, R.; Danila, D.; et al. Association of AR-V7 on Circulating Tumor Cells as a Treatment-Specific Biomarker With Outcomes and Survival in Castration-Resistant Prostate Cancer. JAMA Oncol. 2016, 2, 1441–1449. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Gregory, S.G.; Garcia-Blanco, M.A.; Armstrong, A.J. Using circulating tumor cells to inform on prostate cancer biology and clinical utility. Crit. Rev. Clin. Lab. Sci. 2015, 52, 191–210. [Google Scholar] [CrossRef] [PubMed]
- Khurana, K.K.; Grane, R.; Borden, E.C.; Klein, E.A. Prevalence of circulating tumor cells in localized prostate cancer. Curr. Urol. 2013, 7, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Tommasi, S.; Pilato, B.; Carella, C.; Lasorella, A.; Danza, K.; Vallini, I.; De Summa, S.; Naglieri, E. Standardization of CTC AR-V7 PCR assay and evaluation of its role in castration resistant prostate cancer progression. Prostate 2018. [Google Scholar] [CrossRef] [PubMed]
- Wilbaux, M.; Tod, M.; De Bono, J.; Lorente, D.; Mateo, J.; Freyer, G.; You, B.; Hénin, E. A Joint Model for the Kinetics of CTC Count and PSA Concentration during Treatment in Metastatic Castration-Resistant Prostate Cancer. CPT Pharmacomet. Syst. Pharmacol. 2015, 4, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, D.T.; Sequist, L.V.; Lee, R.J. Circulating tumour cells-monitoring treatment response in prostate cancer. Nat. Rev. Clin. Oncol. 2014, 11, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Albino, G.; Vendittelli, F.; Paolillo, C.; Zuppi, C.; Capoluongo, E. Potential usefulness of CTC detection in follow up of prostate cancer patients. A preliminary report obtained by using Adnagene platform. Arch. Ital. Urol. Androl. 2013, 85, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.P.; Pantel, K.; Tennstedt, P.; Stroelin, P.; Schlomm, T.; Heinzer, H.; Riethdorf, S.; Steuber, T. Limited prognostic value of preoperative circulating tumor cells for early biochemical recurrence in patients with localized prostate cancer. Urol. Oncol. 2016, 34, 235.e11–235.e16. [Google Scholar] [CrossRef] [PubMed]
- Murray, N.P.; Aedo, S.; Fuentealba, C.; Reyes, E. 10 Year Biochemical Failure Free Survival of Men with CD82 Positive Primary Circulating Prostate Cells Treated by Radical Prostatectomy. Asian Pac. J. Cancer Prev. 2018, 19, 1577–1583. [Google Scholar] [CrossRef] [PubMed]
- Strobl, A.N.; Vickers, A.J.; Van Calster, B.; Steyerberg, E.; Leach, R.J.; Thompson, I.M.; Ankerst, D.P. Improving patient prostate cancer risk assessment: Moving from static, globally-applied to dynamic, practice-specific risk calculators. J. Biomed. Inform. 2015, 56, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ankerst, D.P.; Hoefler, J.; Bock, S.; Goodman, P.J.; Vickers, A.; Hernandez, J.; Sokoll, L.J.; Sanda, M.G.; Wei, J.T.; Leach, R.J.; et al. Prostate Cancer Prevention Trial risk calculator 2.0 for the prediction of low- vs. high-grade prostate cancer. Urology 2014, 83, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.M.; Ankerst, D.P.; Chi, C.; Goodman, P.J.; Tangen, C.M.; Lucia, M.S.; Feng, Z.; Parnes, H.L.; Coltman, C.A. Assessing prostate cancer risk: Results from the Prostate Cancer Prevention Trial. J. Natl. Cancer Inst. 2006, 98, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Roobol, M.J.; Verbeek, J.F.M.; van der Kwast, T.; Kümmerlin, I.P.; Kweldam, C.F.; van Leenders, G.J.L.H. Improving the Rotterdam European Randomized Study of Screening for Prostate Cancer Risk Calculator for Initial Prostate Biopsy by Incorporating the 2014 International Society of Urological Pathology Gleason Grading and Cribriform growth. Eur. Urol. 2017, 72, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Yuri, P.; Wangge, G.; Abshari, F.; Satjakoesoemah, A.I.; Perdana, N.R.; Wijaya, C.D.; Tansol, C.; Tigor, A.; Safriadi, F.; Kadar, D.D.; et al. Indonesian prostate cancer risk calculator (IPCRC): An application for predicting prostate cancer risk (a multicenter study). Acta Med. Indones. 2015, 47, 95–103. [Google Scholar] [PubMed]
- Chiu, P.K.; Roobol, M.J.; Nieboer, D.; Teoh, J.Y.; Yuen, S.K.; Hou, S.M.; Yiu, M.K.; Ng, C.F. Adaptation and external validation of the European randomised study of screening for prostate cancer risk calculator for the Chinese population. Prostate Cancer Prostatic Dis. 2017, 20, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.S.; Zhang, N.; Liu, S.H.; Xu, J.F.; Tong, S.J.; Cai, Y.H.; Zhang, L.M.; Bai, P.D.; Hu, M.B.; Jiang, H.W.; et al. The Huashan risk calculators performed better in prediction of prostate cancer in Chinese population: A training study followed by a validation study. Asian J. Androl. 2016, 18, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Xie, L.; Xue, W.; Ye, Z.; Ma, L.; Gao, X.; Ren, S.; Wang, F.; Zhao, L.; Xu, C.; et al. Development and external multicenter validation of Chinese Prostate Cancer Consortium prostate cancer risk calculator for initial prostate biopsy. Urol. Oncol. 2016, 34, 416.e1–416.e7. [Google Scholar] [CrossRef] [PubMed]
- Roehl, K.A.; Antenor, J.A.; Catalona, W.J. Serial biopsy results in prostate cancer screening study. J. Urol. 2002, 167, 2435–2439. [Google Scholar] [CrossRef]
- Seisen, T.; Roudot-Thoraval, F.; Bosset, P.O.; Beaugerie, A.; Allory, Y.; Vordos, D.; Abbou, C.C.; De La Taille, A.; Salomon, L. Predicting the risk of harboring high-grade disease for patients diagnosed with prostate cancer scored as Gleason </= 6 on biopsy cores. World J. Urol. 2015, 33, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Moul, J.W.; Banez, L.L.; Sun, L.; Mouraviev, V.; Xie, D.; Polascik, T.J. Association between percentage of tumor involvement and Gleason score upgrading in low-risk prostate cancer. Med. Oncol. 2012, 29, 3339–3344. [Google Scholar] [CrossRef] [PubMed]
- Emwas, A.-H.M.; Salek, R.M.; Griffin, J.L.; Merzaban, J. NMR-based metabolomics in human disease diagnosis: Applications, limitations, and recommendations. Metabolomics 2013, 9, 1048–1072. [Google Scholar] [CrossRef]
- Kimura, T. East meets west: Ethnic differences in prostate cancer epidemiology between East Asians and Caucasians. Chin. J. Cancer 2012, 31, 421. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Wang, H.K.; Qu, Y.Y.; Ye, D.W. Prostate cancer in East Asia: Evolving trend over the last decade. Asian J. Androl. 2015, 17, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Sterling, W.A.; Weiner, J.; Schreiber, D.; Mehta, K.; Weiss, J.P. The impact of African American race on prostate cancer detection on repeat prostate biopsy in a veteran population. Int. Urol. Nephrol. 2016, 48, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Kallingal, G.J.; Walker, M.R.; Musser, J.E.; Ward, D.E.; McMann, L.P. Impact of race in using PSA velocity to predict for prostate cancer. Mil. Med. 2014, 179, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Su, L.J.; Arab, L.; Steck, S.E.; Fontham, E.T.; Schroeder, J.C.; Bensen, J.T.; Mohler, J.L. Obesity and prostate cancer aggressiveness among African and Caucasian Americans in a population-based study. Cancer Epidemiol. Biomark. Prev. 2011, 20, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, D.K., AWMF). Interdisziplinäre Leitlinie der Qualität S3 zur Früherkennung, Diagnose und Therapie der verschiedenen Stadien des Prostatakarzinoms, Langversion 5.0, 2018, AWMF Registernummer: 043/022OL. 2018. Available online: http://www.leitlinienprogramm-onkolo-gie.de/leitlinien/prostatakarzinom/ (accessed on 15 May 2018).
Figure 1.
Feasibility of liquid biomarker-based diagnostics. The financial burden is coded by colour (green = low, yellow = medium, red = high); at present, advanced analytical methods come with higher high technical requirements and the need for very high analytical expertise; generally, gene expression, genomics, proteomics, and metabolomics require specialized analysis laboratories. In most cases, e.g., for untargeted analyses, standards have not been defined yet; this accelerates the threshold for comprehensive establishment in the clinical routine. For instance, proteomic analyses are still expensive, require high analytical expertise, and are not comprehensively available. On the other hand, proteomic analyses are fairly good and standardized. Comparing metabolic analyses, they require higher expertise than the more standardized proteomics, but are less expensive. The logistical burden grows with the complexity of the clinical and analytical requirements; circle indicates currently well established methods of PCa diagnostics.
Figure 1.
Feasibility of liquid biomarker-based diagnostics. The financial burden is coded by colour (green = low, yellow = medium, red = high); at present, advanced analytical methods come with higher high technical requirements and the need for very high analytical expertise; generally, gene expression, genomics, proteomics, and metabolomics require specialized analysis laboratories. In most cases, e.g., for untargeted analyses, standards have not been defined yet; this accelerates the threshold for comprehensive establishment in the clinical routine. For instance, proteomic analyses are still expensive, require high analytical expertise, and are not comprehensively available. On the other hand, proteomic analyses are fairly good and standardized. Comparing metabolic analyses, they require higher expertise than the more standardized proteomics, but are less expensive. The logistical burden grows with the complexity of the clinical and analytical requirements; circle indicates currently well established methods of PCa diagnostics.


{kind=link}
{kind=link}
Table 1.
PCa biomarker tests for prediction of high-grade PCa (GS ≥ 7).
| Biomarker(s) | Source | Commercial Product | Predict | Avoid Biopsies | Sens. | Spec. | AUC | PPV | NPV | Targeted Patients | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PSA | blood (serum) | Tandem-R® monoclonal immunoradiometric assay (Hybritech Inc., San Diego, CA, USA) | PCa on first biopsy | n.a. | 79% at PSA ≥ 4 ng/mL | 59% at PSA ≥ 4 ng/mL | 0.64 | 40% | 89% | age > 50 years PSA ≥ 4 ng/mL | [33] |
| PSA | blood (serum) | Tandem-R® (Hybritech) | PCa (vs. BPH/Controls) | n.a. | 78% at PSA ≥ 4 ng/mL | 60% (PCa vs. BPH); 94% (PCa vs. Control at PSA ≥ 4 ng/mL | n.r. | n.r. | n.r. | age > 60 years | [32] |
| PSA velocity (0.75 ng/mL/year) | blood (serum) | Tandem-R® (Hybritech) | PCa (vs. BPH/Controls) | n.a. | 72% at PSA ≥ 4 ng/mL | 90% (PCa vs. BPH); 100% PCa vs. Control: at PSA ≥ 4 ng/mL | n.r. | n.r. | n.r. | age >60 years | [32] |
| PSA | blood (serum) | Access Hybritech® | Risk of GS ≥ 7 | n.a. | 90% at PSA ≥4.3 ng/mL | 9% at PSA ≥ 4.4 ng/mL | 0.55 | n.r. | n.r. | age ≥ 50 years PSA 4–10 ng/mL, neg. DRE | [34] |
| fPSA/tPSA | blood (serum) | n.r. | PCa (vs. BPH) | n.a. | 70% (pooled data) | 58% (pooled data) | 0.76 (pooled data) | 41% | 86% (1) | PSA 4.0–10.0 ng/mL | meta-analysis [31] |
| PHI (p2PSA/fPSA × √tPSA) | blood (post-DRE serum) | PHI, prostate health index Beckman Coulter, Atlanta, GA, USA) | Risk of GS ≥ 7 | n.r. | 90% (pooled data) | 17% (pooled data) | 0.67 (pooled data) | n.r. | n.r. | age ≥ 50 years PSA 4–10 ng/mL, neg. DRE | meta-analysis [35] |
| p2PSA/fPSA (%p2PSA) | PHI, prostate health index Beckman Coulter, Atlanta, GA, USA) | Risk of GS ≥ 7 | n.r. | 96% (pooled data) | 9% (pooled data) | 0.54 (pooled data) | n.r. | n.r. | age ≥ 50 years PSA 4–10 ng/mL, neg. DRE | meta-analysis [35] | |
| PHI (p2PSA/ fPSA × √tPSA) | blood (post-DRE serum) | PHI, prostate health index Beckman Coulter, Atlanta, GA, USA) | Risk of GS ≥ 7 | 30.1% | 90% (cutoff 29.8) | 30% (cutoff 29.8) | 0.71 | n.r. | n.r. | age ≥ 50 years PSA 4–10 ng/mL, neg. DRE | [34] |
| intact PSA, free PSA, total PSA, kallikrein-related peptidase 2 (hK2) | blood (post-DRE serum) | 4KScore® Test (OPKO Lab, Nashville, TN, USA) | Risk of GS ≥ 7 | 43% | n.r. | n.r. | 0.82 | n.r. | n.r. | PSA ≥ 3 ng/mL; | [36] |
| expression of 8 auto-antibodies against: CSNK2A2, cestrosomal protein 164 kDa, NK3 homeobox 1, aurora kinase interacting protein 1,5′-UTR BMI1, ARF6, chromosome 3′-UTR region Ropporin/RhoEGF, desmocollin 3 | blood (serum) | Apifiny® (Armune Bioscience, Kalamazoo, MI, USA) | Risk of GS ≥ 7 | n.r. | 60% at PSA > 4 ng/mL [37] | 69% at PSA > 4 ng/mL [37] | 0.69 at PSA > 4 ng/mL [37] | 30% [37] | 89% [37] | PSA ≥ 2.5 ng/mL, initial biopsy | [37,38] |
| prostate cancer gene 3 (PCA3) + PSA mRNA ratio | post-DRE urine | Progensa™ (Gen-Probe Inc., San Diego, CA, USA) | PCa | n.r. | 58% [39] 78% [40] 76% [41] | 72% [39] 57% [40] 52% [41] | 0.68 [39] n.r. [40] 0.80 [41] | n.r. [39] 34% [40] n.r. [41] | n.r. [39] 90% [40] 88% [41] | age ≥ 50 years neg. prior biopsy, repeat biopsy | [39,40,41] |
| exosomes (EV) + (SOC: prostate-specific antigen level, age, race, family history); gene expression (targets revealed): SPDEF, ERG and PCA3 | urine | ExoDx® Prostate IntelliScore urine exosome assay (Exosome Diagnostics, Inc., Waltham, MA, USA) | Risk of GS ≥ 7 | n.r. | 92% | 34% | 0.73 | 36% | 91% | PSA 2–20 ng/mL, initial biopsy | [42] |
| serum PSA + urine PCA3 mRNA + urine TMPRSS2:ERG mRNA | blood (serum); post-DRE urine | Progensa™ (Hologic, Bedford, MA, USA); MiPS test; University of Michigan (MLabs) | Risk of GS ≥ 7 | 35–47% | n.r. | n.r. | 0.77 (PSA + T2:ERG + PCA3 | n.r. | n.r. | elevated PSA (initial biopsy), prior negative biopsy (repeat biopsy) | [43] |
| HOXC6 mRNA + DLX1 mRNA + serum PSA + PSA density + DRE status + age + family history | post-DRE urine | SelectMDx (MDx Health, Irvine, CA, USA) | Risk of GS ≥ 7 | 42% of total; 53% of unne-cessary biopsies | 91% (HOXC6 + DLX1) | 36% (HOXC6 + DLX1) | 0.76 (HOXC6 + DLX1); 0.90 + clin. Para-meters | 28% | 98% | PSA > 4 ng/mL; negative index biopsy | [44] |
| STHLM3 risk-based model: PSA, fPSA, iPSA, hK2, β-microseminoprotein (MSMB), macrophage inhibitory cytokine 1 (MIC1), genetic polymorphisms [232 SNPs], age, family history, previous prostate biopsy, DRE, prostate volume | blood | various | Risk of GS ≥ 7 | 32% biopsies (GS ≥ 7); 44% benign biopsies | n.r. | n.r. | n.r. | n.r. | n.r. | PSA ≥ 3 ng/mL; age 50–69 years; highly selected patients; validation in standard populations needed | [45] |
Abbreviations: sensitivity (sens.); specificity (spec.); receiver-operation-characteristics (ROC) area under the curve (AUC); positive predictive value (PPV); negative predictive value (NPV); benign prostate hyperplasia (BPH); Gleason score (GS); free PSA (fPSA); total PSA (tPSA); not applicable (n.a.); not reported (n.r.). (1) calculated by authors from Table 1 in Huang et al., 2018 [31].
Table 2.
Micro RNAs in prostate cancer diagnosis.
| Reference | Song et al. 2018 [62] | Schaefer et al. 2010 [65] | Walter et al. 2013 [64] | |||
|---|---|---|---|---|---|---|
| Type | Meta-Analysis of 104 Studies | Original Article | Original Article | |||
| Samples | Tissue, Blood, Urine | RPE Frozen Tissue (76 PCa, 79 PCa) | FFPE RPE Tissue (37 PCa) | |||
| Method(s) | Various | miRNA Microarray; 470 miRNAs | PCR Array Profiling | |||
| Measure | Expression in PCa | Expression in PCa | Expr. in GS ≥ 8 vs. GS 6 | |||
| miR-1 ↓ | a | miR-16 ↓ | miR-9 ↑ | i | ||
| miR-18a ↑ | a | miR-31 ↓ | j | miR-27 ↓ | i | |
| miR-21 ↑ | c,l | miR-96 ↑ | e,g,j | miR-30c ↑ | h,l | |
| miR-23b ↓ | a | miR-125b ↓ | k | miR-34 ↑ | i | |
| miR-27b ↓ | a | miR-145 ↓ | miR-92 ↓ | i | ||
| miR-30c ↓ | a,c | miR-149 ↓ | e | miR-96 ↓ | i | |
| miR-31 ↑ | b | miR-181b ↓ | miR-122 ↑ | h,i | ||
| miR-34a ↑ | a | miR-182 ↑ | e | miR-125a ↑ | h | |
| miR-99b ↓ | a | miR-182 * ↑ | miR-125 ↓ | i | ||
| miR-106b ↑ | a | miR-183 ↑ | f | miR-126 ↓ | i | |
| miR-129 ↓ | c | miR-184 ↓ | miR-138 ↑ | i | ||
| miR-139-5p ↓ | a | miR-205 ↓ | e,f,j,k | miR-144 ↑ | i | |
| miR-141 ↑ | a,l | miR-221 ↓ | miR-146b-5p ↑ | h | ||
| miR-145 ↓ | c | miR-222 ↓ | k | miR-148 ↓ | i,m | |
| miR-152 ↓ | a | miR-375 ↑ | e,l,m | miR-181a ↑ | h | |
| miR-182 ↑ | a | miR-181c ↑ | h | |||
| miR-183 ↑ | a | miR-184 ↑ | h,i | |||
| miR-187 ↓ | a | miR-193 ↑ | i | |||
| miR-200a ↑ | a | miR-193b ↑ | h | |||
| miR-200b ↑ | a | miR-198 ↑ | i | |||
| miR-204 ↓ | a | miR-214 ↑ | h | |||
| miR-205 ↓ | a | miR-215 ↑ | i | |||
| miR-224 ↓ | a | miR-222 ↓ | i | |||
| miR-301a ↑ | a | miR-335 ↑ | h,i | |||
| miR-375 ↑ | a,d,l,m | miR-373 ↑ | i | |||
| miR-452 ↓ | a | |||||
| miR-505 ↓ | a | |||||
| let-7c ↓ | a,b,c | |||||
FFPE = formalin-fixed paraffin-embedded; TURP = transurethral resection of the prostate; RPE = radical prostatectomy; a = differentiate PCa from BPH/HC; b = differentiate advanced metastatic from local/primary PCa; c = prediction of poor recurrence free survival; d = worse overall survival; e = AUC of 0.88 combining 5 miRNAs; f = AUC of 0.88 combining two miRNAs; g = can predict biochemical recurrence; h = p < 0.005 in PCa vs. normal epithelium; i = differentiate GS ≥ 8 from GS 6; j = correlation with Gleason score; k = correlation with tumour stage; l = of diagnostic value in serum; m = of diagnostic value in urine; * = indicates reverse miRNA sequence; ↑ = upregulated; ↓ = downregulated.
Table 3.
Long non-coding RNAs (lncRNA) potential biomarkers.
| Name | Function | Diagnostic Value | Reference |
|---|---|---|---|
| PCA3 ↑ (prostate cancer associated 3) | increase of cell proliferation, migration and invasion; inhibition of apoptosis; [85] | predict risk of GS > 7 | [86] |
| TINCR ↓ (Terminal differentiation induced non-coding RNA) | growth inhibition via TRIP13 suppression [79] | not determined | [79] |
| FR0348383 ↑ | unknown | predict PCa-positive biopsy; avoid 52% unnecessary biopsies without missing high-grade PCa | [80] |
| SChLAP1 ↑ (SWI/SNF complex antagonist associated with prostate cancer 1) | increase of cell proliferation, metastasis via downregulation of miRNA-198 and activation of MAPK1 pathway [87] | predict high-risk, lethal PCa; biochemical recurrence after RPE | [81] |
| MALAT1 ↑ (metastasis-associated lung adenocarcinoma transcript 1) | interacts with EZH2, promoting proliferation and invasion [88] | predict PCa-positive biopsy; discriminate between PCa and BPH, PCa and HC | [82] |
RPE = radical prostatectomy; HC = healthy controls; ↑ = upregulated; ↓ = downregulated.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Neuhaus, J.; Yang, B. Liquid Biopsy Potential Biomarkers in Prostate Cancer. Diagnostics 2018, 8, 68. https://doi.org/10.3390/diagnostics8040068
AMA Style
Neuhaus J, Yang B. Liquid Biopsy Potential Biomarkers in Prostate Cancer. Diagnostics. 2018; 8(4):68. https://doi.org/10.3390/diagnostics8040068
Chicago/Turabian StyleNeuhaus, Jochen, and Bo Yang. 2018. "Liquid Biopsy Potential Biomarkers in Prostate Cancer" Diagnostics 8, no. 4: 68. https://doi.org/10.3390/diagnostics8040068
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.