
Risk Factors for Possible Dementia Using the Hopkins Verbal Learning Test and the Mini-Mental State Examination in Shanghai


Abstract
:1. Introduction
- (i)
- a general lack of resources (e.g., a lack of trained staff, time, and financial constraints); and
- (ii)
- high rates of illiteracy and cultural/linguistic differences which can affect the validity of neuropsychological tests.
2. Experimental Section
Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Whole Sample (n = 521) | NCI (n = 406) | MCI (n = 82) | Dementia (n = 33) | p Value |
|---|---|---|---|---|---|
| Age (years, mean ± SD) | 67.5 ± 10.3 | 65.7 ± 9.7 | 71.3 ± 10.2 | 79.8 ± 6.0 | <0.001 |
| Education (below Primary School level %) | 162 (31.1%) | 93 (22.9%) | 38 (46.3%) | 31 (93.9%) | <0.001 |
| Gender (male %) | 237 (45.5%) | 191 (47.0%) | 35 (42.7%) | 11 (33.3%) | NS |
| Occupation (no job or manual %) | 348 (66.8%) | 267 (65.8%) | 48 (58.5%) | 33 (100%) | <0.001 |
| History of Hypertension (yes %) | 119 (22.8%) | 38 (9.4%) | 51 (62.2%) | 30 (90.9%) | <0.001 |
| History of Hyperlipidemia (yes %) | 47 (9.0%) | 15 (3.7%) | 25 (30.5%) | 7 (21.2%) | <0.001 |
| History of Diabetes (yes %) | 33 (6.3%) | 10 (2.5%) | 20 (24.2%) | 3 (9.1%) | <0.001 |
| History of Ischemic Heart Disease (yes %) | 67 (12.9%) | 22 (5.4%) | 34 (41.5%) | 11 (33.3%) | <0.001 |
| Subjective Memory Complaint | 172 (33.0%) | 66 (16.3%) | 76 (92.7%) | 30 (90.9%) | <0.001 |
| Smoking History (yes %) | 129 (24.8%) | 103 (25.4%) | 17 (20.7%) | 9 (27.3%) | NS |
| MMSE Total Score | 26.6 ± 5.2 | 28.2 ± 3.2 | 24.5 ± 3.4 | 12.9 ± 6.6 | <0.001 |
| HVLT Total Score | 22.4 ± 9.0 | 25.4 ± 7.1 | 13.8 ± 5.6 | 6.8 ± 6.1 | <0.001 |

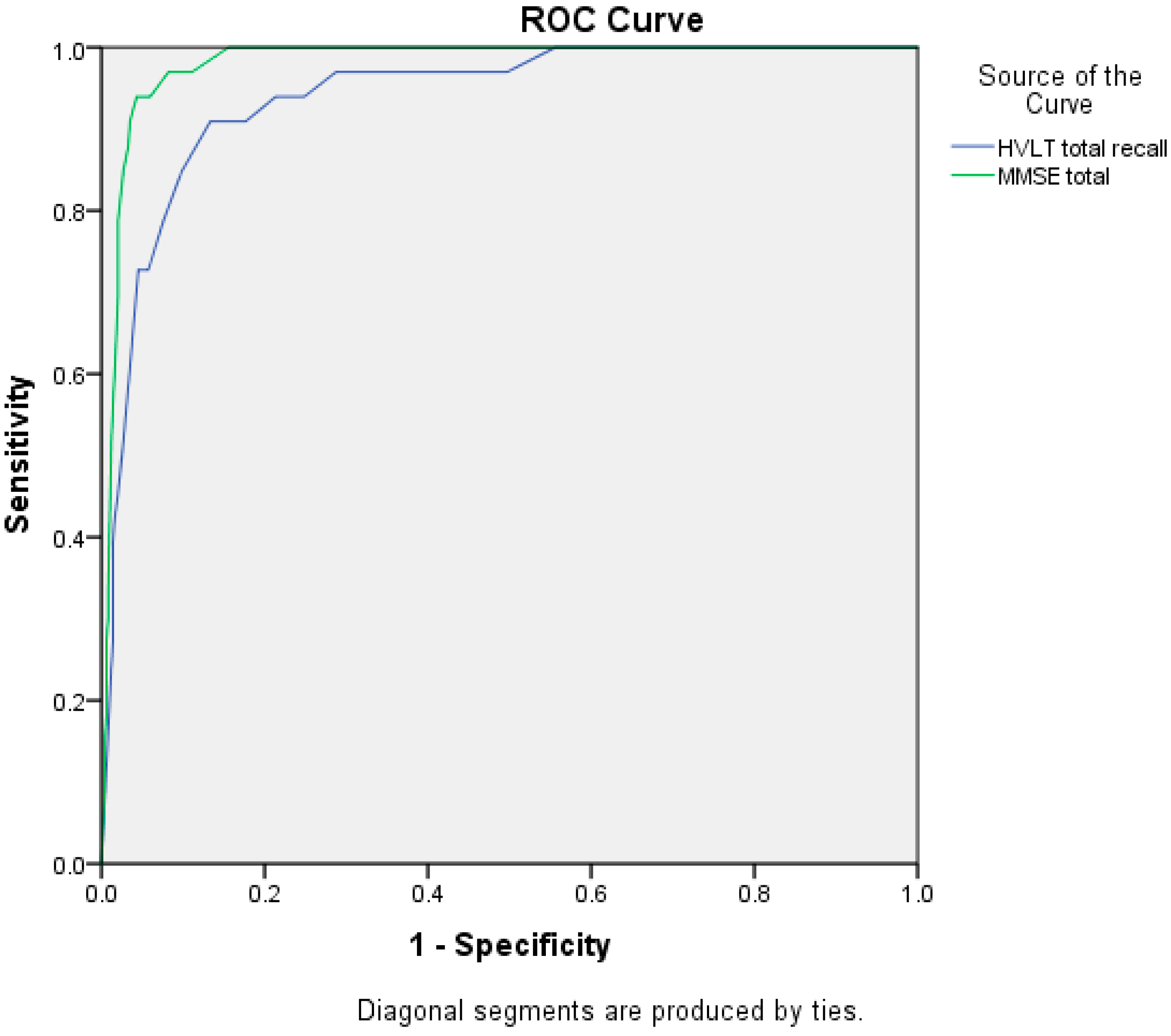
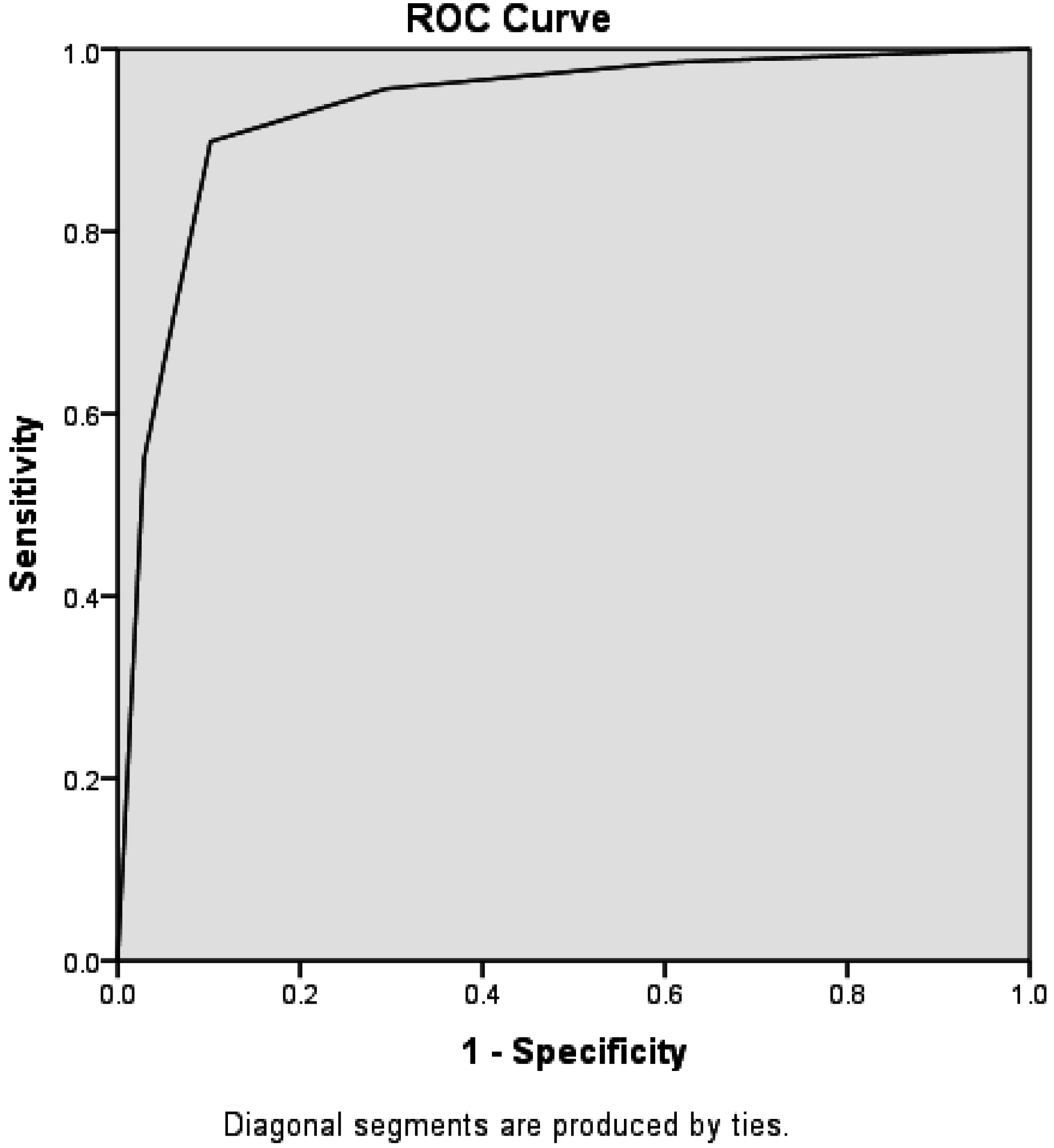
| Tests | AUC (95%CI) | Cut-Off Score | SE | SP |
|---|---|---|---|---|
| HVLT | 0.94 (0.90–0.98) | <19 * | 0.97 | 0.87 |
| <14 | 0.91 | 0.89 | ||
| MMSE | 0.98 (0.97–0.99) | <24 * | 0.97 | 0.92 |
| <22 | 0.94 | 0.96 |
| Groups | DEM (n = 69) | Non-DEM (n = 452) | p Value |
|---|---|---|---|
| Controls (n = 406) | 1 (0.2%) | 404 (99.5%) | <0.001 |
| MCI (n = 82) | 55 (67.1%) | 27 (32.9%) | |
| Dementia (n = 33) | 31 (93.9%) | 2 (6.1%) |
| Dementia Predictors | Odds Ratio (OR) | 95% CI | p Value |
|---|---|---|---|
| Advanced Age (≥68 years) | 4.5 | 1.8–11.2 | 0.001 |
| Low Education (No or Primary Level) | 7.9 | 3.5–17.8 | <0.001 |
| Gender (Female) | 2.4 | 0.9–6.7 | NS |
| History of Hypertension (Yes) | 4.9 | 2.0–11.7 | <0.001 |
| History of Hyperlipidemia (Yes) | 1.4 | 0.5–3.8 | NS |
| History of Diabetes (Yes) | 0.7 | 0.2–2.1 | NS |
| History of Ischemic Heart Disease (Yes) | 0.6 | 0.5–2.9 | NS |
| History of Smoking (Yes) | 0.4 | 0.2–2.0 | NS |
| Subjective Memory Complaint (Yes) | 8.3 | 3.2–21.8 | <0.001 |

4. Discussion

5. Conclusions
Author Contributions
Conflicts of Interest
References
- Bayles, K.A.; Kaszniak, A.W. Communication and Cognition in Normal Aging and Dementia; College-Hill Press: Boston, MA, USA, 1987. [Google Scholar]
- Zhang, M.Y.; Katzman, R.; Salmon, D.; Jin, H.; Cai, G.; Wang, Z.; Qu, G.; Grant, I.; Yu, E.; Levy, P.; et al. The prevalence of dementia and Alzheimer’s disease in Shanghai, China: Impact of age, gender, and education. Ann. Neurol. 1990, 27, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Llibre Rodriguez, J.J.; Ferri, C.P.; Acosta, D.; Guerra, M.; Huang, Y.; Jacob, K.S.; Krishnamoorthy, E.S.; Salas, A.; Sosa, A.L.; Acosta, I.; et al. Prevalence of dementia in Latin America, India, and China: A population-based cross-sectional survey. Lancet 2008, 372, 464–474. [Google Scholar] [CrossRef]
- Zhang, Z.X.; Zahner, G.E.; Román, G.C.; Liu, J.; Hong, Z.; Qu, Q.M.; Liu, X.H.; Zhang, X.J.; Zhou, B.; Wu, C.B.; et al. Dementia subtypes in China: Prevalence in Beijing, Xian, Shanghai, and Chengdu. Arch. Neurol. 2005, 62, 447–453. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Publishing Inc.: Arlington, VA, USA, 1994. [Google Scholar]
- Hogervorst, E.; Combrinck, M.; Lapuerta, P.; Rue, J.; Swales, K.; Budge, M. The Hopkins Verbal Learning Test and screening for dementia. Dement. Geriatr. Cogn. Disord. 2002, 13, 13–20. [Google Scholar] [CrossRef] [PubMed]
- De Jager, C.A.; Hogervorst, E.; Combrink, M.; Budge, M.M. Sensitivity and specificity of neuropsychological tests for mild cognitive impairment, vascular cognitive impairment and Alzheimer’s disease. Psychol. Med. 2003, 33, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Tian, J.; Wei, M.; Miao, Y.; Wang, Y. The utility of the Hopkins Verbal Learning Test (Chinese version) for screening dementia and mild cognitive impairment in a Chinese Population. BMC Neurol. 2012, 8, 360–361. [Google Scholar] [CrossRef]
- Xu, X.; Xiao, S.; Rahardjo, T.B.; Hogervorst, E. Tofu intake is associated with poor cognitive performance among community-dwelling elderly in China. J. Alzheimers Dis. 2015, 4, 669–675. [Google Scholar]
- Xu, X.; Rahardjo, T.B.; Xiao, S.F.; Hogervorst, E. The Hopkins Verbal Learning Test and detection of MCI and mild dementia: A literature review. J. Alzheimers Dis. Parkinsonism 2014, 4, 166. [Google Scholar] [CrossRef]
- Barnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011, 10, 819–828. [Google Scholar] [CrossRef]
- Kivipelto, M.; Ngandu, T.; Laatikainen, T.; Winblad, B.; Soininen, H.; Tuomilehto, J. Risk score for the prediction of dementia risk in 20 years among middle aged people: A longitudinal, population-based study. Lancet Neurol. 2006, 5, 735–741. [Google Scholar] [CrossRef]
- Shah, K.; Qureshi, S.U.; Johnson, M.; Parikh, N.; Schulz, P.E.; Kunik, M.E. Does use of antihypertensive drugs affect the incidence or progression of dementia? A systematic review. Am. J. Geriatr. Pharmacother. 2009, 9, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J. Drug treatment as a cause of falls in old age. Drugs Aging 1991, 14, 289–302. [Google Scholar] [CrossRef]
- Diamond, M.C.; Krech, D.; Rosenzweig, M.R. The effects of an enriched environment on the histology of the rat cerebral cortex of environmentally enriched rats. J. Comp. Neurol. 1964, 131, 357–364. [Google Scholar] [CrossRef]
- Ip, E.Y.; Giza, C.C.; Griesbach, G.S.; Hovda, D.A. Effects of enriched environment and fluid percussion injury on dendritic arborization within the cerebral cortex of the developing rat. J. Neurotrauma 2002, 19, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Clifford, A.; Yesufu, U.A.; Edwards, A.; Bandelow, S.; Hogervorst, E. Maintaining cognitive health in elderly women: An invited review. Aging Health 2009, 5, 655–670. [Google Scholar] [CrossRef]
- Kramer, A.F.; Hahn, S.; Cohen, N.J.; Banich, M.T.; McAuley, E.; Harrison, C.R.; Chason, J.; Vakil, E.; Bardell, L.; Boileau, R.A.; et al. Ageing, fitness and neurocognitive function. Nature 1999, 400, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Heyn, P.C.; Abreu, B.C.; Ottenbacher, K.J. The effects of exercise training on elderly persons with cognitive impairment and dementia: A meta-analysis. Arch. Phys. Med. Rehabil. 2004, 85, 1694–1704. [Google Scholar] [CrossRef] [PubMed]
- Dustman, R.E.; Ruhling, R.O.; Russell, E.M.; Shearer, D.E.; Bonekat, H.W.; Shigeoka, J.W.; Wood, J.S.; Bradford, D.C. Aerobic exercise training and improved neuropsychological function of older individuals. Neurobiol. Aging 1984, 5, 35–42. [Google Scholar] [CrossRef]
- Hogervorst, E.; Clifford, A.; Stock, J.; Xin, X.; Bandelow, S. Exercise to prevent cognitive decline and Alzheimer’s disease: For whom, when, what, and (most importantly) how much? J. Alzheimers Dis. Parkinsonism 2012, 2, e117. [Google Scholar] [CrossRef]
- Stock, J. Physical Activity and Cognitive Ability in Older Adults: The Role of Psychosocial Factors. Ph.D. Thesis, Loughborough University, Loughborough, UK, April 2014. [Google Scholar]
- Schmand, B.; Jonker, C.; Hooijer, C.; Lindeboom, J. Subjective memory complaints may announce dementia. Neurology 1996, 46, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Van Oijen, M.; de Jong, F.J.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M. Subjective memory complaints, education, and risk of Alzheimer’s disease. Alzheimers Dement. 2007, 3, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlager, N.T.; Flicker, L.; Vasikaran, S.; Leedman, P.; Almeida, O.P. Subjective memory complaints with and without objective memory impairment: Relationship with risk factors for dementia. Am. J. Geriatr. Psychiatry 2005, 13, 731–734. [Google Scholar] [CrossRef] [PubMed]
- Schrijnemaekers, A.M.; de Jager, C.A.; Hogervorst, E.; Budge, M.M. Cases with mild cognitive impairment and Alzheimer’s disease fail to benefit from repeated exposure to episodic memory tests as compared with controls. J. Clin. Exp. Neuropsychol. 2006, 28, 438–455. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, X.; Xiao, S.; Rahardjo, T.B.; Hogervorst, E. Risk Factors for Possible Dementia Using the Hopkins Verbal Learning Test and the Mini-Mental State Examination in Shanghai. Diagnostics 2015, 5, 487-496. https://doi.org/10.3390/diagnostics5040487
Xu X, Xiao S, Rahardjo TB, Hogervorst E. Risk Factors for Possible Dementia Using the Hopkins Verbal Learning Test and the Mini-Mental State Examination in Shanghai. Diagnostics. 2015; 5(4):487-496. https://doi.org/10.3390/diagnostics5040487
Chicago/Turabian StyleXu, Xin, Shifu Xiao, Tri Budi Rahardjo, and Eef Hogervorst. 2015. "Risk Factors for Possible Dementia Using the Hopkins Verbal Learning Test and the Mini-Mental State Examination in Shanghai" Diagnostics 5, no. 4: 487-496. https://doi.org/10.3390/diagnostics5040487