
Calcinosis in Rheumatic Disease Is Still an Unmet Need: A Retrospective Single-Center Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Treatment and Outcomes
2.4. Data Analysis
3. Results
3.1. Patient Characteristics
3.1.1. General Description of the Study Lot
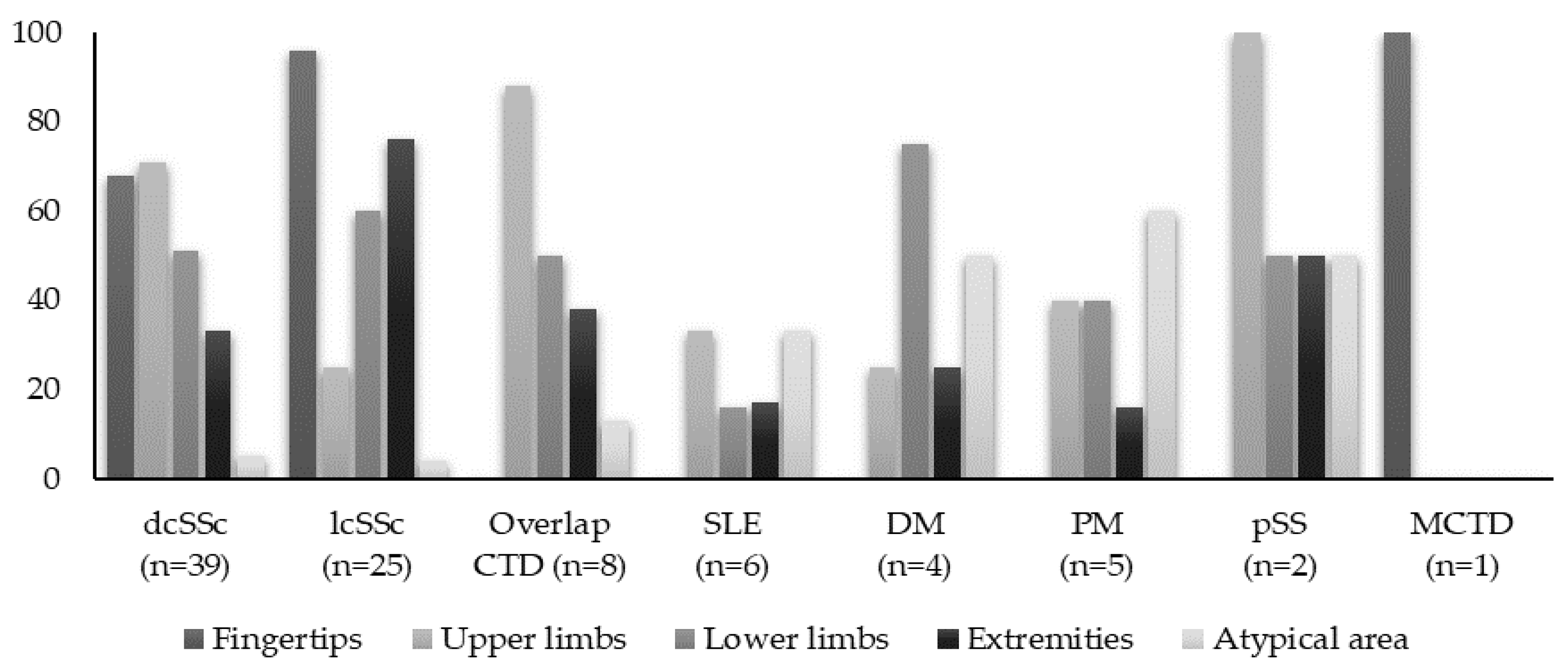
3.1.2. Anatomic Distribution of Calcinosis
3.2. Correlation Analyses between Different IMRD and Subcutaneous Calcinosis
3.3. Treatment Strategies and Outcomes in Patients with IMRD—Related Calcinosis
3.3.1. Treatment of Calcinosis Cutis
3.3.2. Outcomes and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Le, C.; Bedocs, P.M. Calcinosis Cutis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Elahmar, H.; Feldman, B.M.; Johnson, S.R. Management of Calcinosis Cutis in Rheumatic Diseases. J. Rheumatol. 2022, 49, 980–989. [Google Scholar] [CrossRef]
- Baron, M.; Pope, J.; Robinson, D.; Jones, N.; Khalidi, N.; Docherty, P.; Kaminska, E.; Masetto, A.; Sutton, E.; Mathieu, J.-P.; et al. Calcinosis is associated with digital ischaemia in systemic sclerosis—A longitudinal study. Rheumatology 2016, 55, 2148–2155. [Google Scholar] [CrossRef]
- Avouac, J.; Mogavero, G.; Guerini, H.; Drapé, J.L.; Mathieu, A.; Kahan, A.; Allanore, Y. Predictive factors of hand radiographic lesions in systemic sclerosis: A prospective study. Ann. Rheum. Dis. 2011, 70, 630–633. [Google Scholar] [CrossRef]
- Davies, C.A.; Jeziorska, M.; Freemont, A.J.; Herrick, A.L. The differential expression of VEGF, VEGFR-2, and GLUT-1 proteins in disease subtypes of systemic sclerosis. Hum. Pathol. 2006, 37, 190–197. [Google Scholar] [CrossRef]
- Jiang, S.W.; Petty, A.J.; Nicholas, M.W. Innate Immunity in Calcinosis Cutis. Immuno 2022, 2, 443–459. [Google Scholar] [CrossRef]
- Gunawardena, H.; Betteridge, Z.E.; McHugh, N.J. Myositis-specific autoantibodies: Their clinical and pathogenic significance in disease expression. Rheumatology 2009, 48, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.A.; Jeziorska, M.; Freemont, A.J.; Herrick, A.L. Expression of osteonectin and matrix Gla protein in scleroderma patients with and without calcinosis. Rheumatology 2006, 45, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Wetter, D.A. Calcinosis Cutis Occurring in Association with Autoimmune Connective Tissue Disease: The Mayo Clinic Experience with 78 Patients, 1996–2009. Arch. Dermatol. 2012, 148, 455. [Google Scholar] [CrossRef] [PubMed]
- Chander, S.; Gordon, P. Soft tissue and subcutaneous calcification in connective tissue diseases. Curr. Opin. Rheumatol. 2012, 24, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Achebe, I.; Mbachi, C.; Asotibe, J.C.; Paintsil, I. Dystrophic Calcinosis Cutis in Systemic Lupus Erythematosus. Cureus 2020, 12, e8727. [Google Scholar] [CrossRef] [PubMed]
- Davuluri, S.; Duvvuri, B.; Lood, C.; Faghihi-Kashani, S.; Chung, L. Calcinosis in dermatomyositis: Origins and possible therapeutic avenues. Best Pract. Res. Clin. Rheumatol. 2022, 36, 101768. [Google Scholar] [CrossRef]
- Gutierrez, A., Jr.; Wetter, D.A. Calcinosis cutis in autoimmune connective tissue diseases: Calcinosis cutis and connective tissue disease. Dermatol. Ther. 2012, 25, 195–206. [Google Scholar] [CrossRef]
- Yamamoto, A.; Morita, A.; Shintani, Y.; Sakakibara, S.; Tsuji, T. Localized Linear Scleroderma with Cutaneous Calcinosis. J. Dermatol. 2002, 29, 112–114. [Google Scholar] [CrossRef]
- Mormile, I.; Mosella, F.; Turco, P.; Napolitano, F.; De Paulis, A.; Rossi, F.W. Calcinosis Cutis and Calciphylaxis in Autoimmune Connective Tissue Diseases. Vaccines 2023, 11, 898. [Google Scholar] [CrossRef]
- Valenzuela, A.; Stevens, K.; Chung, M.P.; Rodriguez-Reyna, T.S.; Proudman, S.; Baron, M.; Castelino, F.V.; Hsu, V.; Green, L.; Galdo, F.D.; et al. Change in calcinosis over 1 year using the scleroderma clinical trials consortium radiologic scoring system for calcinosis of the hands in patients with systemic sclerosis. Semin. Arthritis Rheum. 2022, 53, 151980. [Google Scholar] [CrossRef]
- Chung, L.; Valenzuela, A.; Fiorentino, D.; Stevens, K.; Li, S.; Harris, J.; Hutchinson, C.; Assassi, S.; Beretta, L.; Lakshminarayanan, S.; et al. Validation of a Novel Radiographic Scoring System for Calcinosis Affecting the Hands of Patients with Systemic Sclerosis: Novel Radiographic Scoring System for Calcinosis. Arthritis Care Res. 2015, 67, 425–430. [Google Scholar] [CrossRef]
- Saketkoo, L.A.; Gordon, J.K.; Fligelstone, K.; Mawdsley, A.; Chaudhry, H.A.; Valenzuela, A.; Christensen, A.; Khalique, S.M.; Jensen, K.; Weinmann, S.C.; et al. Patient Experience of Systemic Sclerosis–Related Calcinosis. Rheum. Dis. Clin. N. Am. 2023, 49, 463–481. [Google Scholar] [CrossRef]
- López-Sundh, A.E.; Quintana-Sancho, A.; Durán-Vian, C.; Reguero-DelCura, L.; Corrales-Martínez, A.F.; Gómez-Fernández, C.; González-López, M.A. Clinical and ultrasound response to intralesional sodium thiosulfate for the treatment of calcinosis cutis in the setting of systemic sclerosis. A case-based review. Clin. Rheumatol. 2021, 40, 2985–2989. [Google Scholar] [CrossRef] [PubMed]
- Starnoni, M.; Pappalardo, M.; Spinella, A.; Testoni, S.; Lattanzi, M.; Feminò, R.; De Santis, G.; Salvarani, C.; Giuggioli, D. Systemic sclerosis cutaneous expression: Management of skin fibrosis and digital ulcers. Ann. Med. Surg. 2021, 71, 102984. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, I.E.; Tjärnlund, A.; Bottai, M.; Werth, V.P.; Pilkington, C.; Visser, M.D.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann. Rheum. Dis. 2017, 76, 1955–1964. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef]
- Van Den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American college of rheumatology/European league against rheumatism collaborative initiative. Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef]
- Kasukawa, R.; Sharp, G.C. Mixed Connective Tissue Disease and Anti-nuclear Antibodies. In Proceedings of the International Symposium on Mixed Connective Tissue Disease and Anti-nuclear Antibodies, Tokyo, Japan, 29–30 August 1986; Excerpta Medica. Elsevier Science Pub. Co.: New York, NY, USA, 1987. ISBN 978-0-444-80868-4. [Google Scholar]
- Boulman, N.; Slobodin, G.; Rozenbaum, M.; Rosner, I. Calcinosis in Rheumatic Diseases. Semin. Arthritis Rheum. 2005, 34, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Domínguez, M.P.; García-Collinot, G.; Saavedra, M.A.; Medina, G.; Carranza-Muleiro, R.A.; Vera-Lastra, O.L.; Jara, L.J. Clinical, biochemical, and radiological characterization of the calcinosis in a cohort of Mexican patients with systemic sclerosis. Clin. Rheumatol. 2017, 36, 111–117. [Google Scholar] [CrossRef]
- Nowaczyk, J.; Zawistowski, M.; Fiedor, P. Local, non-systemic, and minimally invasive therapies for calcinosis cutis: A systematic review. Arch. Dermatol. Res. 2022, 314, 515–525. [Google Scholar] [CrossRef]
- Bartoli, F.; Fiori, G.; Braschi, F.; Amanzi, L.; Bruni, C.; Blagojevic, J.; Bellando-Randone, S.; Cometi, L.; De Souza Mueller, C.; Guiducci, S.; et al. Calcinosis in systemic sclerosis: Subsets, distribution and complications. Rheumatology 2016, 55, 1610–1614. [Google Scholar] [CrossRef]
- Valenzuela, A.; Chung, L. Subcutaneous calcinosis: Is it different between systemic sclerosis and dermatomyositis? J. Scleroderma Relat. Disord. 2022, 7, 7–23. [Google Scholar] [CrossRef]
- Smith, S.; Hanson, J. Extensive Dystrophic Calcinosis Cutis: A Severe Complication of Polymyositis/Systemic Sclerosis Overlap Syndrome. JCR J. Clin. Rheumatol. 2017, 23, 445. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, S.W.; Chung, W.T. Dystrophic calcinosis in a patient with overlap syndrome (scleroderma and rheumatoid arthritis) treated by leflunomide: A case report. Medicine 2018, 97, e13319. [Google Scholar] [CrossRef]
- Okada, J.; Nomura, M.; Shirataka, M.; Kondo, H. Prevalence of soft tissue calcifications in patients with SLE and effects of alfacarcidol. Lupus 1999, 8, 456–461. [Google Scholar] [CrossRef]
- Valenzuela, A.; Baron, M.; Rodriguez-Reyna, T.S.; Proudman, S.; Khanna, D.; Young, A.; Hinchcliff, M.; Steen, V.; Gordon, J.; Hsu, V.; et al. Calcinosis is associated with ischemic manifestations and increased disability in patients with systemic sclerosis. Semin. Arthritis Rheum. 2020, 50, 891–896. [Google Scholar] [CrossRef]
- Muktabhant, C.; Thammaroj, P.; Chowchuen, P.; Foocharoen, C. Prevalence and clinical association with calcinosis cutis in early systemic sclerosis. Mod. Rheumatol. 2021, 31, 1113–1119. [Google Scholar] [CrossRef]
- Pai, S.; Hsu, V. Are there risk factors for scleroderma-related calcinosis? Mod. Rheumatol. 2018, 28, 518–522. [Google Scholar] [CrossRef]
- Richardson, C.; Perin, J.; Zeger, S.; Wigley, F.M.; Hummers, L.K.; Casciola-Rosen, L.; Rosen, A.; Shah, A.A. Cumulative disease damage and anti-PM/Scl antibodies are associated with a heavy burden of calcinosis in systemic sclerosis. Rheumatology 2022, 62, 3636–3643. [Google Scholar] [CrossRef]
- Host, L.V.; Campochiaro, C.; Afonso, A.; Nihtyanova, S.I.; Denton, C.P.; Ong, V.H. High proton pump inhibitor exposure increases risk of calcinosis in systemic sclerosis. Rheumatology 2021, 60, 849–854. [Google Scholar] [CrossRef]
- Calcinosis in Poly-Dermatomyositis: Clinical and Laboratory Predictors and Treatment Options. Available online: https://www.clinexprheumatol.org/abstract.asp?a=10801 (accessed on 6 October 2023).
- Hoeltzel, M.F.; Oberle, E.J.; Robinson, A.B.; Agarwal, A.; Rider, L.G. The Presentation, Assessment, Pathogenesis, and Treatment of Calcinosis in Juvenile Dermatomyositis. Curr. Rheumatol. Rep. 2014, 16, 467. [Google Scholar] [CrossRef]
- D’Aoust, J.; Hudson, M.; Tatibouet, S.; Wick, J.; the Canadian Scleroderma Research Group; Mahler, M.; Baron, M.; Fritzler, M.J. Clinical and Serologic Correlates of Anti-PM/Scl Antibodies in Systemic Sclerosis: A Multicenter Study of 763 Patients: Anti-PM-1α Antibodies and SSc Clinical Phenotype. Arthritis Rheumatol. 2014, 66, 1608–1615. [Google Scholar] [CrossRef]
- Bauer, E.; Fauny, M.; Tanguy, M.; Albuisson, E.; Mandry, D.; Huttin, O.; Chabot, F.; Deibener, J.; Chary-Valckenaere, I.; Loeuille, D. Relationship between calcifications and structural lesions on hand radiography and axial calcifications on CT-scan: A retrospective study in systemic sclerosis. Medicine 2020, 99, e22443. [Google Scholar] [CrossRef]
- Jinnin, M. ‘Narrow-sense’ and ‘broad-sense’ vascular abnormalities of systemic sclerosis. Immunol. Med. 2020, 43, 107–114. [Google Scholar] [CrossRef]
- Manning, J.B.; Marjanovic, E.; Moore, T.L.; Dinsdale, G.; Wilkinson, S.; Dickinson, M.R.; Herrick, A.L.; Murray, A.K. A pilot study of cutaneous oxygenation and perfusion in systemic sclerosis–related digital calcinosis. Rheumatology 2020, 59, 3109–3111. [Google Scholar] [CrossRef] [PubMed]
- Lescoat, A.; Yelnik, C.M.; Coiffier, G.; Wargny, M.; Lamotte, C.; Cazalets, C.; Belhomme, N.; Ballerie, A.; Hatron, P.; Launay, D.; et al. Ulnar Artery Occlusion and Severity Markers of Vasculopathy in Systemic Sclerosis: A Multicenter Cross-Sectional Study. Arthritis Rheumatol. 2019, 71, 983–990. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| dcSSc (n = 39) | lcSSc (n = 25) | Overlap CTD a (n = 8) | SLE (n = 6) | PM (n = 5) | DM (n = 4) | pSS (n = 2) | MCTD (n = 1) | p | |
|---|---|---|---|---|---|---|---|---|---|
| Demographics | |||||||||
| Female | 37 (49) | 19 (79) | 8 (100) | 6 (100) | 5 (100) | 4 (100) | 2 (100) | 1 (100) | 0.58 |
| Age, (IQR), years | 50 (36–60) | 54 (28–73) | 39 (24–55) | 29 (20–48) | 39 (24–55) | 44 (37–68) | 46 (35–67) | 39 | 0.18 |
| Time to onset of calcinosis, (IQR), months | 13 (2–43) | 90 (0–372) | 128 (2–312) | 24 (1–55) | 108 (18–546) | 48 (11–109) | 258 (228–742) | 75 | <0.001 |
| Total observation period, (IQR), years | 0.09 | ||||||||
| Raynaud’s | 31 (79) | 23 (92) | 8 (100) | 1 (16) | - | - | - | 1 (100) | 0.54 |
| Telangiectasias | 18 (46) | 23 (92) | 7 (88) | - | - | - | - | 1 (100) | 0.49 |
| Digital ulcers | 20 (51) | 16 (64) | 5 (62) | - | - | - | - | - | 0.03 |
| Articular involvement | 22 (56) | 24 (96) | 6 (75) | 3 (50) | 2 (40) | 1 (25) | 1 (50) | 1 (100) | 0.06 |
| Muscle involvement | 14 (36) | 16 (64) | 7 (88) | 2 (33) | 5 (100) | 4 (100) | 2 (100) | - | 0.10 |
| GIT involvement | 18 (46) | 21 (84) | 4 (50) | 1 (16) | 1 (20) | 1 (25) | - | 1 (100) | 0.003 |
| Severe GIT disease | 14 (35) | 4 (16) | 2 (25) | - | - | - | - | 1 (100) | <0.001 |
| Peripheric arterial disease | 25 (64) | 20 (80) | 3 (37) | - | - | - | - | - | 0.01 |
| Severe peripheral arterial disease | 19 (48) | 9 (36) | 3 (37) | - | - | - | - | - | 0.02 |
| ILD | 26 (66) | 15 (60) | 5 (63) | - | 2 (40) | - | - | 1 (100) | 0.28 |
| PAH | 13 (33) | 11 (44) | 2 (25) | - | - | - | - | 1 (100) | 0.17 |
| Myocardial disease | 14 (36) | 6 (24) | 1 (12) | - | - | - | - | 1 (100) | 0.21 |
| Chronic kidney disease | 4 (10) | 2 (8) | 1 (12) | 1 (17) | - | - | 1 (50) | - | 0.15 |
| Osteoporosis | 12 (31) | 9 (36) | 2 (25) | 1 (17) | 2 (40) | - | - | - | 0.81 |
| Arterial hypertension | 12 (31) | 13 (52) | 1 (12) | - | 1 (20) | 1 (25) | 1 (50) | - | 0.25 |
| Diabetes | 3 (8) | 2 (8) | - | - | - | 1 (25) | - | - | 0.10 |
| Dyslipidemia | 8 (20) | 8 (32) | 3 (37) | - | - | 1 (25) | 1 (50) | - | 0.11 |
| Malignancy | 4 (10) | 1 (4) | 1 (12) | - | 1 (20) | - | - | - | 0.35 |
| Multivariate Analysis | ||
|---|---|---|
| Variable | OR (95% CI) | p-Value |
| Age | 0.99 (0.97–1.01) | 0.88 |
| Female | 1.83 (1.12–2.95) | 0.02 |
| Disease duration | 1.04 (1.00–1.08) | 0.001 |
| ATA | 1.00 (0.59–1.68) | 0.98 |
| ACA | 1.42 (0.84–2.40) | 0.18 |
| Anti-Pm/Scl | 7.58 (1.13–9.17) | 0.004 |
| mRSS | 1.01 (0.97–1.05) | 0.56 |
| Tendon friction rubs | 0.60 (0.22–1.66) | 0.33 |
| Synovitis | 0.82 (0.42–1.60) | 0.56 |
| Muscle weakness | 0.81 (0.45–1.47) | 0.50 |
| Upper GI symptoms | 0.90 (0.52–1.56) | 0.71 |
| Lower GI symptoms | 1.44 (0.81–2.53) | 0.20 |
| Severe GI disease | 1.27 (1.02–14.76) | 0.001 |
| PAH | 1.96 (0.93–4.41) | 0.07 |
| DU | 1.36 (1.06–3.03) | 0.004 |
| EScSG AI | 1.09 (1.01–1.46) | 0.05 |
| Subcutaneous Lesions Size | ||||
|---|---|---|---|---|
| Variable | ≤1 cm | ≥4 cm | ||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| ATA | 1.90 (1.06–5.57) | 0.04 | 1.42 (0.50–4.01) | 0.50 |
| ACA | 0.41 (0.14–1.19) | 0.10 | 0.66 (0.22–1.98) | 0.46 |
| Anti-Pm/Scl | 0.42 (0.13–1.28) | 0.12 | 2.15 (1.70–6.57) | 0.01 |
| mRSS | 1.02 (0.94–1.11) | 0.51 | 0.98 (0.91–1.06) | 0.72 |
| Tendon friction rubs | 1.06 (0.36–3.11) | 0.91 | 2.05 (0.53–7.97) | 0.29 |
| Synovitis | 1.45 (1.05–3.40) | 0.02 | 1.00 (0.31–3.23) | 0.99 |
| Muscle weakness | 0.65 (0.22–1.89) | 0.43 | 3.12 (1.04–9.31) | 0.04 |
| Upper GI symptoms | 0.89 (0.25–3.13) | 0.86 | 0.83 (0.25–2.72) | 0.76 |
| Lower GI symptoms | 1.72 (0.34–8.61) | 0.50 | 1.54 (0.41–5.71) | 0.51 |
| Severe GI disease | 1.43 (0.41–4.94) | 0.57 | 0.92 (0.28–2.96) | 0.89 |
| Peripheral arterial disease | 2.38 (0.61–9.17) | 0.20 | 1.48 (0.43–5.11) | 0.53 |
| Severe peripheral arterial disease | 0.55 (0.09–3.28) | 0.51 | 1.48 (1.03–5.11) | 0.007 |
| Systemic arterial hypertension | 1.60 (0.62–4.11) | 0.32 | 1.83 (1.29–2.37) | <0.001 |
| PAH | 1.06 (0.36–3.11) | 0.91 | 1.01 (0.98–1.04) | 0.46 |
| ILD | 2.13 (1.77–6.92) | 0.01 | 0.39 (0.13–1.17) | 0.09 |
| DU | 2.44 (1.83–7.10) | 0.02 | 0.83 (0.29–2.37) | 0.73 |
| Malignancy | 1.02 (0.97–1.09) | 0.34 | 1.01 (1.00–3.23) | 0.01 |
| EScSG AI | 1.37 (0.46–4.04) | 0.56 | 2.06 (1.68–6.24) | 0.02 |
| Multivariate Analysis | ||
|---|---|---|
| Variable | OR (95% CI) | p Value |
| Raynaud’s phenomenon | 6.79 (2.63–9.31) | 0.06 |
| DU | 3.68 (1.39–9.74) | 0.009 |
| Severe GI disease | 2.95 (1.88–9.86) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nita, C.; Groseanu, L.; Opris, D.; Predeteanu, D.; Bojinca, V.; Berghea, F.; Vlad, V.; Abobului, M.; Constantinescu, C.; Negru, M.; et al. Calcinosis in Rheumatic Disease Is Still an Unmet Need: A Retrospective Single-Center Study. Diagnostics 2024, 14, 637. https://doi.org/10.3390/diagnostics14060637
Nita C, Groseanu L, Opris D, Predeteanu D, Bojinca V, Berghea F, Vlad V, Abobului M, Constantinescu C, Negru M, et al. Calcinosis in Rheumatic Disease Is Still an Unmet Need: A Retrospective Single-Center Study. Diagnostics. 2024; 14(6):637. https://doi.org/10.3390/diagnostics14060637
Chicago/Turabian StyleNita, Cristina, Laura Groseanu, Daniela Opris, Denisa Predeteanu, Violeta Bojinca, Florian Berghea, Violeta Vlad, Mihai Abobului, Cosmin Constantinescu, Magdalena Negru, and et al. 2024. "Calcinosis in Rheumatic Disease Is Still an Unmet Need: A Retrospective Single-Center Study" Diagnostics 14, no. 6: 637. https://doi.org/10.3390/diagnostics14060637