
New Immunohistochemical Markers for Pleural Mesothelioma Subtyping
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohorts
2.2. IHC Analysis and Scoring
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Different Immunohistochemical Expression among Subtypes
3.3. Score and Cut-Off Selection for Subtype Discrimination: Training Cohort
3.4. Validation Cohort
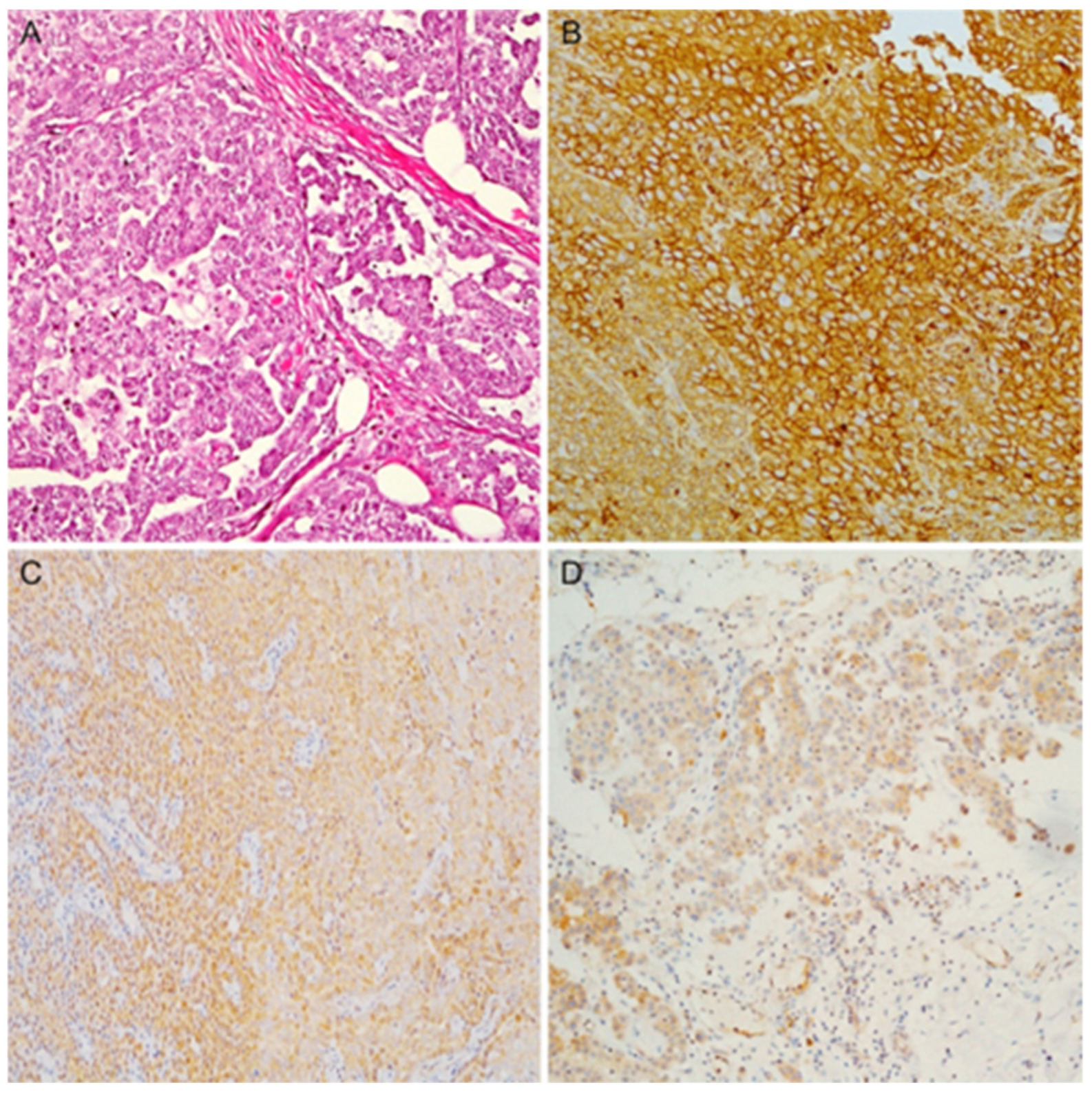
3.5. Epithelioid PMs: IHC and Histological Features
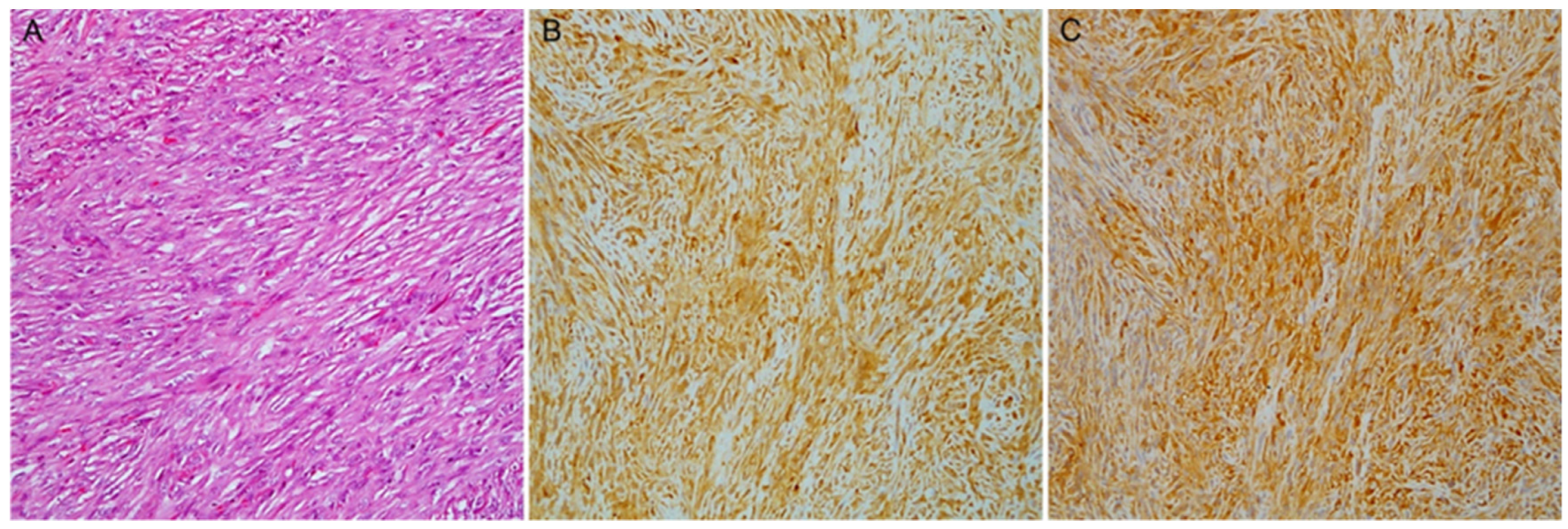
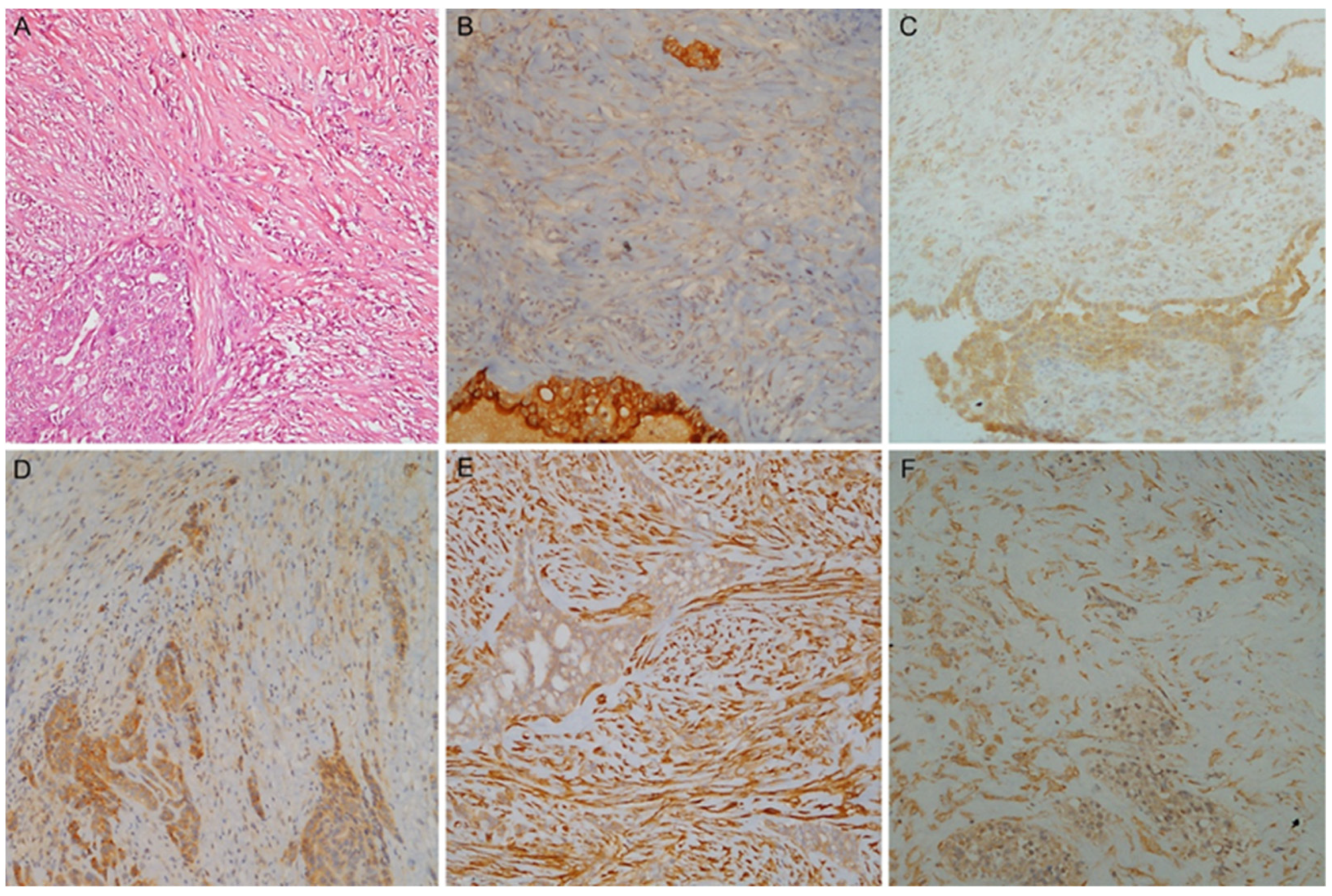
3.6. Biphasic PMs: IHC and Discrimination between Components
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sauter, J.B.R.; Dacic, S.; Gill, R.R. Thoracic Tumours, 5th ed.; WHO Classification of Tumours Editorial Board, Ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2021; Volume 5, pp. 204–219. [Google Scholar]
- Brims, F. Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma. Cancers 2021, 13, 4194. [Google Scholar] [CrossRef]
- Husain, A.N.; Colby, T.V.; Ordonez, N.G.; Allen, T.C.; Attanoos, R.L.; Beasley, M.B.; Butnor, K.J.; Chirieac, L.R.; Churg, A.M.; Dacic, S.; et al. Guidelines for Pathologic Diagnosis of Malignant Mesothelioma 2017 Update of the Consensus Statement From the International Mesothelioma Interest Group. Arch. Pathol. Lab. Med. 2018, 142, 89–108. [Google Scholar] [CrossRef]
- Hjerpe, A.; Abd-Own, S.; Dobra, K. Cytopathologic Diagnosis of Epithelioid and Mixed-Type Malignant Mesothelioma: Ten Years of Clinical Experience in Relation to International Guidelines. Arch. Pathol. Lab. Med. 2018, 142, 893–901. [Google Scholar] [CrossRef]
- Verma, V.; Ahern, C.A.; Berlind, C.G.; Lindsay, W.D.; Shabason, J.; Sharma, S.; Culligan, M.J.; Grover, S.; Friedberg, J.S.; Simone, C.B., 2nd. Survival by Histologic Subtype of Malignant Pleural Mesothelioma and the Impact of Surgical Resection on Overall Survival. Clin. Lung Cancer 2018, 19, e901–e912. [Google Scholar] [CrossRef]
- Nelson, D.B.; Rice, D.C.; Niu, J.; Atay, S.; Vaporciyan, A.A.; Antonoff, M.; Hofstetter, W.L.; Walsh, G.L.; Swisher, S.G.; Roth, J.A.; et al. Long-Term Survival Outcomes of Cancer-Directed Surgery for Malignant Pleural Mesothelioma: Propensity Score Matching Analysis. J. Clin. Oncol. 2017, 35, 3354–3362. [Google Scholar] [CrossRef]
- Hung, Y.P.; Chirieac, L.R. Pathology of Malignant Pleural Mesothelioma. Thorac. Surg. Clin. 2020, 30, 367–382. [Google Scholar] [CrossRef]
- Chirieac, L.R.; Hung, Y.P.; Foo, W.C.; Hofer, M.D.; VanderLaan, P.A.; Richards, W.G.; Sugarbaker, D.J.; Bueno, R. Diagnostic value of biopsy sampling in predicting histology in patients with diffuse malignant pleural mesothelioma. Cancer 2019, 125, 4164–4171. [Google Scholar] [CrossRef]
- Klebe, S.; Brownlee, N.A.; Mahar, A.; Burchette, J.L.; Sporn, T.A.; Vollmer, R.T.; Roggli, V.L. Sarcomatoid mesothelioma: A clinical-pathologic correlation of 326 cases. Mod. Pathol. 2010, 23, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Bueno, R.; Stawiski, E.W.; Goldstein, L.D.; Durinck, S.; De Rienzo, A.; Modrusan, Z.; Gnad, F.; Nguyen, T.T.; Jaiswal, B.S.; Chirieac, L.R.; et al. Comprehensive genomic analysis of malignant pleural mesothelioma identifies recurrent mutations, gene fusions and splicing alterations. Nat. Genet. 2016, 48, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Alcala, N.; Mangiante, L.; Le-Stang, N.; Gustafson, C.E.; Boyault, S.; Damiola, F.; Alcala, K.; Brevet, M.; Thivolet-Bejui, F.; Blanc-Fournier, C.; et al. Redefining malignant pleural mesothelioma types as a continuum uncovers immune-vascular interactions. eBioMedicine 2019, 48, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Bruno, R.; Poma, A.M.; Ali, G.; Distefano, C.; Proietti, A.; Chella, A.; Lucchi, M.; Melfi, F.; Franco, R.; Fontanini, G. Gene Expression Analysis of Biphasic Pleural Mesothelioma: New Potential Diagnostic and Prognostic Markers. Diagnostics 2022, 12, 674. [Google Scholar] [CrossRef] [PubMed]
- Vizcaya, D.; Farahmand, B.; Walter, A.O.; Kneip, C.; Johrens, K.; Tukiainen, M.; Schmitz, A.A. Prognosis of patients with malignant mesothelioma by expression of programmed cell death 1 ligand 1 and mesothelin in a contemporary cohort in Finland. Cancer Treat. Res. Commun. 2020, 25, 100260. [Google Scholar] [CrossRef]
- Inaguma, S.; Wang, Z.; Lasota, J.; Onda, M.; Czapiewski, P.; Langfort, R.; Rys, J.; Szpor, J.; Waloszczyk, P.; Okon, K.; et al. Comprehensive immunohistochemical study of mesothelin (MSLN) using different monoclonal antibodies 5B2 and MN-1 in 1562 tumors with evaluation of its prognostic value in malignant pleural mesothelioma. Oncotarget 2017, 8, 26744–26754. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Higashi, T.; Ozeki, K.; Higashi, A.Y.; Sugimoto, K.; Mine, H.; Takagi, H.; Ozaki, Y.; Muto, S.; Okabe, N.; et al. CLDN15 is a novel diagnostic marker for malignant pleural mesothelioma. Sci. Rep. 2021, 11, 12554. [Google Scholar] [CrossRef] [PubMed]
- Sidi, R.; Pasello, G.; Opitz, I.; Soltermann, A.; Tutic, M.; Rehrauer, H.; Weder, W.; Stahel, R.A.; Felley-Bosco, E. Induction of senescence markers after neo-adjuvant chemotherapy of malignant pleural mesothelioma and association with clinical outcome: An exploratory analysis. Eur. J. Cancer 2011, 47, 326–332. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Akerley, W.; Bazhenova, L.A.; Borghaei, H.; Camidge, D.R.; Cheney, R.T.; Chirieac, L.R.; D’Amico, T.A.; Dilling, T.; et al. NCCN Guidelines Insights: Malignant Pleural Mesothelioma, Version 3.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 825–836. [Google Scholar] [CrossRef]
- Capkova, L.; Koubkova, L.; Kodet, R. Expression of carbonic anhydrase IX (CAIX) in malignant mesothelioma. An immunohistochemical and immunocytochemical study. Neoplasma 2014, 61, 161–169. [Google Scholar] [CrossRef]
- Prabhakaran, S.; Hocking, A.; Kim, C.; Hussey, M.; Klebe, S. The potential utility of GATA binding protein 3 for diagnosis of malignant pleural mesotheliomas. Hum. Pathol. 2020, 105, 1–8. [Google Scholar] [CrossRef]
- Kadota, K.; Villena-Vargas, J.; Nitadori, J.; Sima, C.S.; Jones, D.R.; Travis, W.D.; Adusumilli, P.S. Tumoral CD10 expression correlates with aggressive histology and prognosis in patients with malignant pleural mesothelioma. Ann. Surg. Oncol. 2015, 22, 3136–3143. [Google Scholar] [CrossRef]
- Pasello, G.; Urso, L.; Mencoboni, M.; Grosso, F.; Ceresoli, G.L.; Lunardi, F.; Vuljan, S.E.; Bertorelle, R.; Sacchetto, V.; Ciminale, V.; et al. MDM2 and HIF1alpha expression levels in different histologic subtypes of malignant pleural mesothelioma: Correlation with pathological and clinical data. Oncotarget 2015, 6, 42053–42066. [Google Scholar] [CrossRef]
- Chu, G.J.; Linton, A.; Kao, S.; Klebe, S.; Adelstein, S.; Yeo, D.; Rasko, J.E.J.; Cooper, W.A. High mesothelin expression by immunohistochemistry predicts improved survival in pleural mesothelioma. Histopathology 2023, 83, 202–210. [Google Scholar] [CrossRef]
- Sandeck, H.P.; Roe, O.D.; Kjaerheim, K.; Willen, H.; Larsson, E. Re-evaluation of histological diagnoses of malignant mesothelioma by immunohistochemistry. Diagn. Pathol. 2010, 5, 47. [Google Scholar] [CrossRef]
- Kindler, H.L.; Novello, S.; Bearz, A.; Ceresoli, G.L.; Aerts, J.; Spicer, J.; Taylor, P.; Nackaerts, K.; Greystoke, A.; Jennens, R.; et al. Anetumab ravtansine versus vinorelbine in patients with relapsed, mesothelin-positive malignant pleural mesothelioma (ARCS-M): A randomised, open-label phase 2 trial. Lancet Oncol. 2022, 23, 540–552. [Google Scholar] [CrossRef]
- Ordonez, N.G. Mesothelioma with signet-ring cell features: Report of 23 cases. Mod. Pathol. 2013, 26, 370–384. [Google Scholar] [CrossRef] [PubMed]
- Hager, T.; Borchert, S.; Wessolly, M.; Mathilakathu, A.; Mairinger, E.; Kollmeier, J.; Mairinger, T.; Hegedus, B.; Greimelmaier, K.; Wohlschlaeger, J.; et al. One Third of Malignant Pleural Mesothelioma Shows High Immunohistochemical Expression of MSLN or CXCR4 Which Indicates Potent Candidates for Endo-Radiotherapy. Int. J. Mol. Sci. 2023, 24, 6356. [Google Scholar] [CrossRef] [PubMed]
- Weidemann, S.; Gagelmann, P.; Gorbokon, N.; Lennartz, M.; Menz, A.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Blessin, N.C.; Fraune, C.; et al. Mesothelin Expression in Human Tumors: A Tissue Microarray Study on 12,679 Tumors. Biomedicines 2021, 9, 397. [Google Scholar] [CrossRef]
- Tan, K.; Kajino, K.; Momose, S.; Masaoka, A.; Sasahara, K.; Shiomi, K.; Izumi, H.; Abe, M.; Ohtsuji, N.; Wang, T.; et al. Mesothelin (MSLN) promoter is hypomethylated in malignant mesothelioma, but its expression is not associated with methylation status of the promoter. Hum. Pathol. 2010, 41, 1330–1338. [Google Scholar] [CrossRef]
- Zhang, D.; Sun, B.; Zhao, X.; Sun, H.; An, J.; Lin, X.; Zhu, D.; Zhao, X.; Wang, X.; Liu, F.; et al. Twist1 accelerates tumour vasculogenic mimicry by inhibiting Claudin15 expression in triple-negative breast cancer. J. Cell Mol. Med. 2020, 24, 7163–7174. [Google Scholar] [CrossRef] [PubMed]
- Tabaries, S.; Annis, M.G.; Hsu, B.E.; Tam, C.E.; Savage, P.; Park, M.; Siegel, P.M. Lyn modulates Claudin-2 expression and is a therapeutic target for breast cancer liver metastasis. Oncotarget 2015, 6, 9476–9487. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Li, Y.; Zhang, R.; Chen, J.; Feng, X.; Duan, Y. Low CFB expression is independently associated with poor overall and disease-free survival in patients with lung adenocarcinoma. Oncol. Lett. 2021, 21, 478. [Google Scholar] [CrossRef]
- Shimazaki, R.; Takano, S.; Satoh, M.; Takada, M.; Miyahara, Y.; Sasaki, K.; Yoshitomi, H.; Kagawa, S.; Furukawa, K.; Takayashiki, T.; et al. Complement factor B regulates cellular senescence and is associated with poor prognosis in pancreatic cancer. Cell Oncol. 2021, 44, 937–950. [Google Scholar] [CrossRef] [PubMed]
- Milanovic, M.; Fan, D.N.Y.; Belenki, D.; Dabritz, J.H.M.; Zhao, Z.; Yu, Y.; Dorr, J.R.; Dimitrova, L.; Lenze, D.; Monteiro Barbosa, I.A.; et al. Senescence-associated reprogramming promotes cancer stemness. Nature 2018, 553, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Dou, Z.; Berger, S.L. Senescence Elicits Stemness: A Surprising Mechanism for Cancer Relapse. Cell Metab. 2018, 27, 710–711. [Google Scholar] [CrossRef]
- Markl, B.; Kazik, M.; Harbeck, N.; Jakubowicz, E.; Hoffmann, R.; Jung, T.; Steinfeld, D.; Schenkirsch, G.; Schlimok, G.; Oruzio, D. Impact of uPA/PAI-1 and disseminated cytokeratin-positive cells in breast cancer. BMC Cancer 2019, 19, 692. [Google Scholar] [CrossRef]
- Tian, B.; Chen, X.; Zhang, H.; Li, X.; Wang, J.; Han, W.; Zhang, L.Y.; Fu, L.; Li, Y.; Nie, C.; et al. Urokinase plasminogen activator secreted by cancer-associated fibroblasts induces tumor progression via PI3K/AKT and ERK signaling in esophageal squamous cell carcinoma. Oncotarget 2017, 8, 42300–42313. [Google Scholar] [CrossRef]
- Brungs, D.; Chen, J.; Aghmesheh, M.; Vine, K.L.; Becker, T.M.; Carolan, M.G.; Ranson, M. The urokinase plasminogen activation system in gastroesophageal cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 23099–23109. [Google Scholar] [CrossRef]
- Lin, X.; Lin, B.W.; Chen, X.L.; Zhang, B.L.; Xiao, X.J.; Shi, J.S.; Lin, J.D.; Chen, X. PAI-1/PIAS3/Stat3/miR-34a forms a positive feedback loop to promote EMT-mediated metastasis through Stat3 signaling in Non-small cell lung cancer. Biochem. Biophys. Res. Commun. 2017, 493, 1464–1470. [Google Scholar] [CrossRef]
- Takayama, Y.; Hattori, N.; Hamada, H.; Masuda, T.; Omori, K.; Akita, S.; Iwamoto, H.; Fujitaka, K.; Kohno, N. Inhibition of PAI-1 Limits Tumor Angiogenesis Regardless of Angiogenic Stimuli in Malignant Pleural Mesothelioma. Cancer Res. 2016, 76, 3285–3294. [Google Scholar] [CrossRef]
- Li, D.; Zhang, Y.; Li, Z.; Wang, X.; Qu, X.; Liu, Y. Activated Pak4 expression correlates with poor prognosis in human gastric cancer patients. Tumour Biol. 2015, 36, 9431–9436. [Google Scholar] [CrossRef]
- Cai, S.; Ye, Z.; Wang, X.; Pan, Y.; Weng, Y.; Lao, S.; Wei, H.; Li, L. Overexpression of P21-activated kinase 4 is associated with poor prognosis in non-small cell lung cancer and promotes migration and invasion. J. Exp. Clin. Cancer Res. 2015, 34, 48. [Google Scholar] [CrossRef]
- Begum, A.; Imoto, I.; Kozaki, K.; Tsuda, H.; Suzuki, E.; Amagasa, T.; Inazawa, J. Identification of PAK4 as a putative target gene for amplification within 19q13.12-q13.2 in oral squamous-cell carcinoma. Cancer Sci. 2009, 100, 1908–1916. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yang, Y.; Liu, Y.; Liu, H.; Zhang, W.; Xu, L.; Zhu, Y.; Xu, J. p21-Activated kinase 4 predicts early recurrence and poor survival in patients with nonmetastatic clear cell renal cell carcinoma. Urol. Oncol. 2015, 33, 205.e13–205.e21. [Google Scholar] [CrossRef] [PubMed]
- Song, B.; Wang, W.; Zheng, Y.; Yang, J.; Xu, Z. P21-activated kinase 1 and 4 were associated with colorectal cancer metastasis and infiltration. J. Surg. Res. 2015, 196, 130–135. [Google Scholar] [CrossRef]
- Park, S.; Kim, J.W.; Kim, H.; Kim, J.W.; Kim, Y.J.; Lee, K.W.; Kim, J.H.; Kim, J.H.; Hwang, J.H.; Choi, Y.R.; et al. Prognostic value of p21-activated kinase 4 in resected pancreatic cancer. APMIS 2017, 125, 699–707. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Training Cohort (n = 73) | Validation Cohort (n = 30) |
| Age, years, median (range) | 71 (40–85) | 75 (54–87) |
| Sex, male, n (%) | 58 (79.5) | 25 (83.3) |
| Mesothelioma Subtype | ||
| Epithelioid, n (%) | 31 (42.5) | 11 (36.7) |
| Biphasic, n (%) | 25 (34.2) | 11 (36.7) |
| Sarcomatoid, n (%) | 17 (23.3) | 8 (26.6) |
| Epithelioid subtype (n = 42) | Training Cohort (n = 31) | Validation Cohort (n = 11) |
| High grade, n (%) | 12 (38.7) | 3 (27.3) |
| Mitosis number score | ||
| 1 (≤1 mitosis/2 mm2) | 11 (35.5) | 5 (45.4) |
| 2 (2–4 mitoses/2 mm2) | 15 (48.4) | 3 (27.3) |
| 3 (≥5 mitoses/2 mm2) | 5 (16.1) | 3 (27.3) |
| Nuclear atypia score | ||
| 1 | 8 (25.8) | 3 (27.3) |
| 2 | 17 (54.8) | 5 (45.4) |
| 3 | 6 (19.4) | 3 (27.3) |
| Necrosis presence | 13 (41.9) | 4 (36.4) |
| Scores | CFB Median (IQR) | Mesothelin Median (IQR) | Claudin-15 Median (IQR) | PAI1 Median (IQR) | PAK4 Median (IQR) | |
|---|---|---|---|---|---|---|
| ES | TPS H-score | 70 (55–90) 120 (55–180) | 92.5 (81.25–95) 270 (190–285) | 85 (70–95) 190 (130–210) | 60 (50–80) 120 (82.5–170) | 70 (52.5–82.5) 120 (85–160) |
| BS | TPS H-score | 60 (30–70) 80 (40–120) | 50 (30–70) 117.5 (60–187.5) | 70 (60–75) 150 (130–195) | 85 (80–90) 210 (160–270) | 80 (70–90) 210 (180–240) |
| SS | TPS H-score | 10 (5–20) 10 (5–20) | 0 (0–10) 0 (0–15) | 35 (30–60) 60 (35–80) | 90 (80–95) 210 (190–255) | 70 (65–90) 160 (110–195) |
| ES vs. BS p-value | TPS H-score | 0.04 0.05 | <0.0001 <0.0001 | 0.0006 0.17 | 0.001 <0.0001 | 0.05 <0.0001 |
| ES vs. SS p-value | TPS H-score | <0.0001 <0.0001 | <0.0001 <0.0001 | <0.0001 <0.0001 | <0.0001 <0.0001 | 0.23 0.04 |
| BS vs. SS p-value | TPS H-score | 0.0003 0.0001 | 0.0001 <0.0001 | 0.004 <0.0001 | 0.09 0.23 | 0.25 0.03 |
| Training Cohort | |||||
| Mesothelin | Claudin-15 | CFB | PAI1 | PAK4 | |
| Cut-off | 67.5% | 77.5% | 65% | 72.5% | 62.5% |
| AUC | 0.97 (0.93–0.99) | 0.85 (0.75–0.93) | 0.76 (0.64–0.87) | 0.79 (0.67–0.89) | 0.60 (0.47–0.73) |
| Sensitivity | 0.88 (0.76–0.98) | 0.88 (0.57–1) | 0.86 (0.55–1) | 0.88 (0.62–0.98) | 0.86 (0.43–0.98) |
| Specificity | 1 (0.94–1) | 0.71 (0.51–0.94) | 0.61 (0.32–0.90) | 0.65 (0.42–0.84) | 0.42 (0.23–0.81) |
| Accuracy | 0.93 (0.86–0.97) | 0.81 (0.70–0.89) | 0.75 (0.66–0.82) | 0.77 (0.67–0.85) | 0.67 (0.58–0.77) |
| NPV | 0.86 (0.76–0.97) | 0.83 (0.61–1) | 0.76 (0.57–1) | 0.79 (0.60–0.95) | 0.70 (0.50–0.89) |
| PPV | 1 (0.95–1) | 0.80 (0.72–0.94) | 0.76 (0.67–0.90) | 0.76 (0.68–0.87) | 0.67 (0.61–0.77) |
| Validation Cohort | |||||
| Mesothelin | Claudin-15 | CFB | PAI1 | PAK4 | |
| AUC * | 0.98 (0.92–1) | 0.84 (0.66–0.97) | 0.80 (0.59–0.97) | NA | 0.75 (0.57–0.90) |
| Sensitivity * | 0.79 (0.58–0.95) | 0.84 (0.68–1) | 0.89 (0.74–1) | NA | 0.84 (0.68–1) |
| Specificity * | 0.91 (0.73–1) | 0.73 (0.45–1) | 0.64 (0.36–0.91) | NA | 0.36 (0.09–0.64) |
| Accuracy * | 0.83 (0.70–0.93) | 0.80 (0.63–0.93) | 0.80 (0.67–0.93) | NA | 0.67 (0.53–0.80) |
| NPV * | 0.71 (0.56–0.92) | 0.73 (0.50–1) | 0.78 (0.55–1) | NA | 0.57 (0.25–1) |
| PPV * | 0.94 (0.81–1) | 0.84 (0.71–1) | 0.81 (0.70–0.95) | NA | 0.70 (0.60–0.81) |
| Best Cut-Off on Validation Cohort | |||||
| 87.5% | 75% | 47.5% | 65% | 77.5% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Stefano, I.; Alì, G.; Poma, A.M.; Bruno, R.; Proietti, A.; Niccoli, C.; Zirafa, C.C.; Melfi, F.; Mastromarino, M.G.; Lucchi, M.; et al. New Immunohistochemical Markers for Pleural Mesothelioma Subtyping. Diagnostics 2023, 13, 2945. https://doi.org/10.3390/diagnostics13182945
Di Stefano I, Alì G, Poma AM, Bruno R, Proietti A, Niccoli C, Zirafa CC, Melfi F, Mastromarino MG, Lucchi M, et al. New Immunohistochemical Markers for Pleural Mesothelioma Subtyping. Diagnostics. 2023; 13(18):2945. https://doi.org/10.3390/diagnostics13182945
Chicago/Turabian StyleDi Stefano, Iosè, Greta Alì, Anello Marcello Poma, Rossella Bruno, Agnese Proietti, Cristina Niccoli, Carmelina Cristina Zirafa, Franca Melfi, Maria Giovanna Mastromarino, Marco Lucchi, and et al. 2023. "New Immunohistochemical Markers for Pleural Mesothelioma Subtyping" Diagnostics 13, no. 18: 2945. https://doi.org/10.3390/diagnostics13182945