
Application of Ultrasound Scores (Subjective Assessment, Simple Rules Risk Assessment, ADNEX Model, O-RADS) to Adnexal Masses of Difficult Classification
 , , , and
, , , and
Abstract
:Featured Application
Abstract
1. Introduction
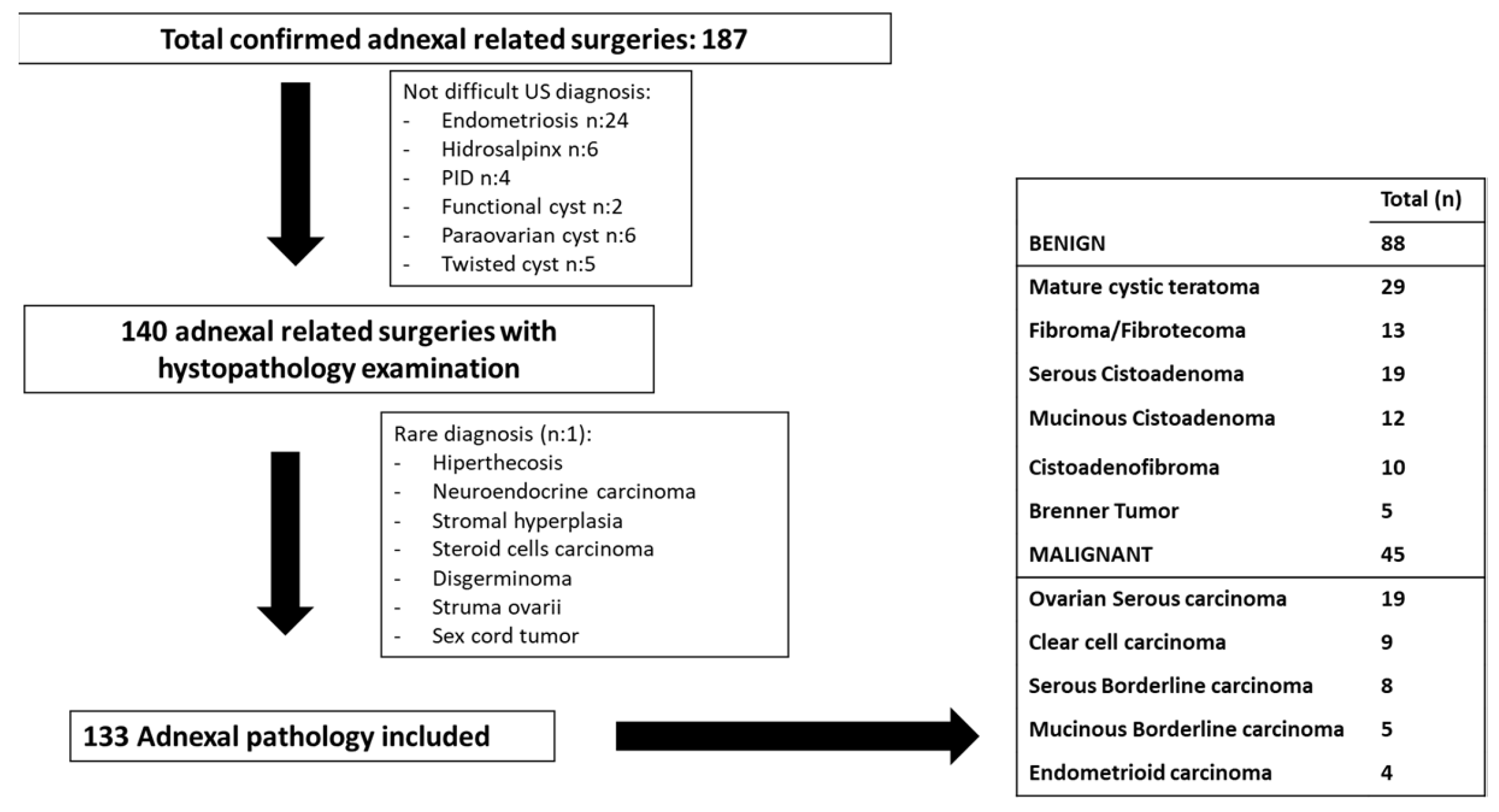
2. Materials and Methods
3. Criteria for Inclusion and Exclusion
4. Methodology
5. Statistical Analysis
6. Results
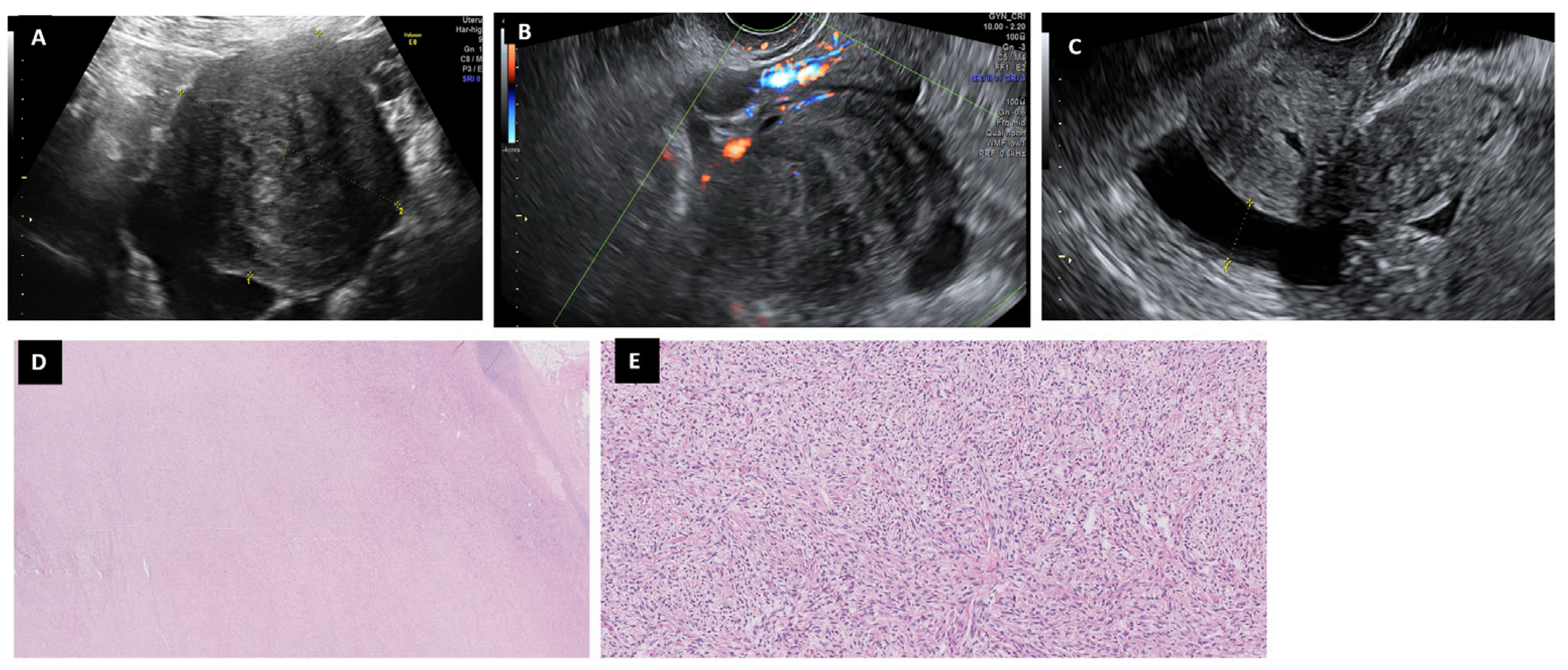
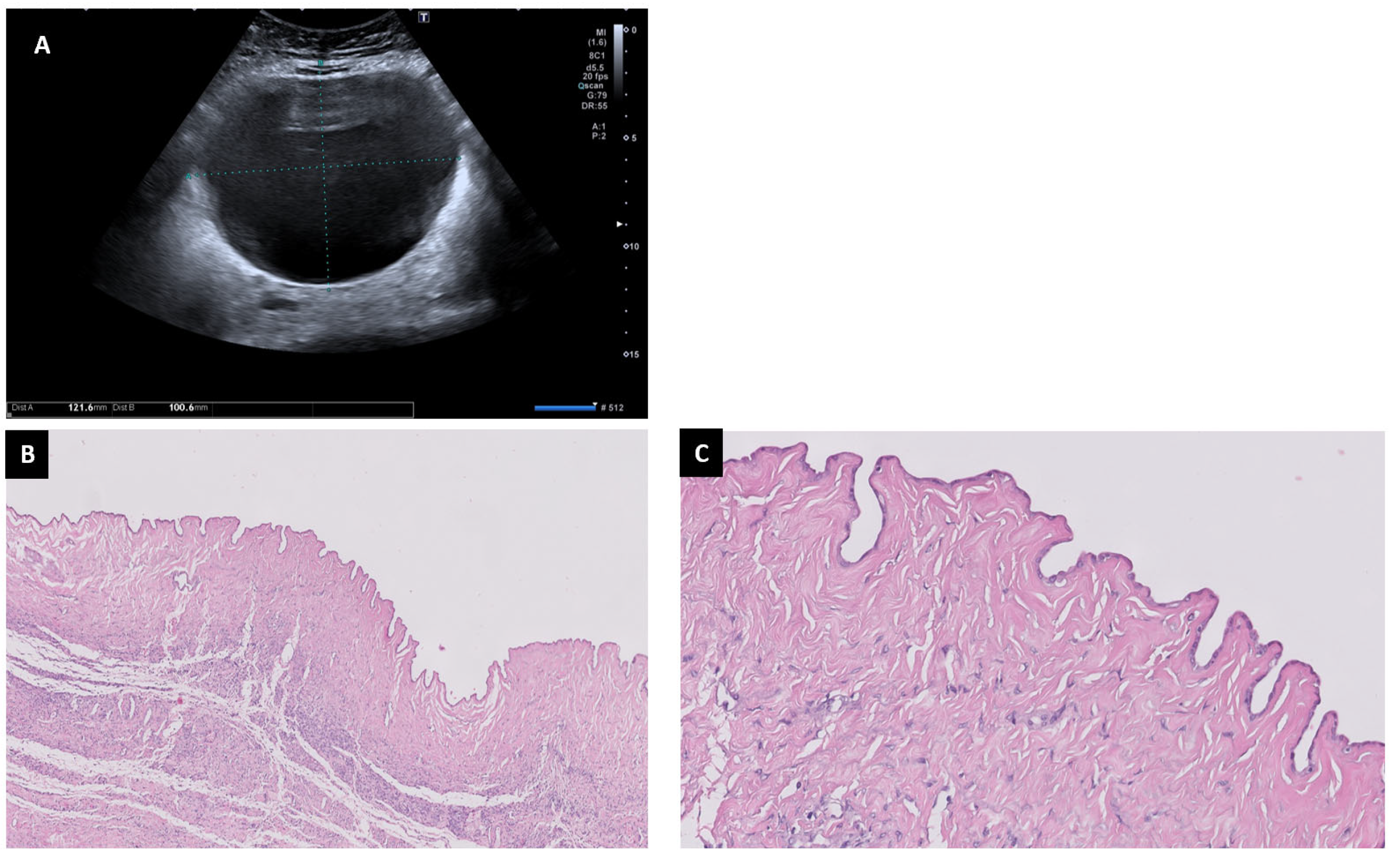
6.1. Fibromas
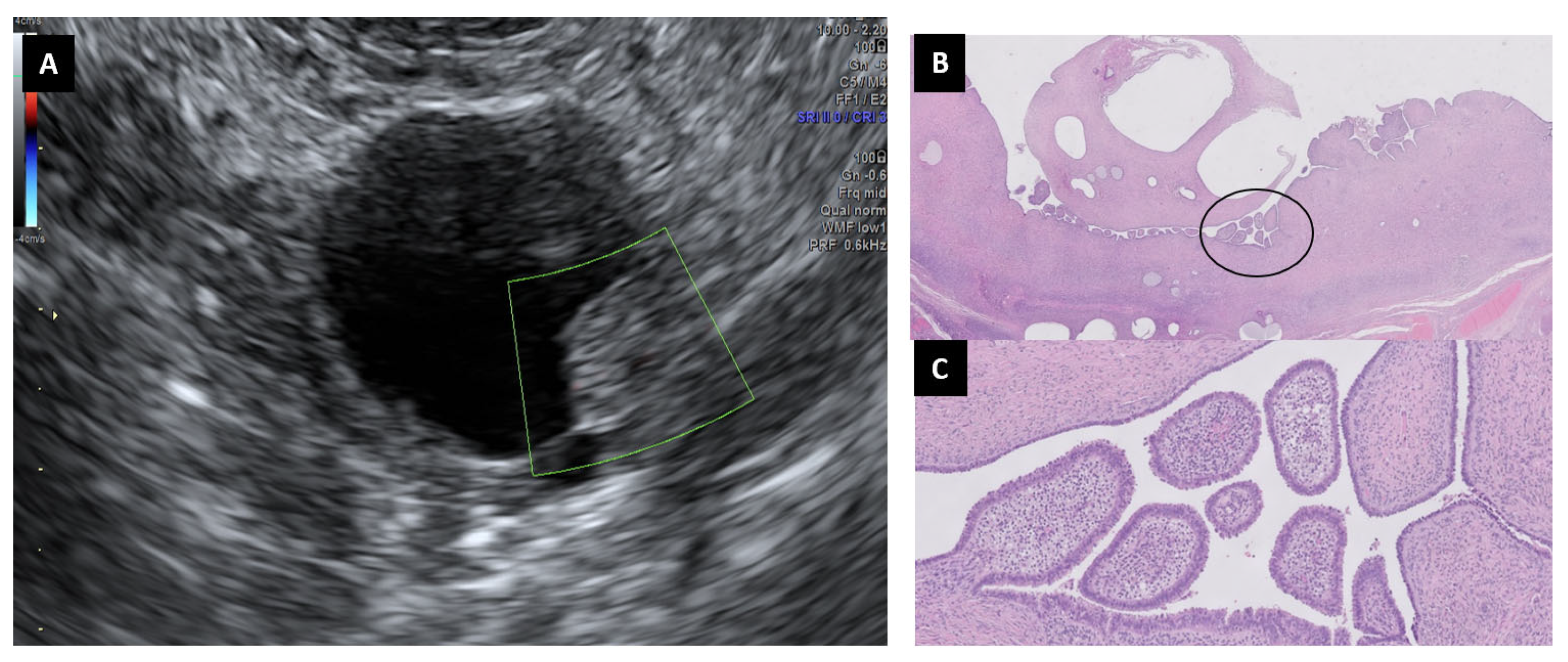
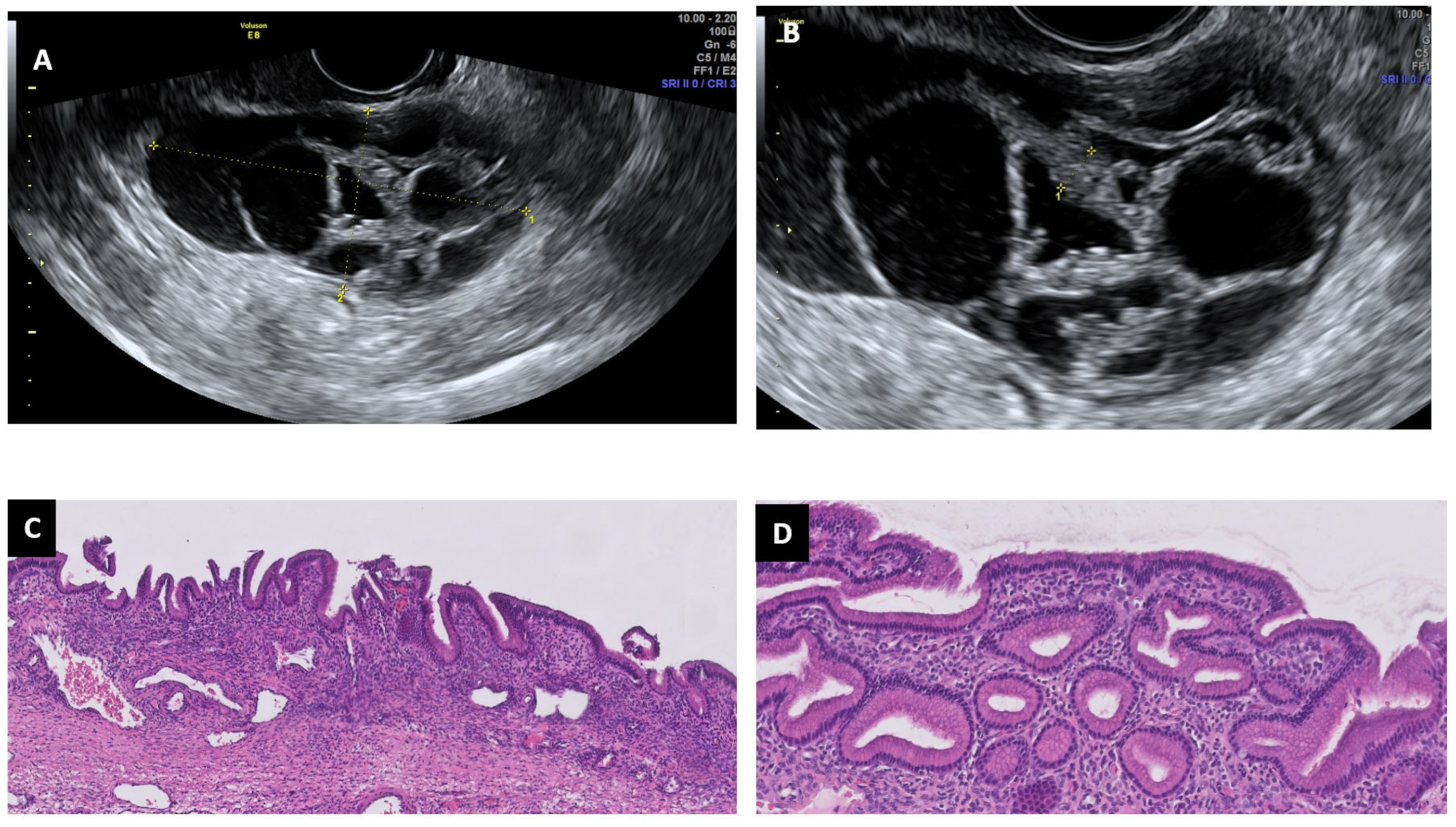
6.2. Cystoadenofibromas
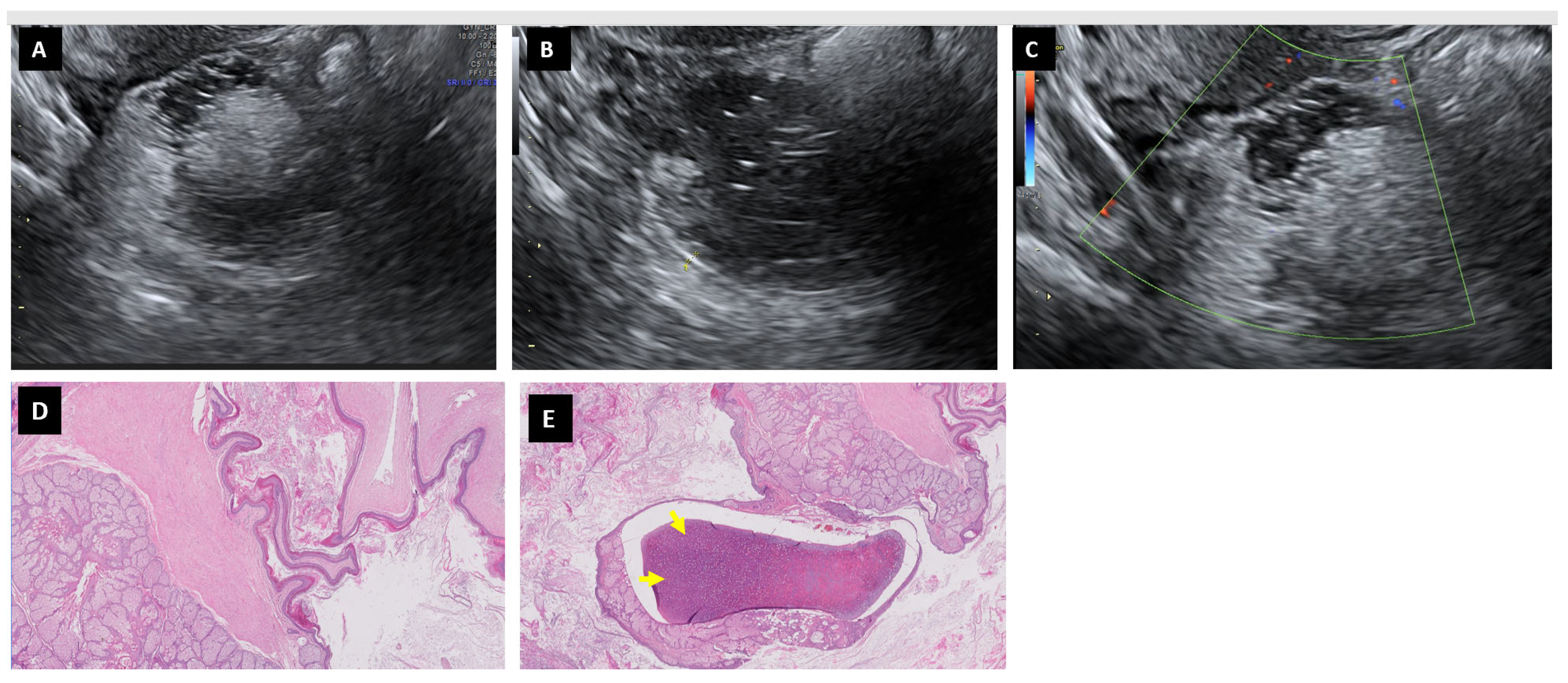
6.3. Mature Cystic Teratomas
6.4. Mucinous Cystadenoma
6.5. Serous Cystadenoma
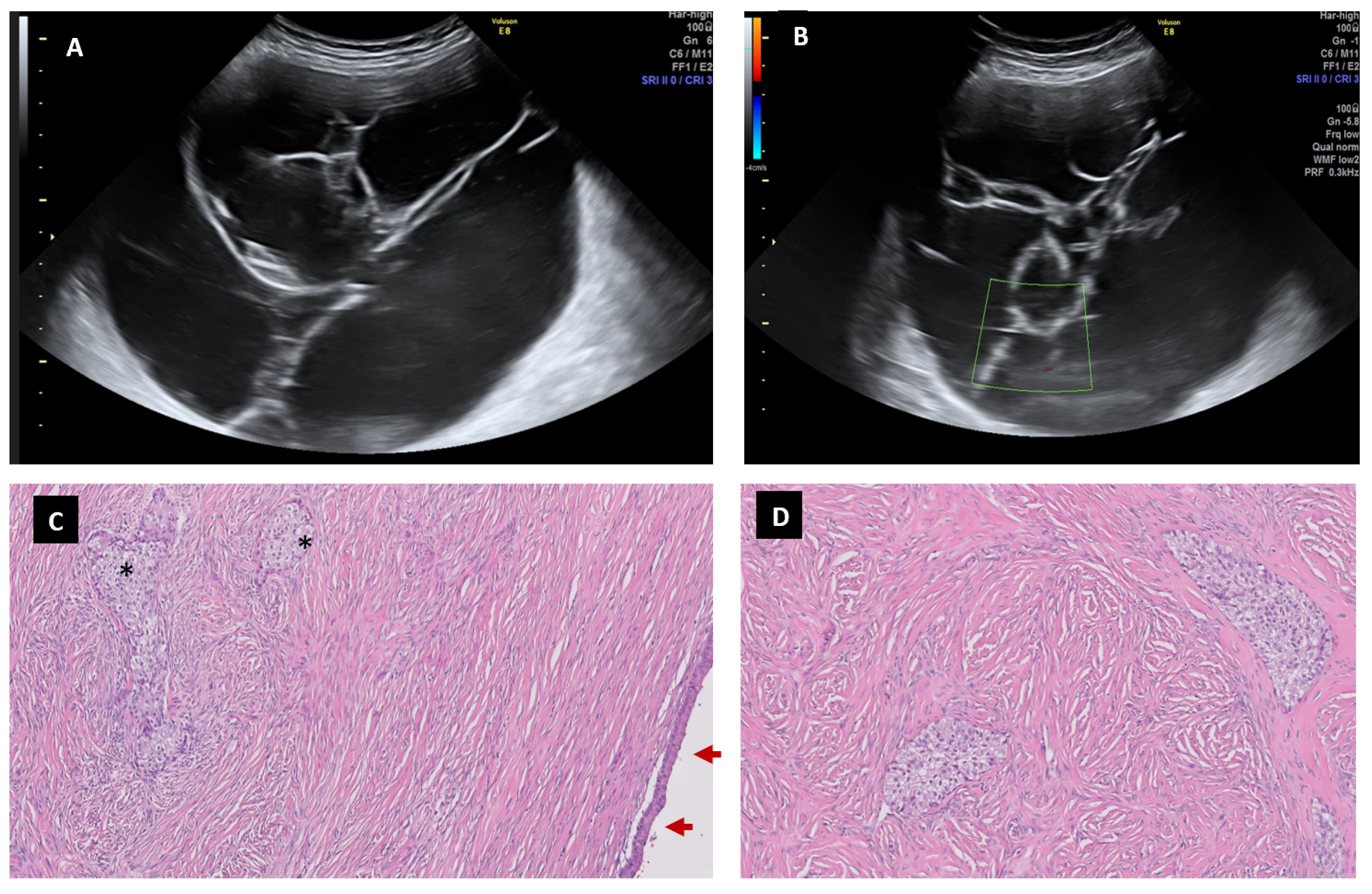
6.6. Brenner Tumor
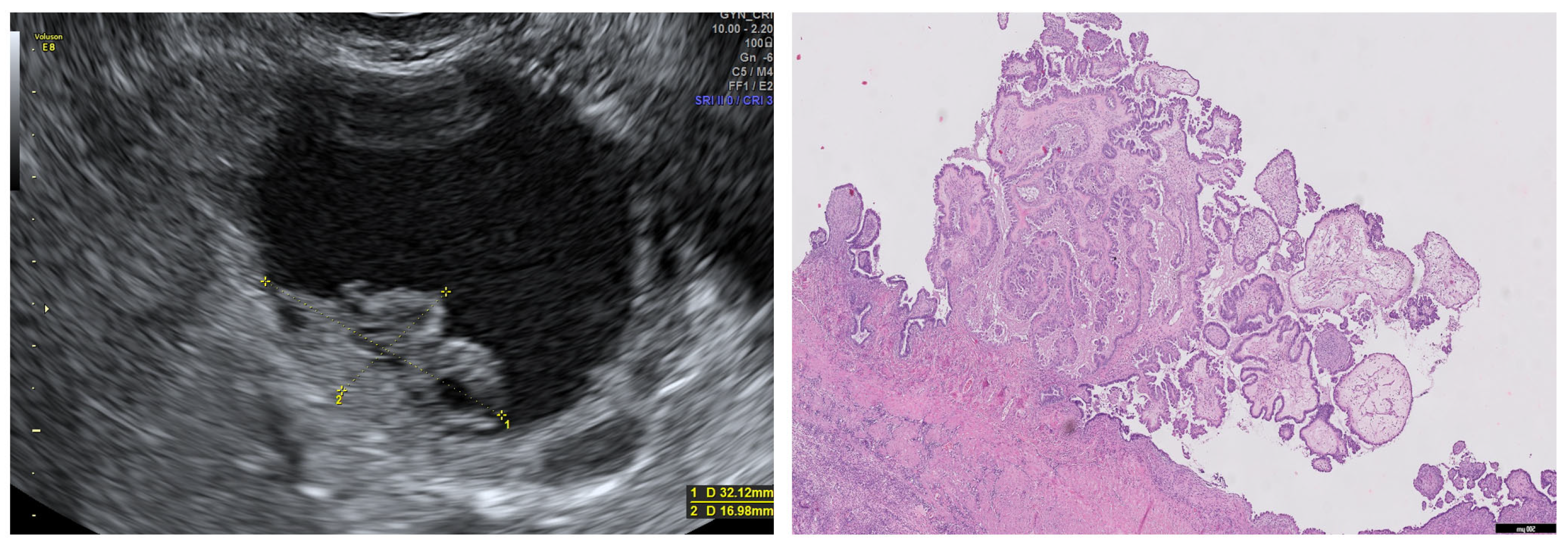
6.7. Borderline Carcinoma
6.8. Serous Carcinoma
6.9. Clear Cell Carcinoma
6.10. Endometrioid Carcinoma
7. Discussion
8. Strengths and Limitations
9. Conclusions
10. Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| US | Ultrasound |
| SA | Subjective Assessment |
| IOTA SRRA | International Ovarian Tumor Analysis Simple Rules Risk Assessment |
| ADNEX model | Assessment of Different Neoplasias in the Adnexa |
| O-RADS | Ovarian Adnexal Reporting and Data System |
| BLM | Mucinous Borderline Carcinoma |
| BLS | Serous Borderline Carcinoma |
References
- Timmerman, D.; Valentin, L.; Bourne, T.H.; Collins, W.P.; Verrelst, H.; Vergote, I. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: A consensus opinion from the International Ovarian Tumor Analysis (IOTA) Group. Ultrasound Obstet. Gynecol. 2000, 16, 500–505. [Google Scholar] [CrossRef]
- Tavoraitė, I.; Kronlachner, L.; Opolskienė, G.; Bartkevičienė, D. Ultrasound Assessment of Adnexal Pathology: Standardized Methods and Different Levels of Experience. Medicina 2021, 57, 708. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.Y.; Park, B.K.; Lee, Y.Y.; Kim, T.-J. Validation of IOTA-ADNEX Model in Discriminating Characteristics of Adnexal Masses: A Comparison with Subjective Assessment. J. Clin. Med. 2020, 9, 2010. [Google Scholar] [CrossRef]
- Viora, E.; Piovano, E.; Poma, C.B.; Cotrino, I.; Castiglione, A.; Cavallero, C.; Sciarrone, A.; Bastonero, S.; Iskra, L.; Zola, P. The ADNEX model to triage adnexal masses: An external validation study and comparison with the IOTA two-step strategy and subjective assessment by an experienced ultrasound operator. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 247, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ameye, L.; Jurkovic, D.; Van Holsbeke, C.; Paladini, D.; Van Calster, B.; Vergote, I.; Van Huffel, S.; et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet. Gynecol. 2008, 31, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Van Calster, B.; Testa, A.; Savelli, L.; Fischerova, D.; Froyman, W.; Wynants, L.; Van Holsbeke, C.; Epstein, E.; Franchi, D.; et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. Am. J. Obstet. Gynecol. 2016, 214, 424–437. [Google Scholar] [CrossRef]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: Prospective multicentre diagnostic study. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef] [PubMed]
- Andreotti, R.F.; Timmerman, D.; Strachowski, L.M.; Froyman, W.; Benacerraf, B.R.; Bennett, G.L.; Bourne, T.; Brown, D.L.; Coleman, B.G.; Frates, M.C.; et al. O-RADS US Risk Stratification and Management System: A Consensus Guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology 2020, 294, 168–185. [Google Scholar] [CrossRef] [PubMed]
- Andreotti, R.F.; Timmerman, D.; Benacerraf, B.R.; Bennett, G.L.; Bourne, T.; Brown, D.L.; Coleman, B.G.; Frates, M.C.; Froyman, W.; Goldstein, S.R.; et al. Ovarian-Adnexal Reporting Lexicon for Ultrasound: A White Paper of the ACR Ovarian-Adnexal Reporting and Data System Committee. J. Am. Coll. Radiol. 2018, 15, 1415–1429. [Google Scholar] [CrossRef]
- Pelayo-Delgado, I.; Sancho, J.; Pelayo, M.; Corraliza, V.; Perez-Mies, B.; Del Valle, C.; Abarca, L.; Pablos, M.J.; Martin-Gromaz, C.; Pérez-Vidal, J.R.; et al. Contribution of Outpatient Ultrasound Transvaginal Biopsy and Puncture in the Diagnosis and Treatment of Pelvic Lesions: A Bicenter Study. Diagnostics 2023, 13, 380. [Google Scholar] [CrossRef]
- Pelayo, M.; Sancho-Sauco, J.; Sanchez-Zurdo, J.; Abarca-Martinez, L.; Borrero-Gonzalez, C.; Sainz-Bueno, J.A.; Alcazar, J.L.; Pelayo-Delgado, I. Ultrasound Features and Ultrasound Scores in the Differentiation between Benign and Malignant Adnexal Masses. Diagnostics 2023, 13, 2152. [Google Scholar] [CrossRef]
- Meinhold-Heerlein, I.; Fotopoulou, C.; Harter, P.; Kurzeder, C.; Mustea, A.; Wimberger, P.; Hauptmann, S.; Sehouli, J. The new WHO classification of ovarian, fallopian tube, and primary peritoneal cancer and its clinical implications. Arch. Gynecol. Obstet. 2016, 293, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Zeppernick, F.; Meinhold-Heerlein, I. The new FIGO staging system for ovarian, fallopian tube, and primary peritoneal cancer. Arch. Gynecol. Obstet. 2014, 290, 839–842. [Google Scholar] [CrossRef] [PubMed]
- Prat, J. FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynaecol. Obstet. 2014, 124, 1–5. [Google Scholar] [CrossRef]
- Valentin, L.; Ameye, L.; Jurkovic, D.; Metzger, U.; Lécuru, F.; Van Huffel, S.; Timmerman, D. Which extrauterine pelvic masses are difficult to correctly classify as benign or malignant on the basis of ultrasound findings and is there a way of making a correct diagnosis? Ultrasound Obstet. Gynecol. 2006, 27, 438–444. [Google Scholar] [CrossRef]
- Paladini, D.; Testa, A.; Van Holsbeke, C.; Mancari, R.; Timmerman, D.; Valentin, L. Imaging in gynecological disease (5): Clinical and ultrasound characteristics in fibroma and fibrothecoma of the ovary. Ultrasound Obstet. Gynecol. 2009, 34, 188–195. [Google Scholar] [CrossRef]
- Chen, H.; Liu, Y.; Shen, L.-F.; Jiang, M.-J.; Yang, Z.-F.; Fang, G.-P. Ovarian thecoma-fibroma groups: Clinical and sonographic features with pathological comparison. J. Ovarian Res. 2016, 9, 81. [Google Scholar] [CrossRef]
- Timmerman, D.; Moerman, P.; Vergote, I. Meigs’ syndrome with elevated serum CA 125 levels: Two case reports and review of the literature. Gynecol. Oncol. 1995, 59, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Van den Bosch, T.; Dueholm, M.; Leone, F.P.; Valentin, L.; Rasmussen, C.K.; Votino, A.; Van Schoubroeck, D.; Landolfo, C.; Installé, A.J.; Guerriero, S.; et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: A consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound Obstet. Gynecol. 2015, 46, 284–298. [Google Scholar] [CrossRef] [PubMed]
- Virgilio, B.A.; De Blasis, I.; Sladkevicius, P.; Moro, F.; Zannoni, G.F.; Arciuolo, D.; Mascilini, F.; Ciccarone, F.; Timmerman, D.; Kaijser, J.; et al. Imaging in gynecological disease (16): Clinical and ultrasound characteristics of serous cystadenofibromas in adnexa. Ultrasound Obstet. Gynecol. 2019, 54, 823–830. [Google Scholar] [CrossRef]
- Alcázar, J.L.; Errasti, T.; Mínguez, J.A.; Galán, M.J.; García-Manero, M.; Ceamanos, C. Sonographic features of ovarian cystadenofibromas: Spectrum of findings. J. Ultrasound Med. 2001, 20, 915–919. [Google Scholar] [CrossRef]
- Goldstein, S.R.; Timor-Tritsch, I.E.; Monteagudo, A.; Monda, S.; Popiolek, D. Cystadenofibromas: Can transvaginal ultrasound appearance reduce some surgical interventions? J. Clin. Ultrasound 2015, 43, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Heremans, R.; Valentin, L.; Sladkevicius, P.; Timmerman, S.; Moro, F.; Van Holsbeke, C.; Epstein, E.; Testa, A.C.; Timmerman, D.; Froyman, W. Imaging in gynecological disease (24): Clinical and ultrasound characteristics of ovarian mature cystic teratomas. Ultrasound Obstet. Gynecol. 2022, 60, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Sancho-Saúco, J.; Corraliza-Galán, V.; de la Fuente, J.L.; Sánchez-Martínez, C.; Pelayo-Delgado, I.; De Pablos-Antona, M.J.; Cabezas-López, E.; García-Pérez, J.C. Anti-NMDA receptor encephalitis: Two case reports associated with ovarian teratoma and a literature review. J. Obstet. Gynaecol. 2019, 39, 864–865. [Google Scholar] [CrossRef] [PubMed]
- Marko, J.; Marko, K.I.; Pachigolla, S.L.; Crothers, B.A.; Mattu, R.; Wolfman, D.J. Mucinous Neoplasms of the Ovary: Radiologic-Pathologic Correlation. Radiographics 2019, 39, 982–997. [Google Scholar] [CrossRef]
- Moro, F.; Zannoni, G.F.; Arciuolo, D.; Pasciuto, T.; Amoroso, S.; Mascilini, F.; Mainenti, S.; Scambia, G.; Testa, A.C. Imaging in gynecological disease (11): Clinical and ultrasound features of mucinous ovarian tumors. Ultrasound Obstet. Gynecol. 2017, 50, 261–270. [Google Scholar] [CrossRef]
- Pascual, A.; Guerriero, S.; Rams, N.; Juez, L.; Ajossa, S.; Graupera, B.; Hereter, L.; Cappai, A.; Pero, M.; Perniciano, M.; et al. Clinical and ultrasound features of benign, borderline, and malignant invasive mucinous ovarian tumors. Eur. J. Gynaecol. Oncol. 2017, 38, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Limaiem, F.; Lekkala, M.R.; Mlika, M. Ovarian Cystadenoma; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: http://www.ncbi.nlm.nih.gov/books/NBK536950/ (accessed on 1 June 2023).
- Weinberger, V.; Minář, L.; Felsinger, M.; Ovesná, P.; Bednaříková, M.; Číhalová, M.; Jandáková, E.; Hausnerová, J.; Chaloupková, B.; Zikán, M. Brenner tumor of the ovary—Ultrasound features and clinical management of a rare ovarian tumor mimicking ovarian cancer. Ginekol. Pol. 2018, 89, 357–363. [Google Scholar] [CrossRef]
- Fagotti, A.; Ludovisi, M.; De Blasis, I.; Virgilio, B.; Di Legge, A.; Mascilini, F.; Moruzzi, M.C.; Giansiracusa, C.; Fanfani, F.; Tropeano, G.; et al. The sonographic prediction of invasive carcinoma in unilocular-solid ovarian cysts in premenopausal patients: A pilot study. Hum. Reprod. 2012, 27, 2676–2683. [Google Scholar] [CrossRef]
- Moro, F.; Baima Poma, C.; Zannoni, G.F.; Vidal Urbinati, A.; Pasciuto, T.; Ludovisi, M.; Moruzzi, M.C.; Carinelli, S.; Franchi, D.; Scambia, G.; et al. Imaging in gynecological disease (12): Clinical and ultrasound features of invasive and non-invasive malignant serous ovarian tumors. Ultrasound Obstet. Gynecol. 2017, 50, 788–799. [Google Scholar] [CrossRef]
- Ludovisi, M.; Foo, X.; Mainenti, S.; Testa, A.C.; Arora, R.; Jurkovic, D. Ultrasound diagnosis of serous surface papillary borderline ovarian tumor: A case series with a review of the literature. J. Clin. Ultrasound 2015, 43, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Suh-Burgmann, E.; Brasic, N.; Jha, P.; Hung, Y.-Y.; Goldstein, R.B. Ultrasound characteristics of early-stage high-grade serous ovarian cancer. Am. J. Obstet. Gynecol. 2021, 225, 409.e1–409.e8. [Google Scholar] [CrossRef] [PubMed]
- Di Legge, A.; Pollastri, P.; Mancari, R.; Ludovisi, M.; Mascilini, F.; Franchi, D.; Jurkovic, D.; Coccia, M.E.; Timmerman, D.; Scambia, G.; et al. Clinical and ultrasound characteristics of surgically removed adnexal lesions with largest diameter ≤ 2.5 cm: A pictorial essay. Ultrasound Obstet. Gynecol. 2017, 50, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.; Capanna, G.; Di Florio, C.; Sollima, L.; Guido, M.; Ludovisi, M. Sonographic characteristics of ovarian Leydig cell tumor. Ultrasound Obstet. Gynecol. 2023. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Pozzati, F.; Moro, F.; Pasciuto, T.; Gallo, C.; Ciccarone, F.; Franchi, D.; Mancari, R.; Giunchi, S.; Timmerman, D.; Landolfo, C.; et al. Imaging in gynecological disease (14): Clinical and ultrasound characteristics of ovarian clear cell carcinoma. Ultrasound Obstet. Gynecol. 2018, 52, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Moro, F.; Magoga, G.; Pasciuto, T.; Mascilini, F.; Moruzzi, M.C.; Fischerova, D.; Savelli, L.; Giunchi, S.; Mancari, R.; Franchi, D.; et al. Imaging in gynecological disease (13): Clinical and ultrasound characteristics of endometrioid ovarian cancer. Ultrasound Obstet. Gynecol. 2018, 52, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Pelayo, M.; Pelayo-Delgado, I.; Sancho-Sauco, J.; Sanchez-Zurdo, J.; Abarca-Martinez, L.; Corraliza-Galán, V.; Martin-Gromaz, C.; Pablos-Antona, M.J.; Zurita-Calvo, J.; Alcázar, J.L. Comparison of Ultrasound Scores in Differentiating between Benign and Malignant Adnexal Masses. Diagnostics 2023, 13, 1307. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SRRA | ADNEX without CA125 | ADNEX with CA125 | O-RADS | ||||
|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 5 | ||||
| Oncology center | Yes | Yes | Yes | No | No | No | No |
| Age | No | Yes | Yes | No | No | No | No |
| Size | ≥100 mm M | Yes | Yes | Yes | Yes | Yes | No |
| Uni/Multilocular | Yes | > or <10 locules | > or <10 locules | Yes | Yes | Yes | Yes |
| Smooth/Irregular | Yes | No | No | Yes | Yes | Yes | Yes |
| Solid components | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Size solid components | <7 mm B | Yes | Yes | No | No | No | No |
| Papillae | ≥4 M | 0/1/2/3/ > 3 | 0/1/2/3/ > 3 | No | No | <4 | ≥4 |
| Septum | No | No | No | Yes | Yes | No | No |
| Acoustic shadows | Yes | Yes | Yes | No | Yes * | Yes | Yes * |
| Blood flow (color score) | 1:B 4:M | No | No | No | Yes | Yes | Yes |
| Ascites | M | Yes | Yes | No | No | No | Yes |
| CA125 | No | No | Yes | No | No | No | No |
| Other features | - | - | - | Typical lesions | - | - | - |
| Age, Years (Mean, SD) | Postmenopausal (n, %) | CA125, IU/mL (Mean, SD) | |
|---|---|---|---|
| Benign | |||
| Fibroma (n:13) | 62.7 ± 10.9 | 10 (76.9%) | 93.2 ± 222.5 |
| Cystoadenofibroma (n:10) | 57.3 ± 9.5 | 7 (70.0%) | 18.7 ± 14.0 |
| Mature cystic teratoma (n:12) | 36.5 ± 13.8 | 5 (17.2%) | 21.6 ± 14.9 |
| Mucinous cystoadenoma (n:12) | 50.9 ± 11.7 | 5 (41.7%) | 26.7 ± 21.1 |
| Serous cystoadenoma (n:19) | 51.2 ± 19.1 | 9 (47.3%) | 15.1 ± 9.4 |
| Brenner tumor (n:5) | 66.4 ± 7.7 | 5 (100.0%) | 29.9 ± 13.3 |
| Malignant | |||
| Borderline (n:13) | 50.3 ± 13.6 | 6 (46.2%) | 49.5 ± 7.7 |
| Serous carcinoma (n:19) | 61.9 ± 11.3 | 17 (89.5%) | 1661.4 ± 3414.7 |
| Clear cell carcinoma (n:9) | 55.7 ± 10.7 | 7 (77.8%) | 216.2 ± 451.3 |
| Endometrioid carcinoma (n:4) | 44.3 ± 8.5 | 2 (50.0%) | 755.0 ± 625.0 |
| Maximum Size (mm) (Mean, SD) | Solid Part | Papillae (n, %) | Acoustic Shadows (n, %) | Ascites (n, %) | |||
|---|---|---|---|---|---|---|---|
| (n, %) | Size (mm) Mean (SD) Min.–Max. | ↑ Doppler | |||||
| Benign | |||||||
| Fibroma (n:13) | 97.1 ± 42.3 | 11 (84.6%) | 76.8 ± 23.2 (44–112) | 1 (7.7%) | 0 (0.0%) | 11 (84.6%) | 9 (69.2%) |
| Cystoadenofibroma (n:10) | 60.0 ± 51.1 | 7 (70.0%) | 12.1 ± 3.9 (6–17) | 0 (0.0%) | 0 (0.0%) | 6 (60.0%) | 0 (0.0%) |
| Mature cystic teratoma (n:12) | 82.3 ± 40.1 | 5 (17.2%) | 37.6 ± 18.1 (17–66) | 3 (10.3%) | 1 (3.4%) | 24 (82.7%) | 0 (0.0%) |
| Mucinous cystoadenoma (n:12) | 121.5 ± 78.8 | 2 (16.7%) | 18.5 ± 9.2 (12–25) | 0 (0.0%) | 3 (25.0%) | 12 (100.0%) | 0 (0.0%) |
| Serous cystoadenoma (n:19) | 85.0 ± 39.6 | 2 (10.5%) | 16.5 ± 4.9 (13–20) | 1 (5.3%) | 1 (5.2%) | 16 (84.2%) | 0 (0.0%) |
| Brenner tumor (n:5) | 108.4 ± 43.1 | 3 (60.0%) | 75.3 ± 34.5 (32–140) | 1 (20.0%) | 0 (0.0%) | 4 (80.0%) | 0 (0.0%) |
| Malignant | |||||||
| Borderline (n:13) | 50.3 ± 13.6 | 6 (46.2%) | 53.5 ± 60.5 (12–210) | 6 (46.1%) | 8 (61.5%) | 5 (38.5%) | 2 (15.4%) |
| Serous carcinoma (n:19) | 61.9 ± 11.3 | 17 (89.5%) | 53.6 ± 23.9 (17–98) | 13 (68.4%) | 8 (42.1%) | 4 (21.0%) | 5 (26.3%) |
| Clear cell carcinoma (n:9) | 55.7 ± 10.7 | 7 (77.8%) | 53.0 ± 39.9 (24–155) | 7 (77.7%) | 2 (22.2%) | 0 (0.0%) | 1 (11.1%) |
| Endometrioid carcinoma (n:4) | 44.3 ± 8.5 | 2 (50.0%) | 47.0 ± 6.0 (41–53) | 3 (75.0%) | 3 (75.0%) | 1 (25.0%) | 1 (25.0%) |
| Subjective Assessment Malignancy | SRRA % Malignancy | ADNEX without CA125 Malignancy | ADNEX with CA125 Malignancy | O-RADS | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. Malignancy (%) | RR [95% CI] p-Value | No. Malignancy (%) | RR [95% CI] p-Value | No. Malignancy (%) | RR [95% CI] p-Value | No. Malignancy (%) | RR [95% CI] p-Value | No. Malignancy (%) | RR [95% CI] p-Value | |
| Benign | ||||||||||
| Fibroma (n:13) | 3 (23.1%) | [reference] | 9 (69.2%) | 3 [1.04, 8.63] 0.018 | 11 (84.6%) | 3.66 [1.32, 10.16] 0.002 | 9 (69.2%) | 3 [1.04, 8.63] 0.018 | 7 (53.9%) | 2.33 [0.77, 7.10] 0.107 |
| Cystoadenofibroma (n:10) | 7 (70.0%) | [reference] | 2 (20.0%) | 0.28 [0.08, 1.05] 0.070 | 6 (60.0%) | 0.86 [0.45, 1.64] 1.000 | 5 (50.0%) | 0.72 [0.34, 1.50] 0.650 | 9 (90.0%) | 1.29 [0.82, 2.03] 0.582 |
| Mature cystic teratoma (n:12) | 3 (10.3%) | [reference] | 2 (6.9%) | 0.67 [0.12, 3.70] 1.000 | 3 (10.3%) | 1 [0.22, 4.55] 1.000 | 1 (3.4%) | 0.33 [0.04, 3.02] 0.611 | 3 (10.3%) | 1 [0.22, 4.55] 1.000 |
| Mucinous cystoadenoma (n:12) | 4 (33.3%) | [reference] | 2 (16.7%) | 0.5 [0.11, 2.23] 0.640 | 2 (16.7%) | 0.5 [0.11, 2.23] 0.640 | 2 (16.7%) | 0.5 [0.11, 2.23] 0.640 | 5 (41.7%) | 1.25 [0.44, 3.55] 1.000 |
| Serous cystoadenoma (n:19) | 3 (15.8%) | [reference] | 3 (15.8%) | 1 [0.23, 4.34] 1.000 | 2 (10.5%) | 0.67 [0.13, 3.55] 1.000 | 2 (10.5%) | 0.67 [0.13, 3.55] 1.000 | 3 (15.8%) | 1 [0.23, 4.34] 1.000 |
| Brenner tumor (n:5) | 4 (80.0%) | [reference] | 1 (25.0%) | 0.25 [0.04, 1.52] 0.206 | 1 (25.0%) | 0.25 [0.04, 1.52] 0.206 | 1 (25.0%) | 0.25 [0.04, 1.52] 0.206 | 3 (75.0%) | 0.75 [0.32, 1.74] 1.000 |
| Malignant | ||||||||||
| Borderline (n:13) | 13 (100%) | [reference] | 10 (76.9%) | 0.77 [0.57, 1.04] 0.220 | 10 (76.9%) | 0.77 [0.57, 1.04] 0.220 | 11 (84.6%) | 0.84 [0.67, 1.07] 0.480 | 13 (100%) | 1 |
| Serous carcinoma (n:19) | 19 (100%) | [reference] | 17 (89.5%) | 0.89 [0.77, 1.04] 0.486 | 19 (100%) | 1 | 19 (100%) | 1 | 19 (100%) | 1 |
| Clear cell carcinoma (n:9) | 9 (100%) | [reference] | 6 (66.7%) | 0.66 [0.42, 1.06] 0.206 | 9 (100%) | 1 | 9 (100%) | 1 | 9 (100%) | 1 |
| Endometrioid carcinoma (n:4) | 4 (100%) | [reference] | 4 (100%) | 1 | 3 (75.0%) | 0.75 [0.46, 1.32] 1.000 | 4 (100%) | 1 | 4 (100%) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelayo, M.; Sancho-Sauco, J.; Sánchez-Zurdo, J.; Perez-Mies, B.; Abarca-Martínez, L.; Cancelo-Hidalgo, M.J.; Sainz-Bueno, J.A.; Alcázar, J.L.; Pelayo-Delgado, I. Application of Ultrasound Scores (Subjective Assessment, Simple Rules Risk Assessment, ADNEX Model, O-RADS) to Adnexal Masses of Difficult Classification. Diagnostics 2023, 13, 2785. https://doi.org/10.3390/diagnostics13172785
Pelayo M, Sancho-Sauco J, Sánchez-Zurdo J, Perez-Mies B, Abarca-Martínez L, Cancelo-Hidalgo MJ, Sainz-Bueno JA, Alcázar JL, Pelayo-Delgado I. Application of Ultrasound Scores (Subjective Assessment, Simple Rules Risk Assessment, ADNEX Model, O-RADS) to Adnexal Masses of Difficult Classification. Diagnostics. 2023; 13(17):2785. https://doi.org/10.3390/diagnostics13172785
Chicago/Turabian StylePelayo, Mar, Javier Sancho-Sauco, Javier Sánchez-Zurdo, Belén Perez-Mies, Leopoldo Abarca-Martínez, Mª Jesús Cancelo-Hidalgo, Jose Antonio Sainz-Bueno, Juan Luis Alcázar, and Irene Pelayo-Delgado. 2023. "Application of Ultrasound Scores (Subjective Assessment, Simple Rules Risk Assessment, ADNEX Model, O-RADS) to Adnexal Masses of Difficult Classification" Diagnostics 13, no. 17: 2785. https://doi.org/10.3390/diagnostics13172785