
Psychopathology, Personality and Depression after Acute Coronary Syndrome: A Network Analysis in an Italian Population
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Baseline Assessment
2.3. Follow-Up Assessments and Outcomes
3. Data Analysis
3.1. State Characteristics and Data Reduction
3.2. Network Estimation
4. Results
4.1. Symptom Data Reduction
4.2. Risk Factors for MDE at Follow Up
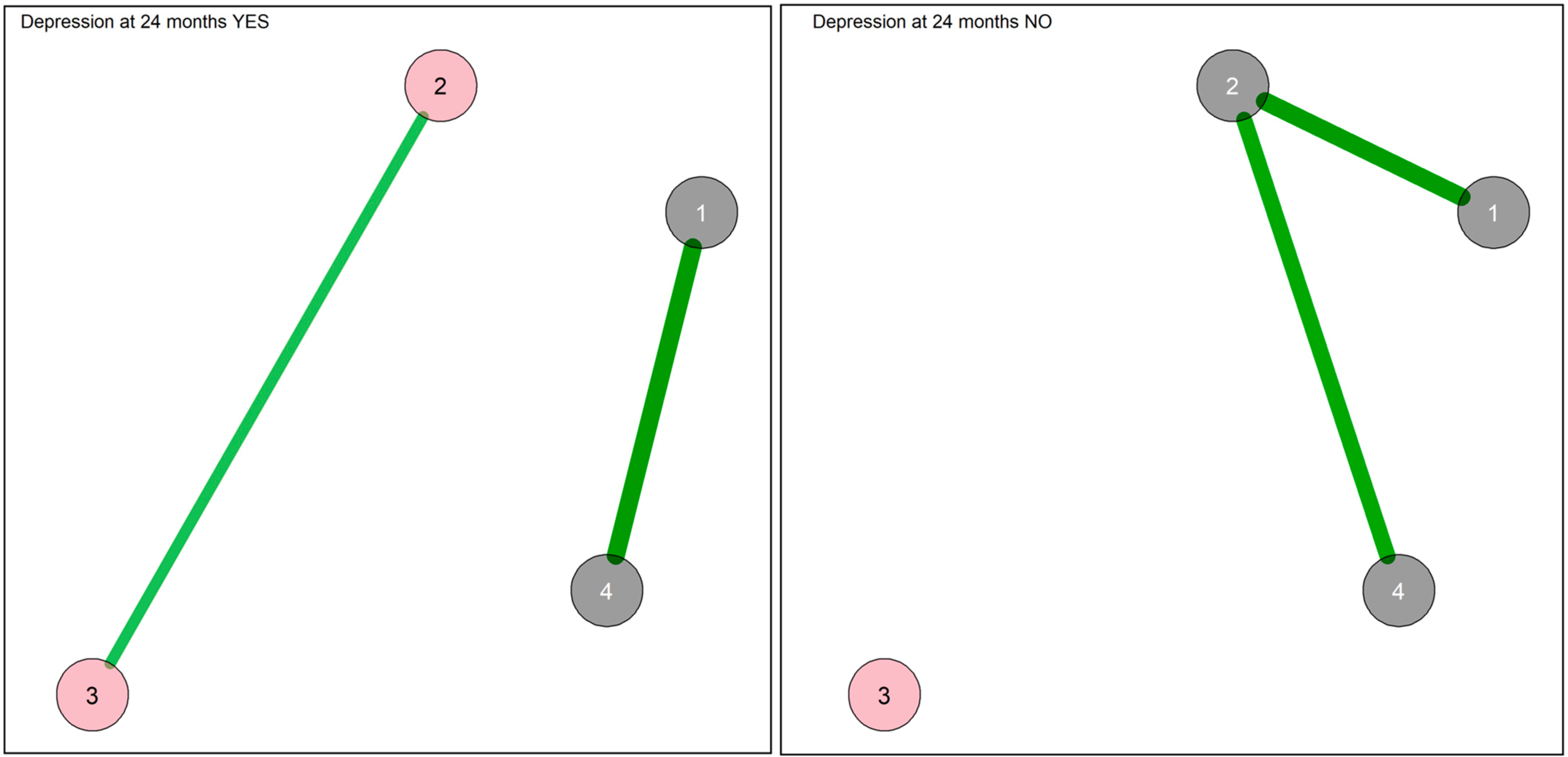
4.2.1. Network of the Baseline State Measures in the Sample Divided According to the Occurrence of MDE
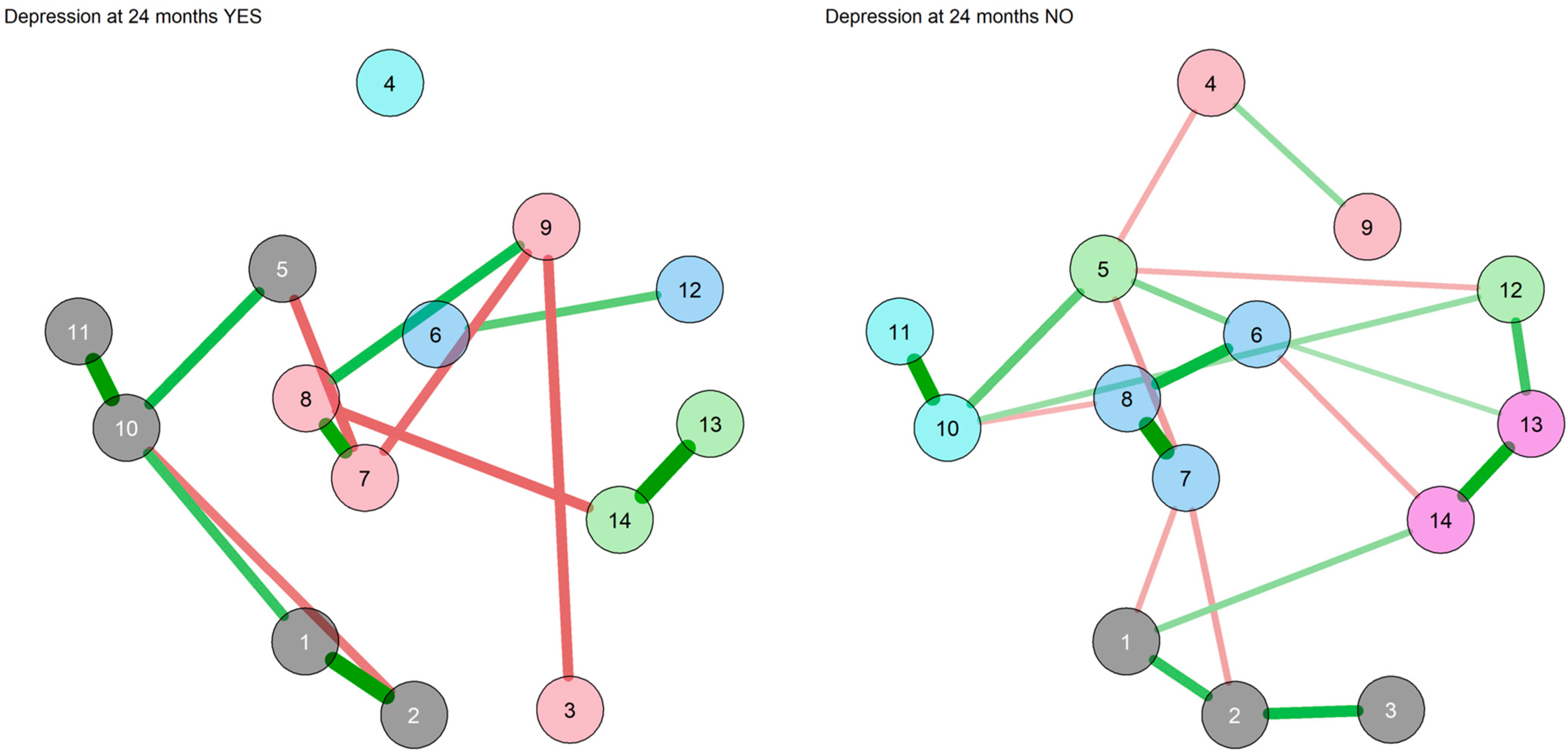
4.2.2. Network of the Trait Measures in the Sample Divided According to the Occurrence of MDE
4.3. Analyses of the Sample Divided According to the Occurrence of MACE
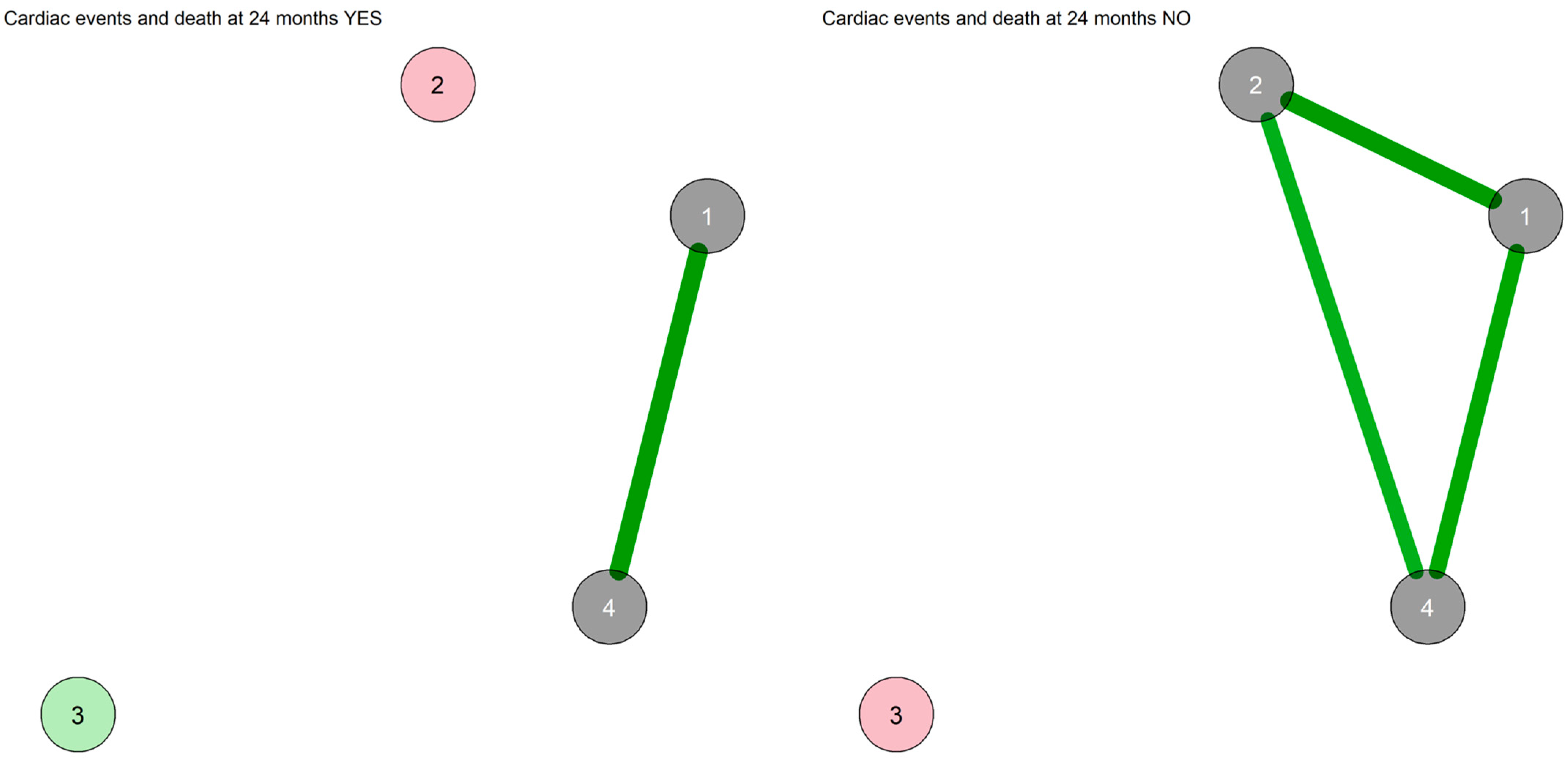
4.3.1. Network of the State Measures in the Sample Divided According to the Occurrence of MACE
4.3.2. Network of the Trait Measures in the Sample Divided According to the Occurrence of MACE
5. Discussion
5.1. Factors Associated with Depression at Follow-Up
5.2. Factors Associated with Cardiovascular Events at Follow-Up
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frost, J.; Rich, R.L.; Robbins, C.W.; Stevermer, J.J.; Chow, R.T.; Leon, K.K.; Bird, M.D. Depression Following Acute Coronary Syndrome Events: Screening and Treatment Guidelines from the AAFP. Am. Fam. Phys. 2019, 99, 786A–786J. [Google Scholar]
- Lim, G.B. Risk Factors: Depression Recognized as a Risk Factor in ACS. Nat. Rev. Cardiol. 2014, 11, 185. [Google Scholar] [CrossRef] [PubMed]
- Alhurani, A.S.; Hamdan-Mansour, A.M.; Ahmad, M.M.; McKee, G.; O’donnell, S.; O’brien, F.; Mooney, M.; Saleh, Z.T.; Moser, D.K. The Association of Persistent Symptoms of Depression and Anxiety with Recurrent Acute Coronary Syndrome Events: A Prospective Observational Study. Healthcare 2022, 10, 383. [Google Scholar] [CrossRef]
- Lichtman, J.H.; Froelicher, E.S.; Blumenthal, J.A.; Carney, R.M.; Doering, L.V.; Frasure-Smith, N.; Freedland, K.E.; Jaffe, A.S.; Leifheit-Limson, E.C.; Sheps, D.S.; et al. Depression as a Risk Factor for Poor Prognosis among Patients with Acute Coronary Syndrome: Systematic Review and Recommendations: A Scientific Statement from the American Heart Association. Circulation 2014, 129, 1350–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smolderen, K.G.; Buchanan, D.M.; Gosch, K.; Whooley, M.; Chan, P.S.; Vaccarino, V.; Parashar, S.; Shah, A.J.; Ho, P.M.; Spertus, J.A. Depression Treatment and 1-Year Mortality After Acute Myocardial Infarction: Insights From the TRIUMPH Registry (Translational Research Investigating Underlying Disparities in Acute Myocardial Infarction Patients’ Health Status). Circulation 2017, 135, 1681–1689. [Google Scholar] [CrossRef] [Green Version]
- Ossola, P.; Generali, I.; Schito, G.; De Panfilis, C.; Tonna, M.; Gerra, M.L.; Marchesi, C. Temperament and Depression After a First Acute Coronary Syndrome. J. Nerv. Ment. Dis. 2019, 207, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Vaccarino, V.; Badimon, L.; Bremner, J.D.; Cenko, E.; Cubedo, J.; Dorobantu, M.; Duncker, D.J.; Koller, A.; Manfrini, O.; Milicic, D.; et al. Depression and Coronary Heart Disease: 2018 Position Paper of the ESC Working Group on Coronary Pathophysiology and Microcirculation. Eur. Heart J. 2020, 41, 1687–1696. [Google Scholar] [CrossRef] [Green Version]
- Mandarano, P.; Ossola, P.; Castiglioni, P.; Faini, A.; Marazzi, P.; Carsillo, M.; Rozzi, S.; Lazzeroni, D. Heart Rate Fractality Disruption as a Footprint of Subthreshold Depressive Symptoms in a Healthy Population. Clin. Neuropsychiatry 2022, 19, 163–173. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Kappelmann, N.; Ye, Z.; Lamers, F.; Moser, S.; Jones, P.B.; Burgess, S.; Penninx, B.W.J.H.; Khandaker, G.M. Association of Inflammation with Depression and Anxiety: Evidence for Symptom-Specificity and Potential Causality from UK Biobank and NESDA Cohorts. Mol. Psychiatry 2021, 26, 7393–7402. [Google Scholar] [CrossRef]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and Cardiovascular Disease: A Clinical Review. Eur. Heart J. 2014, 35, 1365–1372. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Huo, Q.; Du, S.; Shi, X.; Shi, Q.; Cui, S.; Feng, C.; Du, X.; Wang, Y. Social Support and Self-Efficacy as Mediating Factors Affecting the Association Between Depression and Medication Adherence in Older Patients with Coronary Heart Disease: A Multiple Mediator Model with a Cross-Sectional Study. Patient Prefer. Adherence 2022, 16, 285–295. [Google Scholar] [CrossRef]
- Fan, Y.; Shen, B.J.; Tay, H.Y. Depression, Anxiety, Perceived Stress, and Their Changes Predicted Medical Adherence over 9 Months among Patients with Coronary Heart Disease. Br. J. Health Psychol. 2021, 26, 748–766. [Google Scholar] [CrossRef] [PubMed]
- Gehi, A.; Haas, D.; Pipkin, S.; Whooley, M.A. Depression and Medication Adherence in Outpatients with Coronary Heart Disease: Findings from the Heart and Soul Study. Arch. Intern. Med. 2005, 165, 2508–2513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suskin, N.G.; Huitema, A.A.; Hartley, T.; McKelvie, R.S. Sex, Depression, and More in Cardiac Rehabilitation. Can. J. Cardiol. 2021, 37, 357–358. [Google Scholar] [CrossRef] [PubMed]
- Messerli-Bürgy, N.; Molloy, G.J.; Poole, L.; Wikman, A.; Kaski, J.C.; Steptoe, A. Psychological Coping and Recurrent Major Adverse Cardiac Events Following Acute Coronary Syndrome. Br. J. Psychiatry 2015, 207, 256–261. [Google Scholar] [CrossRef] [Green Version]
- Benyamini, Y.; Roziner, I.; Goldbourt, U.; Drory, Y.; Gerber, Y. Depression and Anxiety Following Myocardial Infarction and Their Inverse Associations with Future Health Behaviors and Quality of Life. Ann. Behav. Med. 2013, 46, 310–321. [Google Scholar] [CrossRef]
- Gale, C.R.; Čukić, I.; Batty, G.D.; McIntosh, A.M.; Weiss, A.; Deary, I.J. When Is Higher Neuroticism Protective Against Death? Findings From UK Biobank. Psychol. Sci. 2017, 28, 1345–1357. [Google Scholar] [CrossRef]
- Li, X.-Q.; Tang, X.-R.; Li, L.-L. Antipsychotics Cardiotoxicity: What’s Known and What’s Next. WJP 2021, 11, 736–753. [Google Scholar] [CrossRef]
- Dickens, C.M.; Percival, C.; McGowan, L.; Douglas, J.; Tomenson, B.; Cotter, L.; Heagerty, A.; Creed, F.H. The Risk Factors for Depression in First Myocardial Infarction Patients. Psychol. Med. 2004, 34, 1083–1092. [Google Scholar] [CrossRef]
- Leong, L.K.; Zuhdi, A.S.M.; Hafidz, M.I.A. Clinical Depression among Patients after Acute Coronary Syndrome: A Prospective Single-Tertiary Centre Analysis. Singap. Med. J. 2021, 62, 653–658. [Google Scholar] [CrossRef]
- Doyle, F.; McGee, H.; Conroy, R.; Conradi, H.J.; Meijer, A.; Steeds, R.; Sato, H.; Stewart, D.E.; Parakh, K.; Carney, R.; et al. Systematic Review and Individual Patient Data Meta-Analysis of Sex Differences in Depression and Prognosis in Persons With Myocardial Infarction: A MINDMAPS Study. Psychosom. Med. 2015, 77, 419–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carney, R.M.; Freedland, K.E.; Steinmeyer, B.; Blumenthal, J.A.; De Jonge, P.; Davidson, K.W.; Czajkowski, S.M.; Jaffe, A.S. History of Depression and Survival after Acute Myocardial Infarction. Psychosom. Med. 2009, 71, 253–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frasure-Smith, N.; Lespérance, F.; Gravel, G.; Masson, A.; Juneau, M.; Talajic, M.; Bourassa, M.G. Social Support, Depression, and Mortality during the First Year after Myocardial Infarction. Circulation 2000, 101, 1919–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denollet, J.; Sys, S.U.; Brutsaert, D.L. Personality and Mortality after Myocardial Infarction. Psychosom. Med. 1995, 57, 582–591. [Google Scholar] [CrossRef] [Green Version]
- De Fazio, P.; Caroleo, M.; Rizza, P.; Cerminara, G.; De Serio, D.; Indolfi, C.; Segura-García, C. Specific Personality Traits and Coping Styles Predict Affective Symptoms in Early Post Acute Coronary Syndrome Inpatients. Int. J. Psychiatry Med. 2012, 44, 119–132. [Google Scholar] [CrossRef]
- Romppel, M.; Herrmann-Lingen, C.; Vesper, J.M.; Grande, G. Type D Personality and Persistence of Depressive Symptoms in a German Cohort of Cardiac Patients. J. Affect. Disord. 2012, 136, 1183–1187. [Google Scholar] [CrossRef]
- Roberts, S.B.; Kendler, K.S. Neuroticism and self-esteem as indices of the vulnerability to major depression in women. Psychol. Med. 1999, 29, 1101–1109. [Google Scholar] [CrossRef]
- Parker, G.B.; Cvejic, E.; Vollmer-Conna, U.; McCraw, S.; Granville Smith, I.; Walsh, W.F. Depression and Poor Outcome after an Acute Coronary Event: Clarification of Risk Periods and Mechanisms. Aust. N. Z. J. Psychiatry 2019, 53, 148–157. [Google Scholar] [CrossRef]
- Carless, D.; Douglas, K.; Fox, K.; McKenna, J. An Alternative View of Psychological Well-Being in Cardiac Rehabilitation: Considering Temperament and Character. Eur. J. Cardiovasc. Nurs. 2006, 5, 237–243. [Google Scholar] [CrossRef]
- Peters, R.M.; Lumley, M.A. Relationship of Alexithymia to Cardiovascular Disease Risk Factors among African Americans. Compr. Psychiatry 2007, 48, 34–41. [Google Scholar] [CrossRef]
- Kojima, M.; Frasure-Smith, N.; Lesperance, F. Alexithymia Following Myocardial Infarction Psychometric Properties and Correlates of the Toronto Alexithymia Scale. J. Psychosom. Res. 2001, 51, 487–495. [Google Scholar] [CrossRef] [PubMed]
- 32. Honkalampi, K.; Hintikka, J.; Tanskanen, A.; Lehtonen, J.; Viinamäki, H. Depression is strongly associated with alexithymia in the general population. J. Psychosom. Res. 2000, 48, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.; O’Brien, E.J. The Person-Situation Debate in Historical and Current Perspective. Psychol. Bull. 1985, 98, 513–537. [Google Scholar] [CrossRef] [PubMed]
- Steyer, R.; Schmitt, M.; Eid, M. Latent State-Trait Theory and Research in Personality and Individual Differences. Eur. J. Personal. 1999, 13, 389–408. [Google Scholar] [CrossRef]
- Ossola, P.; Paglia, F.; Pelosi, A.; De Panfilis, C.; Conte, G.; Tonna, M.; Ardissino, D.; Marchesi, C. Risk Factors for Incident Depression in Patients at First Acute Coronary Syndrome. Psychiatry Res. 2015, 228, 448–453. [Google Scholar] [CrossRef] [Green Version]
- Marchesi, C.; Ossola, P.; Scagnelli, F.; Mellini, L.; Tonna, M.; Ardissino, D.; De Panfilis, C. The Role of Alexithymia in Predicting Incident Depression in Patients at First Acute Coronary Syndrome. Compr. Psychiatry 2015, 62, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Marchesi, C.; Ossola, P.; Tonna, M.; De Panfilis, C. The TAS-20 More Likely Measures Negative Affects Rather than Alexithymia Itself in Patients with Major Depression, Panic Disorder, Eating Disorders and Substance Use Disorders. Compr. Psychiatry 2014, 55, 972–978. [Google Scholar] [CrossRef] [Green Version]
- Ossola, P.; Gerra, M.L.; Beltrani, M.; Marchesi, C. Alexithymia and Cardiac Outcome in Patients at First Acute Coronary Syndrome. Int.J. Behav. Med. 2019, 26, 673–679. [Google Scholar] [CrossRef]
- De Panfilis, C.; Ossola, P.; Tonna, M.; Catania, L.; Marchesi, C. Finding Words for Feelings: The Relationship between Personality Disorders and Alexithymia. Personal. Individ. Differ. 2015, 74, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Marchesi, C.; Ossola, P.; Scagnelli, F.; Paglia, F.; Aprile, S.; Monici, A.; Tonna, M.; Conte, G.; Masini, F.; De Panfilis, C.; et al. Type D Personality in Never-Depressed Patients and the Development of Major and Minor Depression after Acute Coronary Syndrome. J. Affect. Disord. 2014, 155, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Marchesi, C.; Ossola, P.; Scagnelli, F.; Paglia, F.; Aprile, S.; Monici, A.; Tonna, M.; Conte, G.; Masini, F.; De Panfilis, C.; et al. Type D Personality in Never Depressed Patients at Their First Acute Coronary Syndrome. Psychother. Psychosom. 2014, 83, 190–191. [Google Scholar] [CrossRef]
- Ossola, P.; De Panfilis, C.; Tonna, M.; Ardissino, D.; Marchesi, C. DS14 Is More Likely to Measure Depression Rather than a Personality Disposition in Patients with Acute Coronary Syndrome. Scand. J. Psychol. 2015, 56, 685–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsboom, D.; Cramer, A.O.J. Network Analysis: An Integrative Approach to the Structure of Psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef] [Green Version]
- Costantini, G.; Epskamp, S.; Borsboom, D.; Perugini, M.; Mõttus, R.; Waldorp, L.J.; Cramer, A.O.J. State of the ARt Personality Research: A Tutorial on Network Analysis of Personality Data in R. J. Res. Personal. 2015, 54, 13–29. [Google Scholar] [CrossRef]
- Borsboom, D. A Network Theory of Mental Disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Hamm, C.W.; Bassand, J.P.; Agewall, S.; Bax, J.; Boersma, E.; Bueno, H.; Caso, P.; Dudek, D.; Gielen, S.; Huber, K.; et al. ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2011, 32, 2999–3054. [Google Scholar] [CrossRef] [PubMed]
- Van De Werf, F.; Bax, J.; Betriu, A.; Blomstrom-Lundqvist, C.; Crea, F.; Falk, V.; Filippatos, G.; Fox, K.; Huber, K.; Kastrati, A.; et al. Management of Acute Myocardial Infarction in Patients Presenting with Persistent ST-Segment Elevation. Eur. Heart J. 2008, 29, 2909–2945. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1974, 12, 189–198. [Google Scholar] [CrossRef]
- APA Diagnostic and Statistical Manual of Mental Disorders. Text Revision (DSM-IV-TR). In Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar] [CrossRef]
- Eagle, K.A.; Lim, M.J.; Dabbous, O.H.; Pieper, K.S.; Goldberg, R.J.; Goodman, S.G.; Granger, C.B.; Steg, P.G.; Gore, J.M.; Flather, M.D.; et al. A Validated Prediction Model for All Forms of Acute Coronary Syndrome Estimating the Risk of 6-Month Postdischarge Death in an International Registry. JAMA 2004, 291, 2727–2733. [Google Scholar] [CrossRef] [Green Version]
- Osler, M.; Mårtensson, S.; Wium-Andersen, I.K.; Prescott, E.; Andersen, P.K.; Jørgensen, T.S.H.; Carlsen, K.; Wium-Andersen, M.K.; Jørgensen, M.B. Depression After First Hospital Admission for Acute Coronary Syndrome: A Study of Time of Onset and Impact on Survival. Am. J. Epidemiol. 2016, 183, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Panchal, H.B.; Ladia, V.; Desai, S. A Meta-Analysis of Mortality and Major Adverse Cardiovascular and Cerebrovascular Events Following Transcatheter Aortic Valve Implantation Versus Surgical Aortic Valve Replacement for Severe Aortic Stenosis. Am. J. Cardiol. 2013, 112, 850–860. [Google Scholar] [CrossRef]
- Moise, N.; Khodneva, Y.; Jannat-khah, D.P.; Richman, J.; Davidson, K.W.; Kronish, I.M.; Shaffer, J.; Safford, M.M. Observational Study of the Differential Impact of Time-Varying Depressive Symptoms on All-Cause and Cause- Specific Mortality by Health Status in Community-Dwelling Adults: The REGARDS Study. BMJ Open 2018, 8, e017385. [Google Scholar] [CrossRef] [Green Version]
- Patti, G.; Cannon, C.P.; Murphy, S.A.; Mega, S.; Pasceri, V.; Briguori, C.; Colombo, A.; Yun, K.H.; Jeong, M.H.; Kim, J.S.; et al. Clinical Benefit of Statin Pretreatment in Patients Undergoing Percutaneous Coronary Intervention: A Collaborative Patient-Level Meta-Analysis of 13 Randomized Studies. Circulation 2011, 123, 1622–1632. [Google Scholar] [CrossRef] [Green Version]
- de Ron, J.; Robinaugh, D.J.; Fried, E.I.; Pedrelli, P.; Jain, F.A.; Mischoulon, D.; Epskamp, S. Quantifying and Addressing the Impact of Measurement Error in Network Models. Behav. Res. Ther. 2022, 157, 104163. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.P.; Garrido, L.E.; Golino, H. Unique Variable Analysis: A Network Psychometrics Method to Detect Local Dependence. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Golino, H.F.; Demetriou, A. Estimating the Dimensionality of Intelligence like Data Using Exploratory Graph Analysis. Intelligence 2017, 62, 54–70. [Google Scholar] [CrossRef]
- Belvederi Murri, M.; Grassi, L.; Caruso, R.; Nanni, M.G.; Zerbinati, L.; Andreas, S.; Ausín, B.; Canuto, A.; Härter, M.; Lopez, M.M.; et al. Depressive Symptom Complexes of Community-Dwelling Older Adults: A Latent Network Model. Mol. Psychiatry 2022, 27, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Golino, H.; Shi, D.; Garrido, L.E.; Christensen, A.; Nieto, M.D. Investigating the Performance of Exploratory Graph Analysis and Traditional Techniques to Identify the Number of Latent Factors: A Simulation and Tutorial. PsyArXiv 2018. [Google Scholar] [CrossRef] [Green Version]
- Golino, H.; Christensen, A.P.; Golino, H.; Christensen, A.P. EGAnet: Exploratory Graph Analysis: A Framework for Estimating the Number of Dimensions in Multivariate Data Using Network Psychometrics. Available online: https://cran.r-project.org/package=EGAnet (accessed on 20 September 2022).
- Christensen, A.P.; Golino, H. On the Equivalency of Factor and Network Loadings. Behav. Res. Methods 2021, 53, 1563–1580. [Google Scholar] [CrossRef] [PubMed]
- Golino, H.F.; Epskamp, S. Exploratory Graph Analysis: A New Approach for Estimating the Number of Dimensions in Psychological Research. PLoS ONE 2017, 12, e0174035. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.R.; Rast, P.; Pericchi, L.R.; Mulder, J. Comparing Gaussian Graphical Models With the Posterior Predictive Distribution and Bayesian Model Selection. Psychol. Methods 2020, 25, 653. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.; Mulder, J. BGGM: Bayesian Gaussian Graphical Models. J. Open Source Softw. 2020, 5, 2111. [Google Scholar] [CrossRef]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. Qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Zhang, B.; Guo, Y.; Zhang, J. The Association between Alexithymia as Assessed by the 20-Item Toronto Alexithymia Scale and Depression: A Meta-Analysis. Psychiatry Res. 2015, 227, 1–9. [Google Scholar] [CrossRef]
- Nekouei, Z.K.; Doost, H.T.; Yousefy, A.; Manshaee, G.; Sadeghei, M. The Relationship of Alexithymia with Anxiety-Depression-Stress, Quality of Life, and Social Support in Coronary Heart Disease (A Psychological Model). J. Educ. Health Promot. 2014, 3, 68. [Google Scholar] [CrossRef]
- van Dooren, F.E.P.; Verhey, F.R.J.; Pouwer, F.; Schalkwijk, C.G.; Sep, S.J.S.; Stehouwer, C.D.A.; Henry, R.M.A.; Dagnelie, P.C.; Schaper, N.C.; van der Kallen, C.J.H.; et al. Association of Type D Personality with Increased Vulnerability to Depression: Is There a Role for Inflammation or Endothelial Dysfunction?—The Maastricht Study. J. Affect. Disord. 2016, 189, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Lenzo, V.; Barberis, N.; Cannavò, M.; Filastro, A.; Verrastro, V.; Quattropani, M.C. The Relationship between Alexithymia, Defense Mechanisms, Eating Disorders, Anxiety and Depression. Riv. Di Psichiatr. 2020, 55, 24–30. [Google Scholar] [CrossRef]
- Mochcovitch, M.D.; Nardi, A.E.; Cardoso, A. Temperament and Character Dimensions and Their Relationship to Major Depression and Panic Disorder. Rev. Bras. De Psiquiatr. 2012, 34, 342–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajraktarov, S.; Gudeva-Nikovska, D.; ManuÅ¡eva, N.; Arsova, S. Personality Characteristics as Predictive Factors for the Occurrence of Depressive Disorder. Open Access Maced. J. Med. Sci. 2017, 5, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, P.T.P. Meaning-Seeking, Self-Transcendence, and Well-being. In Logotherapy and Existential Analysis: Proceedings of the Viktor Frankl Institute Vienna; Batthyány, A., Ed.; Springer: Cham, Switzerland, 2016; Volume 1. [Google Scholar] [CrossRef]
- Wong, P.T.P.; Mayer, C.-H.; Arslan, G. Editorial: COVID-19 and Existential Positive Psychology (PP2.0): The New Science of Self-Transcendence. Front. Psychol. 2021, 12, 5661. [Google Scholar] [CrossRef]
- Liu, P.; Wang, X.; Li, D.; Zhang, R.; Li, H.; Han, J. The Benefits of Self-Transcendence: Examining the Role of Values on Mental Health Among Adolescents Across Regions in China. Front. Psychol. 2021, 12, 630420. [Google Scholar] [CrossRef] [PubMed]
- Ellermann, C.R.; Reed, P.G. Self-Transcendence and Depression in Middle-Age Adults. West. J. Nurs. Res. 2001, 23, 698–713. [Google Scholar] [CrossRef] [PubMed]
- Ormel, J.; de Jonge, P. Unipolar Depression and the Progression of Coronary Artery Disease: Toward an Integrative Model. Psychother. Psychosom. 2011, 80, 264–274. [Google Scholar] [CrossRef] [Green Version]
- Dinga, R.; Marquand, A.F.; Veltman, D.J.; Beekman, A.T.F.; Schoevers, R.A.; van Hemert, A.M.; Penninx, B.W.J.H.; Schmaal, L. Predicting the Naturalistic Course of Depression from a Wide Range of Clinical, Psychological, and Biological Data: A Machine Learning Approach. Transl. Psychiatry 2018, 8, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horackova, K.; Kopecek, M.; Machů, V.; Kagstrom, A.; Aarsland, D.; Motlova, L.B.; Cermakova, P. Prevalence of Late-Life Depression and Gap in Mental Health Service Use across European Regions. Eur. Psychiatr. 2019, 57, 19–25. [Google Scholar] [CrossRef]
- Blazer, D.G. Depression in Late Life: Review and Commentary. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, M249–M265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hintsanen, M.; Pulkki-Råback, L.; Juonala, M.; Viikari, J.S.A.; Raitakari, O.T.; Keltikangas-Järvinen, L. Cloninger’s Temperament Traits and Preclinical Atherosclerosis: The Cardiovascular Risk in Young Finns Study. J. Psychosom. Res. 2009, 67, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Bezgin, C.H.; Bezgin, T.; Kesebir, S. Temperament and Character Profiles and Psychiatric Comorbidities in Patients With Coronary Artery or Valvular Heart Disease: Relationship With Cardiac Disease Severity. J. Clin. Med. Res. 2016, 8, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Lahat, A.; Benson, B.E.; Pine, D.S.; Fox, N.A.; Ernst, M. Neural Responses to Reward in Childhood: Relations to Early Behavioral Inhibition and Social Anxiety. Soc. Cogn. Affect. Neurosci. 2016, 13, nsw122. [Google Scholar] [CrossRef] [Green Version]
- Sher, L. Type D Personality: The Heart, Stress, and Cortisol. QJM: Int. J. Med. 2005, 98, 323–329. [Google Scholar] [CrossRef] [Green Version]
- Garcia, D.; Anckarsäter, H.; Lundström, S. Self-Directedness and Cooperativeness, Psychosocial Dysfunction and Suffering in ESSENCE. Sci. World J. 2013, 2013, 416981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steingrimsson, S.; Carlsen, H.K.; Lundström, E.; Lundström, S.; Nilsson, T. Problematic Alcohol and Drug Use Is Associated with Low Self-Directedness and Cooperativeness. Eur. Addict. Res. 2020, 26, 326–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Miranda Azevedo, R.; Roest, A.M.; Hoen, P.W.; de Jonge, P. Cognitive/Affective and Somatic/Affective Symptoms of Depression in Patients with Heart Disease and Their Association with Cardiovascular Prognosis: A Meta-Analysis. Psychol. Med. 2014, 44, 2689–2703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ossola, P.; Gerra, M.L.; De Panfilis, C.; Tonna, M.; Marchesi, C. Anxiety, Depression, and Cardiac Outcomes after a First Diagnosis of Acute Coronary Syndrome. Health Psychol. 2018, 37, 1115–1122. [Google Scholar] [CrossRef] [Green Version]
- Meyer, T.; Hussein, S.; Lange, H.W.; Herrmann-Lingen, C. Anxiety Is Associated with a Reduction in Both Mortality and Major Adverse Cardiovascular Events Five Years after Coronary Stenting. Eur. J. Prev. Cardiol. 2015, 22, 75–82. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 304 1 |
|---|---|
| Age | 61.43 (10.98) |
| Gender | |
| Female | 59 (19%) |
| Male | 245 (81%) |
| Education | 10.13 (3.75) |
| Marital status | |
| Single | 36 (12%) |
| In a relationship | 223 (73%) |
| Divorced | 24 (7.9%) |
| Widowed | 21 (6.9%) |
| Occupation | |
| Unemployed | 8 (2.6%) |
| Student | 0 (0%) |
| Housewife | 16 (5.3%) |
| Employed | 130 (43%) |
| Retired | 150 (49%) |
| Living | |
| Alone | 52 (17%) |
| Not alone | 252 (83%) |
| Family support | |
| Problematic | 3 (1.0%) |
| Fair | 36 (12%) |
| Good | 265 (87%) |
| Smoking | 93 (36%) |
| Past antidepressants | 1 (0.3%) |
| HADS Anxiety | 9.12 (5.13) |
| HADS Depression | 7.11 (4.22) |
| HADS total score | 16.24 (8.81) |
| PRIME MD total score | 2.87 (3.08) |
| PRIME MD PHQ total score | 15.07 (6.66) |
| TAS-20 DIF | 15.07 (5.73) |
| TAS-20 DDF | 13.02 (4.23) |
| TAS-20 EOT | 21.22 (4.30) |
| TCI Novelty-seeking (NS) | 17.58 (4.94) |
| TCI Harm avoidance (HA) | 15.91 (5.59) |
| TCI Reward dependence (RD) | 14.05 (3.21) |
| TCI Self-directedness (SD) | 29.50 (7.03) |
| TCI Cooperativeness (C) | 29.69 (5.74) |
| TCI Self-transcendence (ST) | 14.44 (5.69) |
| DS-14 Negative affectivity (NA) | 8.98 (6.00) |
| DS-14 Social inhibition (SI) | 10.21 (4.98) |
| DSQ-40 Mature | 5.00 (1.18) |
| DSQ-40 Neurotic | 4.14 (1.39) |
| DSQ-40 Immature | 3.97 (1.14) |
| Characteristic | No, N = 235 1 | Yes, N = 69 1 | p-Value 2 |
|---|---|---|---|
| Age | 61.16 (11.02) | 62.33 (10.86) | 0.359 |
| Gender | 0.022 * | ||
| Female | 39 (17%) | 20 (29%) | |
| Male | 196 (83%) | 49 (71%) | |
| Education | 10.16 (3.74) | 10.04 (3.79) | 0.878 |
| Marital status | 0.038 * | ||
| Single | 29 (12%) | 7 (10%) | |
| In a relationship | 178 (76%) | 45 (65%) | |
| Divorced | 17 (7.2%) | 7 (10%) | |
| Widowed | 11 (4.7%) | 10 (14%) | |
| Occupation | 0.159 | ||
| Unemployed | 6 (2.6%) | 2 (2.9%) | |
| Student | 0 (0%) | 0 (0%) | |
| Housewife | 9 (3.8%) | 7 (10%) | |
| Employed | 105 (45%) | 25 (36%) | |
| Retired | 115 (49%) | 35 (51%) | |
| Living | 0.024 * | ||
| Alone | 34 (14%) | 18 (26%) | |
| Not alone | 201 (86%) | 51 (74%) | |
| Family support | 0.030 * | ||
| Problematic | 2 (0.9%) | 1 (1.4%) | |
| Fair | 22 (9.4%) | 14 (20%) | |
| Good | 211 (90%) | 54 (78%) | |
| Smoking | 73 (36%) | 20 (36%) | 0.995 |
| Past depression | 0 (0%) | 0 (0%) | >0.999 |
| Past antidepressants | 0 (0%) | 1 (1.4%) | 0.227 |
| HADS Anxiety | 9.03 (5.31) | 9.46 (4.48) | 0.999 |
| HADS Depression | 6.75 (4.21) | 8.35 (4.04) | 0.003 * |
| HADS total score | 15.77 (9.05) | 17.81 (7.81) | 0.164 |
| PRIME MD total score | 2.19 (2.13) | 5.19 (4.43) | <0.001 * |
| PRIME MD PHQ total score | 14.54 (6.45) | 17.00 (7.09) | 0.004 * |
| TAS-20 DIF | 14.53 (5.55) | 16.90 (6.01) | 0.004 * |
| TAS-20 DDF | 12.87 (4.24) | 13.55 (4.21) | 0.159 |
| TAS-20 EOT | 21.18 (4.35) | 21.38 (4.18) | 0.820 |
| TCI Novelty-seeking (NS) | 17.16 (4.70) | 18.98 (5.47) | 0.013 * |
| TCI Harm avoidance (HA) | 15.11 (5.53) | 18.64 (4.92) | <0.001 * |
| TCI Reward dependence (RD) | 13.97 (3.24) | 14.34 (3.10) | 0.640 |
| TCI Self-directedness (SD) | 30.30 (6.92) | 26.80 (6.77) | <0.001 * |
| TCI Cooperativeness (C) | 30.15 (5.59) | 28.13 (6.00) | 0.019 * |
| TCI Self-transcendence (ST) | 14.20 (5.60) | 15.25 (5.94) | 0.298 |
| DS-14 Negative affectivity (NA) | 8.00 (5.33) | 12.33 (6.91) | <0.001 * |
| DS-14 Social inhibition (SI) | 9.60 (4.62) | 12.30 (5.62) | <0.001 * |
| DSQ-40 Mature | 5.00 (1.18) | 5.00 (1.18) | 0.784 |
| DSQ-40 Neurotic | 4.09 (1.41) | 4.31 (1.32) | 0.578 |
| DSQ-40 Immature | 3.90 (1.15) | 4.21 (1.09) | 0.062 |
| Characteristic | No, N = 247 1 | Yes, N = 57 1 | p-Value 2 |
|---|---|---|---|
| Age | 60.53 (11.19) | 65.32 (9.09) | 0.002 |
| Gender | 0.443 | ||
| Female | 50 (20%) | 9 (16%) | |
| Male | 197 (80%) | 48 (84%) | |
| Education | 10.26 (3.70) | 9.56 (3.92) | 0.172 |
| Marital status | 0.146 | ||
| Single | 33 (13%) | 3 (5.3%) | |
| In a relationship | 176 (71%) | 47 (82%) | |
| Divorced | 22 (8.9%) | 2 (3.5%) | |
| Widowed | 16 (6.5%) | 5 (8.8%) | |
| Occupation | 0.247 | ||
| Unemployed | 8 (3.2%) | 0 (0%) | |
| Student | 0 (0%) | 0 (0%) | |
| Housewife | 12 (4.9%) | 4 (7.0%) | |
| Employed | 110 (45%) | 20 (35%) | |
| Retired | 117 (47%) | 33 (58%) | |
| Living | 0.770 | ||
| Alone | 43 (17%) | 9 (16%) | |
| Not alone | 204 (83%) | 48 (84%) | |
| Family support | 0.906 | ||
| Problematic | 3 (1.2%) | 0 (0%) | |
| Fair | 30 (12%) | 6 (11%) | |
| Good | 214 (87%) | 51 (89%) | |
| Smoking | 76 (37%) | 17 (34%) | 0.703 |
| Past depression | 0 (0%) | 0 (0%) | >0.999 |
| Past antidepressants | 1 (0.4%) | 0 (0%) | >0.999 |
| HADS Anxiety | 9.04 (5.17) | 9.49 (4.94) | 0.640 |
| HADS Depression | 7.07 (4.26) | 7.30 (4.07) | 0.707 |
| HADS total score | 16.11 (8.93) | 16.79 (8.33) | 0.603 |
| PRIME MD total score | 2.80 (2.84) | 3.16 (3.98) | 0.521 |
| PRIME MD PHQ total score | 15.13 (6.80) | 14.82 (6.09) | 0.808 |
| TAS-20 DIF | 15.14 (5.76) | 14.77 (5.68) | 0.702 |
| TAS-20 DDF | 13.11 (4.31) | 12.67 (3.88) | 0.511 |
| TAS-20 EOT | 21.05 (4.33) | 21.98 (4.13) | 0.235 |
| TCI Novelty-seeking (NS) | 17.65 (4.81) | 17.28 (5.46) | 0.981 |
| TCI Harm avoidance (HA) | 16.10 (5.72) | 15.15 (5.02) | 0.326 |
| TCI Reward dependence (RD) | 14.33 (3.00) | 12.92 (3.78) | 0.011 |
| TCI Self-directedness (SD) | 29.37 (6.98) | 30.02 (7.27) | 0.344 |
| TCI Cooperativeness (C) | 29.98 (5.51) | 28.53 (6.53) | 0.189 |
| TCI Self-transcendence (ST) | 14.64 (5.53) | 13.60 (6.29) | 0.243 |
| DS-14 Negative affectivity (NA) | 8.90 (6.09) | 9.33 (5.64) | 0.515 |
| DS-14 Social inhibition (SI) | 10.09 (4.92) | 10.74 (5.27) | 0.259 |
| DSQ-40 Mature | 5.00 (1.18) | 5.00 (1.17) | 0.973 |
| DSQ-40 Neurotic | 4.14 (1.33) | 4.14 (1.63) | 0.962 |
| DSQ-40 Immature | 3.95 (1.14) | 4.02 (1.16) | 0.594 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Folesani, F.; Luviè, L.; Palazzi, C.; Marchesi, C.; Rossi, R.; Belvederi Murri, M.; Ossola, P. Psychopathology, Personality and Depression after Acute Coronary Syndrome: A Network Analysis in an Italian Population. Diagnostics 2023, 13, 915. https://doi.org/10.3390/diagnostics13050915
Folesani F, Luviè L, Palazzi C, Marchesi C, Rossi R, Belvederi Murri M, Ossola P. Psychopathology, Personality and Depression after Acute Coronary Syndrome: A Network Analysis in an Italian Population. Diagnostics. 2023; 13(5):915. https://doi.org/10.3390/diagnostics13050915
Chicago/Turabian StyleFolesani, Federica, Lorenzo Luviè, Cristina Palazzi, Carlo Marchesi, Rodolfo Rossi, Martino Belvederi Murri, and Paolo Ossola. 2023. "Psychopathology, Personality and Depression after Acute Coronary Syndrome: A Network Analysis in an Italian Population" Diagnostics 13, no. 5: 915. https://doi.org/10.3390/diagnostics13050915