
Assessment of COVID-19 Molecular Testing Capacity in Jordan: A Cross-Sectional Study at the Country Level

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. General Description of the Participating Laboratories
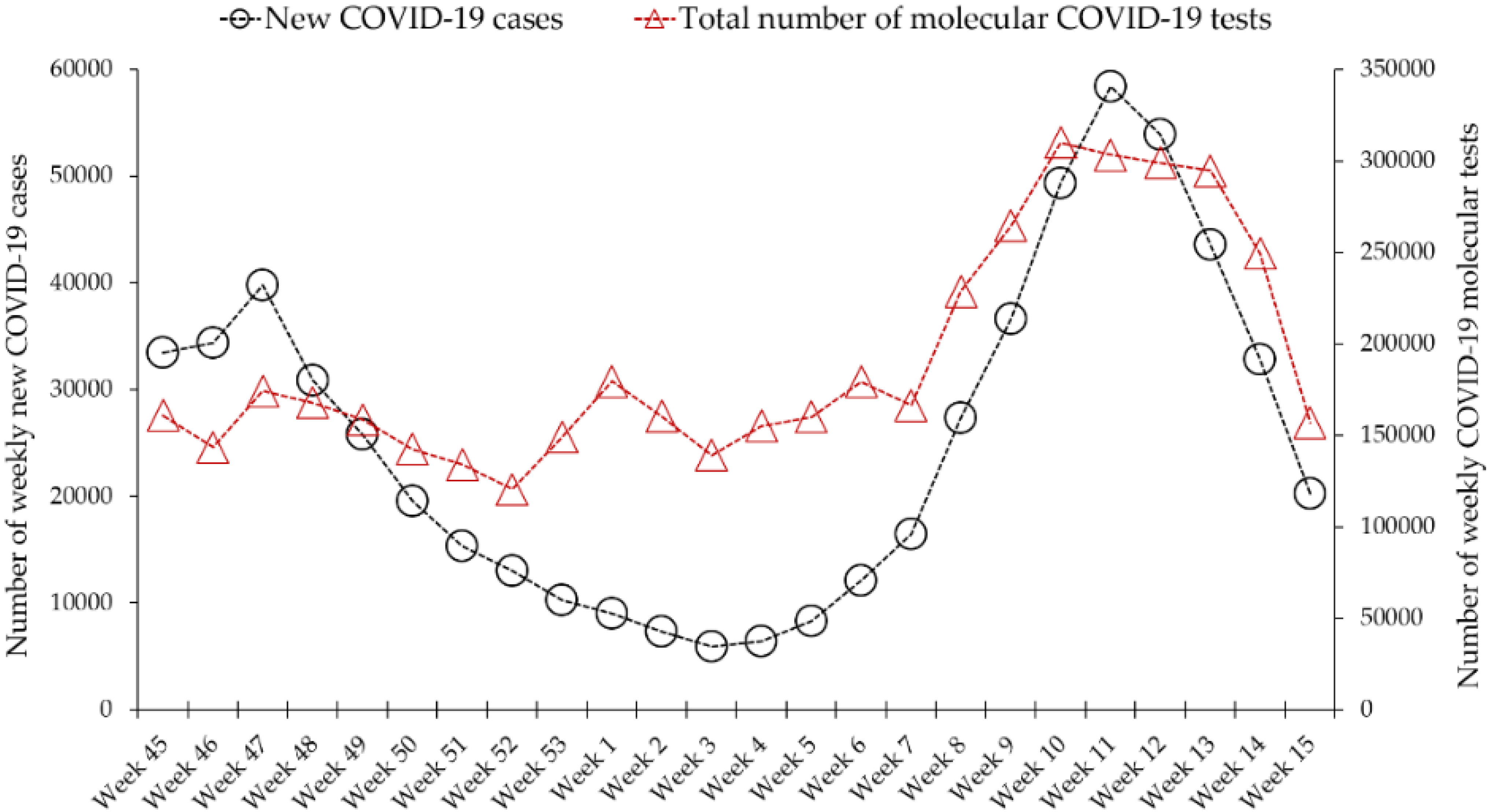
3.2. Assessment of the Total Number of Weekly COVID-19 qPCR Tests in Jordan during the Peaks of the First and Second Waves of COVID-19
3.3. National Average Daily COVID-19 Tests Increased from 225 Tests per 100,000 People in November 2020 to 349 Tests per 100,000 in April 2021
3.4. Daily and Weekly COVID-19 Testing Parameters among the Participating Laboratories in April 2021
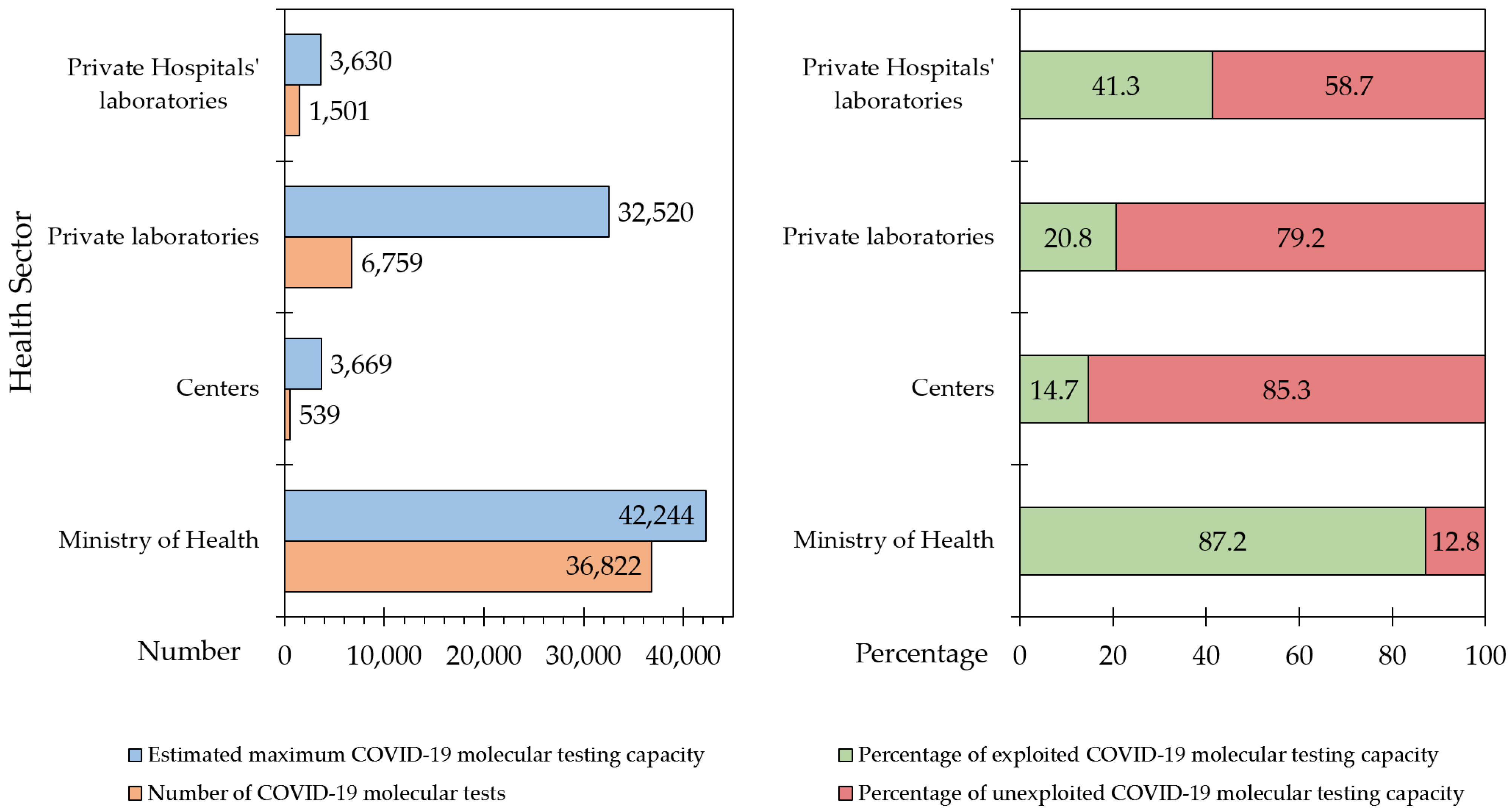
3.5. Estimated Maximum COVID-19 Testing Capacity in Jordan
3.6. Potential Factors Limiting the Utilization of Maximum COVID-19 Molecular Testing Capacity in Jordan
3.7. Factors Affecting the Average Daily COVID-19 Molecular Tests Performed in Jordan
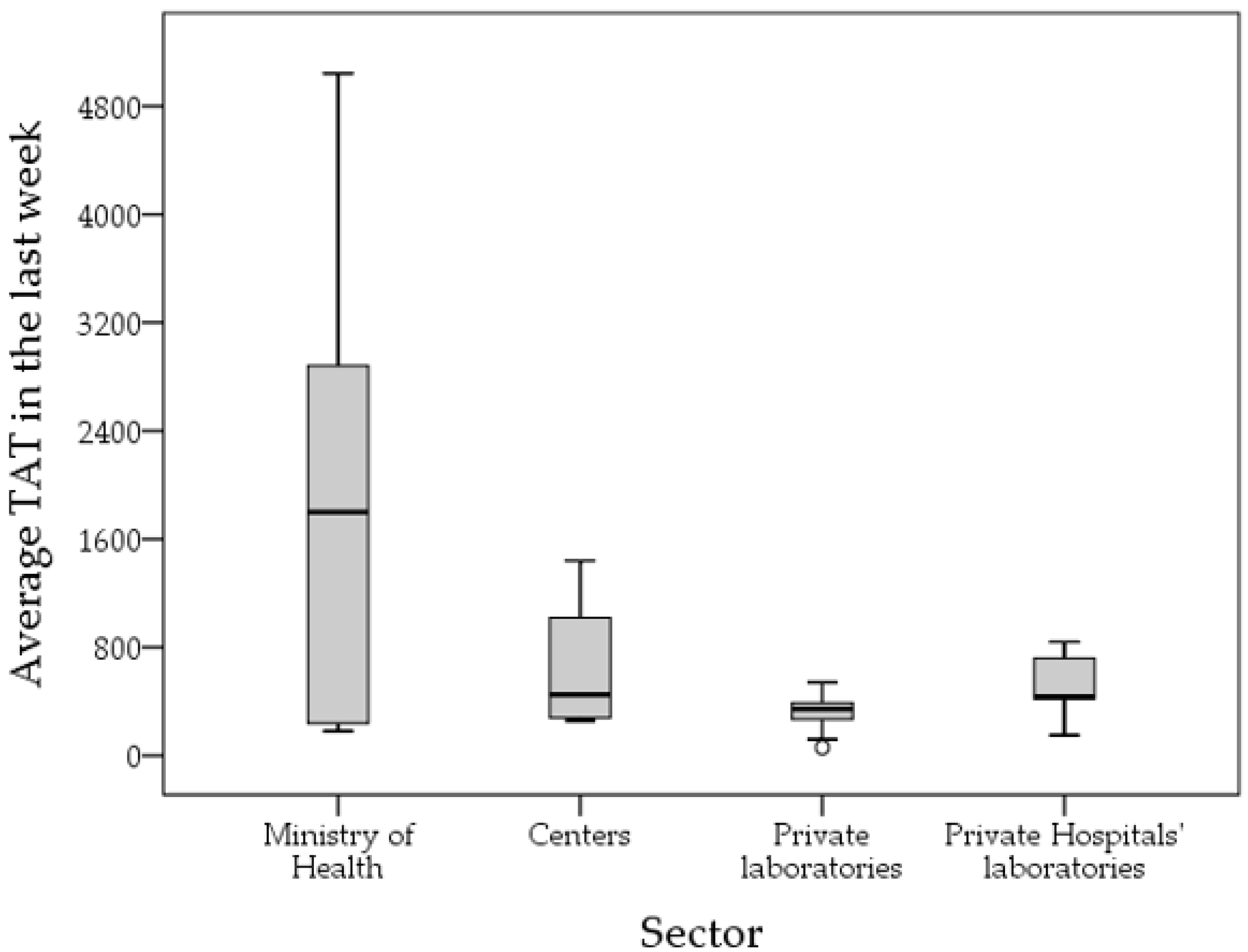
3.8. Descriptive Statistics of TAT for COVID-19 Testing in Jordan
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The World Health Organization (WHO). Laboratory Testing Strategy Recommendations for COVID-19. Available online: https://apps.who.int/iris/bitstream/handle/10665/331509/WHO-COVID-19-lab_testing-2020.1-eng.pdf (accessed on 24 April 2021).
- WHO Director. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—16 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---16-march-2020 (accessed on 18 September 2021).
- Bohn, M.K.; Mancini, N.; Loh, T.P.; Wang, C.B.; Grimmler, M.; Gramegna, M.; Yuen, K.Y.; Mueller, R.; Koch, D.; Sethi, S.; et al. IFCC Interim Guidelines on Molecular Testing of SARS-CoV-2 Infection. Clin. Chem. Lab. Med. 2020, 58, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- Touma, M. COVID-19: Molecular diagnostics overview. J. Mol. Med. 2020, 98, 947–954. [Google Scholar] [CrossRef]
- Bustin, S.; Mueller, R.; Shipley, G.; Nolan, T. COVID-19 and Diagnostic Testing for SARS-CoV-2 by RT-qPCR—Facts and Fallacies. Int. J. Mol. Sci. 2021, 22, 2459. [Google Scholar] [CrossRef] [PubMed]
- Vandenberg, O.; Martiny, D.; Rochas, O.; van Belkum, A.; Kozlakidis, Z. Considerations for diagnostic COVID-19 tests. Nat. Rev. Microbiol. 2021, 19, 171–183. [Google Scholar] [CrossRef]
- Arnaout, R.; Lee, R.A.; Lee, G.R.; Callahan, C.; Cheng, A.; Yen, C.F.; Smith, K.P.; Arora, R.; Kirby, J.E. The Limit of Detection Matters: The Case for Benchmarking Severe Acute Respiratory Syndrome Coronavirus 2 Testing. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e3042–e3046. [Google Scholar] [CrossRef] [PubMed]
- Kanji, J.N.; Zelyas, N.; MacDonald, C.; Pabbaraju, K.; Khan, M.N.; Prasad, A.; Hu, J.; Diggle, M.; Berenger, B.M.; Tipples, G. False negative rate of COVID-19 PCR testing: A discordant testing analysis. Virol. J. 2021, 18, 13. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Monitoring and Evaluation Framework for COVID-19 Response Activities in the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-framework-monitor-responses.pdf (accessed on 24 April 2021).
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef]
- Sichone, J.; Sinkala, M.; Munsaka, S.; Kikonko, M.; Simuunza, M. Assessing required SARS-CoV-2 blanket testing rates for possible control of the outbreak in the epicentre Lusaka province of Zambia with consideration for asymptomatic individuals: A simple mathematical modelling study. PLoS ONE 2021, 16, e0249479. [Google Scholar] [CrossRef]
- Beeching, N.J.; Fletcher, T.E.; Beadsworth, M.B.J. COVID-19: Testing times. BMJ 2020, 369, m1403. [Google Scholar] [CrossRef] [Green Version]
- Lopes-Júnior, L.C.; Bomfim, E.; Silveira, D.S.C.D.; Pessanha, R.M.; Schuab, S.I.P.C.; Lima, R.A.G. Effectiveness of mass testing for control of COVID-19: A systematic review protocol. BMJ Open 2020, 10, e040413. [Google Scholar] [CrossRef]
- Du, Z.; Pandey, A.; Bai, Y.; Fitzpatrick, M.C.; Chinazzi, M.; Pastore y Piontti, A.; Lachmann, M.; Vespignani, A.; Cowling, B.J.; Galvani, A.P.; et al. Comparative cost-effectiveness of SARS-CoV-2 testing strategies in the USA: A modelling study. Lancet Public Health 2021, 6, e184–e191. [Google Scholar] [CrossRef]
- Dighe, A.; Cattarino, L.; Cuomo-Dannenburg, G.; Skarp, J.; Imai, N.; Bhatia, S.; Gaythorpe, K.A.M.; Ainslie, K.E.C.; Baguelin, M.; Bhatt, S.; et al. Response to COVID-19 in South Korea and implications for lifting stringent interventions. BMC Med. 2020, 18, 321. [Google Scholar] [CrossRef] [PubMed]
- Chien, L.-C.; Beÿ, C.K.; Koenig, K.L. Taiwan’s Successful COVID-19 Mitigation and Containment Strategy: Achieving Quasi Population Immunity. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, F.; Cui, J.; Peng, Z.; Chang, Z.; Lai, S.; Chen, Q.; Wang, L.; Gao, G.F.; Feng, Z. Comprehensive large-scale nucleic acid–testing strategies support China’s sustained containment of COVID-19. Nat. Med. 2021, 27, 740–742. [Google Scholar] [CrossRef]
- Cleevely, M.; Susskind, D.; Vines, D.; Vines, L.; Wills, S. A workable strategy for COVID-19 testing: Stratified periodic testing rather than universal random testing. Oxf. Rev. Econ. Policy 2020, 36 (Suppl. 1), S14–S37. [Google Scholar] [CrossRef]
- Mbwogge, M. Mass Testing with Contact Tracing Compared to Test and Trace for the Effective Suppression of COVID-19 in the United Kingdom: Systematic Review. JMIRx Med. 2021, 2, e27254. [Google Scholar] [CrossRef]
- Cirakli, U.; Dogan, I.; Gozlu, M. The Relationship between COVID-19 Cases and COVID-19 Testing: A Panel Data Analysis on OECD Countries. J. Knowl. Econ. 2021, 1–14. [Google Scholar] [CrossRef]
- The World Health Organization (WHO). COVID-19 Strategy Update. Available online: https://www.who.int/docs/default-source/coronaviruse/covid-strategy-update-14april2020.pdf (accessed on 24 April 2021).
- World Health Organization (WHO). Recommendations for National SARS-CoV-2 Testing Strategies and Diagnostic Capacities. Available online: https://apps.who.int/iris/bitstream/handle/10665/342002/WHO-2019-nCoV-lab-testing-2021.1-eng.pdf?sequence=1&isAllowed=y (accessed on 19 September 2021).
- Kroft, S.H. Well-Being, Burnout, and the Clinical Laboratory. Am. J. Clin. Pathol. 2020, 153, 422–424. [Google Scholar] [CrossRef]
- Rowan, N.J.; Laffey, J.G. Challenges and solutions for addressing critical shortage of supply chain for personal and protective equipment (PPE) arising from Coronavirus disease (COVID19) pandemic—Case study from the Republic of Ireland. Sci. Total Environ. 2020, 725, 138532. [Google Scholar] [CrossRef]
- Yuan, D.; Gao, W.; Liang, S.; Yang, S.; Jia, P. Biosafety threats of the rapidly established labs for SARS-CoV-2 tests in China. Environ. Int. 2020, 143, 105964. [Google Scholar] [CrossRef]
- Hendarwan, H.; Syachroni, S.; Aryastami, N.K.; Su’udi, A.; Susilawati, M.D.; Despitasari, M.; Mulyani, U.A.; Sumiarsih, M.; Puspandari, N.; Indrati, A.R. Assessing the COVID-19 diagnostic laboratory capacity in Indonesia in the early phase of the pandemic. WHO South-East Asia J. Public Health 2020, 9, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Al-Tammemi, A.B. The Battle against COVID-19 in Jordan: An Early Overview of the Jordanian Experience. Front. Public Health 2020, 8, 188. [Google Scholar] [CrossRef]
- Sallam, M.; Mahafzah, A. Molecular Analysis of SARS-CoV-2 Genetic Lineages in Jordan: Tracking the Introduction and Spread of COVID-19 UK Variant of Concern at a Country Level. Pathogens 2021, 10, 302. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Taim, D.; Eid, H.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. COVID-19 misinformation: Mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS ONE 2020, 15, e0243264. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Listings of WHO’s Response to COVID-19. Available online: https://www.who.int/news/item/29-06-2020-covidtimeline (accessed on 14 February 2022).
- Our World in Data. Jordan: Coronavirus Pandemic Country Profile. Available online: https://ourworldindata.org/coronavirus/country/jordan (accessed on 23 April 2021).
- Madhav, N.; Oppenheim, B.; Gallivan, M.; Mulembakani, P.; Rubin, E.; Wolfe, N. Pandemics: Risks, impacts, and mitigation. In Disease Control Priorities: Improving Health and Reducing Poverty; Jamison, D.T.G.H., Horton, S., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2018. [Google Scholar]
- Okeke, I.N.; Ihekweazu, C. The importance of molecular diagnostics for infectious diseases in low-resource settings. Nat. Rev. Microbiol. 2021, 19, 547–548. [Google Scholar] [CrossRef]
- Ramadan, N.; Shaib, H. Middle East respiratory syndrome coronavirus (MERS-CoV): A review. Germs 2019, 9, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Walker, P.G.T.; Whittaker, C.; Watson, O.J.; Baguelin, M.; Winskill, P.; Hamlet, A.; Djafaara, B.A.; Cucunubá, Z.; Olivera Mesa, D.; Green, W.; et al. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science 2020, 369, 413–422. [Google Scholar] [CrossRef]
- Eurosurveillance Editorial, T. Updated rapid risk assessment from ECDC on coronavirus disease 2019 (COVID-19) pandemic: Increased transmission in the EU/EEA and the UK. Euro Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2020, 25, 2003121. [Google Scholar] [CrossRef]
- Kebede, A.; Lanyero, B.; Beyene, B.; Mandalia, M.L.; Melese, D.; Girmachew, F.; Mekonnen, A.; Ayana, G.; Yemanebirhan, N.; Hailu, G.; et al. Expanding molecular diagnostic capacity for COVID-19 in Ethiopia: Operational implications, challenges and lessons learnt. Pan Afr. Med. J. 2021, 38, 68. [Google Scholar] [CrossRef] [PubMed]
- Abera, A.; Belay, H.; Zewude, A.; Gidey, B.; Nega, D.; Dufera, B.; Abebe, A.; Endriyas, T.; Getachew, B.; Birhanu, H.; et al. Establishment of COVID-19 testing laboratory in resource-limited settings: Challenges and prospects reported from Ethiopia. Glob. Health Action 2020, 13, 1841963. [Google Scholar] [CrossRef]
- Aisyah, D.N.; Mayadewi, C.A.; Igusti, G.; Manikam, L.; Adisasmito, W.; Kozlakidis, Z. Laboratory Readiness and Response for SARS-CoV-2 in Indonesia. Front. Public Health 2021, 9, 705031. [Google Scholar] [CrossRef] [PubMed]
- Chatzimanolakis, M.; Weber, P.; Arampatzis, G.; Wälchli, D.; Kičić, I.; Karnakov, P.; Papadimitriou, C.; Koumoutsakos, P. Optimal allocation of limited test resources for the quantification of COVID-19 infections. Swiss. Med. Wkly. 2020, 150, w20445. [Google Scholar] [CrossRef]
- Acheampong, G.; Owusu, M.; Nkrumah, B.; Obeng-Boadi, P.; Opare, D.A.; Sambian, D.J.; Angra, P.; Walker, C. Laboratory capacity in COVID-19 diagnosis and the need to enhance molecular testing in Ghana. Glob. Secur. Health Sci. Policy 2021, 6, 10–17. [Google Scholar] [CrossRef]
- Jayamohan, H.; Lambert, C.J.; Sant, H.J.; Jafek, A.; Patel, D.; Feng, H.; Beeman, M.; Mahmood, T.; Nze, U.; Gale, B.K. SARS-CoV-2 pandemic: A review of molecular diagnostic tools including sample collection and commercial response with associated advantages and limitations. Anal. Bioanal. Chem. 2021, 413, 49–71. [Google Scholar] [CrossRef] [PubMed]
- Mardian, Y.; Kosasih, H.; Karyana, M.; Neal, A.; Lau, C.-Y. Review of Current COVID-19 Diagnostics and Opportunities for Further Development. Front. Med. 2021, 8, 562. [Google Scholar] [CrossRef]
- Farooq, M.U.; Hussain, A.; Masood, T.; Habib, M.S. Supply Chain Operations Management in Pandemics: A State-of-the-Art Review Inspired by COVID-19. Sustainability 2021, 13, 2504. [Google Scholar] [CrossRef]
- Okeke, I.N.; Feasey, N.; Parkhill, J.; Turner, P.; Limmathurotsakul, D.; Georgiou, P.; Holmes, A.; Peacock, S.J. Leapfrogging laboratories: The promise and pitfalls of high-tech solutions for antimicrobial resistance surveillance in low-income settings. BMJ Glob. Health 2020, 5, e003622. [Google Scholar] [CrossRef]
- Hu, Y. Regulatory concern of polymerase chain reaction (PCR) carryover contamination. In Polymerase Chain Reaction for Biomedical Applications; IntechOpen: London, UK, 2016; pp. 57–68. [Google Scholar]
- Mögling, R.; Meijer, A.; Berginc, N.; Bruisten, S.; Charrel, R.; Coutard, B.; Eckerle, I.; Enouf, V.; Hungnes, O.; Korukluoglu, G.; et al. Delayed Laboratory Response to COVID-19 Caused by Molecular Diagnostic Contamination. Emerg. Infect. Dis. 2020, 26, 1944–1946. [Google Scholar] [CrossRef]
- Braunstein, G.D.; Schwartz, L.; Hymel, P.; Fielding, J. False Positive Results with SARS-CoV-2 RT-PCR Tests and How to Evaluate a RT-PCR-Positive Test for the Possibility of a False Positive Result. J. Occup. Environ. Med. 2021, 63, e159–e162. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, I.; Alidjinou, E.K.; Ogiez, J.; Pagneux, Q.; Miloudi, S.; Benhalima, I.; Ouafi, M.; Sane, F.; Hober, D.; Roussel, A.; et al. Preanalytical Issues and Cycle Threshold Values in SARS-CoV-2 Real-Time RT-PCR Testing: Should Test Results Include These? ACS Omega 2021, 6, 6528–6536. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Bhatnagar, T.; Rade, K.; Murhekar, M.; Gangakhedkar, R.R.; Nagar, A. Strategic planning to augment the testing capacity for COVID-19 in India. Indian J. Med. Res. 2020, 151, 210–215. [Google Scholar] [CrossRef]
- Mishra, D.K.; Goel, G.; Arora, N.; Krishnan, S.; Bhattacharya, S.; Mathur, P.; Walia, K.; Chandy, M. The importance of intra- and inter-institutional networks for capacity building in severe acute respiratory syndrome coronavirus 2 reverse transcription polymerase chain reaction services: Experience from an oncology centre in eastern India. Indian J. Med. Microbiol. 2020, 38, 9–17. [Google Scholar] [CrossRef]
- Umaru, F.A. Scaling up testing for COVID-19 in Africa: Responding to the pandemic in ways that strengthen health systems. Afr. J. Lab. Med. 2020, 9, 1244. [Google Scholar] [CrossRef] [PubMed]
- Badrick, T.; Wienholt, L.; Fone, D.; Holzhauser, D. The challenge of producing an EQA for the COVID-19 pandemic. Pract. Lab. Med. 2020, 22, e00179. [Google Scholar] [CrossRef] [PubMed]
- Torres, I.; Sippy, R.; Sacoto, F. Assessing critical gaps in COVID-19 testing capacity: The case of delayed results in Ecuador. BMC Public Health 2021, 21, 637. [Google Scholar] [CrossRef]
- Luo, Y.; Wang, J.; Zhang, M.; Wang, Q.; Chen, R.; Wang, X.; Wang, H. COVID-19-another influential event impacts on laboratory medicine management. J. Clin. Lab. Anal. 2021, 35, e23804. [Google Scholar] [CrossRef]
- Leite, J.A.; Gresh, L.; Vicari, A.; Gabastou, J.M.; Perez, E.; Aldighieri, S.; Network, S.l.; Mendez-Rico, J. COVID-19 laboratory preparedness and response in the Americas Region: Lessons learned. PLoS ONE 2021, 16, e0253334. [Google Scholar] [CrossRef]
- Rubin, R. The Challenges of Expanding Rapid Tests to Curb COVID-19. JAMA 2020, 324, 1813–1815. [Google Scholar] [CrossRef]
- El Hage, J.; Gravitt, P.; Ravel, J.; Lahrichi, N.; Gralla, E. Supporting scale-up of COVID-19 RT-PCR testing processes with discrete event simulation. PLoS ONE 2021, 16, e0255214. [Google Scholar] [CrossRef] [PubMed]
- Julie, A.D.; Christopher, A.B.; John, R.F.; Rahul, S.; Jane, E.; Molly, T.; Nancy, T.M.; Hannah, D.; Thomas, H.; Oona, D.; et al. An iteratively optimised process for improving the efficiency and effectiveness of an industrial SARS-CoV-2 diagnostic facility. Res. Sq. 2021, 1–22. [Google Scholar] [CrossRef]
- Smyrlaki, I.; Ekman, M.; Lentini, A.; Rufino de Sousa, N.; Papanicolaou, N.; Vondracek, M.; Aarum, J.; Safari, H.; Muradrasoli, S.; Rothfuchs, A.G.; et al. Massive and rapid COVID-19 testing is feasible by extraction-free SARS-CoV-2 RT-PCR. Nat. Commun. 2020, 11, 4812. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Center | North | South |
|---|---|---|---|
| Health sector | n 1 (%) | n (%) | n (%) |
| Ministry of Health | 7 (19.4) | 5 (50.0) | 5 (100.0) |
| University/research/specialized center | 2 (5.6) | 2 (20.0) | 0 |
| Private laboratories | 17 (47.2) | 3 (30.0) | 0 |
| Private hospital laboratories | 10 (27.8) | 0 | 0 |
| Health Sector | Descriptive Statistics | Staff Number |
|---|---|---|
| Ministry of Health | n 1 | 17 |
| Mean, median | 8, 5 | |
| Range | 2–42 | |
| IQR 2 | 4–8 | |
| University/research/specialized center | n | 4 |
| Mean, median | 8, 8 | |
| Range | 4–13 | |
| IQR | 5–12 | |
| Private laboratories | n | 20 |
| Mean, median | 17, 4 | |
| Range | 2–207 | |
| IQR | 3–12 | |
| Private Hospital laboratories | n | 10 |
| Mean, median | 5, 4 | |
| Range | 2–13 | |
| IQR | 3–5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qaqish, B.; Sallam, M.; Al-Khateeb, M.; Reisdorf, E.; Mahafzah, A. Assessment of COVID-19 Molecular Testing Capacity in Jordan: A Cross-Sectional Study at the Country Level. Diagnostics 2022, 12, 909. https://doi.org/10.3390/diagnostics12040909
Qaqish B, Sallam M, Al-Khateeb M, Reisdorf E, Mahafzah A. Assessment of COVID-19 Molecular Testing Capacity in Jordan: A Cross-Sectional Study at the Country Level. Diagnostics. 2022; 12(4):909. https://doi.org/10.3390/diagnostics12040909
Chicago/Turabian StyleQaqish, Bara’a, Malik Sallam, Maysa Al-Khateeb, Erik Reisdorf, and Azmi Mahafzah. 2022. "Assessment of COVID-19 Molecular Testing Capacity in Jordan: A Cross-Sectional Study at the Country Level" Diagnostics 12, no. 4: 909. https://doi.org/10.3390/diagnostics12040909