
A Robust, Fully Automatic Detection Method and Calculation Technique of Midline Shift in Intracranial Hemorrhage and Its Clinical Application

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Population
2.2. Neural Network Based Automatic Measurement of the Midline Shift
3. Results
3.1. General Characteristics of the Included Patients
3.2. Midline Shift Measurement by Different Methods
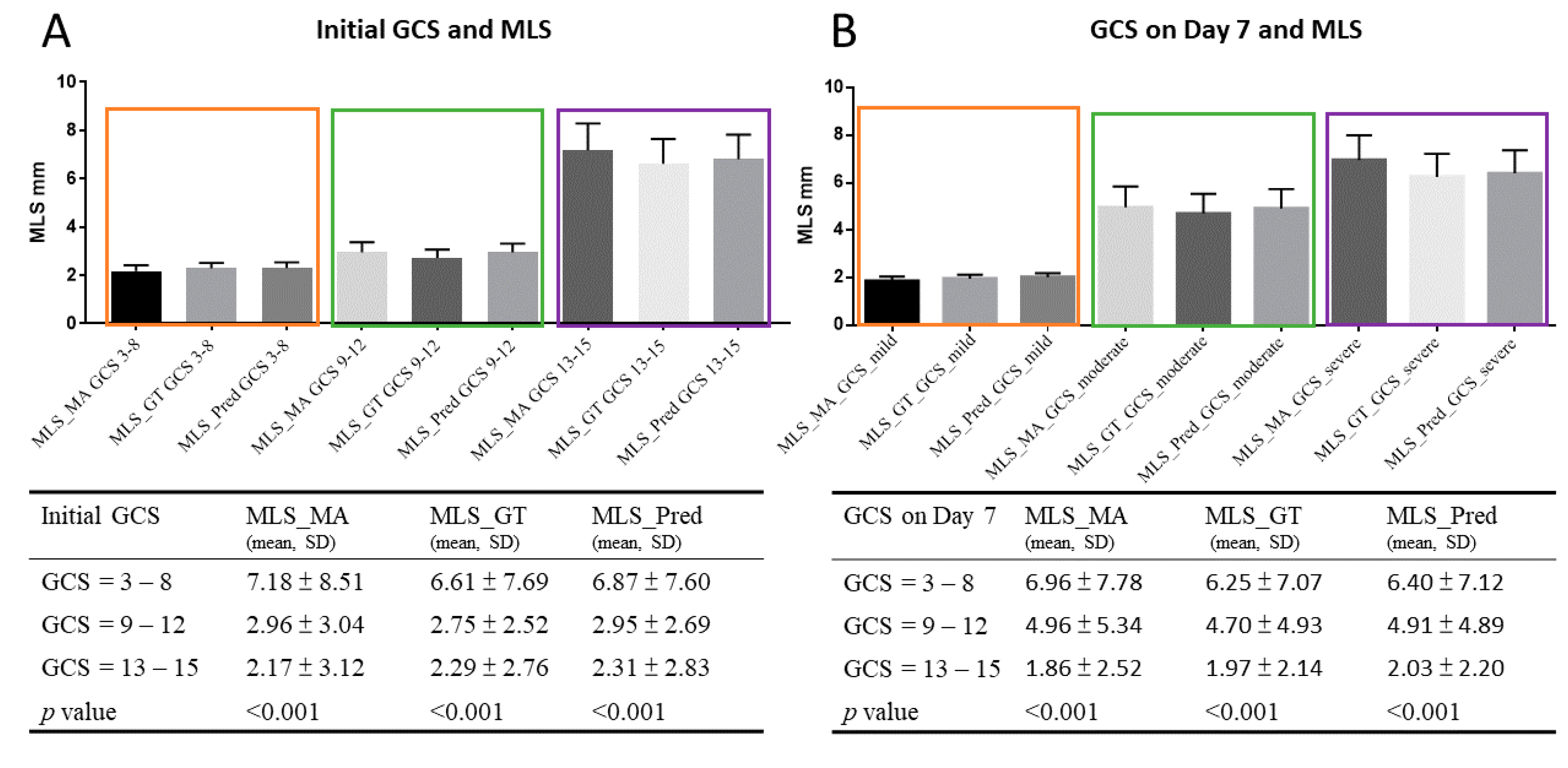
3.3. Midline Shift and Clinical Outcomes
3.4. ROC for Detection of Mortality, Bad Outcomes and Low GCSs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sallam, A.; Abdelaal Ahmed Mahmoud, M.A.A.; Kamel, M.G.; Hamza, M.K.; Yassin, H.M.; Hosny, H.; Younis, M.I.; Ramadan, E.; Algameel, H.Z.; Abdelhaq, M.; et al. The Diagnostic Accuracy of Noninvasive Methods to Measure the Intracranial Pressure: A Systematic Review and Meta-analysis. Anesth. Analg. 2021, 132, 686–695. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.C.; Chen, Y.F.; Xiao, F. Brain Midline Shift Measurement and Its Automation: A Review of Techniques and Algorithms. Int. J. Biomed. Imaging 2018, 2018, 4303161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, L.F.; Toole, B.M.; Bowers, S.A. The National Traumatic Coma Data Bank. Part 2: Patients who talk and deteriorate: Implications for treatment. J. Neurosurg. 1983, 59, 285–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, B.; Beems, T.; van der Vliet, T.M.; Diaz-Arrastia, R.R.; Borm, G.F.; Vos, P.E. Computed tomography and outcome in moderate and severe traumatic brain injury: Hematoma volume and midline shift revisited. J. Neurotrauma 2011, 28, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Bullock, M.R.; Chesnut, R.; Ghajar, J.; Gordon, D.; Hartl, R.; Newell, D.W.; Servadei, F.; Walters, B.C.; Wilberger, J.; Surgical Management of Traumatic Brain Injury Author Group. Surgical management of traumatic parenchymal lesions. Neurosurgery 2006, 58, S25–S46. [Google Scholar] [CrossRef] [PubMed]
- Appendix II: Evaluation of Relevant Computed Tomographic Scan Findings. Neurosurgery 2006, 58, S2–S62. [CrossRef]
- Bhattathiri, P.S.; Gregson, B.; Prasad, K.S.; Mitchell, P.; Soh, C.; Mitra, D.; Gholkar, A.; Mendelow, A.D. Reliability assessment of computerized tomography scanning measurements in intracerebral hematoma. Neurosurg. Focus 2003, 15, E6. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.C.; Xiao, F.; Wong, J.M.; Chiang, I.J. Automatic recognition of midline shift on brain CT images. Comput. Biol. Med. 2010, 40, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Belle, A.; Cockrell, C.; Ward, K.R.; Najarian, K. Automated midline shift and intracranial pressure estimation based on brain CT images. J. Vis. Exp. 2013, 13, 3871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.; Li, S.; Su, B.; Tan, C.L.; Leong, T.Y.; Pang, B.C.; Lim, C.C.; Lee, C.K. Automatic detection and quantification of brain midline shift using anatomical marker model. Comput. Med. Imaging Graph 2014, 38, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards Real-Time Object Detection with Region Proposal Networks. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 1137–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, K.; Gkioxari, G.; Dollar, P.; Girshick, R. Mask R-CNN. IEEE Trans. Pattern Anal. Mach. Intell. 2020, 42, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yu, H. Convolutional Neural Network Based Metal Artifact Reduction in X-ray Computed Tomography. IEEE Trans. Med. Imaging 2018, 37, 1370–1381. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.Y.; Maire, M.; Belongie, S.; Bourdev, L.; Girshick, R.; Hays, J.; Perona, P.; Zitnick, C.L.; Dollár, P. Microsoft COCO: Common Objects in Context. arXiv 2015, arXiv:1405.0312. Available online: https://cocodataset.org/ (accessed on 21 February 2015).
- Jain, S.; Vyvere, T.V.; Terzopoulos, V.; Sima, D.M.; Roura, E.; Maas, A.; Wilms, G.; Verheyden, J. Automatic Quantification of Computed Tomography Features in Acute Traumatic Brain Injury. J. Neurotrauma 2019, 36, 1794–1803. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.I.; Hukkelhoven, C.W.; Marshall, L.F.; Steyerberg, E.W. Prediction of outcome in traumatic brain injury with computed tomographic characteristics: A comparison between the computed tomographic classification and combinations of computed tomographic predictors. Neurosurgery 2005, 57, 1173–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.S.; Li, Q.; Li, R.; Liu, Q.J.; Wang, X.C.; Zhao, L.B.; Xie, P. Defining the Optimal Midline Shift Threshold to Predict Poor Outcome in Patients with Supratentorial Spontaneous Intracerebral Hemorrhage. Neurocrit. Care 2018, 28, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Puffer, R.C.; Yue, J.K.; Mesley, M.; Billigen, J.B.; Sharpless, J.; Fetzick, A.L.; Puccio, A.; Diaz-Arrastia, R.; Okonkwo, D.O. Long-term outcome in traumatic brain injury patients with midline shift: A secondary analysis of the Phase 3 COBRIT clinical trial. J. Neurosurg. 2018, 131, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Xiao, F.; Liao, C.C.; Huang, K.C.; Chiang, I.J.; Wong, J.M. Automated assessment of midline shift in head injury patients. Clin. Neurol. Neurosurg. 2010, 112, 785–790. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Number | 300 | |
| CT scan (slices) | 7269 | |
| Age (mean ± SD, range) | 48.1 ± 15.1 | |
| Types of hemorrhage * | ICH | 153 |
| Acute SDH | 90 | |
| Chronic SDH | 55 | |
| EDH | 5 | |
| IVH | 53 | |
| SAH | 115 | |
| Surgical cases | 93 | |
| ICP insertion | 61 | |
| Initial GCS | 3–8 | 67 |
| 9–13 | 74 | |
| 14–15 | 159 | |
| GCS day 7 | 3–8 | 60 |
| 9–13 | 60 | |
| 14–15 | 172 | |
| GOS score day 30 | 1 | 44 |
| 2 | 32 | |
| 3 | 69 | |
| 4 | 141 | |
| 5 | 10 | |
| Positive pupil reflex, initial | Right (+/−) | 244/36 |
| Left (+/−) | 245/41 | |
| ICP, day 0 (cmH2O, mean ± SD, range) | 18.1 ± 7.9, 0–30 | |
| ICP, day 3 (cmH2O, mean ± SD, range) | 8.9 ± 9.3, 0–70 | |
| Cause of Intracranial Hemoprrhage | ||
|---|---|---|
| Intraparenchymal Hemorrhage | 153 | |
| Trauma | 43 | |
| Spontaneous | 80 | |
| Secondary * | 21 | |
| Postoperative | 9 | |
| Acute Subdural hematoma (ASDH) | 90 | |
| Trauma | 68 | |
| Secondary * | 18 | |
| Postoperative | 4 | |
| Subarachnoid Hemorrhage (SAH) | 115 | |
| Traumatic | 72 | |
| Nontraumatic ** | 43 | |
| Chronic subdural hematoma (CSDH) | 55 | |
| Traumatic | 43 | |
| Nontraumatic *** | 12 | |
| Epidural hemorrhage | 5 | |
| Intraventricular hemorrhage | 53 | |
| MLS MA * | MLS R * | MLS RA * | MLS GT # | MLS Predict # | |
|---|---|---|---|---|---|
| Slices | 300 | 300 | 300 | 6456 | 7570 |
| Mean (mm) | 3.387 | 3.683 | 3.639 | 3.383 | 3.384 |
| Median | 1.300 | 0.0 | 2.000 | 1.490 | 1.520 |
| Max | 29.00 | 32.00 | 29.10 | 25.43 | 24.49 |
| Min | 0.0 | 0.0 | 0.0 | 0.166 | 0.1987 |
| SD | 5.154 | 5.752 | 5.224 | 4.670 | 4.512 |
| Mean of MAE + | 0.213 | 0.936 | |||
| Max of MAE | 6.227 | 6.038 | |||
| CI95 Diff | 2.819–3.955 | 3.050–4.317 | 3.062–4.216 | 2.854–3.913 | 2.872–3.897 |
| Threshold (mm) | Sensitivity | Specificity | |
|---|---|---|---|
| Train | 2 | 89.7% | 72.7% |
| Valid | 2 | 87.5% | 85.7% |
| Test | 2 | 91.7% | 80.0% |
| Train | 5 | 94.0% | 96.5% |
| Valid | 5 | 94.1% | 92.9% |
| Test | 5 | 87.5% | 96.7% |
| Train | 10 | 84.6% | 98.5% |
| Valid | 10 | 83.3% | 96.0% |
| Test | 10 | 85.7% | 97.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, J.-L.; Chen, Y.-L.; Chen, M.-Y.; Chen, B.-A.; Chang, J.-X.; Kao, C.-C.; Hsieh, M.-C.; Peng, Y.-T.; Huang, K.-C.; Chen, P.-Y. A Robust, Fully Automatic Detection Method and Calculation Technique of Midline Shift in Intracranial Hemorrhage and Its Clinical Application. Diagnostics 2022, 12, 693. https://doi.org/10.3390/diagnostics12030693
Yan J-L, Chen Y-L, Chen M-Y, Chen B-A, Chang J-X, Kao C-C, Hsieh M-C, Peng Y-T, Huang K-C, Chen P-Y. A Robust, Fully Automatic Detection Method and Calculation Technique of Midline Shift in Intracranial Hemorrhage and Its Clinical Application. Diagnostics. 2022; 12(3):693. https://doi.org/10.3390/diagnostics12030693
Chicago/Turabian StyleYan, Jiun-Lin, Yao-Lian Chen, Moa-Yu Chen, Bo-An Chen, Jiung-Xian Chang, Ching-Chung Kao, Meng-Chi Hsieh, Yi-Ting Peng, Kuan-Chieh Huang, and Pin-Yuan Chen. 2022. "A Robust, Fully Automatic Detection Method and Calculation Technique of Midline Shift in Intracranial Hemorrhage and Its Clinical Application" Diagnostics 12, no. 3: 693. https://doi.org/10.3390/diagnostics12030693