
Imaging Review of Pelvic Ring Fractures and Its Complications in High-Energy Trauma

 , , ,
, , ,
Abstract
:1. Introduction
2. Epidemiology of Pelvic Trauma
3. Relevant Anatomy and Biomechanics of the Bony Pelvis
4. Classification of Pelvic Ring Fractures
4.1. Pennal Classification
- Anterior–posterior compression.
- Lateral compression.
- Vertical shear.
4.2. Tile Classification
- Type A fractures are stable because the posterior arch of the pelvic ring is intact.
- Type B fractures have rotational instability, but they are vertically stable, due to an incomplete disruption of the posterior arch structures.
- Type C fractures are vertically and rotationally unstable, and they are characterized by a complete disruption of the anterior and posterior arches.
4.3. Young and Burgess Classification
4.3.1. Lateral Compression
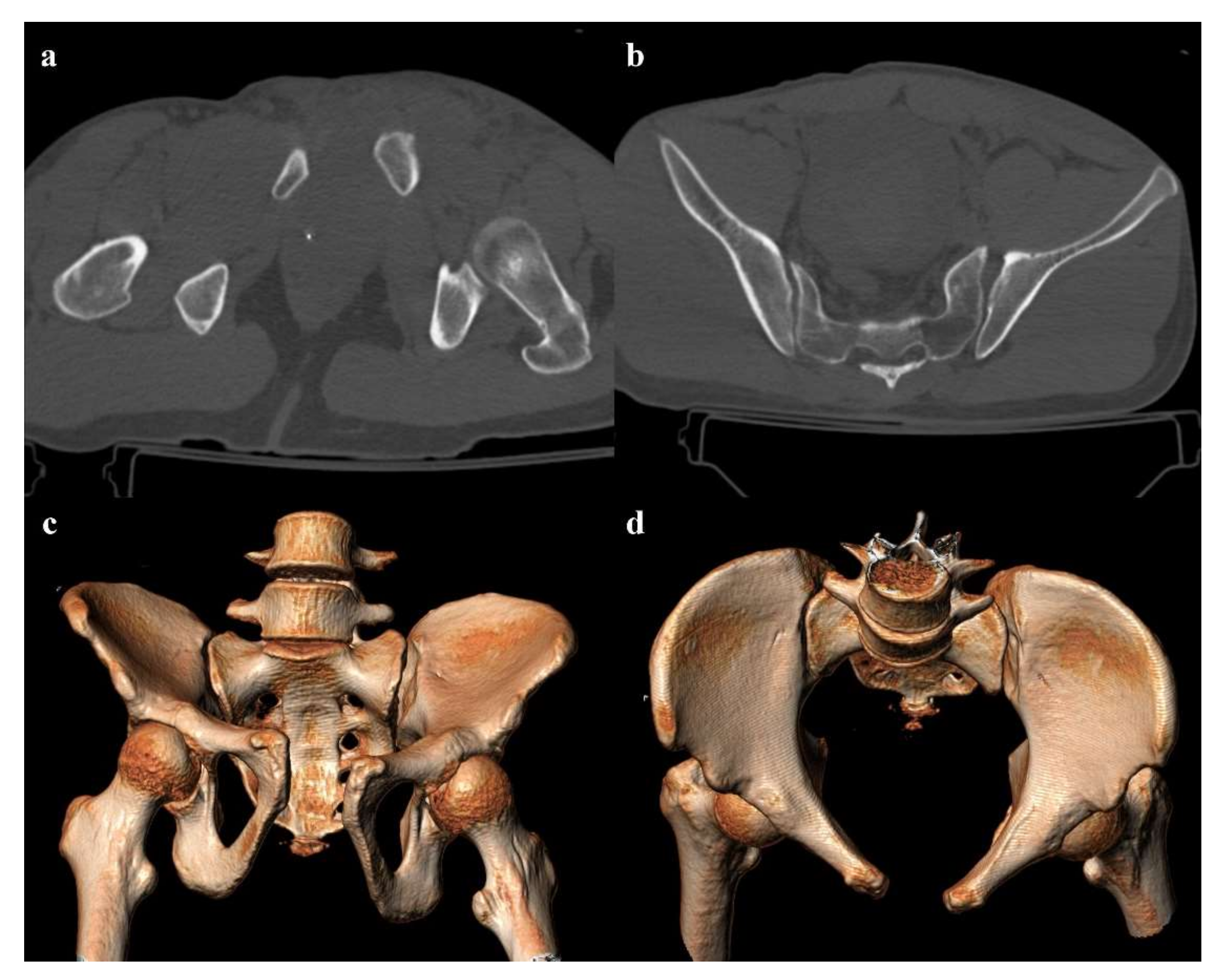
- Grade 3: the lateral compression force is associated with a contralateral anteroposterior compression force, with an external rotation of the contralateral hemipelvis (“windswept pelvis”). Grade 1 or grade 2 lateral compression injuries are associated with a contralateral sacroiliac joint diastasis (Figure 3). Lateral compression grade 3 injuries have a multidirectional instability and require a stable internal fixation [3]. In these lesions, an adjunctive temporary external fixation is useful [3].
4.3.2. Anterior–Posterior Compression
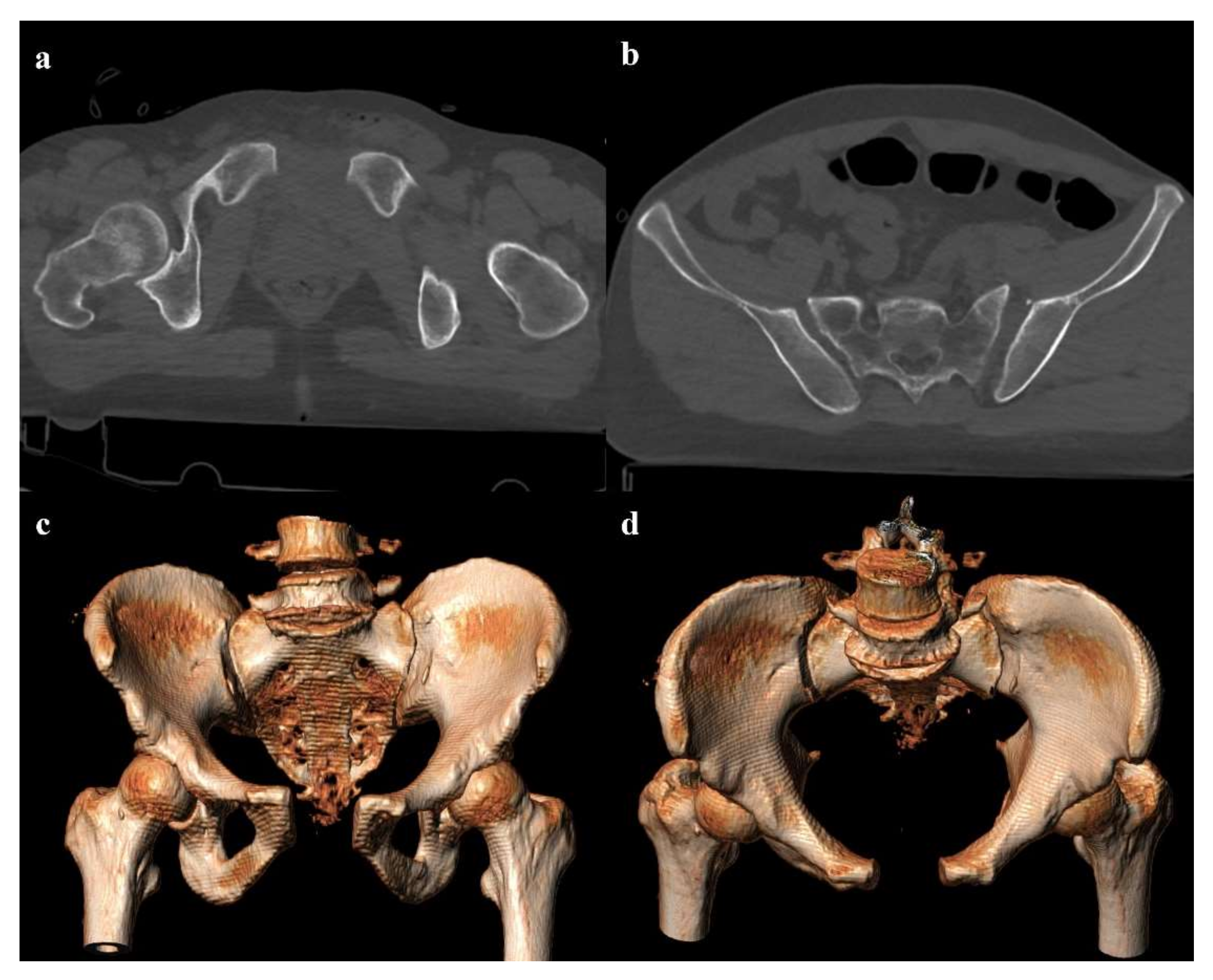
- Grade 2: pubic symphysis diastasis >2.5 cm, possible vertical fracture of the pubic rami, and anterior sacroiliac joint diastasis (Figure 5). The anterior sacroiliac joint diastasis is due to the rupture of the anterior sacroiliac ligament, sacrospinous ligament, and sacrotuberous ligament. Anterior–posterior compression grade 2 injuries have a rotational instability and require a stable internal fixation [3].
4.3.3. Vertical Shear
4.3.4. Combined Mechanism
4.4. Sacral Fractures
- Zone I: the fracture is located in the sacral wing, lateral to the neuroforamina (Figure 2). In 6% of cases, there is an impingement of L5 or S1 nerve root.
- Zone II: the fracture involves the neuroforamina (Figure 1). In 28% of cases, there is an ipsilateral neurological deficit.
- Zone III: the fracture is medial to the neuroforamina and involves the central canal. A combined fracture in this zone may have different morphology (“H”-shaped, “U”-shaped, “λ”-shaped, “T”-shaped), and can result in a spinopelvic dissociation (Figure 8). Zone III fractures can also be divided into four additional groups: anterior angulation of the fracture without dislocation (type 1), anterior angulation of the fracture with retrolisthesis (type 2), complete anterolisthesis of the fracture fragments (type 3), and comminuted fracture of S1 or S2 (type 4) [22]. In zone III fractures, there is a neurological injury in 56% of cases, with bowel and genitourinary dysfunction [8].
- Type A: an injury of lower sacrococcygeal spine, below the level of the sacroiliac joint. These fractures have no impact on the spinopelvic stability.
- Type B: a posterior pelvic fracture, characterized by a unilateral vertical sacral fracture. In these fractures, the posterior pelvic stability may be compromised.
- Type C: spinopelvic fractures, which are unstable.
5. Imaging Evaluation
6. Vascular and Visceral Complications
6.1. Vascular Complications
6.2. Bladder and Urethral Complications
6.3. Testicular Complications
6.4. Nervous Complications
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grotz, M.R.W.; Allami, M.K.; Harwood, P.; Pape, H.C.; Krettek, C.; Giannoudis, P.V. Open pelvic fractures: Epidemiology, current concepts of management and outcome. Injury 2005, 36, 1–13. [Google Scholar] [CrossRef]
- Magnone, S.; Coccolini, F.; Manfredi, R.; Piazzalunga, D.; Agazzi, R.; Arici, C.; Barozzi, M.; Bellanova, G.; Belluati, A.; Berlot, G.; et al. Management of hemodynamically unstable pelvic trauma: Results of the first Italian consensus conference (cooperative guidelines of the Italian Society of Surgery, the Italian Association of Hospital Surgeons, the Multi-specialist Italian Society of Young Surgeons, the Italian Society of Emergency Surgery and Trauma, the Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care, the Italian Society of Orthopaedics and Traumatology, the Italian Society of Emergency Medicine, the Italian Society of Medical Radiology -Section of Vascular and Interventional Radiology- and the World Society of Emergency Surgery). World. J. Emerg. Surg. 2014, 9, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Coccolini, F.; Stahel, P.F.; Montori, G.; Biffl, W.; Horer, T.M.; Catena, F.; Kluger, Y.; Moore, E.E.; Peitzman, A.B.; Ivatury, R.; et al. Pelvic trauma: WSES classification and guidelines. World J. Emerg Surg. 2017, 12, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormak, R.; Strauss, E.J.; Alwatter, B.J.; Tejwani, N.C. Diagnosis and management of pelvic fractures. Bull. NYU Hosp. Jt. Dis. 2010, 68, 281–291. [Google Scholar]
- Yoshihara, H.; Yoneoka, D. Demographic epidemiology of unstable pelvic fracture in the United States from 2000 to 2009: Trends and in-hospital mortality. J. Trauma Acute Care Surg. 2014, 76, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, R.; Scott, A.N.; Tonnos, F.; Hudson, I.; Martin, A.J.; Sethi, A. Patients with pelvic fractures from blunt trauma. What is the cause of mortality and when? Am. J. Surg. 2016, 211, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Trainham, L.; Rizzolo, D.; Diwan, A.; Lucas, T. Emergency management of high-energy pelvic trauma. JAAPA 2015, 28, 28–33. [Google Scholar] [CrossRef]
- Galluzzo, M.; Gaudino, F.; Addeo, G.; Buquicchio, G.L.; Danti, G.; Trinci, M.; Miele, V. Pelvic trauma: Bone. In Diagnostic Imaging in Polytrauma Patients; Miele, V., Trinci, M., Eds.; Springer International Publishing AG: Cham, Switzerland, 2018; pp. 433–460. [Google Scholar]
- Gamble, J.G.; Simmons, S.C.; Freedman, M. The symphysis pubis. Anatomic and pathologic considerations. Clin. Orthop. Relat. Res. 1986, 203, 261–272. [Google Scholar] [CrossRef]
- Becker, I.; Woodley, S.J.; Stringer, M.D. The adult human pubic symphysis: A systematic review. J. Anat. 2010, 217, 475–487. [Google Scholar] [CrossRef]
- Vleeming, A.; Schuenke, M.D.; Masi, A.T.; Carreiro, J.E.; Danneels, L.; Willard, F.H. The sacroiliac joint: An overview of its anatomy, function and potential clinical implications. J. Anat. 2012, 221, 537–567. [Google Scholar] [CrossRef] [PubMed]
- Durkin, A.; Sagi, H.C.; Durham, R.; Flint, L. Contemporary management of pelvic fractures. Am. J. Surg. 2006, 192, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Stambaugh, L.E., III; Blackmore, C.C. Pelvic ring disruptions in emergency radiology. Eur. J. Radiol. 2003, 48, 71–87. [Google Scholar] [CrossRef]
- Khurana, B.; Sheehan, S.E.; Sodickson, A.D.; Weaver, M.J. Pelvic ring fractures: What the orthopedic surgeon wants to know. Radiographics 2014, 34, 1317–1333. [Google Scholar] [CrossRef] [PubMed]
- Stahel, P.F.; Hammerberg, E.M. History of pelvic fracture management: A review. World J. Emerg. Surg. 2016, 11, 18. [Google Scholar] [CrossRef] [Green Version]
- Kurylo, J.C.; Tornetta, P., III. Initial management and classification of pelvic fractures. Instr. Course Lect. 2012, 61, 3–18. [Google Scholar]
- Pennal, G.F.; Tile, M.; Waddell, J.P.; Garside, H. Pelvic disruption: Assessment and classification. Clin. Orthop. Relat. Res. 1980, 151, 12–21. [Google Scholar] [CrossRef]
- Tile, M. Acute pelvis fractures: I. Causation and classification. J. Am. Acad. Orthop. Surg. 1996, 4, 14314–14315. [Google Scholar] [CrossRef] [PubMed]
- Burgess, A.R.; Eastridge, B.J.; Young, J.W.; Ellison, T.S.; Ellison, P.S., Jr.; Bathon, G.H.; Brumback, R.J. Pelvic ring disruptions: Effective classification system and treatment protocols. J. Trauma 1990, 30, 848–856. [Google Scholar] [CrossRef]
- Young, J.W.; Resnik, C.S. Fractures of the pelvis: Current concepts of classification. AJR Am. J. Roentgenol. 1990, 155, 1169–1175. [Google Scholar] [CrossRef]
- Langford, J.R.; Burgess, A.R.; Liporace, F.A.; Haidukewych, G.J. Pelvic fractures: Part 2. Contemporary indications and techniques for definitive surgical management. J. Am. Acad. Orthop. Surg. 2013, 21, 458–468. [Google Scholar] [CrossRef]
- Beckmann, N.; Cai, C. CT characteristics of traumatic sacral fractures in association with pelvic ring injuries: Correlation using the Young-Burgess classification system. Emerg. Radiol. 2017, 24, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Denis, F.; Davis, S.; Comfort, T. Sacral fractures: An important problem. Retrospective analysis of 236 cases. Clin. Orthop. Relat. Res. 1988, 227, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Slater, S.J.; Barron, D.A. Pelvic fractures—A guide to classification and management. Eur. J. Radiol. 2010, 74, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, A.R.; Schroeder, G.D.; Divi, S.N.; Kepler, C.K.; Kleweno, C.P.; Krieg, J.C.; Wilson, J.R.; Holstein, J.H.; Kurd, M.F.; Firoozabadi, R.; et al. Description and reliability of the AOSpine sacral classification system. J. Bone Jt. Surg. Am. 2020, 102, 1454–1463. [Google Scholar] [CrossRef]
- Daffner, R.H.; Sciulli, R.L. CT-guided iliosacral screw placement. Semin. Musculoskelet Radiol. 2013, 17, 407–415. [Google Scholar] [CrossRef]
- Ianniello, S.; di Giacomo, V.; Sessa, B.; Miele, V. First-line sonographic diagnosis of pneumothorax in major trauma: Accuracy of e-FAST and comparison with multidetector computed tomography. Radiol. Med. 2014, 119, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.R.; McGahan, J.P. Focused assessment with sonography in trauma (FAST) in 2017: What radiologists can learn. Radiology 2017, 283, 30–48. [Google Scholar] [CrossRef]
- Ianniello, S.; Piccolo, C.L.; Trinci, M.; Ajmone Cat, C.A.; Miele, V. Extended-FAST plus MDCT in pneumothorax diagnosis of major trauma: Time to revisit ATLS imaging approach? J. Ultrasound 2019, 22, 461–469. [Google Scholar] [CrossRef]
- Christian, N.T.; Burlew, C.C.; Moore, E.E.; Geddes, A.E.; Wagenaar, A.E.; Fox, C.J.; Pieracci, F.M. The focused abdominal sonography for trauma examination can reliably identify patients with significant intra-abdominal hemorrhage in life-threatening pelvic fractures. J. Trauma Acute Care Surg. 2018, 84, 924–928. [Google Scholar] [CrossRef]
- Chaijareenont, C.; Krutsri, C.; Sumpritpradit, P.; Singhatas, P.; Thampongsa, T.; Lertsithichai, P.; Choikrua, P.; Poprom, N. FAST accuracy in major pelvic fractures for decision-making of abdominal exploration: Systematic review and meta-analysis. Ann. Med. Surg. 2020, 60, 175–181. [Google Scholar] [CrossRef]
- Bauman, M.; Marinaro, J.; Tawil, I.; Crandall, C.; Rosenbaum, L.; Paul, I. Ultrasonographic determination of pubic symphyseal widening in trauma: The FAST-PS study. J. Emerg. Med. 2011, 40, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Ianniello, S.; Conte, P.; di Serafino, M.; Miele, V.; Trinci, M.; Vallone, G.; Galluzzo, M. Diagnostic accuracy of pubic symphysis ultrasound in the detection of unstable pelvis in polytrauma patients during e-FAST: The value of FAST–PLUS protocol. A preliminary experience. J. Ultrasound 2021, 24, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Galluzzo, M.; Miele, V. Traumi del bacino. In Diagnostica per Immagini nel Trauma Maggiore; Miele, V., Scaglione, M., Grassi, R., Rotondo, A., Eds.; Elsevier Editore: Milano, Italy, 2010; pp. 231–240. [Google Scholar]
- Paydar, S.; Ghaffarpasand, F.; Foroughi, M.; Saberi, A.; Dehghankhalili, M.; Abbasi, H.; Malekpoor, B.; Bananzadeh, A.M.; Vahid Hosseini, M.; Bolandparvaz, S. Role of routine pelvic radiography in initial evaluation of stable, high-energy, blunt trauma patients. Emerg. Med. J. 2013, 30, 724–727. [Google Scholar] [CrossRef] [PubMed]
- Resnik, C.S.; Stackhouse, D.J.; Shanmuganathan, K.; Young, J.W. Diagnosis of pelvic fractures in patients with acute pelvic trauma: Efficacy of plain radiographs. AJR Am. J. Roentgenol. 1992, 158, 109–112. [Google Scholar] [CrossRef]
- Mohseni, S.; Talving, P.; Kobayashi, L.; Lam, L.; Inaba, K.; Branco, B.C.; Oliver, M.; Dematriades, D. The diagnostic accuracy of 64-slice computed tomography in detecting clinically significant arterial bleeding after pelvic fractures. Am. Surg. 2011, 77, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Wright, A.; Cline, M.; Mazza, M.B.; Alves, T.; Chong, S. Pelvic fractures and associated genitourinary and vascular injuries: A multisystem review of pelvic trauma. AJR Am. J. Roentgenol. 2019, 213, 1297–1306. [Google Scholar] [CrossRef]
- Chaumòitre, K.; Portier, F.; Petit, P.; Merrot, T.; Guillon, P.O.; Panuel, M. CT imaging of pelvic injuries in polytrauma patients. J. Radiol. 2000, 81, 111–122. [Google Scholar]
- Giannecchini, S.; Caturano, V.; Rende, C.; Valentini, V.; Trinci, M.; Miele, V. Pelvic trauma: Vascular/visceral. In Diagnostic Imaging in Polytrauma Patients; Miele, V., Trinci, M., Eds.; Springer International Publishing Publishing AG: Cham, Switzerland, 2018; pp. 461–474. [Google Scholar]
- Ben-Menachem, Y.; Coldwell, D.M.; Young, J.W.; Burgess, A.R. Hemorrhage associated with pelvic fractures: Causes, diagnosis, and emergent management. AJR Am. J. Roentgenol. 1991, 157, 1005–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romano, L.; Pinto, A.; Niola, R.; Stavolo, C.; Cinque, T.; Daniele, S.; Scuderi, M.G.; Gagliardi, N. Bleeding due to pelvic fractures in female patients: Pictorial review of multidetector computed tomography imaging. Curr. Probl. Diagn. Radiol. 2012, 41, 83–92. [Google Scholar] [CrossRef]
- Gänsslen, A.; Giannoudis, P.; Pape, H.C. Hemorrhage in pelvic fracture: Who needs angiography? Curr. Opin. Crit. Care 2003, 9, 515–523. [Google Scholar] [CrossRef]
- Dreizin, D.; Bodanapally, U.; Boscak, A.; Tirada, N.; Issa, G.; Nascone, J.W.; Bivona, L.; Mascarenhas, D.; O’Toole, R.V.; Nixon, E.; et al. CT prediction model for major arterial injury after blunt pelvic ring disruption. Radiology 2018, 287, 1061–1069. [Google Scholar] [CrossRef]
- Tanizaki, S.; Maeda, S.; Ishida, H.; Yamamoto, T.; Yoshikawa, J. Clinical characteristics of external iliac artery branch injury in pelvic trauma. Am. J. Emerg. Med. 2017, 35, 1636–1638. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.C.; Wu, C.H.; Chen, H.W.; Wang, L.J.; Wong, Y.C. Predictors of active arterial hemorrhage on angiography in pelvic fracture patients. Jpn J. Radiol. 2018, 36, 223–230. [Google Scholar] [CrossRef]
- Raniga, S.B.; Mittal, A.K.; Bernstein, M.; Skalski, M.R.; Al-Hadidi, A.M. Multidetector CT in vascular injuries resulting from pelvic fractures: A primer for diagnostic radiologists. Radiographics 2019, 39, 2111–2129. [Google Scholar] [CrossRef]
- Magnussen, R.A.; Tressler, M.A.; Obremskey, W.T.; Kregor, P.J. Predicting blood loss in isolated pelvic and acetabular high-energy trauma. J. Orthop. Trauma 2007, 21, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Agolini, S.F.; Shah, K.; Jaffe, J.; Newcomb, J.; Rhodes, M.; Reed, J.F., III. Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J. Trauma 1997, 43, 395–399. [Google Scholar] [CrossRef]
- Borror, W.; Gaski, G.E.; Steenburg, S. Abdominopelvic bleed rate on admission CT correlates with mortality and transfusion needs in the setting of blunt pelvic fractures: A single institution pilot study. Emerg. Radiol. 2019, 26, 37–44. [Google Scholar] [CrossRef]
- Yoon, W.; Kim, J.K.; Jeong, Y.Y.; Seo, J.J.; Park, J.G.; Kang, H.K. Pelvic arterial hemorrhage in patients with pelvic fractures: Detection with contrast-enhanced CT. Radiographics 2004, 24, 1591–1605. [Google Scholar] [CrossRef] [PubMed]
- Baghdanian, A.H.; Armetta, A.S.; Baghdanian, A.; LeBedis, C.A.; Anderson, S.W.; Soto, J.A. CT of major vascular injury in blunt abdominopelvic trauma. Radiographics 2016, 36, 872–890. [Google Scholar] [CrossRef]
- Kertesz, J.L.; Anderson, S.W.; Murakami, A.M.; Pieroni, S.; Rhea, J.T.; Soto, J.A. Detection of vascular injuries in patients with blunt pelvic trauma by using 64-channel multidetector CT. Radiographics 2009, 29, 151–164. [Google Scholar] [CrossRef]
- Fishman, E.K.; Horton, K.M.; Johnson, P.T. Multidetector CT and three-dimensional CT angiography for suspected vascular trauma of the extremities. Radiographics 2008, 28, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, F.; Ierardi, A.M.; Mazzei, M.A.; Magenta Biasina, A.; Carrafiello, G.; Nicola, R.; Scaglione, M. Dual-phase CT for the assessment of acute vascular injuries in high-energy blunt trauma: The imaging findings and management implications. Br. J. Radiol. 2016, 89, 20150952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjurlin, M.A.; Fantus, R.J.; Mellett, M.M.; Goble, S.M. Genitourinary injuries in pelvic fracture morbidity and mortality using the National Trauma Data Bank. J. Trauma 2009, 67, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Basta, A.M.; Blackmore, C.C.; Wessells, H. Predicting urethral injury from pelvic fracture patterns in male patients with blunt trauma. J. Urol. 2007, 177, 571–575. [Google Scholar] [CrossRef]
- Power, N.; Ryan, S.; Hamilton, P. Computed tomographic cystography in bladder trauma: Pictorial essay. J. Assoc. Can. Radiol. 2004, 55, 304–308. [Google Scholar]
- Ramchandani, P.; Buckler, P.M. Imaging of genitourinary trauma. AJR Am. J. Roentgenol. 2009, 192, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Elkbuli, A.; Ehrhardt, J.D.; Hai, S.; McKenney, M.; Boneva, D. Management of blunt intraperitoneal bladder rupture: Case report and literature review. Int. J. Surg. Case Rep. 2019, 55, 160–163. [Google Scholar] [CrossRef]
- Vaccaro, J.P.; Brody, J.M. CT cystography in the evaluation of major bladder trauma. Radiographics 2000, 20, 1373–1381. [Google Scholar] [CrossRef] [Green Version]
- Quagliano, P.V.; Delair, S.M.; Malhotra, A.K. Diagnosis of blunt bladder injury: A prospective comparative study of computed tomography cystography and conventional retrograde cystography. J. Trauma 2006, 61, 410–421. [Google Scholar] [CrossRef]
- Trinci, M.; Cirimele, V.; Cozzi, D.; Galluzzo, M.; Miele, V. Diagnostic accuracy of pneumo-CT-cystography in the detection of bladder rupture in patients with blunt pelvic trauma. Radiol. Med. 2020, 125, 907–917. [Google Scholar] [CrossRef]
- Andrich, D.E.; Mundy, A.R. The nature of urethral injury in cases of pelvic fracture urethral trauma. J. Urol 2001, 165, 1492–1495. [Google Scholar] [CrossRef]
- Ingram, M.D.; Watson, S.G.; Skippage, P.L.; Patel, U. Urethral injuries after pelvic trauma: Evaluation with urethrography. Radiographics 2008, 28, 1631–1643. [Google Scholar] [CrossRef] [Green Version]
- Zong, Z.W.; Bao, Q.W.; Liu, H.Y.; Shen, Y.; Zhao, Y.F.; Hua, X.; Guo, Q.S.; Zhang, L.Y.; Chen, Y. Diagnosis and treatment of rare complications of pelvic fractures. Chin. J. Traumatol. 2016, 19, 199–205. [Google Scholar] [CrossRef]
- Trinci, M.; Cirimele, V.; Ferrari, R.; Ianniello, S.; Galluzzo, M.; Miele, V. Diagnostic value of contrast-enhanced ultrasound (CEUS) and comparison with color Doppler ultrasound and magnetic resonance in a case of scrotal trauma. J. Ultrasound 2020, 23, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Di Serafino, M.; Acampora, C.; Iacobellis, F.; Schillirò, M.L.; Borzelli, A.; Barbuto, L.; Oliva, G.; Pezzullo, F.; Segreto, S.; Vallone, G.; et al. Ultrasound of scrotal and penile emergency: How, why and when. J. Ultrasound 2021, 24, 211–226. [Google Scholar] [CrossRef]
- Mohrs, O.K.; Thoms, H.; Egner, T.; Brunier, A.; Eiers, M.; Kauczor, H.U.; Hallscheidt, P. MRI of patients with suspected scrotal or testicular lesions: Diagnostic value in daily practice. AJR Am. J. Roentgenol. 2012, 199, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, S.; Choi, S.H.; Jeong, W.K.; Choi, J.H. The efficacy of magnetic resonance imaging for the diagnosis of testicular rupture: A prospective preliminary study. J. Trauma 2009, 66, 239–242. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Kim, D.H.; Brodke, D.S.; Harris, M.; Chapman, J.R.; Schildahuer, T.; Routt, M.L.; Sasso, R.C. Diagnosis and management of sacral spine fractures. Instr. Course Lect. 2004, 53, 375–385. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues-Pinto, R.; Kurd, M.K.; Schroeder, G.D.; Kepler, C.K.; Krieg, J.C.; Holstein, J.H.; Bellabarba, C.; Firoozabadi, R.; Oner, F.C.; Kandziora, F.; et al. Sacral fractures and associated injuries. Glob. Spine J. 2017, 7, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Garozzo, D.; Zollino, G.; Ferraresi, S. In lumbosacral plexus injuries can we identify indicators that predict spontaneous recovery or the need for surgical treatment? Results from a clinical study on 72 patients. J. Brachial Plex. Peripher. Nerve Inj. 2014, 9, e1–e9. [Google Scholar] [CrossRef]
- Neufeld, E.A.; Shen, P.Y.; Nidecker, A.E.; Runner, G.; Bateni, C.; Tse, G.; Chin, C. MR imaging of the lumbosacral plexus: A review of techniques and pathologies. J. Neuroimaging 2015, 25, 691–703. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Fracture | Fracture Stability | Associated Intrapelvic Complications | Management of Polytrauma Patient |
|---|---|---|---|
| Lateral compression | Bladder injuries Sacral nerves injuries | ||
| Grade 1 | Stable | Nonoperative management | |
| Grade 2 | Rotational instability | Surgical fixation | |
| Grade 3 | Multidirectional instability | Surgical fixation | |
| Anterior–posterior compression | Vascular injuries Bladder and urethral injuries Testicular injuries | ||
| Grade 1 | Stable | Nonoperative management | |
| Grade 2 | Rotational instability | Surgical fixation | |
| Grade 3 | Multidirectional instability | Surgical fixation | |
| Vertical shear | Multidirectional instability | Vascular injuries Bladder and urethral injuries Sacral nerves injuries | Surgical fixation |
| Combined mechanism | Multidirectional instability | Vascular injuries Bladder and urethral injuries Testicular injuries Sacral nerves injuries | Surgical fixation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leone, E.; Garipoli, A.; Ripani, U.; Lanzetti, R.M.; Spoliti, M.; Creta, D.; Giannace, C.; Galluzzo, A.; Trinci, M.; Galluzzo, M. Imaging Review of Pelvic Ring Fractures and Its Complications in High-Energy Trauma. Diagnostics 2022, 12, 384. https://doi.org/10.3390/diagnostics12020384
Leone E, Garipoli A, Ripani U, Lanzetti RM, Spoliti M, Creta D, Giannace C, Galluzzo A, Trinci M, Galluzzo M. Imaging Review of Pelvic Ring Fractures and Its Complications in High-Energy Trauma. Diagnostics. 2022; 12(2):384. https://doi.org/10.3390/diagnostics12020384
Chicago/Turabian StyleLeone, Edoardo, Andrea Garipoli, Umberto Ripani, Riccardo Maria Lanzetti, Marco Spoliti, Domenico Creta, Carolina Giannace, Antonio Galluzzo, Margherita Trinci, and Michele Galluzzo. 2022. "Imaging Review of Pelvic Ring Fractures and Its Complications in High-Energy Trauma" Diagnostics 12, no. 2: 384. https://doi.org/10.3390/diagnostics12020384