1. Introduction
Breast cancer is the most frequent form of cancer amongst women, and, in the most part, the presence of metastases dictates the survival rate. Approximately 6% of women diagnosed with breast cancer have metastases present at the moment of presentation [
1,
2]. Between 2 and 5% of total diagnosed cancer patients will develop orbital metastases [
3]. Breast cancer can metastasize in many organs, but it is responsible for the most frequent orbital metastases (28.5–58.8% of all cases of orbital metastasis) followed by prostate and lung cancer [
4]. Invasive lobular carcinoma (ILC) has a higher likelihood to metastasize in unusual sites such as the gastrointestinal tract, genitourinary system, peritoneum, retroperitoneal, bone, bone marrow, central nervous system, leptomeninges, and orbit, whereas invasive ductal carcinoma (IDC) often metastasizes to the lung, liver, bone, and brain [
5].
Although the majority of the patients with orbital metastases, male or female, have a history of breast cancer [
6], in 25% of the cases, orbital metastases are the first manifestation of this disease [
7]. Differentiation between an orbital metastasis and a primary orbital tumor may be complicated by the diverse symptomatology or by the absence of a known breast cancer diagnosis. Establishing the diagnosis of orbital metastases requires the implicit tissue biopsy or, when it is possible, surgical excision of the tumor.
We present the case of a 57-year-old postmenopausal woman diagnosed with unilateral retroocular metastasis as the first and only symptom of a mammary tubulo-lobular carcinoma. This fact leads us to evaluate the current specialty literature regarding the incidence, clinical presentation, diagnostic modalities, therapeutic management, treatment response, and disease-progression free survival of invasive breast cancer with orbital metastasis.
2. Case Report
A 57-year-old postmenopausal Caucasian country side woman, with no family history of breast or gynecological cancer. She had her menarche at the age of 15, gave birth at the age of 23, breast fed for two years, never used hormonal contraception accused the following since March 2015: diplopia, diminished visual acuity, orbital tenderness, mild exophthalmia of her left eye and ptosis of the left eyelid, all debuting insidiously. Furthermore, the patient has several comorbidities such as diabetes mellitus type 2, essential arterial hypertension, and mixed cardiomyopathy.
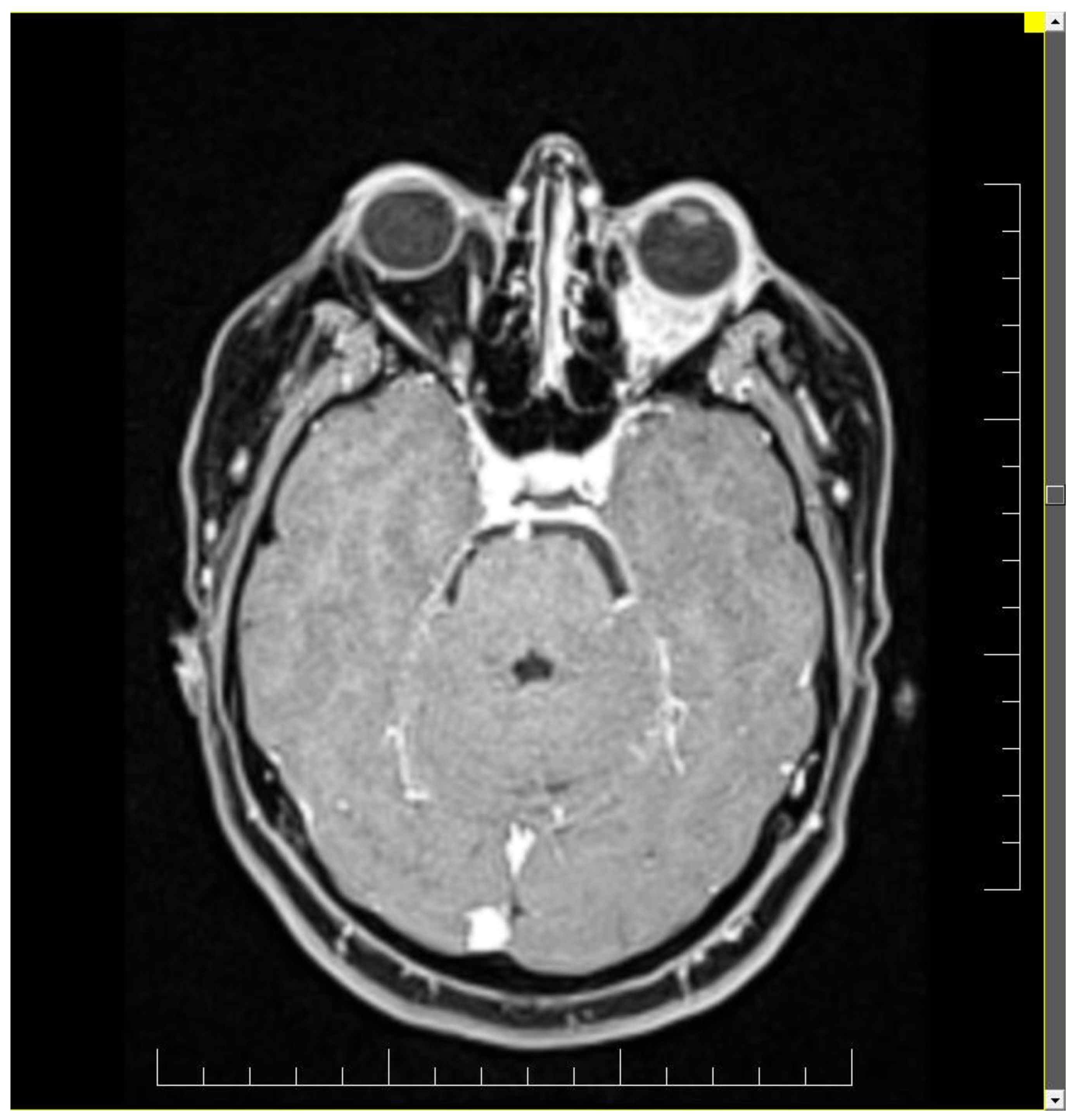
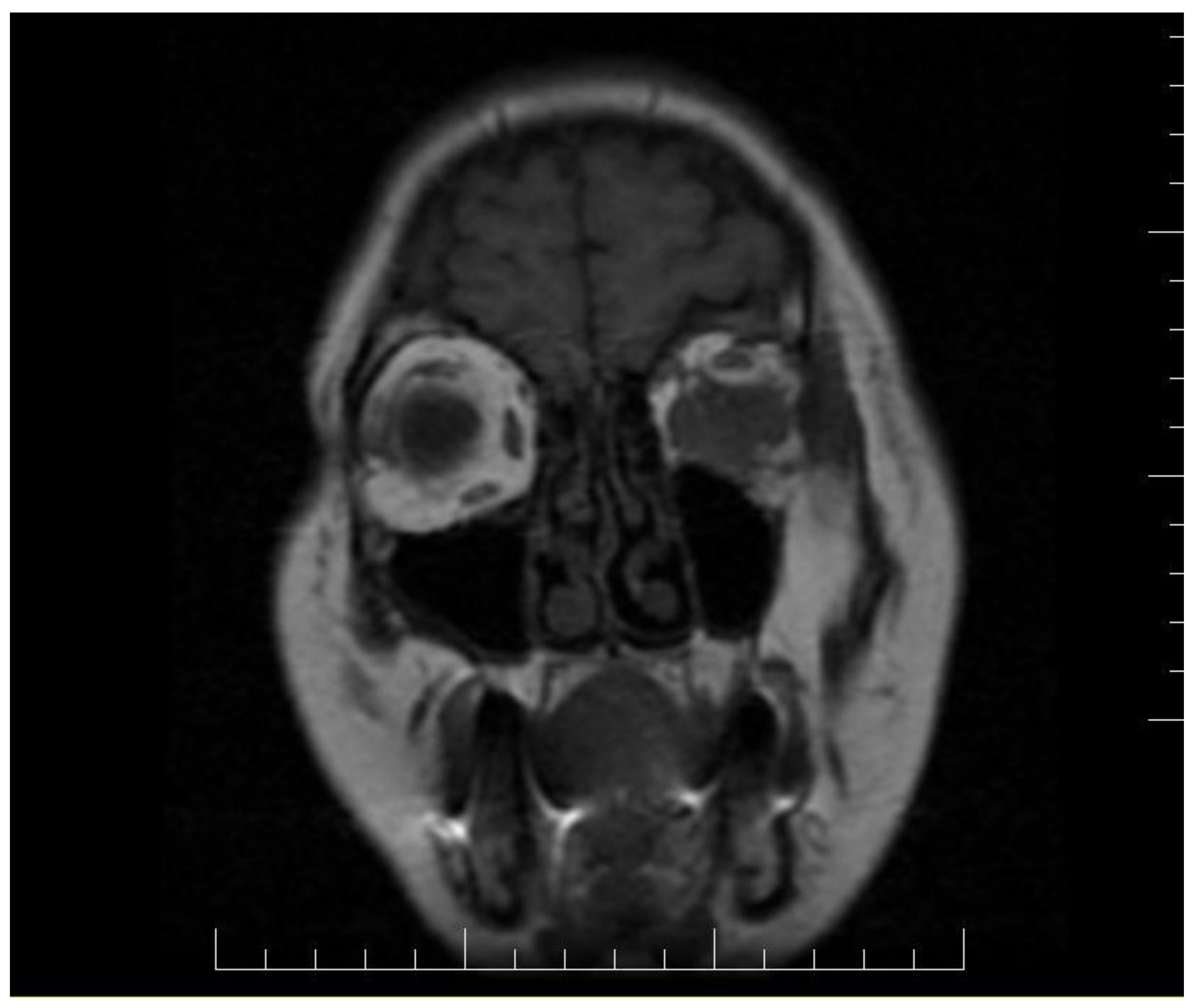
Ophthalmologic and neurologic examinations revealed reduced visual acuity, reduced mobility in all directions of the eye, normal intraocular pressure, hypoesthesia of the left hemi-face, paresis of the 3rd and 4th nerve of the left eye and paresis of the 5th nerve. Magnetic resonance imaging (MRI) and computed tomography (CT) scan detect a tumor situated in the left retroocular space in the intraconal area, which cuffs the left optic nerve and invades the extra-ocular muscles (
Figure 1 and
Figure 2). Differential diagnosis included diabetic retinopathy, thyroid ophthalmopathy, lymphoma, primary or metastatic neoplasia. The thyroid function tests were normal and the ophthalmologic exam excluded diabetic retinopathy.
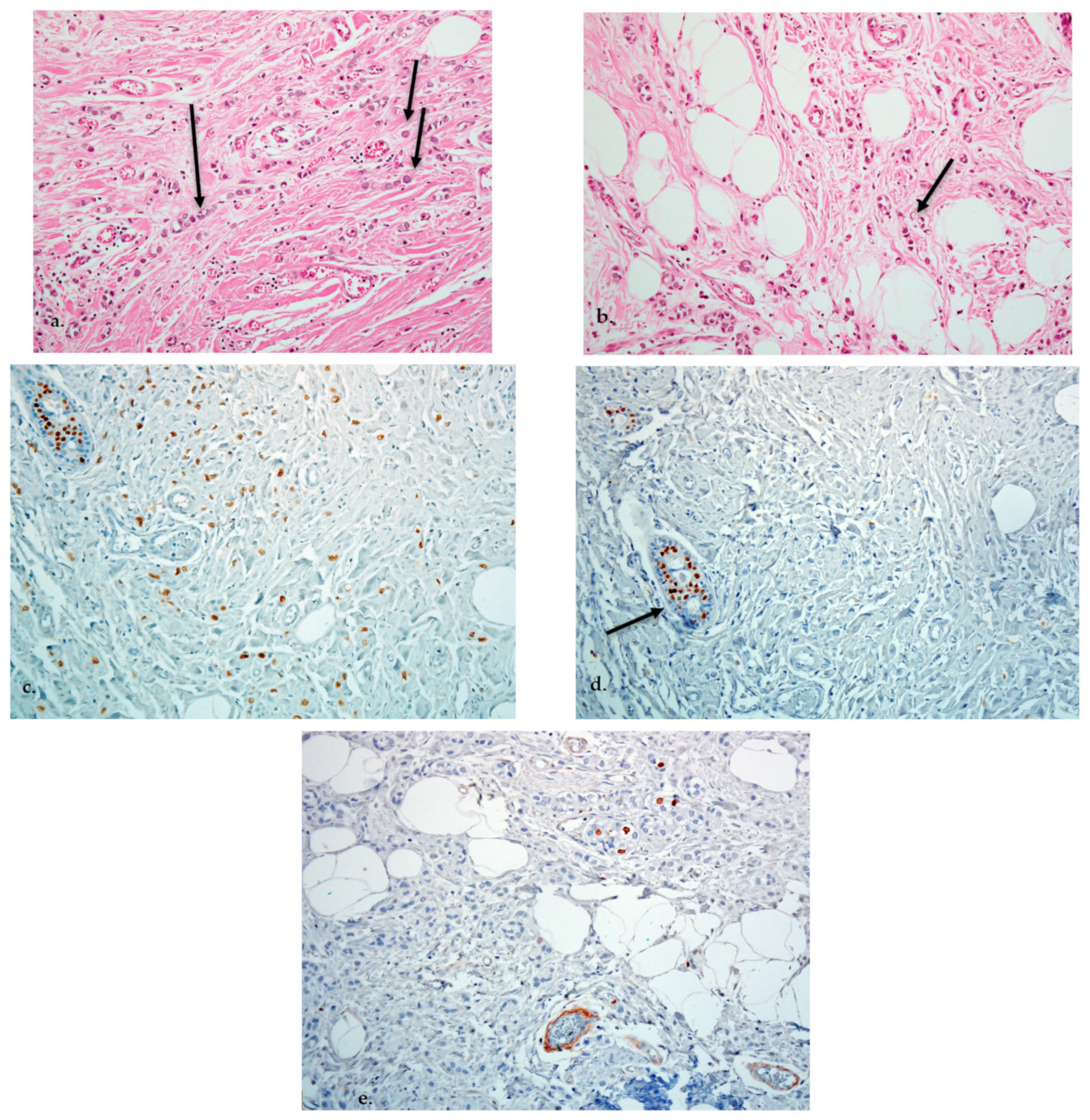
In June 2015 an excisional biopsy of the tumor was made and the pathological report confirmed the metastasis of an invasive ductal breast cancer. Immunohistochemistry (IHC) analysis revealed carcinoembryonic antigen, synaptophysin, cytokeratin 20 negativity and cytokeratin (CK) 7, estrogen receptor (ER) positivity.
In July 2015 the patient was referred to our oncology clinic for management of an orbital metastasis with primary breast cancer. She was in a good general health status, had normal weight and Eastern Cooperative Oncology Group (ECOG) 0. Clinical examination of the breasts revealed a palpable mass of 2.5/3 cm in size in the left upper outer quadrant and the enlargement of ipsilateral axillary lymph nodes (cN1). In the upper internal quadrant of the right breast a tumor of 1.5/1 cm with a firm consistency and a smooth surface is palpated. The value of carbohydrate antigen 15-3 (CA 15-3) was 53 U/mL (normal values < 28 U/mL). Subsequently, standard mammography and bilateral breast echography were performed. Mammography showed in the upper external quadrant of the left breast a density asymmetry, with multiple micro-calcifications and associates multiple axillary adenopathies without the visualization of the fatty hilum (
Figure 3). On the upper internal quadrant of the right breast, mammography also revealed an oval shaped image with benign characteristics suggestive for a fibroadenoma (
Figure 4). Breast ultrasound revealed the left breast discerned an inhomogeneous hypoechogenic area of 23/22 mm, imprecisely delimited in the upper external quadrant and ipsilateral adenopathies. Breast imaging reporting and data system score (BIRADS) was 5 for the left breast, suggestive of malignancy. For the right breast, the BIRADS score was 2 with a suggestive aspect of mammary fibroadenoma. The established clinical diagnosis for this stage was: left superior external quadrant breast cancer cT2 cN1 pM1 stage IV.
In July 2015 surgical treatment is performed on the left breast tumor: sectorial mastectomy with ipsilateral lymphadenectomy. Pathological examination revealed a grade 2 invasive carcinoma, tubulo-lobular subtype with lympho-vascular invasion, perineural invasion and positive margins, 10 positive axillary lymph nodes out of 10 examined, pT2pN3a—according to the 7th edition of the Union of International Cancer Control (UICC) Tumor, Nodes, Metastasis (TNM) classification. Furthermore, IHC staining showed ER—positive (67%), PR—negative, human epidermal growth factor receptor 2 (HER2/neu) negative and Ki-67 index of 9% (luminal B subtype). Post-surgery total body CT scan detects no other distant metastases. (
Figure 5).
In September 2015, the patient was referred to the radiotherapy department for external beam radiation therapy. The residual left orbital mass was irradiated with 50 Grays (Gy) in 25 fractions on the left eye. Concomitantly, hormonal therapy with aromatase inhibitors was initiated: Anastrozole 1 mg o.d. (once a day), daily. Additionally, she underwent further radiation therapy on the chest wall, breast and internal mammary lymph nodes (total dose 50 Gy/25 fractions) and left axillary and left supraclavicular nodes (total dose 50 Gy/20 fractions).
After radiation therapy was finalized, the patient was followed up according to the 2015 European Society of Medical Oncology (ESMO) recommendations.
After two years from the initial breast cancer diagnosis, the patient developed a depression, anhedonia, hypochondriac preoccupations, memory and concentration disorders, anxiety and mixt insomnia reason why she was referred to a psychiatrist. She was diagnosed with a depressive disorder for which she was prescribed citalopramum 20 mg o.d. and alprazolamum 0.5 mg t.i.d (three times a day).
At a follow-up control from February 2019 the patient is asymptomatic with the exception of unilateral blindness secondary to irradiation. ECOG performance status was 0. Biologically, CA15-3 tumor marker value was increased at 4339 U/mL, whilst the rest of the blood tests were normal. Bilateral mammography and clinical exam did not yield any signs of relapse. Considering that the value of CA15-3 was over 15 times the upper limit, a total body CT scan was scheduled for April of 2019. It revealed a left retroocular relapse, bone metastases, ascites in a medium quantity and peritoneal carcinomatosis. Palliative mono-chemotherapy is initiated with Paclitaxel 175 milligrams (mg)/m2 every 3 weeks, combined with bisphosphonates: Ibandronic Acid 6 mg every 3 weeks.
The chemotherapy was barely tolerated with several adverse reactions: grade 2 emesis on the first two cycles of chemotherapy which required antiemetic intravenous medication, febrile neutropenia after the 4th cycle which remitted after symptomatic approach with antibiotics and antipyretics. On the following cycles secondary prophylaxis with a granulocyte colony-stimulating factor was associated. During chemotherapy, the patient developed grade 3, peripheral neuropathy, and expression of the addition of chemotherapy toxicity to the underlying diabetes mellitus with unfavorable response to co-analgesics. Furthermore, at a follow up psychiatric consult, Zopiclonum 7.5 mg o.d. was added to manage the mixt insomnia. ECOG performance was elevated to 2.
After the 6th cycle of chemotherapy, patient status got worse secondary to clinical disease progression, complicated with sub-occlusive syndrome and increase in ascites quantity. The patient was transferred to the palliative care ward. Unfortunately, despite best supportive care, patient evolution was unfavorable resulting in her death in December 2019.
3. Discussions
Several solid tumors and pseudo tumors can cause metastases of the eye and orbit, but breast cancer gives more frequently metastases at this level with variable incidences [
4,
7,
8].
It is possible that the orbital metastases incidence may be higher than reported, and this underestimation could be explained by the fact of patients with orbital lesions of small dimensions are asymptomatic, or the clinical picture of ocular metastases is overshadowed by the other metastases in other organs [
9]. The autopsy studies report a higher rate of ocular metastases [
10].
In contrast to uveal metastases, which can be bilateral (up to 25%), unilateral orbital metastases are the usual presentation and the superior lateral extraconal quadrant is most frequently involved [
11]. Orbital metastases are usually discovered in known breast cancer patients and they are found in the context of a multi-system end-stage disease [
12]. Most reports cite that up to 25% of the total orbital metastases cases are discovered before the diagnosis of the primary tumor [
7,
13], as our case did.
Unlike primary orbital tumors, where the symptoms tend to onset earlier, symptoms produced by orbital metastasis include diplopia, pain, vision re-duction, proptosis, alterations of eye motility, the emergence of a tangible mass, ptosis, displacement of the globe, conjunctive chemosis, enophthalmos, papilledema, retinal folds, paresthesia, and pulsation, unlike primary orbital tumors, the symptoms tend to onset earlier. [
7]. Our patient presented several of the most frequent symptoms and namely vision loss, alteration of ocular motility and proptosis in the affected eye secondary to extra-ocular muscle infiltration.
MRI is the gold standard for evaluating orbital tumors because this ensures a better contrast of the soft tissue and does not afflict ionizing radiation. Imaging patterns such as the appearance of a mass accompanied by muscular or fatty infiltration generally suggests the presence of a mammary carcinoma metastasis, osseous affection indicates the existence of prostate cancer and prevailing muscular affliction reveals a melanoma. Mainly, orbital metastases are located exclusively in extraconal spaces (50%) and the rest are found either in intraconal spaces (30%) or in both (20%) [
14]. The execution of diffusion weighted imaging can improve the differential diagnosis between an orbital process and a benign tumor (such as a hemangioma), sarcoidosis, Wegener granulomatosis and lymphoproliferative disorders. If the T2-weighted images series shows hypointense signals it may correspond to an inflammatory pseudo tumor, while hyperintense lesions may reveal a lymphoma or metastasis [
14,
15].
To establish a definitive diagnosis, a tissue biopsy is needed (open biopsy or fine needle aspiration). However, in a known metastatic cancer patient, a new orbital metastasis does not require a pathological confirmation [
16]. The situations in which a biopsy is required are the following: patients with no known previous cancer, a solitary metastasis to the orbit with no other metastatic disease or in those cases in which decreasing tumor burden may result in a more effective chemotherapy or irradiation [
17].
Breast cancer is histologically a very heterogeneous disease. ILC represents 10–15% of the total breast cancers, being, histologically, the second most frequent type of breast cancer after invasive ductal carcinoma [
18]. The ILC histological subtype metastasizes in the orbitals more frequently than invasive ductal carcinoma [
19]. In our patient’s case, the histopathology results of the primary breast tumor are discordant with the orbital metastasis, revealing a less common subtype of breast cancer and namely tubulo-lobular carcinoma. According to the 2012 World Health Organization (WHO) classification, tubulo-lobular carcinoma is a distinct subtype of mammary carcinoma with overlapping morphologic features of ductal and lobular invasive carcinoma. Some authors consider it a subtype of invasive ductal carcinoma, based on positivity for E-cadherin, while others claim it is a variant of invasive lobular carcinoma [
20,
21]. In our case, the contingent with lobular morphology and the small ducts from the breast resection specimen were negative for E-cadherin, with internal positive control on the benign glands. The presence of small ducts imposed classification as ductulo-lobular carcinoma rather than mixed, lobular and ductal carcinoma in which the ductal component had to be positive for E-cadherin. In the specimen of retroorbital metastasis excised in another hospital, there were also described small tubules/ductules and no IHC staining for E-cadherin was performed.
Considering that most metastatic breast cancers are incurable, the intent of the treatment is palliative and to improve overall survival and quality of life. The treatment of orbital metastases includes radiotherapy, hormone therapy, and systemic chemotherapy with or without target therapy. Usually, in this setting, metastasectomy is not recommended since this will not cure the disease and is associated with higher ocular morbidity [
4,
7,
8]. In a few selected patients, as is the presented case, the excision of the tumor could establish a diagnosis [
8]. External beam radiation therapy is the main treatment option for orbital and ocular adnexal metastases with an objective response rate up to 79% [
22]. Despite symptom alleviation or remission [
4], potential significant side effects could outweigh the benefits (cataract formation, radiation retinopathy) [
8]. In the reported case, the patient developed cataract as a side effect with progressive blindness of her left eye. The gold standard treatment is still in debate. In a retrospective study by Rosset et al., it was found that 3 out of 26 patients with unilateral disease developed contralateral metastasis when only one eye was irradiated versus none of the 10 patients who received bilateral irradiation [
23]. On the other hand, basing on another study by Chik et al. in which none of the 11 patients has developed contralateral metastases regardless if they received unilateral or bilateral irradiation, we consider that the only reasonable option is to treat only the affected eye and consider irradiating the contralateral eye when metastases occur [
24].
Endocrine therapy should be considered the treatment of first choice for a postmenopausal metastatic breast cancer with positive estrogen receptors, regardless of the metastatic site and if a rapid tumor response is not necessary. Chemotherapy is given to patients with concomitant progressive systemic disease or if the disease has progressed on hormone therapy [
25]. Although the surgical modality of primary metastatic breast cancer has a well-established role in prevention and/or treating local complication, more and more studies have shown that the regional treatment of the primary tumor, especially followed by RT, has a good impact on the prognosis with improved survival in patients with metastatic breast cancer [
26,
27].
The prognosis of patients with orbital metastases is poor. The median survival after diagnosis of orbital metastases from a breast cancer primary is ranging from 22 to 31 months, although survival up to 116 months has been reported [
4,
8]. Our patient had a progression free survival of four years with hormonotherapy. Disease recurrence was chemo refractory with taxane-based therapy. After eight only months, patient had deceased through organ insufficiency and disease progression. Overall survival of our patient was 56 months, which is longer than the median survival reported in literature.


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




