A Narrative Review of the Classification and Use of Diagnostic Ultrasound for Conditions of the Achilles Tendon

Department of Internal Medicine, Division of Rheumatology, The Ohio State University Wexner Medical Center, 543 Taylor Ave, Columbus, OH 43203, USA
Diagnostics 2020, 10(11), 944; https://doi.org/10.3390/diagnostics10110944
Submission received: 15 September 2020
/
Revised: 3 November 2020
/
Accepted: 4 November 2020
/
Published: 13 November 2020
(This article belongs to the Special Issue Rheumatic Diseases: Diagnosis, Treatment and Management)
Abstract
:Enthesitis is a cardinal feature of spondyloarthropathies. The Achilles insertion on the calcaneus is a commonly evaluated enthesis located at the hindfoot, generally resulting in hindfoot pain and possible tendon enlargement. For decades, diagnosis of enthesitis was based upon patient history of hindfoot or posterior ankle pain and clinical examination revealing tenderness and/or enlargement at the site of the tendon insertion. However, not all hindfoot or posterior ankle symptoms are related to enthesitis. Advanced imaging, including magnetic resonance imaging (MRI) and ultrasound (US), has allowed for more precise evaluation of hindfoot and posterior ankle conditions. Use of US in diagnosis has helped confirm some of these cases but also identified other conditions that may have otherwise been misclassified without use of advanced imaging diagnostics. Conditions that may result in hindfoot and posterior ankle symptoms related to the Achilles tendon include enthesitis (which can include retrocalcaneal bursitis and insertional tendonopathy), midportion tendonopathy, paratenonopathy, superficial calcaneal bursitis, calcaneal ossification (Haglund deformity), and calcific tendonopathy. With regard to classification of these conditions, much of the existing literature uses confusing nomenclature to describe conditions in this region of the body. Some terminology may imply inflammation when in fact there may be none. A more uniform approach to classifying these conditions based off anatomic location, symptoms, clinical findings, and histopathology is needed. There has been much debate regarding appropriate use of tendonitis when there is no true inflammation, calling instead for use of the terms tendinosis or tendonopathy. To date, there has not been clear examination of a similar overuse of the term enthesitis in conditions where there is no underlying inflammation, thus raising the need for more comprehensive taxonomy.
1. Introduction
A principal feature of spondyloarthropathies is inflammation of the tendon, ligament, and joint capsule insertions into the bones, termed enthesitis [1]. Enthesitis can involve many parts of the body, including the insertions of the Achilles, plantar fascia, quadriceps tendon at the upper patellar pole, patellar ligament at the lower patellar pole and tibial tubercle, deltoid at the acromion and clavicle, flexor and extensor tendons at the phalanges, and vertebral ligaments at the spine. [2,3,4,5]. More progressive thinking has led to the model of the enthesis being more than an insertion site but being a unique enthesis organ, including the insertion, the fibrocartilage, bursa, fat pad, adjacent trabecular bone networks, and deeper fascia [6].
Clinical assessment of enthesitis can be done by applying ~4 kg/cm2 of pressure (enough to blanch the tip of the examiner’s fingernail) and assessing for tenderness [5]. There have been several clinical indices developed to assess enthesial disease activity. The first published index was the Mander/Newcastle Enthesitis Index (MEI), which identified 66 enthesial sites for examination [5,7]. However, assessment of some of these deeper located enthesial areas can be time consuming and also challenging with physical exam alone [8]. Subsequent disease activity indices aimed to condense the examination, with most having less than 16 examination sites. Even with these more focused assessments, the Achilles remained a fixture in these indices, including the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES), the Spondyloarthritis Research Consortium of Canada Enthesitis Index (SPARCC), the Glasgow Ultrasound Enthesitis Scoring System (GUESS), and Leeds Enthesitis Index (LEI) [9,10,11,12].
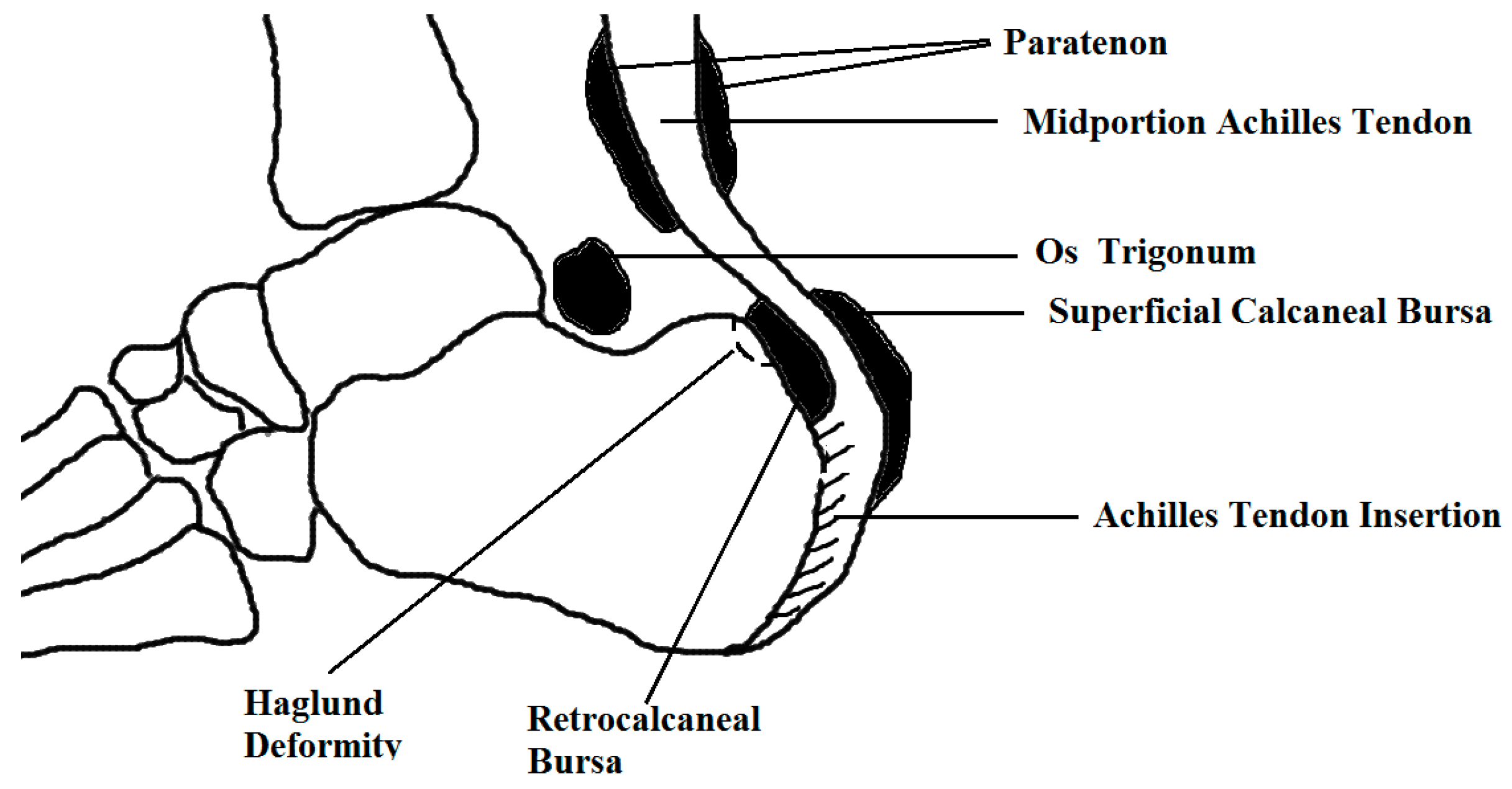
Diagnosis of enthesitis on clinical exam alone, however, may have limitations as the differential for hindfoot and posterior ankle pain is not exclusive to enthesitis [13,14]. Table 1 includes conditions that may result in pain and/or swelling in the hindfoot and posterior ankle. Some of these conditions, such as an Achilles rupture, are stand-alone conditions not considered a feature of a spondyloarthropathy. Others, such as retrocalcaneal bursitis, may be seen in the context of enthesitis when considering the enthesis as an organ encompassing the bursa and fibrocartilage, for example. Discerning a more accurate etiology to hindfoot symptoms is especially important in diagnosing a spondyloarthropathy. Increasing use of imaging, such as ultrasound (US) and magnetic resonance imaging (MRI), bone scan, and computerized tomography (CT) scan have demonstrated accuracy in detection of both inflammatory and chronic changes in enthesitis [15,16,17,18,19,20]. Identifying the cause of hindfoot pain has important implications in treatment, as different conditions may respond better to medication, exercise, or surgery [21]. Figure 1 illustrates the anatomy and localizes the site of involvement for several conditions that may result in symptoms.
2. Methods
In this narrative literature review, databases of PubMed and the Cochrane Library were searched to review the relevant literature. In addition Google Scholar, conference proceedings, and bibliographies of review articles were searched for relevant articles. Key index words were ultrasound, enthesitis, spondyloarthropathy, Achilles, hindfoot, ankle, tendonopathy, tendonitis, paratenon, calcific tendonopathy, retrocalcaneal bursitis, and superficial calcaneal bursitis. Published data from 1927 to 2020 are included in this review.
3. A Word about Words
The words used to describe the pathology involving the conditions of the Achilles tendon can be confusing and redundant. Over time, rheumatologists, orthopedists, sports medicine physicians, physiatrists, podiatrists, radiologists, and pathologists have utilized classification schemes that have helped contribute to some of this muddled nomenclature. Reviewing and comparing the literature can be difficult as definitions used by one group may not be the same used by another.
The first area lacking clarity involves the terminology for describing tendons. In general, “tendonopathy”, sometimes spelled “tendinopathy”, is a catch all term describing pain, swelling, and functional changes in and around tendons [22]. It is an umbrella term that essentially describes tendon pain without specifically denoting the specific pathology; it can include tears, inflammatory enthesitis, or chronic degeneration [23]. When one is not able to differentiate whether the tendon pathology is related to inflammation or degeneration, it may be more accurate to use the word tendonopathy.
The use of the term tendonopathy to describe non-specific Achilles tendon conditions in the hindfoot and posterior ankle is inhibited in clinical practice. Billing codes are an intrinsic part of clinical documentation; however, the widely used coding system for billing in the US, the International Classification of Diseases-10-Clinical Modification (ICD-10-CM), lacks a billable code for tendonopathy. ICD-10-CM was implemented 1 October 2015; it was designed with a combination of letters and numbers to correspond to a specific condition [24]. Perhaps the lack of consensus on describing tendonopathies, including Achilles tendonopathies, may have led to the noticeable absence in the ICD-10-CM coding system.
There are several codes that approximate tendonopathy, but in general these can be overly inclusive, utilizing descriptors not necessarily seen in tendonopathies alone. For example, M67.89 denotes other disorders of the synovium and tendon [25]. This is too specific for a tendonopathy as selection of this code suggests there is synovial involvement, which is not the case with all tendonopathies.
While some codes are too specific, some are not specific enough. For example, M67.873 and M67.874 describe other specified disorders of the right or left foot, respectively [26,27]. This unfortunately does not limit pathology to the tendon and is too overly general as this could include other such conditions such as injuries, blood clots, rashes, fractures, bone erosions, ossifications, and tears.
Some codes used in clinical practice are frankly just inaccurate. Many providers may end up selecting the closest thing they can find to the term tendonopathy, which may be the codes for tendonitis. M76.60, M76.1, or M76.2 denote Achilles tendonitis of an unspecified leg, the right leg, or the left leg, respectively [28]. The suffix “-itis” implies inflammation, and so tendinitis it seems would describe inflammation of the actual tendon. Therefore, use of the tendonitis coding would be inaccurate in describing non-inflammatory, degenerative tendon pathologies.
The traditional use of the word tendonitis among sports medicine practitioners involves a tendon injury, often from a repetitive mechanical load, with a subsequent inflammatory response [29,30]. However, studies have not been able to support evidence for inflammation, at least histologically, within an overloaded tendon [31,32]. In rat models by Zamora et al., in an overloaded model of the rat plantaris tendon, there was no evidence of inflammatory cells on histologic review [33]. This concept that there is a lack of histologic inflammation in tendonitis is further supported in clinical practice, as use of non-steroidal anti-inflammatory medications and corticosteroids have yielded limited long-term success in patients with clinical tendonitis [34]. Therefore, in patients without histologic evaluation, tendonopathy may be a more appropriate descriptor in clinical practice.
The suffix “-osis” implies degeneration; therefore, while tendinitis describes inflammation of the actual tendon itself, tendinosis describes degeneration of the tendon [29]. The collagen degeneration of tendinosis generally occurs in response to chronic overuse [35]. The collagen fibers become disorganized and lose their parallel alignment, becoming loosely packed, interspersed with mucoid ground substance [36]. On histologic examination, tendinosis can result in hypercellularity with increased tenocyctes with myofibroblastic differentiation (tendon repair cells) and neovascularization; however, classic inflammatory cells are generally absent [37]. Like the tendonitis term, the term tendinosis may be better confirmed with histologic evaluation. Therefore, in clinical practice, use of the word tendonopathy may be more befitting without histologic review.
There are other commonly used classifications which overlap with the above nomenclature, which are similarly disagreed upon in the literature. One of the oldest terms still adopted in practice today is the Haglund terminology. Haglund syndrome was first described almost 90 years ago [38,39]. Haglund syndrome is a description for a retrocalcaneal bursitis associated with or without an abnormal protuberance of the posterosuperior border of the calcaneus [39]. A Haglund deformity or exostosis is a description for the enlargement of the calcaneus; it results from tendinosis, overuse, or the wearing of improperly fitted shoes [40]. Haglund disease instead describes osteochondrosis of the accessory navicular bone [41]. Use of the Haglund nomenclature may be confusing given the diversity of what these terms describe. More recently, some experts have recommended, in lieu of Haglund terminology, adoption of a nomenclature system classified off anatomic location, symptoms, clinical findings, and histopathology [41].
Enthesitis also overlaps with the above terminology and is also not immune to this war of the words. Enthesitis deserves the same linguistic dissection as tendonitis and its counterparts. Similar to the term tendonopathy, enthesopathy is an umbrella term; it describes pathologies of the tendon/ligament insertions, or more progressively, the enthesis organ [42]. Like tendonitis, use of the suffix “-itis” should be reserved to describe actual inflammation of the enthesis. Use of the suffix “-osis” describes degeneration, and so the term “enthesosis” could be considered reasonable to describe degeneration at the enthesis. However, a PubMed search and even a Google search for “enthesosis” yields no results and to the knowledge of the author, this is not a term used in clinical settings. It is important to consider implications of the broad adoption of enthesitis in cases that may not be truly inflammatory. Much like tendinosis, the term enthesosis may be more appropriate in clinical practice when there is a lack of clearly active inflammatory changes.
Much like the Haglund deformity, the enthesophyte (mineralized or ossified scars, or bone spurs) is an often used term that at times gets interchanged with enthesitis or may even be considered by some to be a defining feature of enthesitis [43]. This, however, may be a confusing term as enthesophytes have been found to be a common phenomenon in healthy and aging individuals and may not necessarily imply inflammation [44,45]. Arguably, if the term enthesosis were in use, enthesophytes, which could be a degenerative phenomenon, could be a characteristic of this non-inflammatory condition.
In addition, greater consideration should be given to describing the anatomy of the enthesis. As noted earlier, the enthesis describes the insertion of tendon and ligaments onto bone with a more recent shift introduced by McGonagle et al. almost 20 years ago, reclassifying the enthesis as a unique organ; this organ includes, collectively, the insertion, the fibrocartilage, bursa, fat pad, adjacent trabecular bone networks, and deeper fascia [1]. Using this broader definition to frame enthesopathies, the term enthesitis should refer to an inflammation within any of these substructures. While this is technically correct, it may be more precise to describe the actual substructures demonstrating pathology when describing enthesopathic findings [46]. This may be more in line with the recommendations put forth by Maffulli et al., with regards to using anatomic location, symptoms, clinical findings, and histopathology to describe hindfoot and posterior ankle conditions in lieu of the Haglund terminology [47]. Specifically, the enthesopathy classification may better be described on the basis of anatomic location with a focus on the specific substructures of the enthesis such as the bursa and Achilles insertion.
Use of the substructure description of enthesopathies would be important in helping unify the nomenclature of the hindfoot and posterior ankle. It also would help better describe patients with inflammatory conditions. For example, a patient with a retrocalcaneal bursitis, Doppler signal at the enthesis, and erosion could be classified as having enthesitis; arguably, so too could a patient with a thickened tendon alone at the insertion since this could also involve inflammation in the enthesis. However, if each substructure location were described, one could more precisely define and classify patients with posterior ankle and hindfoot inflammation.
For the purposes of this article, the word tendonopathy will be used to refer to pathologies of the tendon and paratenonopathy to pathologies of the paratenon. Further subclassifications of tendinosis, tendonitis, paratenonosis, or paratenonitis would further expand the differential. The word enthesitis will be used when discussing the inflammation at the enthesis and, where possible, further discussion of the substructure locations within the enthesis will be discussed.
4. Imaging Modalities for the Hindfoot and Posterior Ankle
Radiographs have limited utility in assessing soft tissue conditions; however, in chronic enthesitis, bony changes, including enthesophytes and erosions, may be seen at the attachments of the Achilles [15]. Radiographs may detect these late stage changes. They also can identify other bony abnormalities in the posterior ankle, including calcific tendonitis and posterior superior calcaneal prominences (Haglund deformities), which can be seen in retrocalcaneal bursitis and insertional Achilles tendonopathy [47,48].
Magnetic resonance imaging (MRI) is highly sensitive for active enthesitis; it captures the enthesis as well as associated soft tissue involvement and bone marrow edema [49]. Both exercise-induced tendonopathy and spondyloarthropathies can demonstrate retrocalcaneal bursitis, subcutaneous edema and calcaneal bone marrow edema [18,50,51,52,53]. In spondyloarthropathy patients with severe enthesitis, the thickness of the Achilles tendon is significantly increased [52,53]. In addition to inflammation, MRI is also excellent for detecting full-thickness or partial tendon tears [54].
Medical infrared thermography (MIT) is a less often used imaging modality for the evaluation of tendonopathy; it analyzes physiological function related to blood flow and the control of skin temperature [55]. In relation to tendonopathies, changes in blood flow from neovascularization may affect skin temperature at detectable MIT levels [55,56,57]. There have been limited studies to date evaluating use in the Achilles, but researchers have called for more attention to this non-invasive diagnostic tool [56,58,59,60].
Ultrasound (US) is a highly sensitive and commonly used tool for diagnostic assessments of tendons and entheseal sites [61,62,63,64]. Given the superficial position of the Achilles tendon, and ability of high resolution probes to demonstrate tendon fibers and small structures, US is an imaging modality of choice to evaluate the Achilles tendon [65]. US can depict tendon thickening, enthesophytes, and erosions [66]. US can demonstrate tendon swelling and thickening, discontinuity of tendon fibers, focal hypoechoic intratendinous areas, and fluid around the tendon [67]. In 2004, the Outcome Measures in Rheumatology (OMERACT) US Specialist Interest Group defined enthesitis on US as an “abnormally hypoechoic (loss of normal fibrillar architecture) and/or thickened tendon or ligament at its bony attachment (may occasionally contain hyperechoic foci consistent with calcification), seen in two perpendicular planes that may exhibit Doppler signal and/or bony changes, including enthesophytes, erosions, or irregularity” [68]. Table 2 highlights some of the principle findings on US examination for pathologies related to the Achilles tendon.
Compared to MRI, US remains a highly sensitive test for early diagnosis of enthesitis and generally costs less than MRI [18,87]. It is fast, can be done at the bedside, is reproducible, and is generally a preferred method for assessing tendon pathology among rheumatologists [61,62,63,64,65,66,67,88].
One pitfall in diagnostic US can be improper interpretation of artifacts [89,90]. With regard to the posterior ankle and hindfoot, edge artifact and anisotropy are of particular concern. Anistropy occurs when tissues show abnormal echogenicity, most commonly loss of echogenicity, due to an oblique insonating angle [91]. Tendons or ligaments may appear as hypoechoic and thus could be misinterpreted as tendinosis or tears [92]. Edge artifact occurs when a curved surface reflects the US beam away from the transducer, appearing as hypoechoic parallel lines projecting along the edges of the target [92]. Edge artifact could lead to the curved Achilles tendon being misinterpreted as paratenon thickening [92].
5. Enthesopathy
The normal disease progression for enthesitis in spondyloarthropathies is purported to begin with local, destructive, microscopic, inflammatory lesions that evolve towards fibrous scarring and new bone formation [66]. The findings on US can include decreased echogenicity of the enthesis, increased dimensions of the enthesis, structural lesions (such as enthesophytes), erosions, and increased vascularity seen on Doppler examination [9,10,11,12,66]. Gandjbakhch et al. reviewed PubMed and Embase databases from 1985–2010 for the most common criteria of enthesitis on US examinations; they found these to include thickened entheses, hypoechogenicity, enthesophytes, bony irregularity at the enthesis, erosions, and surrounding bursitis [69]. Sudoł-Szopińska et al. point out, however, that these criteria are not specific for inflammation and they may originate from chronic damage and degeneration of the enthesis [43]. This finding from damage and degeneration is more aligned with the proposed term enthesosis. Ultimately, this supports the contention that broad use of the term enthesitis may be too far reaching and perhaps use of enthesopathy may be more appropriate in this context when it may unclear if there is truly inflammatory activity present.
Previous studies have looked at the sensitivity and specificity of US in diagnosing enthesitis compared to clinical exam; however, definitions of what constitutes inflammatory enthesitis may not be fully consistent among all studies. Including enthesophytes in the enthesitis scoring, Balint et al. found clinical exam compared to US was less sensitive and specific for enthesitis (22.5% and 79.7%, respectively) [11]. De Miguel et al. utilized the MAdrid Sonographic Enthesis Index (MASEI) to evaluate the diagnostic accuracy of US at the enthesis [93]. The MASEI scoring includes enthesis thickness, structure, calcification/bone proliferation, erosion, bursa, and power Doppler signal in the cortical bone profile, tendon, and bursa. The study looked at 113 early spondyloarthritis patients compared to 57 non-inflammatory control individuals and 24 inflammatory control individuals. The ultrasound score was 23.36 ± 11.40 (mean ± SD) in spondyloarthritis patients and 12.26 ± 6.85 and 16.04 ± 9.94 in the non-inflammatory and inflammatory control groups (p < 0.001), respectively. In evaluating US to diagnose enthesitis with the MASEI scoring, the investigators found a sensitivity of 53.1%, a specificity of 83.3% [93].
Much of the previously reported literature on US use for enthesitis is based on varying scoring/classification systems, some of whose findings are not necessarily specific for inflammation but could also be found in degenerative enthesopathies and chronic microinjuries [4,57,94,95,96,97,98,99]. Scoring or classification systems that may include degenerative features such as enthesophytes may more accurately be classifying enthesopathies rather than specific enthesitis.
There are key findings on US, however, that may help better discern inflammatory enthesitis from a non-inflammatory enthesopathy. Several studies have found the presence of blood vessels in the enthesis to be specific for spondyloarthropathies [3,4,11,98,99]. D’Agostino et al. evaluated entheses of 164 patients with a spondyloarthropathy, 34 with mechanical back pain (MBP) and 30 with rheumatoid arthritis (RA); vascularization at the enthesis was found in 81% of spondyloarthropathy patients but in none of the patients with MBP or RA [100]. While this is not histologic confirmation of inflammation, neovascularization within this region may be the closest finding on US to confirming inflammatory changes.
Poulain et al. further assessed the sensitivity and specificity of power Doppler ultrasound (PDUS) for identifying patients fulfilling the Assessment of SpondyloArthritis International Society (ASAS) classification criteria for axial spondyloarthropathy [101]. Those fulfilling the criteria were deemed ASAS+ and those not fulfilling it were ASAS−. Baseline PDUS was performed at eight entheseal sites with PDUS enthesitis defined by the presence of vascularization at the entheseal insertion. Four hundred two patients with inflammatory back pain underwent a PDUS evaluation; PDUS enthesitis was detected in 58 (14.4%) patients, of which 40 (14.2%) were ASAS+ and 18 (17%) were ASAS−. The sensitivity of PDUS enthesitis was 13.9% and the specificity was 83.5%; the positive predictive value was 69% and negative predictive value was 26.8% for meeting ASAS criteria for axial spondyloarthropathy. Additionally, they found that, of the 18 ASAS− patients with positive PDUS, 59% fulfilled Amor’s criteria, 88% fulfilled European Spondyloarthropathy Study Group criteria, and 59% both [101].
An increasing number of studies have further demonstrated the presence of blood vessels at the tendon insertion in the cortical bone in spondyloarthropathy patients [100,102,103,104]. However, there is no clear consensus on which substructures in these studies demonstrated Doppler signal (e.g., tendon, bursa). This may make it challenging to fully compare studies as what one author may call enthesitis, another may classify the same finding as tendonitis.
D’Agostino et al. developed a criteria for evaluating what the authors termed enthesitis. The scoring system included points for tendon thickness, hypoechogenicity, calcification, erosion, and vascularization [100]. More specific to enthesitis, the authors semiquantified vascularization with Doppler signal on a scale of 0–3. The vascularization was scored as 0 if Doppler signal was absent, 1 if Doppler signal was minimal (one color spot detected), 2 if Doppler signal was moderate (two spots), or 3 if Doppler signal was severe (≥three spots) [100].
In addition to vascularization, Achilles tendon thickness may also be more specific for enthesitis and may correlate with clinical disease activity indices. In 2017, Ahmed et al. compared US with the Psoriatic Arthritis Disease Activity Score (PASDAS) [105]. PASDAS is a disease activity index for psoriatic arthritis based on patient (PtGA) and physician (PhGA) global, visual analog scale (VAS) scores, tender (SJC66) and swollen (SJC68) joint counts, dactylitis, enthesitis, the physical component score of the short form 36 health survey (SF36-PCS), and C-reactive protein (CRP) level [106]. In comparing 35 psoriatic arthritis patients to 30 matched controls, Achilles tendon thickness in active psoriatic arthritis correlated highly with PASDAS scoring (r = 0.796, p < 0.001) [105]. However, it should be noted that the tendon thickness could also be a feature seen in non-inflammatory tendonopathies or enthesopathies.
The Sonographic Enthesitis Index was developed to distinguish between acute and chronic enthesopathy, and identified findings were seen in acute inflammatory enthesial changes and chronic lesions [107]. The authors found increased tendon thickness, hypoechogenicity, peritendinous edema, and bursitis to be more characteristic of acute enthesopathies. Tears, loss of tendon thickness, intratendinous calcifications, and bone erosions were more typical of chronic enthesopathies. With specific regard to the Achilles, the presence of bone erosion was a feature in chronic enthesitis while bursitis was a feature of more acute inflammation [107].
US is a useful tool for diagnosing enthesopathy and can help differentiate inflammatory findings of vascularization and tendon thickness that are more often seen in enthesitis. Experts have called for a validated US scoring system for enthesitis not confounded by mechanical factors or obesity [46,108]. Currently used scoring systems may be impacted by body mass index (BMI), for example, MASEI scores, GUESS scores, thickness of the Achilles tendon, and enthesophyte scores correlate with increased BMI [109,110,111,112]. In evaluation of suspected enthesitis, other causes to hindfoot and posterior ankle pain may be elucidated in the workup as outlined in Table 1. The remainder of this article will review some of these other pathologies and how US may help in diagnosis of these conditions.
6. Achilles Tendonopathy
Achilles tendonopathy includes tendonitis and tendonosis. On US, the normal tendon morphology is one of parallel hyperechoic striations [70,113]. Tendonopathy may result in alterations in the tendon morphology and/or echogenicity on US [71,72,85]. Echogenicity refers to a tissue’s ability to reflect or transmit sound waves [73]. Hyperechoic structures appear white on the screen, hypoechoic structures appear gray on the screen, and anechoic structures appear black on the screen [72]. In tendonopathies, echogenicity may be decreased from intrasubstance tearing and mucoid degeneration while tendon dimensions may be increased from secondary hypertrophy [74]. Neovascularization may also be seen, as evidenced on US by color power Doppler [75].
Tendonopathy can occur at the insertion of the Achilles tendon or more proximally, at the midportion of the tendon, with the latter being more than twice as common [10,76,77]. Discerning the location of tendonopathy has implications in potential treatment responses. Over 80% of patients with midportion tendonopathy will respond to exercise-based management, whereas only up to 25% of those with insertional Achilles tendonopathy will, and ultimately 47% may go on to need surgical intervention [78,79,80,81].
Khan et al. evaluated US accuracy in patients diagnosed clinically with tendonopathy. They demonstrated US had a sensitivity of 0.80 and specificity of 0.49 in diagnosing tendonopathy compared with the clinical exam, and neither color nor power Doppler improved the accuracy of US [82]. Studies have also looked at reproducibility of posterior ankle measurements, particularly the Achilles measurements, and have demonstrated intra- and inter-rater reliability of ultrasound measurement of the Achilles tendon size [114]. Using US to diagnose and evaluate tendon morphology has some limitations, however. One area of uncertainty is what exactly constitutes a normal Achilles measurement, as size variations have been demonstrated even in healthy subjects [115].
There are several risk factors associated with development of tendonopathies. Diabetes and dyslipidemia have been proposed as independent risk factors [116,117]. Higher body mass index (BMI) and older age are associated with higher risk of developing insertional Achilles tendonopathy, with bone deformity, intratendinous calcifications, and distal tendinosis occurring more frequently in individuals with a higher BMI and older age [21,118,119]. Several genetic variants have been proposed, specifically in relation to Achilles tendon injuries, including COL5A1, tenascin C, and matrix metalloproteinase 3 (MMP3) gene [120,121,122].
7. Calcific Tendonopathy
For the purposes of this paper, calcific tendonopathies are discussed as a unique entity; however, calcifications are considered a feature of tendonopathies and not a stand-alone condition. The reason for separating out this finding here is to draw attention to the differences in treating calcific tendonopathy compared to non-calcific tendonopathy. Calcifications within the tendon may respond to extracorporeal shock wave therapy, prolotherapy, and surgery [123,124,125].
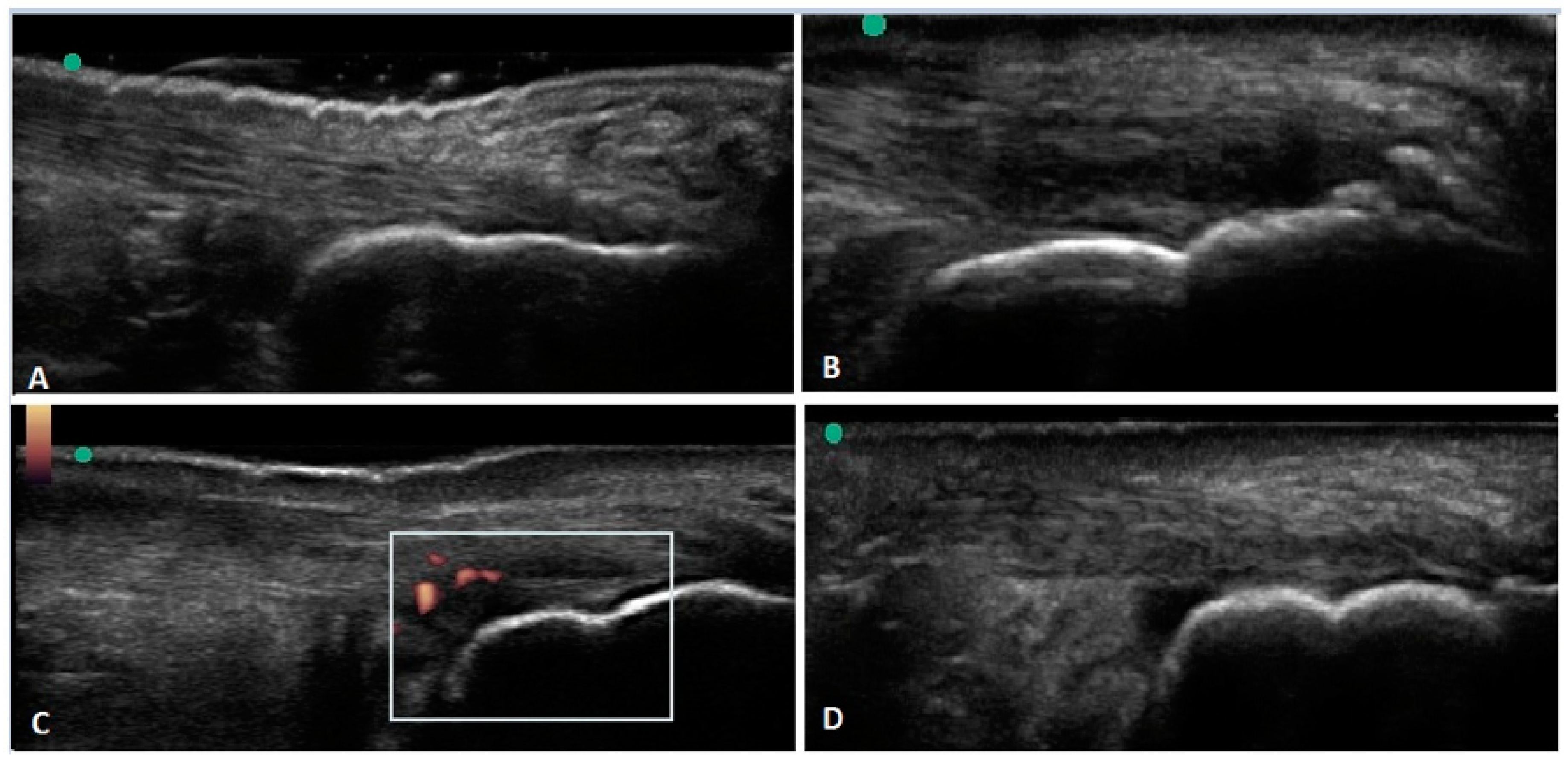
Calcification can occur either at the insertion of the Achilles, termed calcific insertional tendonopathy, or more proximally along the midportion of the Achilles. Dystrophic calcification or ossification may appear on US, appearing as echogenic collections with posterior acoustic shadowing [74]. Calcific insertional tendonopathy is characterized by ossification of the enthesial fibrocartilage with ossification or bone spur formation at the insertion of the tendon [40]. Figure 2B illustrates an example of US findings of calcific tendonopathy.
Given that calcifications of the tendons are not usually classified as a separate entity in the US literature, data on actual specificity and sensitivity of US in assessing calcific tendonopathies as a stand-alone finding is limited, especially with regard to the Achilles tendon. However, there are studies demonstrating high sensitivity for US in identifying shoulder calcific tendonitis [126,127].
8. Retrocalcaneal and Superficial Calcaneal Bursitis
Bursa are synovium-lined, sac-like structures located near bony prominences and between bones, muscles, tendons, and ligaments; bursitis refers to swelling or inflammation of the bursa sacs [128]. Bursitis may occur from overuse, infection, trauma, and inflammatory disorders [129]. There are two noteworthy bursa in the hindfoot, the retrocalcaneal bursa and the superficial calcaneal bursa. Figure 1 illustrates that the retrocalcaneal bursa is deep to the Achilles tendon, adjacent to the calcaneus and the superficial calcaneal bursa is superior to the Achilles tendon. Figure 2D is an example of US findings of retrocalcaneal bursitis.
The retrocalcaneal bursa is a constant bursa that can be visible on US in 25% of healthy individuals [130]. In 1998, Olivieri et al. evaluated the diagnostic accuracy of US in demonstrating hindfoot bursitis [53]. They evaluated 14 patients meeting Amor criteria for spondyloarthropathies. Using MRI as the gold standard, they found that while US had a high specificity, it surprisingly had low sensitivity. They reported US had 50% sensitivity and 100% specificity [53].
9. Paratenonopathy
Unlike most other tendons in the body, the Achilles is surrounded by a paratenon [10,131,132,133,134,135]. A paratenon is loose, vascular, areolar connective tissue surrounding the tendon with a thin layer of synovial cells [37,135,136]. The paratenon is adjacent to the Achilles tendon, located approximately 4–6 cm above the calcaneus; it helps supply blood to the Achilles tendon [136,137,138]. Paratenon abnormalities are more frequently observed on the medial aspect of the Achilles tendon [138]. On US, the paratenon may appear as hypoechoic edematous fat and fluid extending several centimeters craniocaudally [75].
There are limited investigations reviewing ultrasound diagnostic accuracy of paratenonopathies. In 2015, Stecco et al. compared paratenon thickness between healthy and symptomatic individuals [139]. They found the mean value of the paratenon in a normal subject of 0.95 mm (SD 0.16) compared to symptomatic patients who had a mean value of 1.27 mm (SD 0.29). The ultrasound evaluation demonstrated a statistically significant difference of paratenon thickness between normal subjects and symptomatic patients (p = 0.0005). The authors also still found a significant difference in paratenon thickness after controlling for BMI (p = 0.041) [139].
10. Achilles Tendon Tears and Muscle Ruptures
On US, intratendon tears appear as discretely margined defects within the tendon itself [85]. Fluid may be visualized separating the torn margins of the tendon fibers; these may exhibit edge artifact, also known as diffraction shadowing [75,86]. Figure 2C is an example of an intrasubstance Achilles tear. Plantaris ruptures can mimic the appearance of paratenonitis on ultrasound with hypoechoic edematous fat and fluid extending craniocaudally; however, the torn tendon ends can be seen at the margins of the edema [75].
When compared with surgery, US is sensitive and specific for detecting tendon tears [140]. It can also further differentiate partial- from full-thickness tears in the Achilles tendon [133]. Ultrasound has some limitations, however, in differentiating a partial Achilles tendon rupture from a discrete area of tendinosis [141]. Data on diagnostic accuracy of US in diagnosing Achilles ruptures ranges from 79.6% to 100% [60,125,142,143,144].
Griffin et al. determined that performing the Thompson test during the real time Achilles ultrasound test (RAUT) is more sensitive and more specific than traditional (static) ultrasound [142]. For static ultrasound, accuracy was high with a sensitivity and specificity of 76.8% and 74.8% for the novice reviewers and 79.6% and 86.4% for attending reviewers, respectively. The incorporation of RAUT testing increased this further, with a sensitivity and specificity of 87.2% and 81.1% for the novice group and 86.4% and 91.7% for the attending group, respectively [142].
Clinically, Achilles tendon ruptures are more commonly seen in people participating in running, jumping, and agility activities involving eccentric loading and explosive plyometric contractions [145]. In runners, increased femoral anteversion, leg length discrepancy, muscle weakness, increased body mass index, and older age increase intrinsic risk of Achilles tendon rupture [145]. Extrinsic risk factors for tendon tears and ruptures of the Achilles include fluoroquinolones and corticosteroids [146].
11. Conclusions
Ultrasound imaging has proven to be an important tool that can help in localizing more precisely the source of symptoms in the hindfoot and posterior ankle. Pain and/or swelling in this region has a broad differential, focused largely on the Achilles tendon or its adjacent structures. With US, it is possible to visualize these areas. With regard to the enthesis organ, US can further help identify substructures and determine the extent of their involvement. This may help further characterize and classify individuals with enthesopathies. Use of color Doppler may help further identify features more consistent with inflammatory conditions, including enthesitis.
A critical issue with the literature has been inconsistency in describing pathologies of this region. Adoption of a uniform nomenclature involving anatomy and histologic references would be an important step in advancing further research and clinical practice.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflict of interest.
References
- McGonagle, D.; Gibbon, W.; Emery, P. Classification of inflammatory arthritis by enthesitis. Lancet 1998, 352, 1137–1140. [Google Scholar] [CrossRef]
- D’Agostino, M.-A.; Olivieri, I. Enthesitis. Best Pract. Res. Clin. Rheumatol. 2006, 20, 473–486. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, M.-A.; Said-Nahal, R.; Brasseur, J.-L.; Dougados, M.; Breban, M. Assessment of peripheral enthesitis in the spondylarthropathies by ultrasonography combined with power Doppler: A cross-sectional study. Arthritis Rheum. 2003, 48, 523–533. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, M.A.; Aegerter, P.; Bechara, K.; Salliot, C.; Judet, O.; Chimenti, M.S.; Monnet, D.; Le Parc, J.-M.; Landais, P.; Breban, M. How to diagnose spondyloarthritis early? Accuracy of peripheral enthesitis detection by power Doppler ultrasonography. Ann. Rheum. Dis. 2011, 70, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Mease, P.J. Measures of psoriatic arthritis: Tender and Swollen Joint Assessment, Psoriasis Area and Severity Index (PASI), Nail Psoriasis Severity Index (NAPSI), Modified Nail Psoriasis Severity Index (mNAPSI), Mander/Newcastle Enthesitis Index (MEI), Leeds Enthesit. Arthritis Rheum. 2011, 63, S64–S85. [Google Scholar] [CrossRef]
- McGonagle, D.; Stockwin, L.; Isaacs, J.; Emery, P. An enthesitis based model for the pathogenesis of spondyloarthropathy. Additive effects of microbial adjuvant and biomechanical factors at disease sites. J. Rheumatol. 2001, 28, 2155–2159. [Google Scholar]
- Mander, M.; Simpson, J.M.; McLellan, A.; Walker, D.A.; Goodacre, J.; Dick, W.C. Studies with an enthesis index as a method of clinical assessment in ankylosing spondylitis. Ann. Rheum. Dis. 1987, 46, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Klauser, A.S.; Wipfler, E.; Dejaco, C.; Moriggl, B.; Duftner, C.; Schirmer, M. Diagnostic values of history and clinical examination to predict ultrasound signs of chronic and acute enthesitis. Clin. Exp. Rheumatol. 2008, 26, 548–553. [Google Scholar]
- Heuft-Dorenbosch, L.; Spoorenberg, A.; Van Tubergen, A.; Landewé, R.; Tempel, H.V.V.; Mielants, H.; Dougados, M.; Van Der Heijde, D. Assessment of enthesitis in ankylosing spondylitis. Ann. Rheum. Dis. 2003, 62, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Maksymowych, W.P.; Mallon, C.; Morrow, S.; Shojania, K.; Olszynski, W.P.; Wong, R.L.; Sampalis, J.; Conner-Spady, B. Development and validation of the Spondyloarthritis Research Consortium of Canada (SPARCC) Enthesitis Index. Ann. Rheum. Dis. 2008, 68, 948–953. [Google Scholar] [CrossRef]
- Balint, P.V.; Kane, D.; Wilson, H.; McInnes, I.B.; Sturrock, R.D. Ultrasonography of entheseal insertions in the lower limb in spondyloarthropathy. Ann. Rheum. Dis. 2002, 61, 905–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, P.J.; Helliwell, P.S. Measuring clinical enthesitis in psoriatic arthritis: Assessment of existing measures and development of an instrument specific to psoriatic arthritis. Arthritis Rheum. 2008, 59, 686–691. [Google Scholar] [CrossRef]
- Weinfeld, S.B. Achilles Tendon Disorders. Med. Clin. N. Am. 2014, 98, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Puddu, G.; Ippolito, E.; Postacchini, F. A classification of achilles tendon disease. Am. J. Sports Med. 1976, 4, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Kehl, A.S.; Corr, M.; Weisman, M.H. Review: Enthesitis: New Insights into Pathogenesis, Diagnostic Modalities, and Treatment. Arthritis Rheumatol. 2016, 68, 312–322. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Marzo-Ortega, H.; O’Connor, P.; Gibbon, W.; Pease, C.; Reece, R.; Emery, P. The role of biomechanical factors and HLA-B27 in magnetic resonance imaging-determined bone changes in plantar fascia enthesopathy. Arthritis Rheum. 2002, 46, 489–493. [Google Scholar] [CrossRef]
- Erdem, C.; Sarikaya, S.; Erdem, L.; Özdolap, Ş.; Gündoğdu, S. MR imaging features of foot involvement in ankylosing spondylitis. Eur. J. Radiol. 2005, 53, 110–119. [Google Scholar] [CrossRef]
- Kamel, M.; Eid, H.; Mansour, R. Ultrasound detection of heel enthesitis: A comparison with magnetic resonance imaging. J. Rheumatol. 2003, 30, 774–778. [Google Scholar]
- Özdoğan, Ö.; Değirmenci, B.; Şenocak, Ö.; Gülbahar, S.; Arslan, G.; Taşçı, C.; Akalın, E.; Durak, H. Tc-99m HIG Scintigraphy in Detection of Active Inflammation in Ankylosing Spondylitis. Mol. Imaging Radionucl. Ther. 2011, 20, 52–58. [Google Scholar] [CrossRef]
- Østergaard, M.; Lambert, R.G. Imaging in ankylosing spondylitis. Ther. Adv. Musculoskelet. Dis. 2012, 4, 301–311. [Google Scholar] [CrossRef]
- Zellers, J.A.; Bley, B.C.; Pohlig, R.T.; Alghamdi, N.H.; Silbernagel, K.G. Frequency of Pathology on Diagnostic Ultrasound and Relationship to Patient Demographics in Individual with Insertional Achilles Tendonopathy. Int. J. Sports Phys. Ther. 2019, 14, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Loiacono, C.; Palermi, S.; Massa, B.; Belviso, I.; Romano, V.; Di Gregorio, A.; Sirico, F.; Sacco, A.M. Tendonopathy: Pathophysiology, Therapeutic Options, and Role of Nutraceutics. A Narrative Literature Review. Medicina 2019, 55, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charnoff, J.; Naqvi, U. Tendinosis (Tendinitis) [Updated 28 April 2020]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK448174/ (accessed on 11 September 2020).
- Monestime, J.P.; Mayer, R.W.; Blackwood, A. Analyzing the ICD-10-CM Transition and Post-implementation Stages: A Public Health Institution Case Study. Perspect. Health Inf. Manag. 2019, 16, 1a. [Google Scholar] [PubMed]
- ICD-10-CM Code M67.879. ICD List. [Internet] 2020. Available online: https://icdlist.com/icd-10/M67.879 (accessed on 11 September 2020).
- ICD-10-CM Code M67.873. ICD List. [Internet] 2020. Available online: https://icdlist.com/icd-10/M67.873 (accessed on 11 September 2020).
- ICD-10-CM Code M67.874. ICD List. [Internet] 2020. Available online: https://icdlist.com/icd-10/M67.874 (accessed on 11 September 2020).
- ICD-10-CM Code M76.6. ICD.Codes. Available online: https://icd.codes/icd10cm/M766 (accessed on 11 September 2020).
- Almekinders, L.C.; Temple, J.D. Etiology, diagnosis, and treatment of tendonitis: An analysis of the literature. Med. Sci. Sports Exerc. 1998, 30, 1183–1190. [Google Scholar] [CrossRef]
- Khan, K.M.; Cook, J.L.; Kannus, P.; Maffulli, N.; Bonar, S.F. Time to abandon the “tendinitis” myth. BMJ 2002, 324, 626–627. [Google Scholar] [CrossRef]
- Alfredson, H.; Forsgren, S.; Thorsen, K.; Lorentzon, R. In vivo investigation of ECRB tendons with microdialysis technique—no signs of inflammation but high amounts of glutamate in tennis elbow. Acta Orthop. Scand. 2000, 71, 475–479. [Google Scholar] [CrossRef] [Green Version]
- Alfredson, H.; Forsgren, S.; Thorsen, K.; Lorentzon, R. In vivo microdialysis and immunohistochemical analyses of tendon tissue demonstrated high amounts of free glutamate and glutamate NMDAR1 receptors, but no signs of inflammation, in Jumper’s knee. J. Orthop. Res. 2001, 19, 881–886. [Google Scholar] [CrossRef]
- Zamora, A.J.; Marini, J.F. Tendon and myo-tendinous junction in an overloaded skeletal muscle of the rat. Brain Struct. Funct. 1988, 179, 89–96. [Google Scholar] [CrossRef]
- Andres, B.M.; Murrell, G.A. Treatment of tendonopathy: What works, what does not, and what is on the horizon. Clin. Orthop. Relat. Res. 2008, 466, 1539–1554. [Google Scholar] [CrossRef] [Green Version]
- Bass, L.E. Tendinopathy: Why the Difference Between Tendinitis and Tendinosis Matters. Int. J. Ther. Massage Bodyw. Res. Educ. Pr. 2012, 5, 14–17. [Google Scholar] [CrossRef]
- Kaeding, C.; Best, T.M. Tendinosis: Pathophysiology and nonoperative treatment. Sports Health 2009, 1, 284–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, K.M.; Cook, J.L.; Bonar, F.; Astrom, M. Histopathology of common overuse tendon conditions: Update and implications for clinical management. Sports Med. 1999, 27, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Sofka, C.M.; Adler, R.S.; Positano, R.; Pavlov, H.; Luchs, J.S. Haglund’s Syndrome: Diagnosis and Treatment Using Sonography. HSS J. 2006, 2, 27–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haglund, P. Beitrag zur Klinik der Achillessehne. Z. Orthop 1927, 49, 49–58. [Google Scholar]
- Vaishya, R.; Agarwal, A.K.; Azizi, A.T.; Vijay, V. Haglund’s Syndrome: A Commonly Seen Mysterious Condition. Cureus 2016, 8, e820. [Google Scholar] [CrossRef] [Green Version]
- Van Dijk, C.N.; Van Sterkenburg, M.N.; Wiegerinck, J.I.; Karlsson, J.; Maffulli, N. Terminology for Achilles tendon related disorders. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 835–841. [Google Scholar] [CrossRef] [Green Version]
- Sudoł-Szopińska, I.; Kwiatkowska, B.; Prochorec-Sobieszek, M.; Maśliński, W. Enthesopathies and enthesitis. Part 1. Etiopathogenesis. J. Ultrason. 2015, 15, 72–84. [Google Scholar] [CrossRef]
- Sudoł-Szopińska, I.; Kwiatkowska, B.; Prochorec-Sobieszek, M.; Pracoń, G.; Walentowska-Janowicz, M.; Maslinski, W. Enthesopathies and enthesitis. Part 2: Imaging studies. J. Ultrason. 2015, 15, 196–207. [Google Scholar] [CrossRef]
- Shaibani, A.; Workman, R.; Rothschild, B.M. The significance of enthesopathy as a skeletal phenomenon. Clin. Exp. Rheumatol. 1993, 11, 399–403. [Google Scholar]
- Gencc, H.; Cakit, B.D.; Tuncbilek, I.; Erdem, H.R.; Tuncbilek, I. Ultrasonographic evaluation of tendons and enthesal sites in rheumatoid arthritis: Comparison with ankylosing spondylitis and healthy subjects. Clin. Rheumatol. 2004, 24, 272–277. [Google Scholar] [CrossRef]
- Kaeley, G.S. Enthesitis in psoriatic arthritis (Part 2): Imaging. Rheumatology 2020, 59, i15–i20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffulli, N.; Denaro, V.; Loppini, M. Letters to the Editor. Foot Ankle Int. 2012, 33, 807–808. [Google Scholar] [CrossRef] [PubMed]
- Bulstra, G.H.; Van Rheenen, T.A.; Scholtes, V.A. Can We Measure the Heel Bump? Radiographic Evaluation of Haglund’s Deformity. J. Foot Ankle Surg. 2015, 54, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Eshed, I.; Bollow, M.; McGonagle, D.G.; Tan, A.L.; Althoff, C.E.; Asbach, P.; Hermann, K.G.A. MRI of enthesitis of the appendicular skeleton in spondyloarthritis. Ann. Rheum. Dis. 2007, 66, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Barozzi, L.; Olivieri, I.; De Matteis, M.; Padula, A.; Pavlica, P. Seronegative spondylarthropathies: Imaging of spondylitis, enthesitis and dactylitis. Eur. J. Radiol. 1998, 27, S12–S17. [Google Scholar] [CrossRef]
- Haims, A.H.; Schweitzer, M.E.; Patel, R.S.; Hecht, P.; Wapner, K.L. MR imaging of the Achilles tendon: Overlap of findings in symptomatic and asymptomatic individuals. Skelet. Radiol. 2000, 29, 640–645. [Google Scholar] [CrossRef]
- Olivieri, I.; Gemignani, G.; Bini, C.; Grassi, L.; Pasero, G. Diffuse Achilles tendon thickening in juvenile onset seronegative HLA-B27 positive spondyloarthropathy. J. Rheumatol. 1988, 15, 381–382. [Google Scholar]
- Olivieri, I.; Barozzi, L.; Padula, A.; De Matteis, M.; Pierro, A.; Cantini, F.; Salvarani, C.; Pavlica, P. Retrocalcaneal bursitis in spondyloarthropathy: Assessment by ultrasonography and magnetic resonance imaging. J. Rheumatol. 1998, 25, 1352–1357. [Google Scholar]
- Weinreb, J.H.; Sheth, C.; Apostolakos, J.; McCarthy, M.-B.; Barden, B.; Cote, M.P.; Mazzocca, A.D. Tendon structure, disease, and imaging. Muscle Ligaments Tendons J. 2019, 4, 66–73. [Google Scholar] [CrossRef]
- Ring, E.F.J.; Ammer, K. Infrared thermal imaging in medicine. Physiol. Meas. 2012, 33, R33–R46. [Google Scholar] [CrossRef]
- Hildebrandt, C.; Raschner, C.; Ammer, K. An Overview of Recent Application of Medical Infrared Thermography in Sports Medicine in Austria. Sensors 2010, 10, 4700–4715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoksrud, A.; Ohberg, L.; Alfredson, H.; Bahr, R. Color doppler ultrasound findings in patellar tendinopathy (jumper’s knee). Am. J. Sports Med. 2008, 36, 1813–1820. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, S.; Fernando, R.; Screen, H.; Waugh, C.; Tucker, A.; Morrissey, D. The use of medical infrared thermography in the detection of tendinopathy: A systematic review. Phys. Ther. Rev. 2016, 21, 75–82. [Google Scholar] [CrossRef]
- Sanz-López, F.; Martínez-Amat, A.; Hita-Contreras, F.; Valero-Campo, C.; Berzosa, C. Thermographic Assessment of Eccentric Overload Training Within Three Days of a Running Session. J. Strength Cond. Res. 2016, 30, 504–511. [Google Scholar] [CrossRef]
- Kannus, P. Etiology and pathophysiology of chronic tendon disorders in sports. Scand. J. Med. Sci. Sports 1997, 7, 78–85. [Google Scholar] [CrossRef]
- D’Agostino, M.-A.; Breban, M. Ultrasonography in inflammatory joint disease: Why should rheumatologists pay attention? Jt. Bone Spine 2002, 69, 252–255. [Google Scholar] [CrossRef]
- Grassi, W.; Salaffi, F.; Filippucci, E. Ultrasound in rheumatology. Best Pract. Res. Clin. Rheumatol. 2005, 19, 467–485. [Google Scholar] [CrossRef]
- D’Agostino, M.A. Ultrasound imaging in spondyloarthropathies. Best Pract. Res. Clin. Rheumatol. 2010, 24, 693–700. [Google Scholar] [CrossRef]
- Grassi, W.; Filippucci, E.; Farina, A.; Cervini, C. Sonographic imaging of tendons. Arthritis Rheum. 2000, 43, 969–976. [Google Scholar] [CrossRef]
- Grechenig, W.; Clement, H.; Bratschitsch, G.; Fankhauser, F.; Peicha, G. Sonographische Achillessehnendiagnostik [Ultrasound diagnosis of the Achilles tendon]. Orthopade 2002, 31, 319–325. [Google Scholar] [CrossRef]
- Carroll, M.; Dalbeth, N.; Boocock, M.; Rome, K. The assessment of lesions of the Achilles tendon by ultrasound imaging in inflammatory arthritis: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2015, 45, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Paavola, M.; Paakkala, T.; Kannus, P.; Järvinen, M. Ultrasonography in the differential diagnosis of Achilles tendon injuries and related disorders. A comparison between pre-operative ultrasonography and surgical findings. Acta Radiol. 1998, 39, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Terslev, L.; Naredo, E.; Iagnocco, A.; Balint, P.V.; Wakefield, R.J.; Aegerter, P.; Aydin, S.Z.; Bachta, A.; Hammer, H.B.; Bruyn, G.A.W.; et al. Defining Enthesitis in Spondyloarthritis by Ultrasound: Results of a Delphi Process and of a Reliability Reading Exercise. Arthritis Rheum. 2014, 66, 741–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandjbakhch, F.; Terslev, L.; Joshua, F.; Wakefield, R.J.; Naredo, E.; D’Agostino, M.-A.; Force, O.U.T. Ultrasound in the evaluation of enthesitis: Status and perspectives. Arthritis Res. Ther. 2011, 13, R188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodgson, R.J.; O’Connor, P.J.; Grainger, A.J. Tendon and ligament imaging. Br. J. Radiol. 2012, 85, 1157–1172. [Google Scholar] [CrossRef] [Green Version]
- Adler, R.; Sofka, C.M. Percutaneous Ultrasound-Guided Injections in the Musculoskeletal System. Ultrasound Q. 2003, 19, 3–12. [Google Scholar] [CrossRef]
- Kainberger, F.M.; Engel, A.; Barton, P.; Huebsch, P.; Neuhold, A.; Salomonowitz, E. Injury of the Achilles tendon: Diagnosis with sonography. Am. J. Roentgenol. 1990, 155, 1031–1036. [Google Scholar] [CrossRef] [Green Version]
- Bigeleisen, P.E. (Ed.) Ultrasound-Guided Regional Anesthesia and Pain Medicine; Lippincott Williams and Wilkins: London, UK, 2010. [Google Scholar]
- El-Khalek, A.M.A.; Borga, M.; El-Essawya, S.; El Sallab, R.M.; Ezzata, A. Role of ultrasonography in the evaluation of Achilles tendon disorders. Benha Med. J. 2016, 33, 54. [Google Scholar] [CrossRef]
- Robinson, P. Sonography of Common Tendon Injuries. Am. J. Roentgenol. 2009, 193, 607–618. [Google Scholar] [CrossRef]
- Paavola, M.; Kannus, P.; Järvinen, T. Achilles tendonopathy. J. Bone Jt. Surg. 2002, 84, 2062–2076. [Google Scholar] [CrossRef]
- Li, H.Y.; Hua, Y.H. Achilles Tendonopathy: Current Concepts about the Basic Science and Clinical Treatments. Biomed. Res. Int. 2016, 2016, 6492597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegerinck, J.I.; Kerkhoffs, G.M.; van Sterkenburg, M.N.; Sierevelt, I.N.; van Dijk, C.N. Treatment for insertional Achilles tendonopathy: A systematic review. Knee Surg. Sport Traumatol. Arthrosc. 2013, 21, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, P.; Lorentzon, R. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg. Sports Traumatol. Arthrosc. 2003, 11, 327–333. [Google Scholar] [CrossRef]
- Mafi, N.; Lorentzon, R.; Alfredson, H. Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee Surg. Sports Traumatol. Arthrosc. 2000, 9, 42–47. [Google Scholar] [CrossRef]
- Nicholson, C.W.; Berlet, G.C.; Lee, T.H. Prediction of the Success of Nonoperative Treatment of Insertional Achilles Tendinosis Based on MRI. Foot Ankle Int. 2007, 28, 472–477. [Google Scholar] [CrossRef]
- Khan, K.M.; Forster, B.B.; Robinson, J.; Cheong, Y.; Louis, L.; MacLean, L.E.; Taunton, J. Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two year prospective study. Br. J. Sports Med. 2003, 37, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Hirji, Z.; Hunjun, J.S.; Choudur, H.N. Imaging of the Bursae. J. Clin. Imaging Sci. 2011, 1, 22. [Google Scholar] [CrossRef]
- McNally, E.G. Practical Musculoskeletal Ultrasound, 2nd ed.; Elsievier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Brinckmann, P.; Frobin, F.; Leivseth, G. Musculoskeletal Biomechanics; Thieme: New York, NY, USA, 2002. [Google Scholar]
- Berg, K.; Peck, J.; Boulger, C.; Bahner, D.P. Patellar tendon rupture: An ultrasound case report. BMJ Case Rep. 2013, 2013, bcr2012008189. [Google Scholar] [CrossRef] [Green Version]
- Aagesen, A.L.; Melek, M. Choosing the Right Diagnostic Imaging Modality in Musculoskeletal Diagnosis. Prim. Care Clin. Off. Pr. 2013, 40, 849–861. [Google Scholar] [CrossRef]
- O’Connor, P.J.; Grainger, A.J.; Morgan, S.R.; Smith, K.L.; Waterton, J.C.; Nash, A.F.P. Ultrasound assessment of tendons in asymptomatic volunteers: A study of reproducibility. Eur. Radiol. 2004, 14, 1968–1973. [Google Scholar] [CrossRef]
- Ricci, V.; Soylu, A.R.; Özçakar, L. Artifacts and Artistic Facts. Am. J. Phys. Med. Rehabil. 2019, 98, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Baad, M.; Lu, Z.F.; Reiser, I.; Paushter, D. Clinical Significance of US Artifacts. Radiographics 2017, 37, 1408–1423. [Google Scholar] [CrossRef] [PubMed]
- Fornage, B.D. The hypoechoic normal tendon. A pitfall. J. Ultrasound Med. 1987, 6, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.-T.; Chang, K.-V.; Hsu, Y.-C.; Hsu, P.-C.; Ricci, V.; Özçakar, L. Artifacts in Musculoskeletal Ultrasonography: From Physics to Clinics. Diagnostics 2020, 10, 645. [Google Scholar] [CrossRef] [PubMed]
- De Miguel, E.; Muñoz-Fernández, S.; Castillo, C.; Cobo-Ibáñez, T.; Martín-Mola, E. Diagnostic accuracy of enthesis ultrasound in the diagnosis of early spondyloarthritis. Ann. Rheum. Dis. 2010, 70, 434–439. [Google Scholar] [CrossRef]
- Czyrny, Z. Diagnostic anatomy and diagnostics of enthesal pathologies of the rotator cuff. J. Ultrason. 2012, 12, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Dębek, A.; Nowicki, P.; Czyrny, Z. Ultrasonographic diagnostics of pain in the lateral cubital compartment and proximal forearm. J. Ultrason. 2012, 12, 188–201. [Google Scholar] [CrossRef] [Green Version]
- Feydy, A.; Lavie-Brion, M.-C.; Gossec, L.; Lavie, F.; Guerini, H.; Nguyen, C.; Rannou, F.; Drapé, J.-L.; Dougados, M. Comparative study of MRI and power Doppler ultrasonography of the heel in patients with spondyloarthritis with and without heel pain and in controls. Ann. Rheum. Dis. 2011, 71, 498–503. [Google Scholar] [CrossRef]
- Czyrny, Z. Sonographic and histological appearance of heel enthesopathy, what the “heel spurs” really are and what are their consequences. J. Ortop. Trauma Surg. Relat. Res. 2010, 2, 23–36. [Google Scholar]
- Maffulli, N.; Kader, D. Tendonopathy of tendo Achillis. J. Bone Jt. Surg. 2002, 84, 1–8. [Google Scholar] [CrossRef]
- D’Agostino, M.A.; Aegerter, P.; Jousse-Joulin, S.; Chary-Valckenaere, I.; Lecoq, B.; Gaudin, P.; Brault, I.; Schmitz, J.; Dehaut, F.-X.; Le Parc, J.-M.; et al. How to evaluate and improve the reliability of power Doppler ultrasonography for assessing enthesitis in spondyloarthritis. Arthritis Rheum. 2009, 61, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Poulain, C.; D’Agostino, M.A.; Thibault, S.; Daures, J.P.; Ferkal, S.; Le Corvoisier, P.; Rahmouni, A.; Loeuille, D.; Dougados, M.; Claudepierre, P. Can power Doppler ultrasound of the entheses help in classifying recent axial spondyloarthritis? Data from the DESIR cohort. RMD Open 2018, 4, e000686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippucci, E.; Aydin, S.Z.; Karadag, O.; Salaffi, F.; Gutierrez, M.; Direskeneli, H.; Grassi, W. Reliability of high-resolution ultrasonography in the assessment of Achilles tendon enthesopathy in seronegative spondyloarthropathies. Ann. Rheum. Dis. 2009, 68, 1850–1855. [Google Scholar] [CrossRef] [PubMed]
- De Miguel, E.; Cobo, T.; Rubio-Muñoz, P.; Naredo, E.; Usón, J.; Acebes, J.C.; Andréu, J.L.; Martín-Mola, E. Validity of enthesis ultrasound assessment in spondyloarthropathy. Ann. Rheum. Dis. 2008, 68, 169–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiris, A.; Kaya, A.; Ozgocmen, S.; Kocakoc, E. Assessment of enthesitis in ankylosing spondylitis by power Doppler ultrasonography. Skelet. Radiol. 2006, 35, 522–528. [Google Scholar] [CrossRef]
- Ahmed, M.M.; Elolemy, G.G.; Alfeeli, A.K.; Baqer, A.B.; Gad, A.M. Ultrasonographic Enthesopathy and Disease Activity in Psoriatic Arthritis. Open Access Maced. J. Med Sci. 2017, 5, 651–656. [Google Scholar] [CrossRef] [Green Version]
- Helliwell, P.S.; Fitzgerald, O.; Fransen, J.; Gladman, D.D.; Kreuger, G.G.; Duffin, K.C.; McHugh, N.; Mease, P.; Strand, V.; Waxman, R.; et al. The development of candidate composite disease activity and responder indices for psoriatic arthritis (GRACE project). Ann. Rheum. Dis. 2012, 72, 986–991. [Google Scholar] [CrossRef] [Green Version]
- Alcalde, M.; Acebes, J.C.; Cruz, M.; González-Hombrado, L.; Herrero-Beaumont, G.; Sánchez-Pernaute, O. A Sonographic Enthesitic Index of lower limbs is a valuable tool in the assessment of ankylosing spondylitis. Ann. Rheum. Dis. 2007, 66, 1015–1019. [Google Scholar] [CrossRef] [Green Version]
- Kaeley, G.S.; Eder, L.; Aydin, S.Z.; Gutierrez, M.; Bakewell, C. Enthesitis: A hallmark of psoriatic arthritis. Semin. Arthritis Rheum. 2018, 48, 35–43. [Google Scholar] [CrossRef]
- Gisondi, P.; Tinazzi, I.; El-Dalati, G.; Gallo, M.; Biasi, D.; Barbara, L.M.; Girolomoni, G. Lower limb enthesopathy in patients with psoriasis without clinical signs of arthropathy: A hospital-based case-control study. Ann. Rheum. Dis. 2008, 67, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Eder, L.; Jayakar, J.; Thavaneswaran, A.; Haddad, A.; Chandran, V.; Salonen, D.; Rosen, C.F.; Gladman, D.D. Is the Madrid Sonographic Enthesitis Index Useful for Differentiating Psoriatic Arthritis from Psoriasis Alone and Healthy Controls? J. Rheumatol. 2014, 41, 466–472. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Can, M.; Alibaz-Oner, F.; Keser, G.; Kurum, E.; Inal, V.; Yazisiz, V.; Birlik, M.; Emmungil, H.; Atagunduz, P.; et al. A relationship between spinal new bone formation in ankylosing spondylitis and the sonographically determined Achilles tendon enthesophytes. Rheumatol. Int. 2016, 36, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.Z.; Filippucci, E.; Atagunduz, P.; Yavuz, S.; Grassi, W.; Direskeneli, H.; Aydin, S.Z. Sonographic measurement of Achilles tendon thickness in seronegative spondyloarthropathies. Eur. J. Rheumatol. 2014, 1, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Boezaart, A.P.; Ihnatsenka, B. Ultrasound: Basic understanding and learning the language. Int. J. Shoulder Surg. 2010, 4, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoirs, K.A.; Childs, J.T. Are Ultrasound Measurements of Achilles Tendon Size Reliable? A Systematic Review of Rater Reliability. Ultrasound Med. Biol. 2018, 44, 2476–2491. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.N.; Labib, S.A. The Achilles Tendon in Healthy Subjects: An Anthropometric and Ultrasound Mapping Study. J. Foot Ankle Surg. 2018, 57, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Holmes, G.B.; Lin, J. Etiologic factors associated with symptomatic Achilles tendonopathy. Foot Ankle Int. 2006, 27, 952–959. [Google Scholar] [CrossRef]
- Gaida, J.E.; Alfredson, L.; Kiss, Z.S.; Wilson, A.; Alfredson, H.; Cook, J. Dyslipidemia in Achilles tendonopathy is characteristic of insulin resistance. Med. Sci. Sports Exerc. 2009, 41, 1194–1197. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, F.; Papalia, R.; Paciotti, M.; Franceschetti, E.; Di Martino, A.; Maffulli, N.; Denaro, V. Obesity as a risk factor for tendonopathy: A systematic review. Int. J. Endocrinol. 2014, 1, 10. [Google Scholar]
- Scott, R.T.; Hyer, C.F.; Granata, A. The correlation of Achilles tendonopathy and body mass index. Foot Ankle Spec. 2013, 6, 283–285. [Google Scholar] [CrossRef]
- Mokone, G.G.; Schwellnus, M.P.; Noakes, T.D.; Collins, M. The COL5A1 gene and Achilles tendon pathology. Scand. J. Med. Sci. Sports 2006, 16, 19–26. [Google Scholar] [CrossRef]
- Mokone, G.G.; Gajjar, M.; September, A.V.; Schwellnus, M.P.; Greenberg, J.; Noakes, T.D.; Collins, M. The Guanine-Thymine Dinucleotide Repeat Polymorphism within the Tenascin-C Gene is Associated with Achilles Tendon Injuries. Am. J. Sports Med. 2005, 33, 1016–1021. [Google Scholar] [CrossRef] [PubMed]
- Raleigh, S.M.; van der Merwe, L.; Ribbans, W.J.; Smith, R.K.; Schwellnus, M.P.; Collins, M. Variants within the MMP3 gene are associated with Achilles tendonopathy: Possible interaction with the COL5A1 gene. Br. J. Sports Med. 2009, 43, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Zhang, J.; Cai, Y. Utility of ultrasonography in assessing the effectiveness of extracorporeal shock wave therapy in insertional Achilles tendonopathy. BioMed Res. Int. 2016, 2016, 2580969. [Google Scholar] [CrossRef] [PubMed]
- Johansson, K.; Sarimo, J.J.; Lempainen, L.L.; Laitala-Leinonen, T.; Orava, S.Y. Calcific spurs at the insertion of the Achilles tendon: A clinical and histological study. Muscle Ligaments Tendons J. 2013, 2, 273–277. [Google Scholar]
- Buchanan, B.K.; DeLuca, J.P.; Lammlein, K.P. Technical Innovation Case Report: Ultrasound-Guided Prolotherapy Injection for Insertional Achilles Calcific Tendinosis. Case Reports Orthop. 2016, 2016, 1560161. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.S.; Rosas, H.; Craig, J. Musculoskeletal Ultrasound: Elbow Imaging and Procedures. Semin. Musculoskelet. Radiol. 2010, 14, 449–460. [Google Scholar] [CrossRef]
- Martín-Hervás, C.; Romero, J.; Navas-Acién, A.; Reboiras, J.J.; Munuera, L. Ultrasonographic and magnetic resonance images of rotator cuff lesions compared with arthroscopy or open surgery findings. J. Shoulder Elb. Surg. 2001, 10, 410–415. [Google Scholar] [CrossRef]
- Williams, C.H.; Sternard, B.T. Bursitis. [Updated 2020 Aug 15]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513340/ (accessed on 12 September 2020).
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG). 2006; Bursitis: Overview. 26 July 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK525773/# (accessed on 12 September 2020).
- Schmidt, W.A.; Schmidt, H.; Schicke, B.; Gromnica-Ihle, E. Standard reference values for musculoskeletal ultrasonography. Ann. Rheum. Dis. 2004, 63, 988–994. [Google Scholar] [CrossRef] [Green Version]
- Hartgerink, P.; Fessell, D.P.; Jacobson, J.A.; Van Holsbeeck, M.T. Full-versus Partial-Thickness Achilles Tendon Tears: Sonographic Accuracy and Characterization in 26 Cases with Surgical Correlation. Radiology 2001, 220, 406–412. [Google Scholar] [CrossRef]
- Martinoli, C.E.; Derchi, L.; Pastorino, C.; Bertolotto, M.; Silvestri, E. Analysis of echotexture of tendons with US. Radiology 1993, 186, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Asplund, C.A.; Best, T.M. Achilles tendon disorders. BMJ 2013, 346, f1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agur, A. Grant’s Atlas of Anatomy, 9th ed.; Williams and Wilkins: Baltimore, MD, USA, 1991. [Google Scholar]
- Robinson, P.; White, L.M. The Biomechanics and Imaging of Soccer Injuries. Semin. Musculoskelet. Radiol. 2005, 9, 397–420. [Google Scholar] [CrossRef] [PubMed]
- Teitz, C.C.; Garrett, W.E.J.; Miniaci, A.; Lee, M.H.; Mann, R.A. Tendon Problems in Athletic Individuals. J. Bone Jt. Surg. Am. Vol. 1997, 79, 138–152. [Google Scholar] [CrossRef]
- Scheller, A.D.; Kasser, J.R.; Quigley, T.B. Tendon injuries about the ankle. Orthop. Clin. N. Am. 1980, 11, 801–811. [Google Scholar]
- Rees, J.; Maffulli, N.; Cook, J. Management of tendonopathy. Am. J. Sports Med. 2009, 37, 1855–1867. [Google Scholar] [CrossRef]
- Stecco, A.; Busoni, F.; Stecco, C.; Mattioli-Belmonte, M.; Soldani, P.; Condino, S.; Ermolao, A.; Zaccaria, M.; Gesi, M. Comparative ultrasonographic evaluation of the Achilles paratenon in symptomatic and asymptomatic subjects: An imaging study. Surg. Radiol. Anat. 2014, 37, 281–285. [Google Scholar] [CrossRef]
- Goodwin, D.W. Imaging of the Achilles’ tendon. Foot Ankle Clin. 2000, 5, 135–148. [Google Scholar]
- Waitches, G.M.; Rockett, M.; Brage, M.; Sudakoff, G. Ultrasonographic-surgical correlation of ankle tendon tears. J. Ultrasound Med. 1998, 17, 249–256. [Google Scholar] [CrossRef]
- Griffin, M.J.; Olson, K.; Heckmann, N.; Charlton, T.P. Realtime Achilles Ultrasound Thompson (RAUT) Test for the Evaluation and Diagnosis of Acute Achilles Tendon Ruptures. Foot Ankle Int. 2016, 38, 36–40. [Google Scholar] [CrossRef]
- Grechenig, W.; Clement, H.G.; Fellinger, M. Value of ultrasound imaging of the Achilles tendon in traumatology. Radiologe 1997, 37, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Margetic, P.; Miklić, D.; Rakić-Ersek, V.; Doko, Z.; Lubina, Z.I.; Brkljacić, B. Comparison of ultrasonographic and intraoperative findings in Achilles tendon rupture. Coll. Antropol. 2007, 31, 279–284. [Google Scholar] [PubMed]
- Hess, G.W. Achilles tendon rupture: A review of etiology, population, anatomy, risk factors, and injury prevention. Foot Ankle Spec. 2010, 3, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Zabraniecki, L.; Negrier, I.; Vergne, P.; Arnaud, M.; Bonnet, C.; Bertin, P.; Treves, R. Fluoroquinolone induced tendonopathy: Report of 6 cases. J. Rheumatol. 1996, 23, 516–520. [Google Scholar] [PubMed]
- Aström, M. Partial rupture in chronic Achilles tendonopathy. A retrospective analysis of 342 cases. Acta Orthop. Scand. 1998, 69, 404–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Hindfoot and posterior ankle anatomy.

Figure 2.
Ultrasound imaging of Achilles tendon. Figure 2 illustrates several examples of ultrasound findings in the posterior ankle and hindfoot. (A) Normal imaging of hindfoot/posterior ankle. (B) Insertional Achilles calcific tendonopathy. (C) Intrasubstance Achilles tear with surrounding neovascularization. (D) Retrocalcaneal bursitis. Note the green dot indicates probe orientation. The box in C is the color box indicating the region of color Doppler assessment.
Figure 2.
Ultrasound imaging of Achilles tendon. Figure 2 illustrates several examples of ultrasound findings in the posterior ankle and hindfoot. (A) Normal imaging of hindfoot/posterior ankle. (B) Insertional Achilles calcific tendonopathy. (C) Intrasubstance Achilles tear with surrounding neovascularization. (D) Retrocalcaneal bursitis. Note the green dot indicates probe orientation. The box in C is the color box indicating the region of color Doppler assessment.


{kind=link}
{kind=link}
Table 1.
Etiologies for hindfoot and posterior ankle pain and/or swelling.
| Differential Diagnoses for Conditions of the Achilles Region |
|---|
| Midportion Achilles tendonopathy |
| Insertional Achilles tendonopathy * |
| Achilles paratenonopathy |
| Midportion Achilles calcific tendonopathy |
| Insertional Achilles calcific tendonopathy * |
| Enthesopathy |
| Retrocalcaneal bursitis *,¶ |
| Superficial calcaneal bursitis |
| Os trigonum syndrome |
| Tophaceous gout |
| Calcium pyrophosphate deposition disease |
| Achilles tendon xanthomata |
| Ruptured gastrocnemius |
| Ruptured plantaris |
| Ruptured popliteal cyst with extravasation down gastrocnemius |
| Calcaneal ossification (also known as Haglund deformity) ¶ |
Note: the above terms with the suffix -opathy include their respective -itis and -osis subclassifications. * Features of enthesitis. ¶ Features of Haglund syndrome.
Table 2.
Ultrasound findings for Achilles tendon pathologies.
| Condition | Ultrasound Findings | References |
|---|---|---|
| Enthesopathy |
| [9,10,11,12,66,69] |
| Tendonopathy |
| [70,71,72,73,74,75,76,77,78,79,80,81,82] |
| Bursitis |
| [83] |
| Paratenonopathy |
| [75,84] |
| Tendon tear |
| [75,85,86] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mascarenhas, S. A Narrative Review of the Classification and Use of Diagnostic Ultrasound for Conditions of the Achilles Tendon. Diagnostics 2020, 10, 944. https://doi.org/10.3390/diagnostics10110944
AMA Style
Mascarenhas S. A Narrative Review of the Classification and Use of Diagnostic Ultrasound for Conditions of the Achilles Tendon. Diagnostics. 2020; 10(11):944. https://doi.org/10.3390/diagnostics10110944
Chicago/Turabian StyleMascarenhas, Sheryl. 2020. "A Narrative Review of the Classification and Use of Diagnostic Ultrasound for Conditions of the Achilles Tendon" Diagnostics 10, no. 11: 944. https://doi.org/10.3390/diagnostics10110944
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.