
Clinical Outcome of Discordant Empirical Therapy and Risk Factors Associated to Treatment Failure in Children Hospitalized for Urinary Tract Infections

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Methods
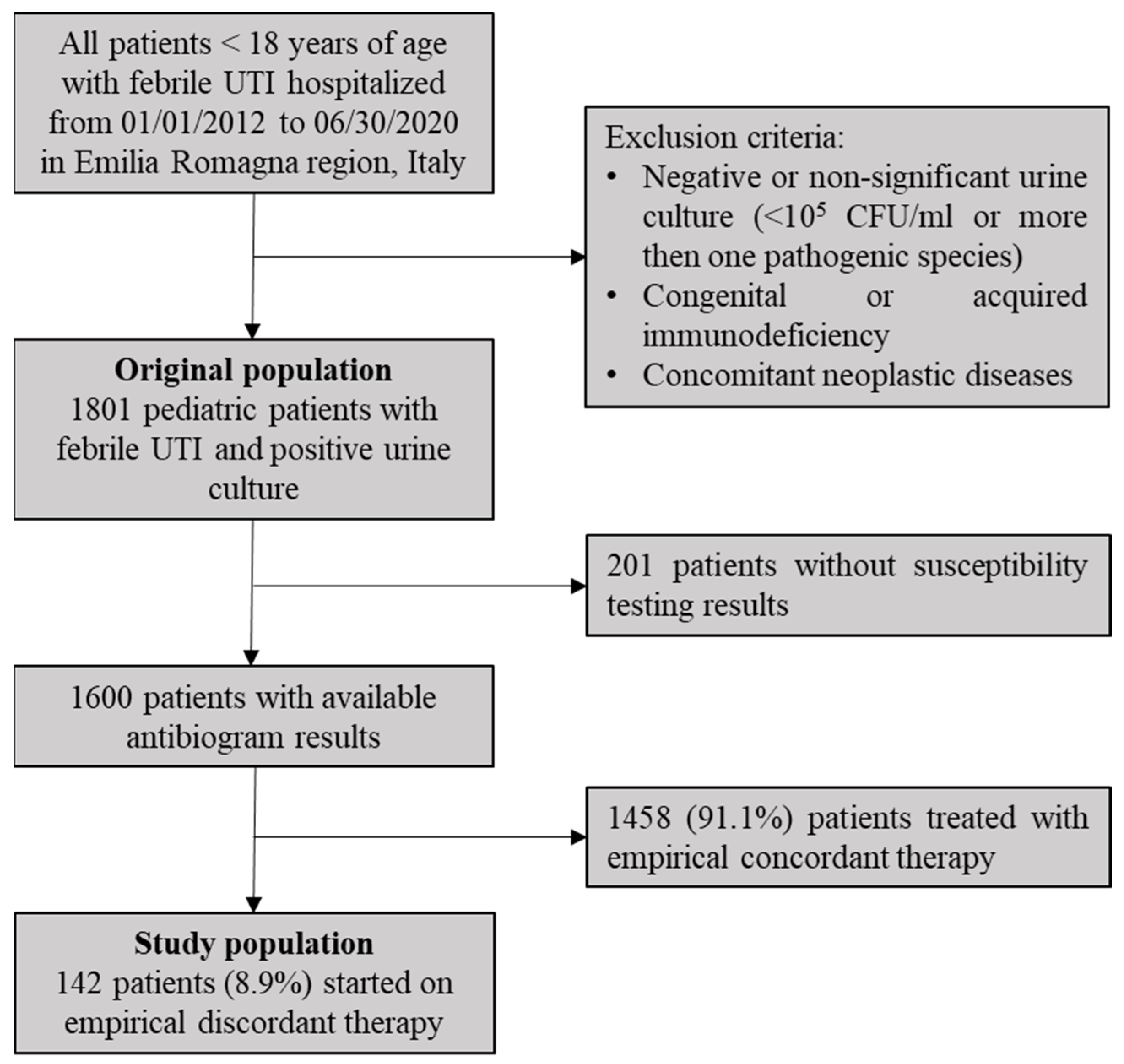
2.1. Study Design and Population
2.2. Data Evaluation
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spencer, J.D.; Schwaderer, A.; McHugh, K.; Hains, D.S. Pediatric urinary tract infections: An analysis of hospitalizations, charges, and costs in the USA. Pediatr Nephrol. 2010, 25, 2469–2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedman, A.L. Urologic Diseases in America Project. Urologic diseases in North America Project: Trends in resource utilization for urinary tract infections in children. J. Urol. 2005, 173, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Montini, G.; Tullus, K.; Hewitt, I. Febrile urinary tract infections in children. N. Engl. J. Med. 2011, 365, 239–250. [Google Scholar] [CrossRef]
- Keren, R.; Shaikh, N.; Pohl, H.; Gravens-Mueller, L.; Ivanova, A.; Zaoutis, L.; Patel, M.; Deberardinis, R.; Parker, A.; Bhatnagar, S.; et al. Risk Factors for Recurrent Urinary Tract Infection and Renal Scarring. Pediatrics 2015, 136, e13–e21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copp, H.L.; Halpern, M.S.; Maldonado, Y.; Shortliffe, L.D. Trends in hospitalization for pediatric pyelonephritis: A population based study of California from 1985 to 2006. J. Urol. 2011, 186, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Saperston, K.N.; Shapiro, D.J.; Hersh, A.L.; Copp, H.L. A Comparison of Inpatient vs. Outpatient Resistance Patterns of Pediatric Urinary Tract Infection. J. Urol. 2014, 191, 1608–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakran, W.; Smolkin, V.; Odetalla, A.; Halevy, R.; Koren, A. Community-acquired urinary tract infection in hospitalized children: Etiology and antimicrobial resistance. A comparison between first episode and recurrent infection. Clin. Pediatr. 2015, 54, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Penna, F.J.; Eleswarapu, S.; Pucheril, D.; Weaver, J.; Abd-El-Barr, A.-E.; Wagner, J.C.; Lakshmanan, Y.; Menon, M.; Trinh, Q.-D.; et al. Incidence, admission rates, and economic burden of pediatric emergency department visits for urinary tract infection: Data from the nationwide emergency department sample, 2006 to 2011. J. Pediatr. Urol. 2015, 11, 246.e1–246.e8. [Google Scholar] [CrossRef]
- Nieminen, O.; Korppi, M.; Helminen, M. Healthcare costs doubled when children had urinary tract infections caused by extended-spectrum β-lactamase-producing bacteria. Acta. Paediatr. 2017, 106, 327–333. [Google Scholar] [CrossRef]
- Bryce, A.; Costelloe, C.; Wootton, M.; Butler, C.C.; Hay, A.D. Comparison of risk factors for, and prevalence of, antibiotic resistance in contaminating and pathogenic urinary Escherichia coli in children in primary care: Prospective cohort study. J. Antimicrob. Chemother. 2018, 73, 1359–1367. [Google Scholar] [CrossRef] [Green Version]
- Esposito, S.; Maglietta, G.; Di Costanzo, M.; Ceccoli, M.; Vergine, G.; La Scola, C.; Malaventura, C.; Falcioni, A.; Iacono, A.; Crisafi, A.; et al. Retrospective 8-Year Study on the Antibiotic Resistance of Uropathogens in Children Hospitalised for Urinary Tract Infection in the Emilia-Romagna Region, Italy. Antibiotics 2021, 10, 1207. [Google Scholar] [CrossRef]
- Copp, H.L.; Shapiro, D.J.; Hersh, A.L. National ambulatory antibiotic prescribing patterns for pediatric urinary tract infection, 1998–2007. Pediatrics 2011, 127, 1027–1033. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, I.K.; Zucchetta, P.; Rigon, L.; Maschio, F.; Molinari, P.P.; Tomasi, L.; Toffolo, A.; Pavanello, L.; Crivellaro, C.; Bellato, S.; et al. Early treatment of acute pyelonephritis in children fails to reduce renal scarring: Data from the Italian Renal Infection Study Trials. Pediatrics 2008, 122, 486–490. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, N.; Mattoo, T.K.; Keren, R.; Ivanova, A.; Cui, G.; Moxey-Mims, M.; Majd, M.; Ziessman, H.A.; Hoberman, A. Early Antibiotic Treatment for Pediatric Febrile Urinary Tract Infection and Renal Scarring. JAMA Pediatr. 2016, 170, 848–854. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics. Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Urinary Tract Infection in under 16s: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/cg54 (accessed on 2 November 2021).
- Frimodt-Møller, N. Correlation between pharmacokinetic/pharmacodynamic parameters and efficacy for antibiotics in the treatment of urinary tract infection. Int. J. Antimicrob. Agents 2002, 19, 546–553. [Google Scholar] [CrossRef]
- Mark, D.G.; Hung, Y.-Y.; Salim, Z.; Tarlton, N.J.; Torres, E.; Frazee, B.W. Third-Generation Cephalosporin Resistance and Associated Discordant Antibiotic Treatment in Emergency Department Febrile Urinary Tract Infections. Ann. Emerg. Med. 2021, 78, 357–369. [Google Scholar] [CrossRef]
- Frazee, B.W.; Trivedi, T.; Montgomery, M.; Petrovic, D.F.; Yamaji, R.; Riley, L. Emergency Department Urinary Tract Infections Caused by Extended-Spectrum beta-Lactamase-Producing Enterobacteriaceae: Many Patients Have No Identifiable Risk Factor and Discordant Empiric Therapy Is Common. Ann. Emerg. Med. 2018, 72, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Jerardi, K.E.; Auger, K.A.; Shah, S.S.; Hall, M.; Hain, P.D.; Myers, A.L.; Williams, D.J.; Tieder, J.S. Discordant antibiotic therapy and length of stay in children hospitalized for urinary tract infection. J. Hosp. Med. 2012, 7, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Zhu, F.H.; Rodado, M.P.; Asmar, B.I.; Salimnia, H.; Thomas, R.; Abdel-Haq, N. Risk factors for community acquired urinary tract infections caused by extended spectrum β-lactamase (ESBL) producing Escherichia coli in children: A case control study. Infect. Dis. 2019, 51, 802–809. [Google Scholar] [CrossRef]
- Selekman, R.E.; Shapiro, D.J.; Boscardin, J.; Williams, G.; Craig, J.C.; Brandström, P.; Pennesi, M.; Roussey-Kesler, G.; Hari, P.; Copp, H.L. Uropathogen Resistance and Antibiotic Prophylaxis: A Meta-analysis. Pediatrics 2018, 142, e20180119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, R.; Dogan, H.S.; Hoebeke, P.; Kočvara, R.; Nijman, R.J.; Radmayr, C.; Tekgül, S. European Association of Urology; European Society for Pediatric Urology. Urinary tract infections in children: EAU/ESPU guidelines. Eur. Urol. 2015, 67, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Bitsori, M.; Maraki, S.; Koukouraki, S.; Galanakis, E. Pseudomonas aeruginosa urinary tract infection in children: Risk factors and outcomes. J. Urol. 2012, 187, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Montini, G.; Toffolo, A.; Zucchetta, P.; Dall’Amico, R.; Gobber, D.; Calderan, A.; Maschio, F.; Pavanello, L.; Molinari, P.P.; Scorrano, D.; et al. Antibiotic treatment for pyelonephritis in children: Multicentre randomised controlled non-inferiority trial. BMJ 2007, 335, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhaus, T.J.; Berger, C.; Buechner, K.; Parvex, P.; Bischoff, G.; Goetschel, P.; Husarik, D.; Willi, U.; Molinari, L.; Rudin, C.; et al. Randomised trial of oral versus sequential intravenous/oral ephalosporins in children with pyelonephritis. Eur. J. Pediatr. 2008, 167, 1037–1047. [Google Scholar] [CrossRef]
- Strohmeier, Y.; Hodson, E.M.; Willis, N.S.; Webster, A.; Craig, J. Antibiotics for acute pyelonephritis in children. Cochrane Database Syst. Rev. 2014, 7, CD003772. [Google Scholar] [CrossRef]
- Wang, M.E.; Lee, V.; Greenhow, T.L.; Beck, J.; Bendel-Stenzel, M.; Hames, N.; McDaniel, C.; King, E.; Sherry, W.; Parmar, D.; et al. Clinical Response to Discordant Therapy in Third-Generation Cephalosporin-Resistant UTIs. Pediatrics 2020, 145, e20191608. [Google Scholar] [CrossRef]
- Madhi, F.; Jung, C.; Timsit, S.; Levy, C.; Biscardi, S.; Lorrot, M.; Grimprel, E.; Hees, L.; Craiu, I.; Galerne, A.; et al. Urinary-tract Infection due to Extended-Spectrum Beta-lactamase–producing Enterobacteriaceae in Children Group. Febrile urinary-tract infection due to extended-spectrum beta-lactamase-producing Enterobacteriaceae in children: A French prospective multicenter study. PLoS ONE 2018, 13, e0190910. [Google Scholar]
- Chastain, D.B.; King, S.T.; Stover, K.R. Rethinking urinary antibiotic breakpoints: Analysis of urinary antibiotic concentrations to treat multidrug resistant organisms. BMC Res. Notes 2018, 11, 497. [Google Scholar] [CrossRef]
- Zhao, F.; Yang, H.; Bi, D.; Khaledi, A.; Qiao, M. A systematic review and meta-analysis of antibiotic resistance patterns, and the correlation between biofilm formation with virulence factors in uropathogenic E. coli isolated from urinary tract infections. Microb. Pathog. 2020, 144, 104196. [Google Scholar] [CrossRef]
- González, M.J.; Robino, L.; Iribarnegaray, V.; Zunino, P.; Scavone, P. Effect of different antibiotics on biofilm produced by uropathogenic Escherichia coli isolated from children with urinary tract infection. Pathog. Dis. 2017, 75, ftx053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venekamp, R.P.; Sanders, S.L.; Glasziou, P.P.; Del Mar, C.B.; Rovers, M.M. Antibiotics for acute otitis media in children. Cochrane Database Syst. Rev. 2015, 6, CD000219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: Systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Kang, H.; Kwak, E.; Rhim, J.-W.; Ahn, Y.; Lee, H.; Jeong, D.; Kang, J. Impact of Antibiotic Prescribing Patterns on Susceptibilities of Uropathogens in Children below 24 Months Old. Antibiotics 2020, 9, 915. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | N = 142 |
|---|---|
| Mean age, years (SD) | 1.8 (3.1) |
| Sex, n | |
| Males | 85 (59.9%) |
| Females | 57 (40.1%) |
| Prenatal pyelectasis, n | 15 (10.6%) |
| Prematurity at birth, n | 27 (19.0%) |
| Urological malformations, n | 23 (16.2%) |
| VUR, n | 13 (9.1%) |
| History of recurrent UTIs, n | 23 (16.2%) |
| Antibiotic prophylaxis, n | 13 (9.1%) |
| Antibiotic therapy in previous 30 days, n | 19 (13.4%) |
| Pyelectasis, n | 49 (34.5%) |
| Mean CRP, mg/dL (SD) | 7.4 (8.3) |
| Mean WBC count, cell/mm3 (SD) | 15,257.3 (5828.0) |
| Mean treatment delay from fever onset, days (SD) | 1.6 (1.5) |
| Pathogens | n (%) | Treatment Failure n (%) |
|---|---|---|
| Escherichia coli | 105 (73.9) | 48 (45.7) |
| Klebsiella spp. | 13 (9.1) | 7 (53.8) |
| Enterobacter spp. | 11 (7.7) | 4 (36.4) |
| Pseudomonas aeruginosa | 7 (4.9) | 6 (85.7) |
| Enterococcus faecalis | 2 (1.4) | 1 (50.0) |
| Proteus mirabilis | 2 (1.4) | 1 (50.0) |
| Citrobacter spp. | 2 (1.4) | - |
| ESBL | 24 (16.9) | 13 (54.2) |
| MDR/XDR | 34 (23.9) | 20 (58.8) |
| Simple resistance | 105 (73.9) | 45 (42.8) |
| Empirical Therapy | n (%) | Treatment Failure (%) |
|---|---|---|
| Penicillin/beta-lactamase inhibitor combinations | 63 (44.4) | 36 (57.1) |
| Penicillin/aminoglycoside combinations | 31 (21.8) | 11 (35.5) |
| 3rd-generation cephalosporins | 28 (19.7) | 11 (39.3) |
| Penicillins | 11 (7.7) | 4 (36.4) |
| Cephalosporin/aminoglycoside combinations | 3 (2.1) | 1 (33.3) |
| Aminoglycosides | 1 (0.7) | - |
| 2nd-generation cephalosporins | 1 (0.7) | 1 (100) |
| Fluoroquinolones | 1 (0.7) | 1 (100) |
| Other | 3 (2.1) | - |
| Parameter | Odds Ratio (OR) | 95 % CI | p Value |
|---|---|---|---|
| Male | 0.69 | 0.35–1.36 | 0.29 |
| Age groups | |||
| <3 months | 1.00 | ||
| 3 months–2 years | 1.94 | 0.89–4.20 | 0.09 |
| 2–6 years | 1.76 | 0.53–5.88 | 0.35 |
| >6 years | 2.20 | 0.73–6.65 | 0.16 |
| History of recurrent UTIs | 3.23 | 1.13–9.98 | <0.05 |
| VUR | 1.67 | 0.42–7.44 | 0.42 |
| Urological malformations | 1.98 | 0.55–7.97 | 0.23 |
| Pyelectasis | 1.54 | 0.69–3.45 | 0.25 |
| Antibiotic prophylaxis | 1.10 | 0.28–4.58 | 0.88 |
| Antibiotic therapy in previous 30 days | 5.02 | 1.46–21.82 | <0.01 |
| ESBL | 1.36 | 0.51–3.70 | 0.49 |
| MDR/XDR | 1.85 | 0.79–4.40 | 0.12 |
| Simple resistance pattern | 0.51 | 0.22–1.16 | 0.08 |
| Escherichia coli | 0.80 | 0.35–1.81 | 0.55 |
| Pseudomonas aeruginosa | 7.30 | 1.85–62.10 | <0.05 |
| Klebsiella spp. | 1.34 | 0.36–5.10 | 0.61 |
| Enterobacter spp. | 0.62 | 0.13–2.57 | 0.45 |
| Discordant treatment with penicillin/beta-lactamase inhibitor combinations | 1.94 | 0.94–4.03 | 0.05 |
| Discordant treatment with 3rd-generation cephalosporins | 0.80 | 0.32–2.00 | 0.61 |
| Discordant treatment with penicillins + aminoglycoside | 0.56 | 0.23–1.34 | 0.15 |
| Intravenous route of administration | 0.59 | 0.26–1.34 | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Autore, G.; Neglia, C.; Di Costanzo, M.; Ceccoli, M.; Vergine, G.; La Scola, C.; Malaventura, C.; Falcioni, A.; Iacono, A.; Crisafi, A.; et al. Clinical Outcome of Discordant Empirical Therapy and Risk Factors Associated to Treatment Failure in Children Hospitalized for Urinary Tract Infections. Children 2022, 9, 128. https://doi.org/10.3390/children9020128
Autore G, Neglia C, Di Costanzo M, Ceccoli M, Vergine G, La Scola C, Malaventura C, Falcioni A, Iacono A, Crisafi A, et al. Clinical Outcome of Discordant Empirical Therapy and Risk Factors Associated to Treatment Failure in Children Hospitalized for Urinary Tract Infections. Children. 2022; 9(2):128. https://doi.org/10.3390/children9020128
Chicago/Turabian StyleAutore, Giovanni, Cosimo Neglia, Margherita Di Costanzo, Martina Ceccoli, Gianluca Vergine, Claudio La Scola, Cristina Malaventura, Alice Falcioni, Alessandra Iacono, Antonella Crisafi, and et al. 2022. "Clinical Outcome of Discordant Empirical Therapy and Risk Factors Associated to Treatment Failure in Children Hospitalized for Urinary Tract Infections" Children 9, no. 2: 128. https://doi.org/10.3390/children9020128