
Importance of Early Intervention in Reducing Autistic Symptoms and Speech–Language Deficits in Children with Autism Spectrum Disorder

Abstract
:1. Introduction
Present Study
2. Methodology
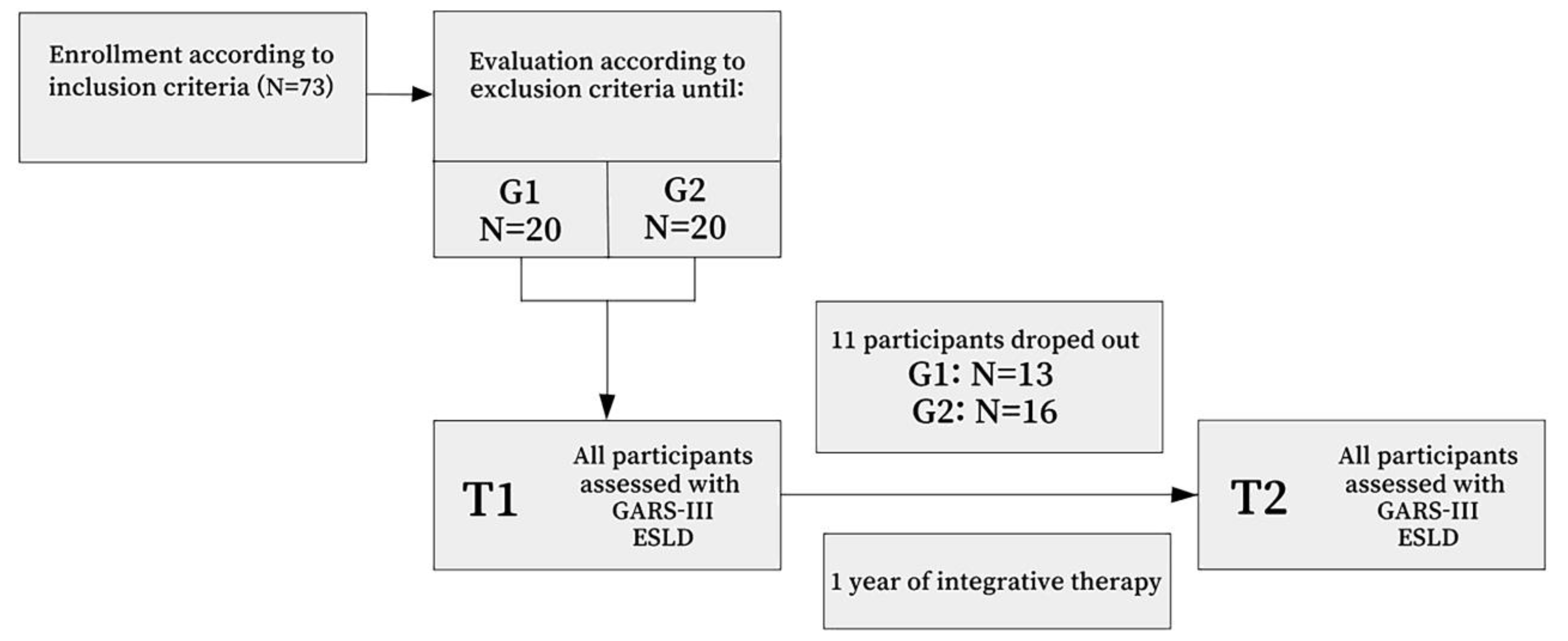
2.1. Study Design
2.2. Sample
2.3. Instruments
3. Intervention
3.1. Procedure
3.2. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Time Point of Testing | Younger Group Mean ± SD | Older Group Mean ± SD | Difference between Groups on T1 and T2 | Effect of Group on Autism Index between T1 and T2 | |
|---|---|---|---|---|---|
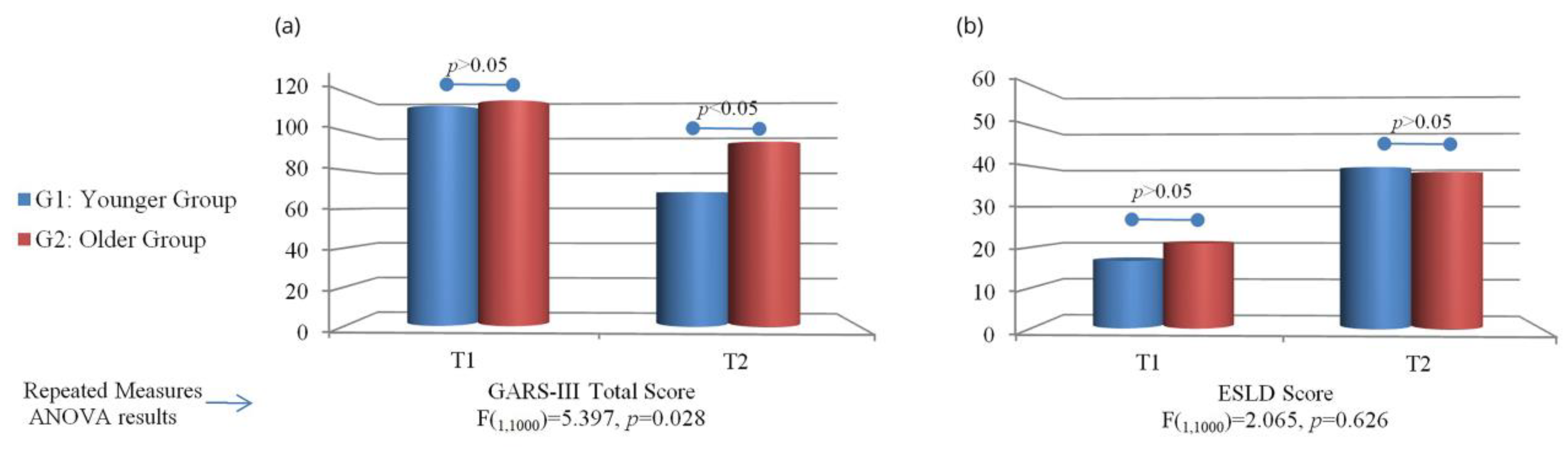
| Total Qustionnaire | T1 | 113 ± 9.15 | 115.62 ± 9.15 | p > 0.05 | F(1,1000) = 15.575, p = 0.001 |
| T2 | 68.61 ± 16.99 | 94.25 ± 18.41 | p < 0.05 | ||
| t = 9.795; p < 0.000 | t = 5.696; p < 0.000 | ||||
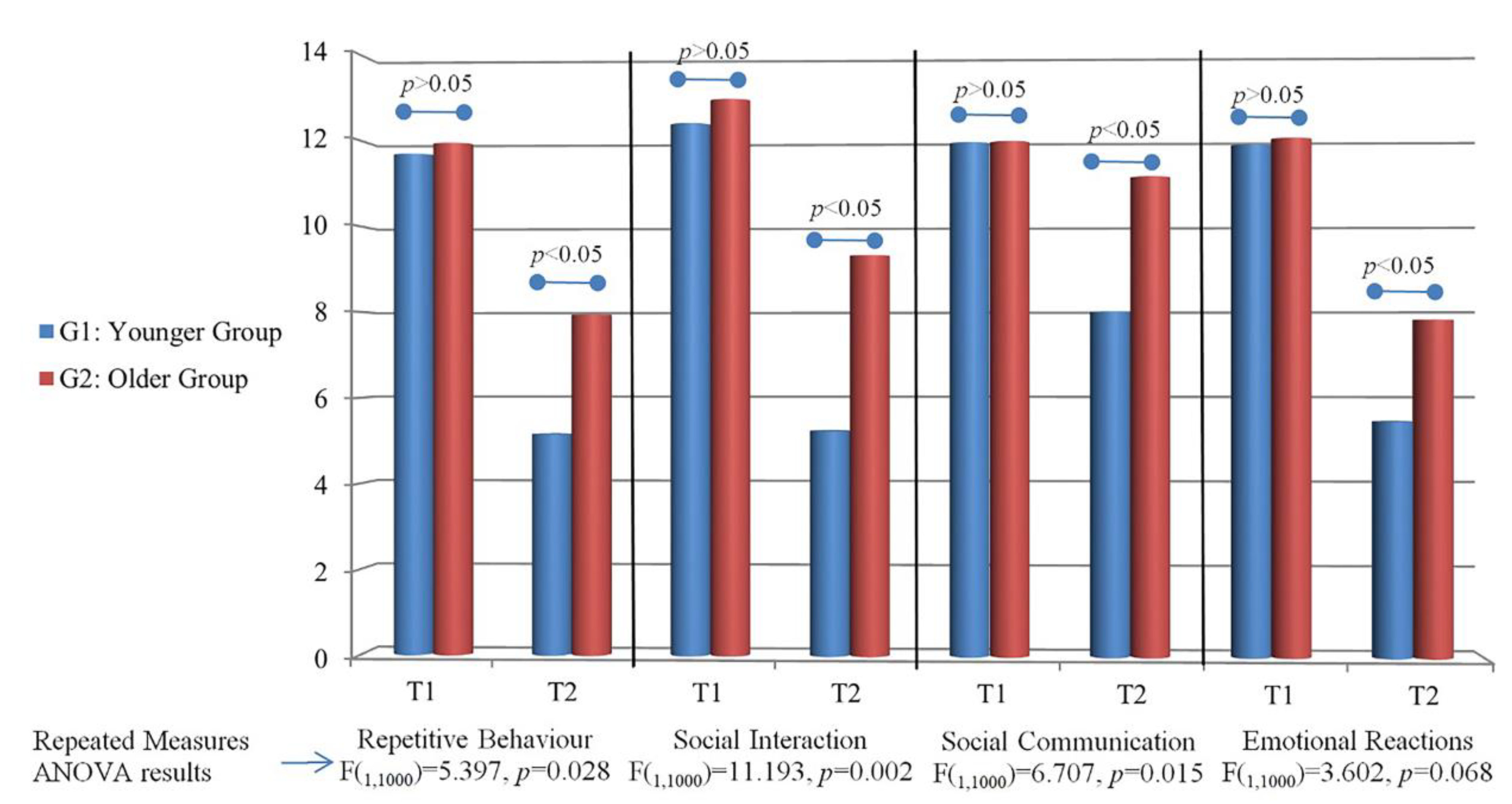
| Repetetive Behaviour | T1 | 11.69 ± 2.93 | 11.94 ± 2.29 | p > 0.05 | F(1,1000) = 5.397, p = 0.028 |
| T2 | 5.15 ± 2.27 | 7.94 ± 2.74 | p < 0.05 | ||
| t = 6.921; p < 0.000 | t = 6.461; p < 0.000 | ||||
| Social Interaction | T1 | 12.38 ± 2.63 | 12.94 ± 1.48 | p > 0.05 | F(1,1000) = 11.193, p = 0.002 |
| T2 | 5.23 ± 2.77 | 9.31 ± 2.84 | p < 0.05 | ||
| t = 7.506; p < 0.000 | t = 6.539; p < 0.000 | ||||
| Social Communication | T1 | 11.92 ± 0.28 | 11.94 ± 0.25 | p > 0.05 | F(1,1000) = 6.707, p = 0.015 |
| T2 | 8.00 ± 4.28 | 11.12 ± 1.96 | p < 0.05 | ||
| t = 3.282; p < 0.007 | t = 1.676; p < 0.115 | ||||
| Emotional Reactions | T1 | 11.85 ± 2.82 | 12.00 ± 2.48 | p > 0.05 | F(1,1000) = 3.602, p = 0.068 |
| T2 | 5.46 ± 2.40 | 7.81 ± 3.37 | p < 0.05 | ||
| t = 7.635; p < 0.000 | t = 5.289; p < 0.000 | ||||
Appendix B
| Time Point of Testing | Younger Group Mean ± SD | Older Group Mean ± SD | Difference between Groups on T1 and T2 | Effect of Group on between T1 and T2 | |
|---|---|---|---|---|---|
| ESLD | T1 | 16.61 ± 6.83 | 20.94 ± 8.85 | p > 0.05 | F(1,1000) = 2.065, p = 0.626 |
| T2 | 39.69 ± 9.51 | 38.52 ± 13.57 | p > 0.05 | ||
| p < 0.000 | p < 0.000 | ||||
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Vol. 10; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Stepanova, E.; Dowling, S.; Phelps, M.; Findling, R.L. Pharmacotherapy of emotional and behavioral symptoms associated with autism spectrum disorder in children and adolescents. Dialogues Clin. Neurosci. 2017, 19, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Robain, F.; Franchini, M.; Kojovic, N.; Wood de Wilde, H.; Schaer, M. Predictors of treatment outcome in preschoolers with autism spectrum disorder: An observational study in the greater Geneva area, Switzerland. J. Autism Dev. Disord. 2020, 50, 3815–3830. [Google Scholar] [CrossRef] [PubMed]
- Russell, G.; Stapley, S.; Newlove-Delgado, T.; Salmon, A.; White, R.; Warren, F.; Pearson, A.; Ford, T. Time trends in autism diagnosis over 20 years: A UK population-based cohort study. J. Child Psychol. Psychiatry 2022, 63, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Newschaffer, C.J.; Croen, L.A.; Daniels, J.; Giarelli, E.; Grether, J.K.; Levy, S.E.; Mandell, D.S.; Miller, L.A.; Pinto-Martin, J.; Reaven, J.; et al. The epidemiology of autism spectrum disorders. Annu. Rev. Public Health 2007, 28, 235. [Google Scholar] [CrossRef] [Green Version]
- Bajo, J.; Wiggins, L.; Christensen, D.; Meanner, M.; Daniels, J.; Warren, Z.; Kurzius-Spencer, M.; Zahorodny, W.; Robinson Rosenberg, C.; White, T.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years-Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1, Erratum in MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 503. [Google Scholar]
- Fombonne, E. Editorial: The rising prevalence of autism. J. Child Psychol. Psychiatry Allied Discip. 2018, 59, 717–720. [Google Scholar] [CrossRef] [Green Version]
- Sacrey, L.-A.R.; Bennett, J.A.; Zwaigenbaum, L. Early infant development and intervention for autism spectrum disorder. J. Child Neurol. 2015, 30, 1921–1929. [Google Scholar] [CrossRef]
- Stefanatos, G.A. Regression in autistic spectrum disorders. Neuropsychol. Rev. 2008, 18, 305–319. [Google Scholar] [CrossRef]
- Libertus, K.; Sheperd, K.A.; Ross, S.W.; Landa, R.J. Limited fine motor and grasping skills in 6-month-old infants at high risk for autism. Child Dev. 2014, 85, 2218–2231. [Google Scholar] [CrossRef] [Green Version]
- Zwaigenbaum, L.; Bryson, S.; Garon, N. Early identification of autism spectrum disorders. Behav. Brain Res. 2013, 251, 133–146. [Google Scholar] [CrossRef]
- Tsai, C.H.; Chen, K.L.; Li, H.J.; Chen, K.H.; Hsu, C.W.; Lu, C.H.; Hsieh, K.Y.; Huang, C.Y. The symptoms of autism including social communication deficits and repetitive and restricted behaviors are associated with different emotional and behavioral problems. Sci. Rep. 2020, 10, 20509. [Google Scholar] [CrossRef]
- Uljarevic, M.; Hamilton, A. Recognition of emotions in autism: A formal meta-analysis. J. Autism Dev. Disord. 2013, 43, 1517–1526. [Google Scholar] [CrossRef]
- Sigman, M.; Dijamco, A.; Gratier, M.; Rozga, A. Early detection of core deficits in autism. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S. Mindblindness: An Essay on Autism and Theory of Mind; MIT Press: Cambridge, MA, USA, 1997. [Google Scholar]
- Chawarska, K.; Paul, R.; Klin, A.; Hannigen, S.; Dichtel, L.E.; Volkmar, F. Parental recognition of developmental problems in toddlers with autism spectrum disorders. J. Autism Dev. Disord. 2007, 37, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Harrop, C.; McConachie, H.; Emsley, R.; Leadbitter, K.; Green, J. Restricted and repetitive behaviors in autism spectrum disorders and typical development: Cross-sectional and longitudinal comparisons. J. Autism Dev. Disord. 2014, 44, 1207–1219. [Google Scholar] [CrossRef] [PubMed]
- Honey, E.; Leekam, S.; Turner, M.; McConachie, H. Repetitive behaviour and play in typically developing children and children with autism spectrum disorders. J. Autism Dev. Disord. 2007, 37, 1107–1115. [Google Scholar] [CrossRef]
- Buzhardt, J.; Wallisch, A.; Irvin, D.; Boyd, B.; Salley, B.; Jia, F. Exploring Growth in Expressive Communication of Infants and Toddlers With Autism Spectrum Disorder. J. Early Interv. 2022, 44, 3–22. [Google Scholar] [CrossRef]
- Tager-Flusberg, H. Strategies for conducting research on language in autism. J. Autism Dev. Disord. 2004, 34, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Tager-Flusberg, H.; Paul, R.; Lord, C. Language and Communication in Autism. In Handbook of Autism and Pervasive Developmental Disorders: Diagnosis, Development, Neurobiology, and Behavior; Volkmar, F.R., Paul, R., Klin, A., Cohen, D., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2005; pp. 335–364. [Google Scholar]
- Volden, J.; Sorenson, A. Bossy and nice requests: Varying language register in speakers with autism spectrum disorder (ASD). J. Commun. Disord. 2009, 42, 58–73. [Google Scholar] [CrossRef]
- Bruner, J.S. From communication to language—A psychological perspective. Cognition 1974, 3, 255–287. [Google Scholar] [CrossRef]
- Hurtado, N.; Marchman, V.A.; Fernald, A. Does input influence uptake? Links between maternal talk, processing speed and vocabulary size in Spanish-learning children. Dev. Sci. 2008, 11, F31–F39. [Google Scholar] [CrossRef] [PubMed]
- Puerto, E.; Aguilar, J.; Lopez, C.; Chavez, D. Using multilayer fuzzy cognitive maps to diagnose autism spectrum disorder. Appl. Soft Comput. 2019, 75, 58–71. [Google Scholar] [CrossRef]
- Maw, S.S.; Haga, C. Effectiveness of cognitive, developmental, and behavioural interventions for Autism Spectrum Disorder in preschool-aged children: A systematic review and meta-analysis. Heliyon 2018, 4, e00763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolb, B.; Gibb, R. Brain plasticity and behaviour in the developing brain. J. Can. Acad. Child Adolesc. Psychiatry 2011, 20, 265. [Google Scholar]
- McWilliam, R. Routines-Based Early Intervention. In Supporting Young Children and Their Families; Brookes: Baltimore, MD, USA, 2010. [Google Scholar]
- Zhou, B.; Xu, Q.; Li, H.; Zhang, Y.; Wang, Y.; Rogers, S.J.; Xu, X. Effects of parent-implemented Early Start Denver Model intervention on Chinese Toddlers with autism spectrum disorder: A non-randomized controlled trial. Autism Res. 2018, 11, 654–666. [Google Scholar] [CrossRef]
- Peters-Scheffer, N.; Didden, R.; Korzilius, H.; Sturmey, P. A meta-analytic study on the effectiveness of comprehensive ABA-based early intervention programs for children with autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 60–69. [Google Scholar] [CrossRef]
- Rogers, S.J.; Vismara, L.; Wagner, A.L.; McCormick, C.; Young, G.; Ozonoff, S. Autism treatment in the first year of life: A pilot study of infant start, a parent-implemented intervention for symptomatic infants. J. Autism Dev. Disord. 2014, 44, 2981–2995. [Google Scholar] [CrossRef] [Green Version]
- Vivanti, G.; Paynter, J.; Duncan, E.; Fothergill, H.; Dissanayake, C.; Rogers, S.J. Effectiveness and feasibility of the Early Start Denver Model implemented in a group-based community childcare setting. J. Autism Dev. Disord. 2014, 44, 3140–3153. [Google Scholar] [CrossRef]
- Granpeesheh, D.; Dixon, D.R.; Tarbox, J.; Kaplan, A.M.; Wilke, A.E. The effects of age and treatment intensity on behavioral intervention outcomes for children with autism spectrum disorders. Res. Autism Spectr. Disord. 2009, 3, 1014–1022. [Google Scholar] [CrossRef]
- Shi, B.; Wu, W.; Dai, M.; Zeng, J.; Luo, J.; Cai, L.; Wan, B.; Jing, J. Cognitive, language, and behavioral outcomes in children with autism spectrum disorders exposed to early comprehensive treatment models: A meta-analysis and meta-regression. Front. Psychiatry 2021, 12, 691148. [Google Scholar] [CrossRef]
- Čuturić, N. Lestvica Psihičkog Razvoja Rane Dečje Dobi Brunet-Lezine; Zavod SR Slovenije za produktivnost dela: Ljubljana, Slovenia, 1973. [Google Scholar]
- Gilliam, J. Gilliam Autism Rating Scale, 3rd ed.; Pro-Ed: Austin, TX, USA, 2014. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Adamović, T.; Kosanović, R.; Madić, D.; Ribarić-Jankes, K.; Sovilj, M.; Đoković, S. Correlation between Balance Ability and Speech-Language Development in Children. Coll Antropol. 2015, 39 (Suppl. 1), 11–20. [Google Scholar]
- Rakonjac, M.; Cuturilo, G.; Stevanovic, M.; Jelicic, L.; Subotic, M.; Jovanovic, I.; Drakulic, D. Differences in speech and language abilities between children with 22q11.2 deletion syndrome and children with phenotypic features of 22q11.2 deletion syndrome but without microdeletion. Res. Dev. Disabil. 2016, 55, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Vujović, M.; Sovilj, M.; Plešinac, S.; Rakonjac, M.; Jeličić, L.; Adamović, T.; Stokić, M. Effect of antenatal maternal anxiety on the reactivity of fetal cerebral circulation to auditory stimulation, and early child development. Srp. Arh. Celok. Lek. 2019, 147, 327–334. [Google Scholar] [CrossRef]
- Adamović, T.; Jurišić-Škevin, A.; Madić, D.; Sovilj, M.; Jeličić, L.; Maksimović, S.; Subotić, M. Head righting reflex in newborns as the predictive factor of early child development: A longitudinal study. Early Child Dev. Care 2020, 192, 748–760. [Google Scholar] [CrossRef]
- Maksimović, S.; Stanojević, N.; Fatić, S.; Punišić, S.; Adamović, T.; Petrović, N.; Nenadović, V. Multidisciplinary speech and language therapy approach in a child with multiple disabilities including blindness due to retinopathy of prematurity: A case study with a one year follow-up. Logop. Phoniatr. Vocology 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bogavac, I.; Jeličić, L.; Nenadović, V.; Subotić, M.; Janjić, V. The speech and language profile of a child with turner syndrome–a case study. Clin. Linguist. Phon. 2022, 36, 565–578. [Google Scholar] [CrossRef]
- Maksimović, S.; Jeličić, L.; Marisavljević, M.; Fatić, S.; Gavrilović, A.; Subotić, M. Can EEG Correlates Predict Treatment Efficacy in Children with Overlapping ASD and SLI Symptoms: A Case Report. Diagnostics 2022, 12, 1110. [Google Scholar] [CrossRef]
- Jeličić, L.; Sovilj, M.; Bogavac, I.; Drobnjak, A.; Gouni, O.; Kazmierczak, M.; Subotić, M. The impact of maternal anxiety on early child development during the COVID-19 pandemic. Front. Psychol. 2021, 12, 792053. [Google Scholar] [CrossRef]
- Walton, J.K.; Das, R.S. An Empirical Study of Hearing Impairment, Intelligence, and Habilitation of Speech Utilizing the Kostić Methodology; Department of Psychology, University of Wisconsin-Superior: Superior, WI, USA, 1973. [Google Scholar]
- Das, R.S.; Kain, F.M.; Walton, J.K. The Effects of the Kostić Methodology on Speech Sound Quality and Laryngeal Voice of Hearing Impaired Children; Department of Psychology, University of Wisconsin-Superior: Superior, WI, USA, 1973. [Google Scholar]
- Kostić, D. Speech and the Hearing Impaired Child; Indian Statistical Institute: Kolkata, India, 1980. [Google Scholar]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics 2010, 125, e17–e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haglund, N.; Dahlgren, S.O.; Gustafsson, P.; Råstam, M.; Källén, K. Early screening for autism in child health services. Austin J. Autism Relat. Disabil. 2017, 3. Available online: https://austinpublishinggroup.com/autism/fulltext/autism-v3-id1038.php (accessed on 22 September 2022).
- Kupferstein, H. Evidence of increased PTSD symptoms in autistics exposed to applied behavior analysis. Adv. Autism 2018, 4, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Penhune, V.B. Sensitive periods in human development: Evidence from musical training. Cortex 2011, 47, 1126–1137. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, P.; Rivera-Gaxiola, M. Neural substrates of language acquisition. Annu. Rev. Neurosci. 2008, 31, 511–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, J.J.; Botteron, K.N.; Dager, S.R.; Elison, J.T.; Estes, A.M.; Gu, H.; Hazlett, H.C.; Pandey, J.; Paterson, S.J.; Schultz, R.T.; et al. Longitudinal patterns of repetitive behavior in toddlers with autism. J. Child Psychol. Psychiatry 2014, 55, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Leekam, S.R.; Prior, M.R.; Uljarevic, M. Restricted and repetitive behaviors in autism spectrum disorders: A review of research in the last decade. Psychol. Bull. 2011, 137, 562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.M.; Yoder, K.J.; Ganzel, B.L.; Goodwin, M.S.; Belmonte, M.K. Harnessing repetitive behaviours to engage attention and learning in a novel therapy for autism: An exploratory analysis. Front. Psychol. 2012, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Mooney, E.L.; Gray, K.M.; Tonge, B.J.; Sweeney, D.J.; Taffe, J.R. Factor analytic study of repetitive behaviours in young children with pervasive developmental disorders. J. Autism Dev. Disord. 2009, 39, 765–774. [Google Scholar] [CrossRef]
- McKinnon, C.J.; Eggebrecht, A.T.; Todorov, A.; Wolff, J.J.; Elison, J.T.; Adams, C.M.; Snyder, A.Z.; Estes, A.M.; Zwaigenbaum, L.; Botteron, K.N.; et al. Restricted and repetitive behavior and brain functional connectivity in infants at risk for developing autism spectrum disorder. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 50–61. [Google Scholar] [CrossRef]
- Wolff, J.J.; Swanson, M.R.; Elison, J.T.; Gerig, G.; Pruett, J.R., Jr.; Styner, M.A.; Vachet, C.; Botteron, K.N.; Dager, S.R.; Estes, A.M.; et al. Neural circuitry at age 6 months associated with later repetitive behavior and sensory responsiveness in autism. Mol. Autism 2017, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Mundy, P.; Delgado, C.; Block, J.; Venezia, M.; Hogan, A.; Seibert, J. A Manual for the Early Social Communication Scales (ESCS); MIND Institute, University of California at Davis: Davis, CA, USA, 2003. [Google Scholar]
- Tomasello, M.; Farrar, M.J. Joint attention and early language. Child Dev. 1986, 57, 1454–1463. [Google Scholar] [CrossRef]
- Charman, T. Why is joint attention a pivotal skill in autism? Philos. Trans. R. Soc. London. Ser. B Biol. Sci. 2003, 358, 315–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landa, R.J. Efficacy of early interventions for infants and young children with, and at risk for, autism spectrum disorders. Int. Rev. Psychiatry 2018, 30, 25–39. [Google Scholar] [CrossRef]
- Mundy, P.; Bullen, J. The bidirectional social-cognitive mechanisms of the social-attention symptoms of autism. Front. Psychiatry 2021, 12, 2570. [Google Scholar] [CrossRef]
- Fuller, E.A.; Kaiser, A.P. The effects of early intervention on social communication outcomes for children with autism spectrum disorder: A meta-analysis. J. Autism Dev. Disord. 2020, 50, 1683–1700. [Google Scholar] [CrossRef] [PubMed]
- Kasari, C.; Paparella, T.; Freeman, S.; Jahromi, L.B. Language outcome in autism: Randomized comparison of joint attention and play interventions. J. Consult. Clin. Psychol. 2008, 76, 125. [Google Scholar] [CrossRef]
- Murray, D.S.; Creaghead, N.A.; Manning-Courtney, P.; Shear, P.K.; Bean, J.; Prendeville, J.A. The relationship between joint attention and language in children with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2008, 23, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Pontoppidan, M.; Niss, N.K.; Pejtersen, J.H.; Julian, M.M.; Væver, M.S. Parent report measures of infant and toddler social-emotional development: A systematic review. Fam. Pract. 2017, 34, 127–137. [Google Scholar] [CrossRef] [Green Version]
- Bryson, S.E.; Zwaigenbaum, L.; Brian, J.; Roberts, W.; Szatmari, P.; Rombough, V.; McDermott, C. A prospective case series of high-risk infants who developed autism. J. Autism Dev. Disord. 2007, 37, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.R.; Baranek, G.T.; Crais, E.R.; Steven Reznick, J.; Dykstra, J.; Perryman, T. The first year inventory: Retrospective parent responses to a questionnaire designed to identify one-year-olds at risk for autism. J. Autism Dev. Disord. 2007, 37, 49–61. [Google Scholar] [CrossRef]
- Otsuka, S.; Uono, S.; Yoshimura, S.; Zhao, S.; Toichi, M. Emotion perception mediates the predictive relationship between verbal ability and functional outcome in high-functioning adults with autism spectrum disorder. J. Autism Dev. Disord. 2017, 47, 1166–1182. [Google Scholar] [CrossRef] [Green Version]
- Sappok, T.; Heinrich, M.; Böhm, J. The impact of emotional development in people with autism spectrum disorder and intellectual developmental disability. J. Intellect. Disabil. Res. 2020, 64, 946–955. [Google Scholar] [CrossRef] [PubMed]
- Garrido, D.; Watson, L.R.; Carballo, G.; Garcia-Retamero, R.; Crais, E.R. Infants at-risk for autism spectrum disorder: Patterns of vocalizations at 14 months. Autism Res. 2017, 10, 1372–1383. [Google Scholar] [CrossRef] [PubMed]
- Mayo, J.; Chlebowski, C.; Fein, D.A.; Eigsti, I.M. Age of first words predicts cognitive ability and adaptive skills in children with ASD. J. Autism Dev. Disord. 2013, 43, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Kover, S.T.; Edmunds, S.R.; Weismer, S.E. Brief report: Ages of language milestones as predictors of developmental trajectories in young children with autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 2501–2507. [Google Scholar] [CrossRef] [PubMed]
- Hampton, L.H.; Kaiser, A.P. Intervention effects on spoken-language outcomes for children with autism: A systematic review and meta-analysis. J. Intellect. Disabil. Res. 2016, 60, 444–463. [Google Scholar] [CrossRef]
- Lane, J.D.; Lieberman-Betz, R.; Gast, D.L. An analysis of naturalistic interventions for increasing spontaneous expressive language in children with autism spectrum disorder. J. Spec. Educ. 2016, 50, 49–61. [Google Scholar] [CrossRef]



| No. | Gender | Age Mean ± SD | IQ Mean ± SD | |
|---|---|---|---|---|
| G1 | 13 | M = 9; F = 4 | 41.08 ± 3.57 | 73.10 ± 9.51 |
| G2 | 16 | M = 11; F = 5 | 54.37 ± 3.37 | 70.50 ± 16.01 |
| p = 0.652 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maksimović, S.; Marisavljević, M.; Stanojević, N.; Ćirović, M.; Punišić, S.; Adamović, T.; Đorđević, J.; Krgović, I.; Subotić, M. Importance of Early Intervention in Reducing Autistic Symptoms and Speech–Language Deficits in Children with Autism Spectrum Disorder. Children 2023, 10, 122. https://doi.org/10.3390/children10010122
Maksimović S, Marisavljević M, Stanojević N, Ćirović M, Punišić S, Adamović T, Đorđević J, Krgović I, Subotić M. Importance of Early Intervention in Reducing Autistic Symptoms and Speech–Language Deficits in Children with Autism Spectrum Disorder. Children. 2023; 10(1):122. https://doi.org/10.3390/children10010122
Chicago/Turabian StyleMaksimović, Slavica, Maša Marisavljević, Nina Stanojević, Milica Ćirović, Silvana Punišić, Tatjana Adamović, Jelena Đorđević, Ivan Krgović, and Miško Subotić. 2023. "Importance of Early Intervention in Reducing Autistic Symptoms and Speech–Language Deficits in Children with Autism Spectrum Disorder" Children 10, no. 1: 122. https://doi.org/10.3390/children10010122