Pharmacological Activities of Phytomedicines: A Challenge Horizon for Rational Knowledge


1
Department of Biomedical Sciences, Pharmacy Faculty, University of Alcalá, 28805 Alcalá de Henares, Madrid, Spain
2
Pharmacy Faculty, University of Alcalá, 28805 Alcalá de Henares, Madrid, Spain
*
Author to whom correspondence should be addressed.
Challenges 2018, 9(1), 15; https://doi.org/10.3390/challe9010015
Submission received: 5 February 2018
/
Revised: 10 March 2018
/
Accepted: 10 March 2018
/
Published: 23 March 2018
Abstract
:Herbal drugs have been widely used throughout the course of history. Traditional knowledge based on religious beliefs and/or experience has been transmitted orally between generations. First attempts to provide scientific evidence came in the 19th century when potent compounds were first isolated. Since then, modern pharmacology theory has been assumed by phytotherapy. Scientists have tried to elucidate the molecular mechanism of each compound and, for a pharmacological indication, propose an effective and secure dose. Stepwise, clinical trials confirm the benefits of herbal drug use in therapeutics, especially for chronic diseases. However, herbal drugs exert pleiotropic effects, and there is still a need for a complete, rational, and widely accepted theory that can explain phytotherapy efficacy. The “-omics” might help with this matter. Studies of modification in the gene expression profile, the metabolome, and the physiopathological state after the administration of a herbal extract could provide relevant information that verifies herbal therapies.
{kind=link}
{kind=link}
1. Introduction
Herbal medicine has always been an important source of medicine (Figure 1). It has been successfully applied in clinics for thousands of years all around the world. Archeological studies have documented that man has possibly used plants as drugs for at least 60,000 years [1,2]. Knowledge concerning the medicinal use of plants has been transmitted orally from generation to generation by tribal societies [3,4,5]. The medical use of plants has strongly evolved over time. At first, regardless of the underlying philosophical premises, it entailed trial and error [6]. However, the selection of medicinal plants progressed into a more rational and conscious process, and in the 16th century Ben Co. Gang Mu emerged as the first treatise on herbal drugs, where essential elements of the scientific method can be observed [7]. Similar experiences became manifest in the so-called medicinal systems or folk medicine, such as traditional European medicine, traditional Chinese medicine, Indian Ayurveda, Japanese Kampo, or traditional Arabic and Islamic medicine [6]. The mutual influence between traditional medicinal systems and a chronology of influential herbals and authors of traditional medicine focused on the Mediterranean and Europe was studied by Leonti et al. [8]. In the 17th century, scientists observed the clinical usefulness of herbal products containing potent agents that elicit a strong response in low doses. Two hundred years later, an emphasis was placed on learning about the principal compound responsible for herbs’ therapeutic effects. In this process, the plant extracts were first separated into many fractions. Then, bioassays were performed for each fraction to select the most active samples for further separation. Following the separation and bioassay loop, some active substances were purified through chemical methods [9]. Examples of the first pure chemical entities isolated from herbs for medicinal use include morphine, an analgesic compound from opium poppy (Papaver somniferum, Papaveraceae), quinine, used for leg cramps at night, from cinchona bark (Cinchona succirubra, Rubiaceae), and salicin, an antipyretic from willow bark (Salix spp., Salicaceae) [10]. They were assumed by modern medicine in the form of single active chemical ingredients and verified in their medical system and pharmacological workflow pattern in terms of their efficacy, security, and stability, among others. In contrast to single compound drugs, herbal preparations represent highly complex multicomponent mixtures. However, to date, there is still no rational basis for the use of a large number of herbal remedies, some of which are in the market or are far from being sufficient or scientifically valid [6]. Some of the reasons could be the complicated and varying chemical composition or the lack of concrete evidence about their biological activity and contribution to the therapeutic effect [11]. On a global perspective, we are yet in need of a rational, complete, and widely accepted theory to explain phytotherapy efficacy and the mechanisms of action in herbal drugs. For this purpose, a new approach based on the “-omics” could prove extremely useful.
2. The “Modern Medicine Approach” Was Not Enough
A great number of herbs have been analyzed under the approach described previously, and a compound or group of compounds have been proposed as the biologically active agents that play the key role in the pharmacological effect [12]. Sometimes, this approach has resulted in the ability to discover compounds with great selectivity for a chosen target [13], which can be as diverse as enzymes, receptors, antibodies, or signal cascades, but generally, herbal extracts are a mixture of bioactive or inactive compounds, and it has been suggested that the biological activity of herbal medicine results from the combination of different active components [14]. Systems biology has revealed that human cells and tissues are composed of complex, networked systems with redundant, convergent, and divergent signaling pathways, with different possibilities of interaction when such a great number of compounds converge [13]. The combination of effects is described with the terms additivity, synergy, and antagonism, although both synergy and antagonism can be defined in relation to an additive expectation [5].
Strictly speaking, synergism, which was advanced in a landmark paper by Williamson [15] and further outlined by Ulrich-Merzenich et al. [16], is defined by a combined effect of substances that is greater than would be expected from the individual contributions [17]. Sarris et al. [18] defined it as a “super-additive” biological effect when combined, as opposed to being just the sum of their individual parts or additivity (e.g., 1 + 1 = 5, not 2). Antagonism, or “negative synergy”, on the contrary, appears if it works backwards and a reduced effect is achieved. To better understand synergy, the example of actein, a triterpene glycoside isolated from the roots and rhizomes of Cimicifuga racemosa (black cohosh), and digitoxin, a cardiac glycoside present in the plant Digitalis purpurea, can be used. According to investigations carried out by Einbond et al. [19], the inhibitory effect on Na+-K+-ATPase activity, compared with the summation effect obtained by each one administered alone, is higher when co-administered. In this case, this observation is an example of pharmacodynamic synergy because actein or digitoxin facilitates the action of the other in the same target. Synergy can also be related to pharmacokinetic parameters. For example, permeability values and the absorption rate of some drugs can be altered. Coumarins can increase the active absorption via carrier-mediated proteins (i.e., of flavonoids) and inhibit P-gp-mediated efflux systems [20]. That is exactly what happens in a plant extract. The ingredients with little or no direct activity on the pathogenic process may assist the “actives” to reach the target, either by improving bioavailability or decreasing the metabolism and excretion of the active principle [21], and in the overall pharmacological effects and the therapeutic efficacy of multi-extract preparations, constituents are involved synergistically [22]. In the same sense, the complex matrix in a plant can also exhort protection of the active principles, through antioxidative and other protection actions [23]. The expected overall effect is not easy to predict based on the known effects of the different substances in an individual herbal preparation assuming that each component acts on different pharmacological targets. In the case previously described (actein/digitoxin), not only does Na+-K+-ATPase activity increase, but the expression of NF-κB promoters, p-ERK, p-Akt, and cyclin D1 protein levels are also affected.
The treatment of diseases with mono-substance therapy, “the silver bullet concept”, in other words, with a characterized compound and a perfectly defined mechanism of action at a particular dose that fulfills the positive (efficacy/stability) and negative requirements (such as toxicity) has been inherited from classical pharmacology and assumed by phytotherapy in an attempt to achieve rationality. However, especially in the treatment of chronic diseases, it is increasingly viewed as inadequate in many clinical situations due to ineffectiveness, resistance problems, and the side effects that may occur [24]. For these reasons, the herbal medicinal preparation derived from several herbal plants that contains a large number of secondary phytochemical compounds has been seen as feasible for chronic therapies. The rationale behind combinations is frequently questioned, and it remains challenging to assess the individual contribution of each of the combination partners to the overall activity of the preparation [25,26]. The new trends suggest an integrative approach, called “the shotgun approach”, in which a wide variety of compounds act together on multiple targets to produce a final action through a balance resulting from minor changes.
3. The “-Omic” Technologies; Present and Future
Epigenetic studies are already demonstrating that combinations of constituents do not only have the added effect of triggering an increase in the number of expressed genes; they do in fact trigger new genes altogether [18]. Furthermore, the effect could or could not be dose-dependent, and targeting a particular step in a signaling pathway can have qualitatively (directionally) different effects depending on the actual state of the system mediated. That is what happens, i.e., on the regulatory NF-κB clusters [27] or in the protein networks and regulatory feedback loops. The mechanism underlying phytotherapy efficacy is, clearly, much more sophisticated. A good example of this can be found in the work of Ulrich-Merzenich et al. [16], who showed a summary map of genes expressed in human chondrocytes stimulated with willow bark extract STW-33-1 (30 μg/mL and 50 μg/mL) as well as with quercetin (10 μM), diclofenac (30 μg/mL), and acetylsalicyclic acid (50 μg/mL). Undoubtedly, the results demonstrated that each of the substances and extracts, in spite of the fact that all exert anti-inflammatory activity, has a specific gene expression profile, as well as that the willow bark extract showed a different gene expression profile depending on the dose administered. To study this further, a similar map of genes expressed in the blood cells of rats after the animals were treated with willow bark extract STW-33-1 and its different fractions (ethanol, ethyl acetate, and water) was constructed. In this case, as might be expected, the treatment with different fractions of the extract leads to distinct gene expression profiles in vivo as a direct consequence of the different combinations of compounds and their concentration in each fraction. To sum up, it must be concluded that not only is the pattern of gene expression (signature in some texts) different depending on whether a substance or a mixture of substances (extract) is administered, presumably more complex in the last case, but also depending on the substance/extract concentration or the extract fraction administered.
The development and refinement of “-omic” technologies, including genomics/transcriptomics, proteomics, and metabolomics, has led to advances in the assessment of both the efficacy and, no less important, safety of herbal medicines [29,30] referred to by some authors as “herbomics”, although this term is still in its infancy. An interesting study is the one published by Wang et al. [31], in which the possible toxicological role of Matricaria chamomilla was evaluated using metabolomics approaches. After tea administration in human volunteers (200 mL/day for 2 weeks, made from fresh flowers), urine was analyzed during the dosing period and two weeks later. Its administration results in an increase in the excretion of some metabolites (including glycine and hippurate), while creatinine excretion decreased, with baseline parameters still altered 14 days later. Apart from the therapeutic effect, it is clear that Matricaria chamomilla tea modified patients’ homeostasis. On that basis, the authors suggest that gut microflora might have been disrupted. Security assessment must include the kinds of techniques able to fulfill differences between the toxicology of a specific compound and that of whole herbs or an extract. Despite the high level of complexity and cost of “-omic” techniques, they are the only way the pharmacological action of many species can be fully understood. They are the key to a rational and fully accepted form of phytotherapy.
4. Conclusions
All of this methodology needs to start from standardization. If a mixture of compounds is tested, quantification of at least one or a few identified biologically active substances is needed, a fingerprint. This may not be enough sometimes, if assured according to conventional methods. Thus, it is the only method whereby it is possible to get reproducible results and compare the expression profiles of complex mixtures between them or with other substances (monotherapy). In such a case, first, which pharmacological and therapeutic contributions each distinct active component of an extract preparation provides and, secondly, which chemical substances or substance groups from the extracts are responsible for which specific pharmacological effects [22] must be elucidated. Additionally, an evaluation of the “surrogate” plant components that represent the activity of the plant extract should follow standardization [32,33]. Based on the findings, companies should initiate harmonization processes to fulfill the requirements and achieve the expected pharmaceutical quality of herbal remedies [34]. With this valuable framework, it would be easier for the legislator to establish a regulation that could overcome the complex and sometimes not-always-clear overall situation, at least in Europe [35].
It must be noted that, once this first point is clear, the bioavailability will continue to be a capital need to determine whether the defined compound(s) or group of compounds can be absorbed at a rate sufficient to achieve a therapeutic concentration and to maintain it for the minimum time necessary. Once all that work has been completed, and based on the phytopharmaceutical and disease profiles, relevant relationships that can be suitable for clinical application may be identified [36]. Solid principles and promising preclinical results are a helpful starting point for clinical studies to determine the efficacy of a new plant medication [28]. Among them, the integrated metabolomics strategy can be used in pharmacokinetic study of herbal medicines to demonstrate their biological fates, thereby linking the plant metabolome to human metabolome is essential [37].
The benefits of the application of this new approach for phytotherapy investigation and its translation to clinical practice “rationalize the therapeutic superiority of many plant extracts over single isolated constituents” [16]. If phytopreparations are fully understood, the prescription could be selected to meet the patient’s needs, at least in stratified medicine targeted at subgroups of patients [31]. Finding the appropriate drug for each ailment and in the precise dose at each disease state and physiological condition would be a dream come true. That requires assessing the “personal safety” to reduce/keep secondary or adverse effects to a minimum as much as possible. All of this is to the benefit of patients but also in the interest of the administration, prompting cost reduction.
Finally, a better comprehension of phytotherapy efficacy could lead to convergent levels of therapeutically value evidence [38]. This fact enables the selection of better “candidate plant/indication” binomials and the concentration of efforts (critical mass of researchers, financial resources or patients) in clinical trials that are most likely a worthwhile cause. In the same sense, better knowledge of how herbal drugs are effective in the complicated interplay of biological processes and dysfunctional systems that causes a disease can provide guidance regarding what secondary and adverse effects can be expected [39], which makes it easier to focus on them and avoid that which remains unnoticed.
Despite all of this, there is no shortage of authors, such as Gertsch [40], who recall that this appealing concept of “natural product triggered network pharmacology” needs to be proven in many ways and that, alternatively, we should not ignore the possibility, sometimes true, that many medicinal plants could be simply mediators of a significant “meaning response” (placebo effect) in a cultural context and do not contain pharmacologically active molecules, at least not for a certain disease.
Acknowledgments
Javier Rodríguez Villanueva wants to thank Instituto Nacional de Investigación y Tecnología Agraria y Alimentaria (INIA) for the grant “Ayuda Social 2016” received for further studies in phytotherapy.
Author Contributions
All authors contributed equally. Javier Rodríguez Villanueva conceived and designed the work reported here.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lietava, J. Medicinal plants in a Middle Paleolithic grave Shanidar IV. J. Ethnoparmacol. 1992, 35, 263–266. [Google Scholar] [CrossRef]
- Sommer, J.D. The Shanidar IV “flower burial”: A re-evaluation of Neanderthal burial ritual. Camb. Archaeol. J. 1999, 9, 127–137. [Google Scholar] [CrossRef]
- Pan, S.Y.; Litscher, G.; Gao, S.H.; Zhou, S.F.; Yu, Z.L.; Chen, H.Q.; Zhang, S.F.; Tang, M.K.; Sun, J.N.; Ko, K.M.; et al. Historical perspective of traditional indigenous medical practices: The current renaissance and conservation of herbal resources. Evid. Based Complement. Altern. Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Petrovska, B.B. Historical review of medicinal plants’ usage. Pharmacogn. Rev. 2012, 6, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.C. Trace and Evans, Pharmacognosy, 16th ed.; Churchill Livingstone Elsevier: London, UK, 2009. [Google Scholar]
- Furst, R. Zündorf Evidence-Based Phytotherapy in Europe: Where Do We Stand? Planta Med. 2015, 81, 962–967. [Google Scholar] [PubMed]
- Waller, F. Phytotherapie der traditionellen chinesischen Medizin. Z. Physiother. 1998, 19, 77–89. [Google Scholar]
- Leonti, M.; Verpoort, R. Traditional Mediterranean and European herbal medicines. J. Ethnopharmacol. 2017, 199, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jin, Y.; Zhou, C.; Qu, H.; Cheng, Y. Discovering active compounds from mixture of natural products by data mining approach. Med. Biol. Eng. Comput. 2008, 46, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, M.; Barnes, J.; Gibbons, J.; Williamson, E. Fundamentals of Pharmacognosy and Phytotherapy, 2nd ed.; Churchill Livingstone Elsevier: London, UK, 2012. [Google Scholar]
- Cheng, Y.; Wang, Y.; Wang, X. A causal relationship discovery-based approach to identifying active components of herbal medicine. Comput. Biol. Chem. 2006, 30, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Villanueva, J.; Martin Esteban, J. An Insight into a Blockbuster Phytomedicine; Marrubium vulgare L. Herb. More of a Myth than a Reality? Phytother. Res. 2016, 30, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Borisy, A.A.; Elliott, P.J.; Hurst, N.W.; Lee, M.S.; Lehar, J.; Price, E.R.; Serbedzija, G.; Zimmermann, G.R.; Foley, M.A.; Stockwell, B.R.; et al. Systematic discovery of multicomponent therapeutics. Proc. Natl. Acad. Sci. USA 2003, 100, 7977–7982. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, J.D. Phytochemistry and medicinal plants. Phytochemistry 2001, 56, 237–243. [Google Scholar] [CrossRef]
- Williamson, E.M. Synergy and other interactions in phytomedicines. Phytomedicine 2001, 8, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Ulrich-Merzenich, G.; Zeitler, H.; Jobst, D.; Panek, D.; Vetter, H.; Wagner, H. Application of the “-Omic-” technologies in phytomedicine. Phytomedicine 2007, 14, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Atangwho, I.J.; Ebong, P.E.; Eyong, E.U.; Asmawi, M.Z.; Ahmad, M. Synergistic antidiabetic activity of Vernonia amygdalina and Azadirachta indica: Biochemical effects and possible mechanism. J. Ethnopharmacol. 2012, 141, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J.; Ng, C.H.; Schweitzer, I. ‘Omic’ genetic technologies for herbal medicines in psychiatry. Phytother. Res. 2012, 26, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Einbond, L.S.; Shimizu, M.; Ma, H.; Wu, H.A.; Goldsberry, S.; Sicular, S.; Panjikaran, M.; Genovese, G.; Cruz, E. Actein inhibits the Na+-K+-ATPase and enhances the growth inhibitory effect of digitoxin on human breast cancer cells. Biochem. Biophys. Res. Commun. 2008, 375, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.L.; Liao, Z.G.; Zhu, J.Y.; Zhao, G.W.; Yang, M.; Yin, R.L.; Cao, Y.C.; Zhang, J.; Zhao, L.J. The absorption characterization effects and mechanism of Radix Angelicae dahuricae extracts on baicalin in Radix Scutellariae using in vivo and in vitro absorption models. J. Ethnopharmacol. 2012, 139, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Rasoanaivo, P.; Wright, C.W.; Willcox, M.L.; Gilbert, B. Whole plant extracts versus single compounds for the treatment of malaria: Synergy and positive interactions. Malar. J. 2011, 10 (Suppl. 1), S4. [Google Scholar] [CrossRef] [PubMed]
- Wegener, T.; Wagner, H. The active components and the pharmacological multi-target principle of STW 5 (Iberogast). Phytomedicine 2006, 13 (Suppl. 5), 20–35. [Google Scholar] [CrossRef] [PubMed]
- Cañigueral, S.; Tschopp, R. The Development of Herbal Medicinal Products. Quality, Safety, and Efficacy as Key Factors. Pharm. Med. 2008, 22, 107–118. [Google Scholar] [CrossRef]
- Wagner, H.; Ulrich-Merzenich, G. Synergy research: Approaching a new generation of phytopharmaceuticals. Phytomedicine 2009, 16, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Villanueva, J.; Rodriguez Villanueva, L. Experimental and Clinical Pharmacology of Ziziphus jujuba Mills. Phytother. Res. 2017, 31, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aziz, H.; Kelber, O.; Lorkowski, G.; Storr, M. Evaluating the Multitarget Effects of Combinations through Multistep Clustering of Pharmacological Data: The Example of the Commercial Preparation Iberogast. Planta Med. 2017, 83, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Ihekwaba, A.E.; Broomhead, D.S.; Grimley, R.; Benson, N.; White, M.R.; Kell, D.B. Synergistic control of oscillations in the NF-kappaB signalling pathway. Syst. Biol. (Stevenage) 2005, 152, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Villanueva, J.; Martin Esteban, J.; Rodríguez Villanueva, L. A Reassessment of the Marrubium vulgare L. Herb’s Potential Role in Diabetes Mellitus Type 2: First Results Guide the Investigation toward New Horizons. Medicines 2017, 4. [Google Scholar] [CrossRef] [PubMed]
- Ouedraogo, M.; Baudoux, T.; Stévigny, C.; Nortier, J.; Colet, J.M.; Efferth, T.; Qu, F.; Zhou, J.; Chan, K.; Shaw, D.; et al. Review of current and “omics” methods for assessing the toxicity (genotoxicity, teratogenicity and nephrotoxicity) of herbal medicines and mushrooms. J. Ethnopharmacol. 2012, 140, 492–512. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Villanueva, J.; Martin Esteban, J.; Rodríguez Villanueva, L. Solving the puzzle: What is behind our forefathers’ anti-inflammatory remedies? J. Intercult. Ethnopharmacol. 2017, 6, 128–143. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tang, H.; Nicholson, J.K.; Hylands, P.J.; Sampson, J.; Holmes, E. A metabonomic strategy for the detection of the metabolic effects of chamomile (Matricaria recutita L.) ingestion. J. Agric. Food Chem. 2005, 53, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Ulrich-Merzenich, G.; Panek, D.; Zeitler, H.; Wagner, H.; Vetter, H. New perspectives for synergy research with the “omic”-technologies. Phytomedicine 2009, 16, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Buriani, A.; Garcia-Bermejo, M.L.; Bosisio, E.; Xu, Q.; Li, H.; Dong, X.; Simmonds, M.S.; Carrara, M.; Tejedor, N.; Lucio-Cazana, J.; et al. Omic techniques in systems biology approaches to traditional Chinese medicine research: Present and future. J. Ethnopharmacol. 2012, 140, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, N.; Manchikanti, P.; Dey, S. Herbal drugs: Standards and regulation. Fitoterapia 2010, 81, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Claeson, P. Requirements on efficacy of herbal medicinal products. J. Ethnopharmacol. 2014, 158 Pt B, 463–466. [Google Scholar] [CrossRef] [PubMed]
- He, S.M.; Li, C.G.; Liu, J.P.; Chan, E.; Duan, W.; Zhou, S.F. Disposition pathways and pharmacokinetics of herbal medicines in humans. Curr. Med. Chem. 2010, 17, 4072–4113. [Google Scholar] [CrossRef] [PubMed]
- Lan, K.; Jia, W. An integrated metabolomics and pharmacokinetic strategy for multi-component drugs evaluation. Curr. Drug Metab. 2010, 11, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Gertsch, J. Botanical drugs, synergy, and network pharmacology: Forth and back to intelligent mixtures. Planta Med. 2011, 77, 1086–1098. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Noh, K.; Shin, M.; Park, J.; Lee, K.; Nam, H.; Lee, D. In silico profling of systemic efects of drugs to predict unexpected interactions. Nat. Sci. Rep. 2018, 8, 1612. [Google Scholar] [CrossRef] [PubMed]
- Gertsch, J. How scientific is the science in ethnopharmacology? Historical perspectives and epistemological problems. J. Ethnopharmacol. 2009, 122, 177–183. [Google Scholar] [CrossRef] [PubMed]
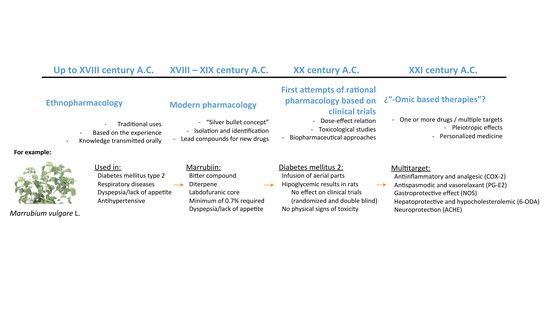
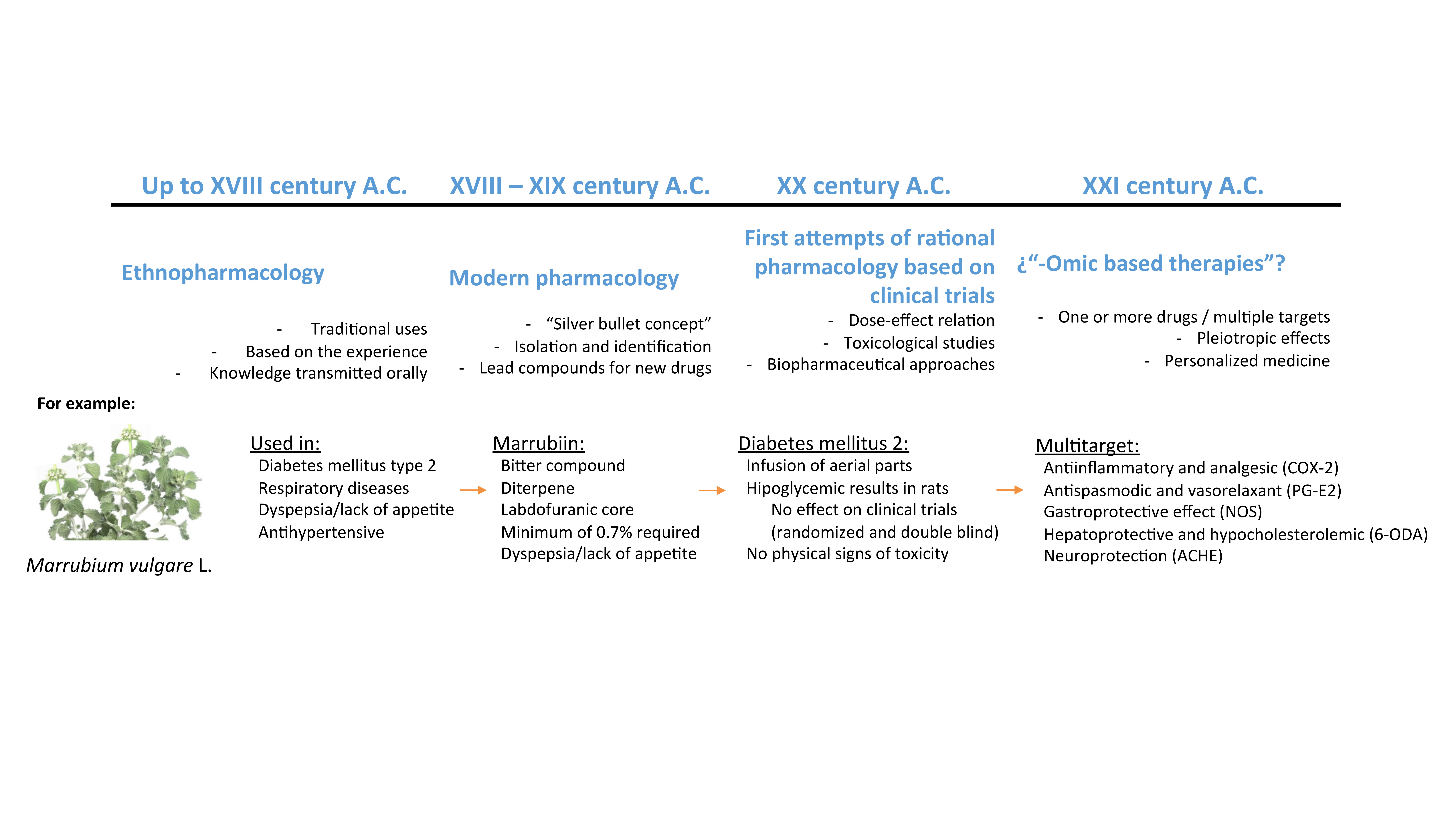
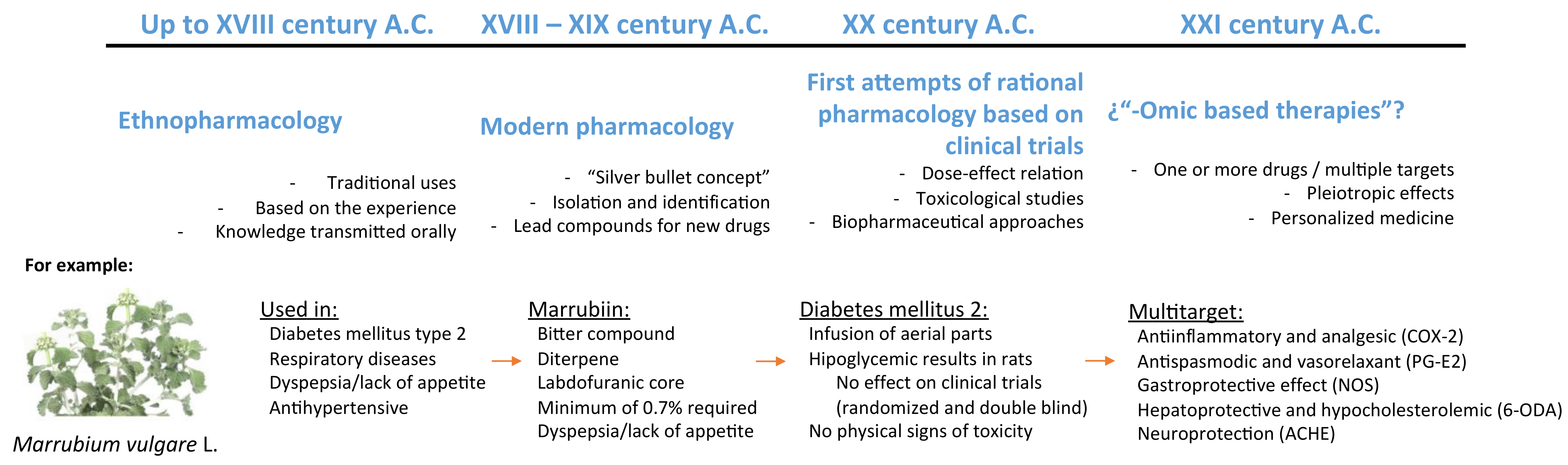
Figure 1.
Schematic representation of the herbal therapeutic evolution flow. Marrubium vulgare L. has been selected to exemplify each of the periods represented. Example data obtained from Rodríguez Villanueva [12,28]. COX-2: cyclo-oxigenase-2; PG-E2: prostaglandin-E2; NOS: nitric oxide synthase; 6-ODA: 6-octadecynoic acid.
Figure 1.
Schematic representation of the herbal therapeutic evolution flow. Marrubium vulgare L. has been selected to exemplify each of the periods represented. Example data obtained from Rodríguez Villanueva [12,28]. COX-2: cyclo-oxigenase-2; PG-E2: prostaglandin-E2; NOS: nitric oxide synthase; 6-ODA: 6-octadecynoic acid.

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rodríguez Villanueva, J.; Martín Esteban, J.; Rodríguez Villanueva, L. Pharmacological Activities of Phytomedicines: A Challenge Horizon for Rational Knowledge. Challenges 2018, 9, 15. https://doi.org/10.3390/challe9010015
AMA Style
Rodríguez Villanueva J, Martín Esteban J, Rodríguez Villanueva L. Pharmacological Activities of Phytomedicines: A Challenge Horizon for Rational Knowledge. Challenges. 2018; 9(1):15. https://doi.org/10.3390/challe9010015
Chicago/Turabian StyleRodríguez Villanueva, Javier, Jorge Martín Esteban, and Laura Rodríguez Villanueva. 2018. "Pharmacological Activities of Phytomedicines: A Challenge Horizon for Rational Knowledge" Challenges 9, no. 1: 15. https://doi.org/10.3390/challe9010015
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.