

Prognostic Implication of Lymphovascular Invasion in Early Gastric Cancer Meeting Endoscopic Submucosal Dissection Criteria: Insights from Radical Surgery Outcomes

Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
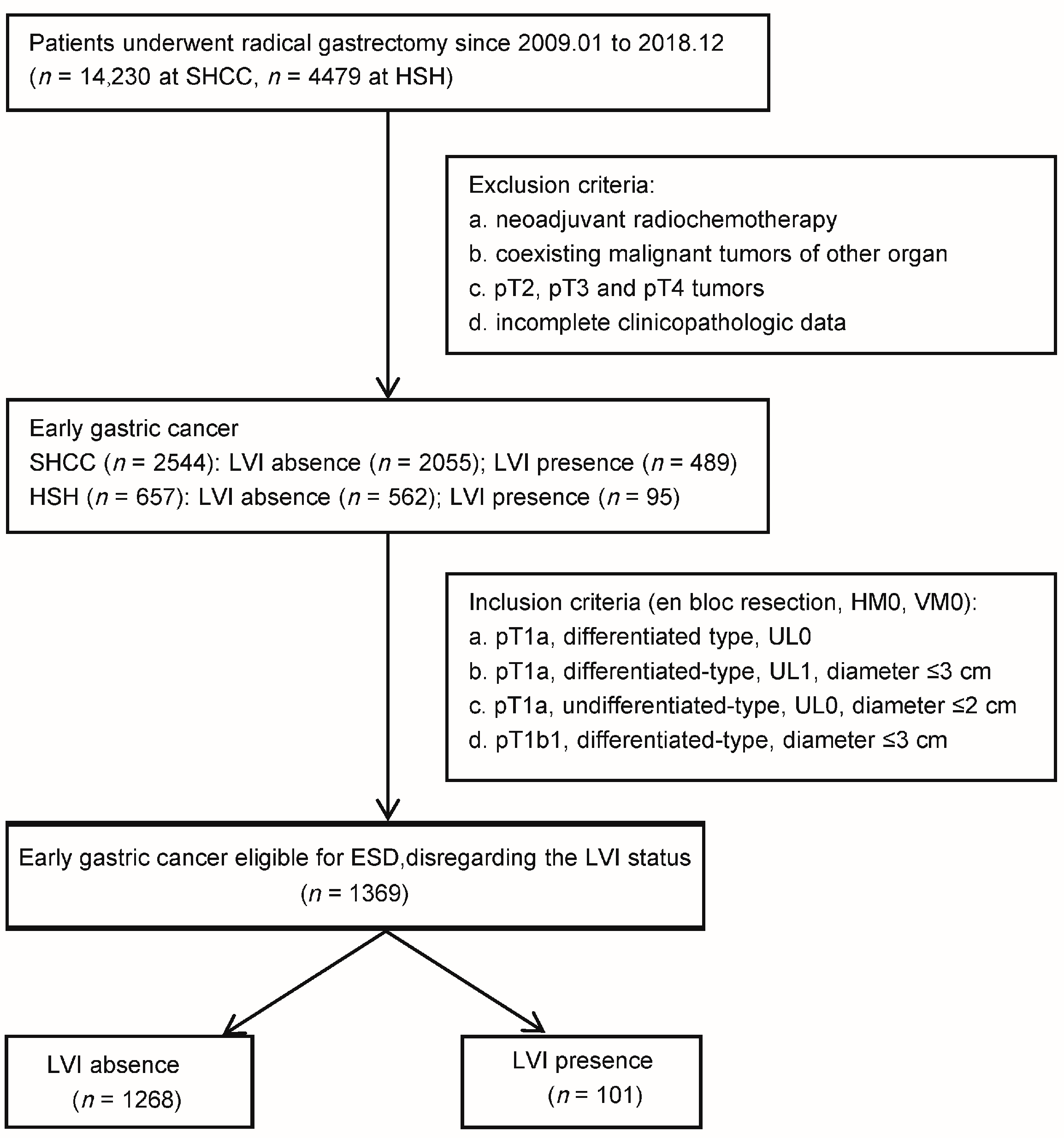
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics of EGC Patients Meeting ESD Criteria
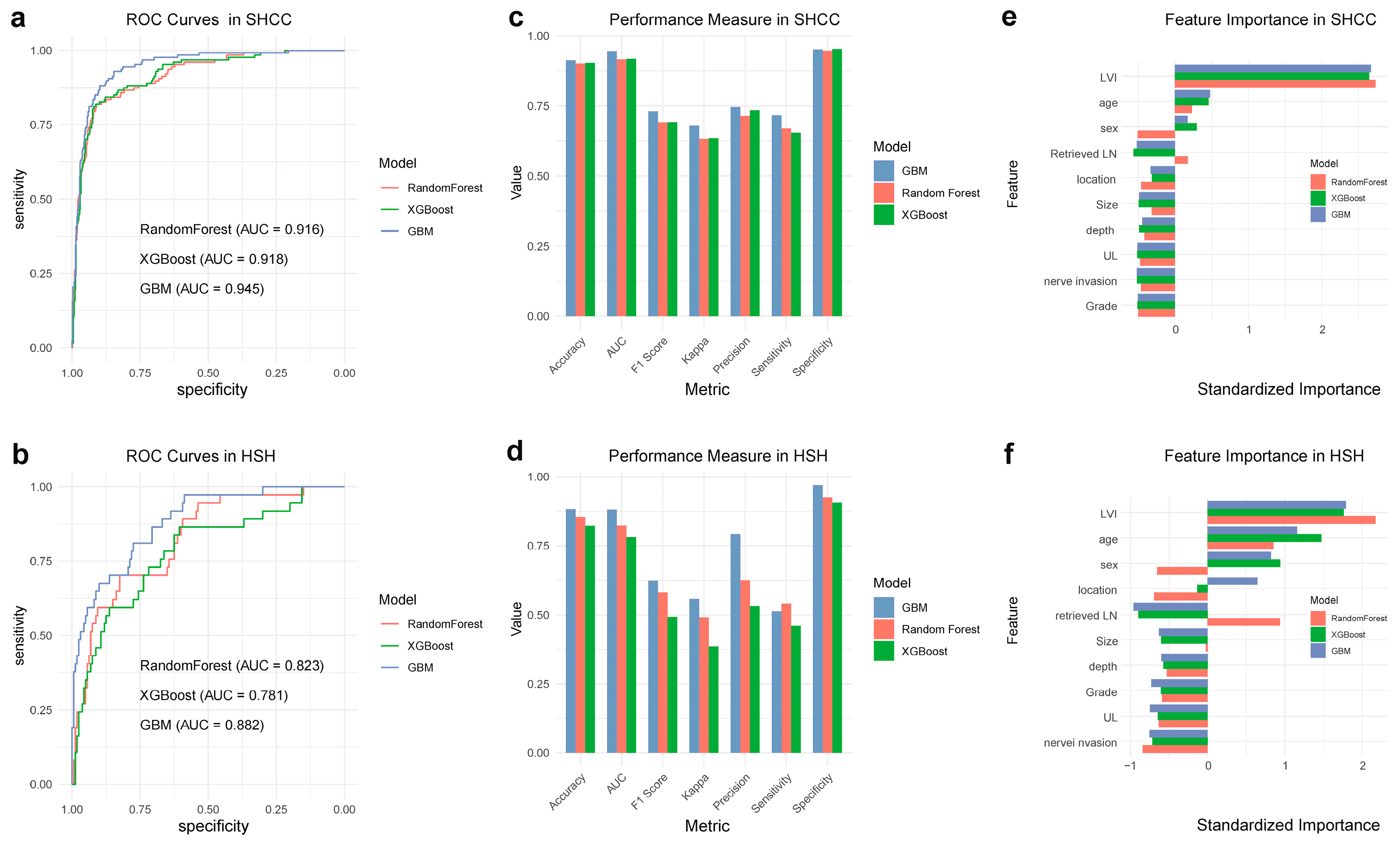
3.2. Evaluating LVI as a Predictive Marker for LNM
3.3. Postoperative Morbidity and Mortality
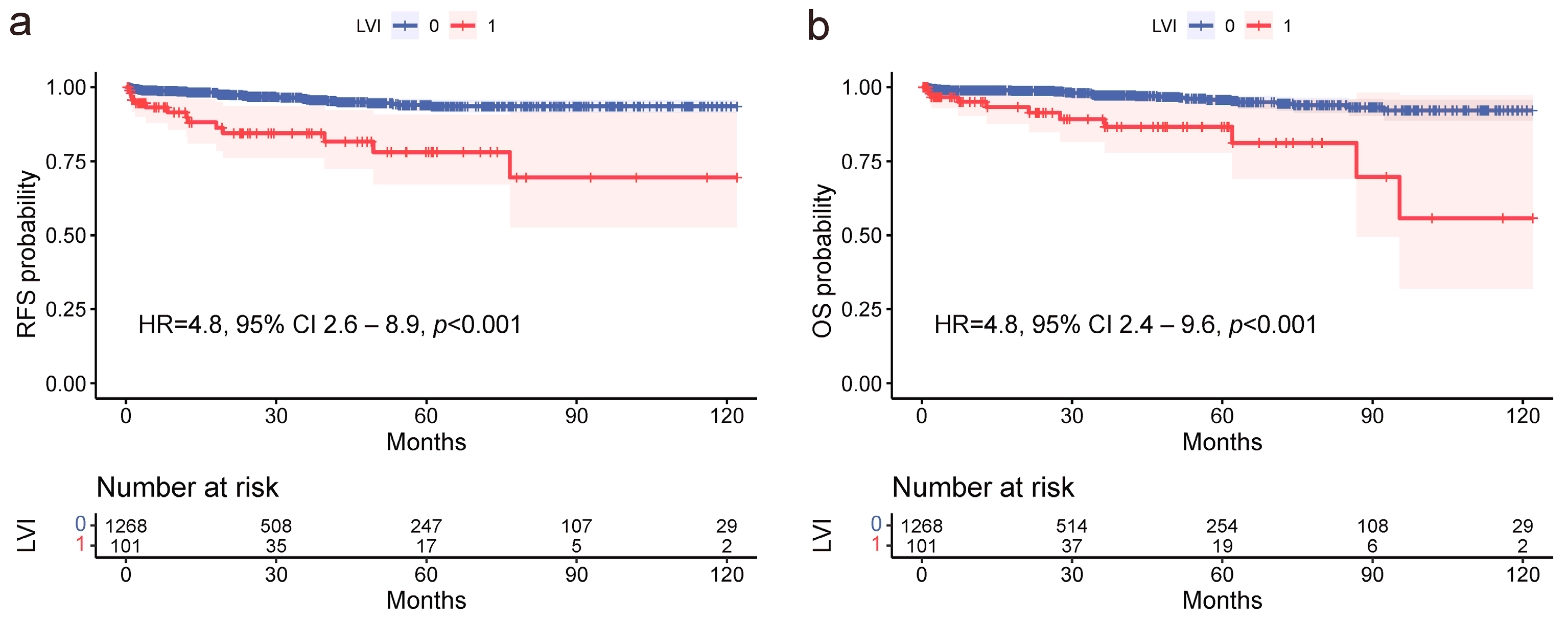
3.4. Prognostic Factors in EGC Patients Meeting ESD Criteria at Both Centers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hatta, W.; Gotoda, T.; Oyama, T.; Kawata, N.; Takahashi, A.; Yoshifuku, Y.; Hoteya, S.; Nakagawa, M.; Hirano, M.; Esaki, M.; et al. A Scoring System to Stratify Curability after Endoscopic Submucosal Dissection for Early Gastric Cancer: “eCura System”. Am. J. Gastroenterol. 2017, 112, 874–881. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Yoshida, N.; Yano, T.; Horimatsu, T.; Uedo, N.; Kawata, N.; Kanzaki, H.; Hori, S.; Yao, K.; Abe, S.; et al. Assessment of Outcomes From 1-Year Surveillance After Detection of Early Gastric Cancer Among Patients at High Risk in Japan. JAMA Netw. Open 2022, 5, e2227667. [Google Scholar] [CrossRef]
- Liu, Q.; Ding, L.; Qiu, X.; Meng, F. Updated Evaluation of Endoscopic Submucosal Dissection versus Surgery for Early Gastric Cancer: A Systematic Review and Meta-Analysis. Int. J. Surg. 2020, 73, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Lordick, F.; Carneiro, F.; Cascinu, S.; Fleitas, T.; Haustermans, K.; Piessen, G.; Vogel, A.; Smyth, E.C. Gastric Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2022, 33, 1005–1020. [Google Scholar] [CrossRef]
- Ajani, J.A.; D’Amico, T.A.; Bentrem, D.J.; Chao, J.; Cooke, D.; Corvera, C.; Das, P.; Enzinger, P.C.; Enzler, T.; Fanta, P.; et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 167–192. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021 (6th Edition). Gastric Cancer 2023, 26, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Guideline Committee of the Korean Gastric Cancer Association (KGCA); Development Working Group & Review Panel. Korean Practice Guideline for Gastric Cancer 2018: An Evidence-Based, Multi-Disciplinary Approach. J. Gastric Cancer 2019, 19, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Song, J.H.; Lee, S.; Cho, M.; Kim, Y.M.; Kim, H.-I.; Hyung, W.J. Lymphovascular Invasion: Traditional but Vital and Sensible Prognostic Factor in Early Gastric Cancer. Ann. Surg. Oncol. 2021, 28, 8928–8935. [Google Scholar] [CrossRef]
- Ma, Z.; Liang, C.; Huang, Y.; He, L.; Liang, C.; Chen, X.; Huang, X.; Xiong, Y.; Liu, Z. Can Lymphovascular Invasion Be Predicted by Preoperative Multiphasic Dynamic CT in Patients with Advanced Gastric Cancer? Eur. Radiol. 2017, 27, 3383–3391. [Google Scholar] [CrossRef]
- Jiang, W.; Meng, R.; Cheng, Y.; Wang, H.; Han, T.; Qu, N.; Yu, T.; Hou, Y.; Xu, S. Intra- and Peritumoral Based Radiomics for Assessment of Lymphovascular Invasion in Invasive Breast Cancer. J. Magn. Reson. Imaging 2024, 59, 613–625. [Google Scholar] [CrossRef]
- Lee, H.; Yoo, S.-Y.; Park, I.J.; Hong, S.-M.; Lim, S.-B.; Yu, C.S.; Kim, J.C. The Prognostic Reliability of Lymphovascular Invasion for Patients with T3N0 Colorectal Cancer in Adjuvant Chemotherapy Decision Making. Cancers 2022, 14, 2833. [Google Scholar] [CrossRef]
- Sako, A.; Kitayama, J.; Ishikawa, M.; Yamashita, H.; Nagawa, H. Impact of Immunohistochemically Identified Lymphatic Invasion on Nodal Metastasis in Early Gastric Cancer. Gastric Cancer 2006, 9, 295–302. [Google Scholar] [CrossRef]
- Zhang, C.-D.; Ning, F.-L.; Zeng, X.-T.; Dai, D.-Q. Lymphovascular Invasion as a Predictor for Lymph Node Metastasis and a Prognostic Factor in Gastric Cancer Patients under 70 Years of Age: A Retrospective Analysis. Int. J. Surg. 2018, 53, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Afrash, M.R.; Shafiee, M.; Kazemi-Arpanahi, H. Establishing Machine Learning Models to Predict the Early Risk of Gastric Cancer Based on Lifestyle Factors. BMC Gastroenterol. 2023, 23, 6. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.-L.; Dong, J.; Zhang, C.; Huang, Y.-B.; Pan, W. Application of Machine Learning in the Diagnosis of Gastric Cancer Based on Noninvasive Characteristics. PLoS ONE 2020, 15, e0244869. [Google Scholar] [CrossRef]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine Learning Applications in Cancer Prognosis and Prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef]
- Tian, H.; Ning, Z.; Zong, Z.; Liu, J.; Hu, C.; Ying, H.; Li, H. Application of Machine Learning Algorithms to Predict Lymph Node Metastasis in Early Gastric Cancer. Front. Med. 2022, 8, 759013. [Google Scholar] [CrossRef]
- Talebi, A.; Celis-Morales, C.A.; Borumandnia, N.; Abbasi, S.; Pourhoseingholi, M.A.; Akbari, A.; Yousefi, J. Predicting Metastasis in Gastric Cancer Patients: Machine Learning-Based Approaches. Sci. Rep. 2023, 13, 4163. [Google Scholar] [CrossRef]
- Park, J.W.; Ahn, S.; Lee, H.; Min, B.-H.; Lee, J.H.; Rhee, P.-L.; Kim, K.-M.; Kim, J.J. Predictive Factors for Lymph Node Metastasis in Early Gastric Cancer with Lymphatic Invasion after Endoscopic Resection. Surg. Endosc. 2017, 31, 4419–4424. [Google Scholar] [CrossRef] [PubMed]
- An, J.Y.; Baik, Y.H.; Choi, M.G.; Noh, J.H.; Sohn, T.S.; Kim, S. Predictive Factors for Lymph Node Metastasis in Early Gastric Cancer With Submucosal Invasion: Analysis of a Single Institutional Experience. Ann. Surg. 2007, 246, 749–753. [Google Scholar] [CrossRef]
- Son, S.Y.; Park, J.Y.; Ryu, K.W.; Eom, B.W.; Yoon, H.M.; Cho, S.J.; Lee, J.Y.; Kim, C.G.; Lee, J.H.; Kook, M.-C.; et al. The Risk Factors for Lymph Node Metastasis in Early Gastric Cancer Patients Who Underwent Endoscopic Resection: Is the Minimal Lymph Node Dissection Applicable? A Retrospective Study. Surg. Endosc. 2013, 27, 3247–3253. [Google Scholar] [CrossRef]
- Wu, L.; Liang, Y.; Zhang, C.; Wang, X.; Ding, X.; Huang, C.; Liang, H. Prognostic Significance of Lymphovascular Infiltration in Overall Survival of Gastric Cancer Patients after Surgery with Curative Intent. Chin. J. Cancer Res. 2019, 31, 785–796. [Google Scholar] [CrossRef]
- Noma, D.; Inamura, K.; Matsuura, Y.; Hirata, Y.; Nakajima, T.; Yamazaki, H.; Hirai, Y.; Ichinose, J.; Nakao, M.; Ninomiya, H.; et al. Prognostic Effect of Lymphovascular Invasion on TNM Staging in Stage I Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2018, 19, e109–e122. [Google Scholar] [CrossRef]
- Ono, H.; Yao, K.; Fujishiro, M.; Oda, I.; Nimura, S.; Yahagi, N.; Iishi, H.; Oka, M.; Ajioka, Y.; Ichinose, M.; et al. Guidelines for Endoscopic Submucosal Dissection and Endoscopic Mucosal Resection for Early Gastric Cancer. Dig. Endosc. 2016, 28, 3–15. [Google Scholar] [CrossRef]
- Yamamoto, H. Endoscopic Submucosal Dissection--Current Success and Future Directions. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 519–529. [Google Scholar] [CrossRef]
- Liu, P.; Li, L.; Wang, J.; Song, H.; He, C. Lymph Node Metastasis Risk Factors and Applicability of Endoscopic Submucosal Dissection in Mixed-Type Early Gastric Cancer in Chinese Patients. J. Gastrointest. Oncol. 2021, 12, 1444–1453. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Gotoda, T.; Hatta, W.; Oyama, T.; Kawata, N.; Takahashi, A.; Yoshifuku, Y.; Hoteya, S.; Nakagawa, M.; Hirano, M.; et al. Survival Benefit of Additional Surgery After Non-Curative Endoscopic Submucosal Dissection for Early Gastric Cancer: A Propensity Score Matching Analysis. Ann. Surg. Oncol. 2017, 24, 3353–3360. [Google Scholar] [CrossRef] [PubMed]
- Kawata, N.; Kakushima, N.; Takizawa, K.; Tanaka, M.; Makuuchi, R.; Tokunaga, M.; Tanizawa, Y.; Bando, E.; Kawamura, T.; Sugino, T.; et al. Risk Factors for Lymph Node Metastasis and Long-Term Outcomes of Patients with Early Gastric Cancer after Non-Curative Endoscopic Submucosal Dissection. Surg. Endosc. 2017, 31, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Eom, B.W.; Kim, Y.-I.; Kim, K.H.; Yoon, H.M.; Cho, S.-J.; Lee, J.Y.; Kim, C.G.; Kook, M.-C.; Kim, Y.-W.; Nam, B.-H.; et al. Survival Benefit of Additional Surgery after Noncurative Endoscopic Resection in Patients with Early Gastric Cancer. Gastrointest. Endosc. 2017, 85, 155–163.e3. [Google Scholar] [CrossRef] [PubMed]
- Al-Rohil, R.N.; Milton, D.R.; Nagarajan, P.; Curry, J.L.; Feldmeyer, L.; Torres-Cabala, C.A.; Ivan, D.; Prieto, V.G.; Tetzlaff, M.T.; Aung, P.P. Intratumoral and Peritumoral Lymphovascular Invasion Detected by D2-40 Immunohistochemistry Correlates with Metastasis in Primary Cutaneous Merkel Cell Carcinoma. Hum. Pathol. 2018, 77, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-I.; Kook, M.-C.; Choi, J.E.; Lee, J.Y.; Kim, C.G.; Eom, B.W.; Yoon, H.M.; Ryu, K.W.; Kim, Y.-W.; Choi, I.J. Evaluation of Submucosal or Lymphovascular Invasion Detection Rates in Early Gastric Cancer Based on Pathology Section Interval. J. Gastric Cancer 2020, 20, 165–175. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (N) | LVI-Positive | LVI-Negative | p Value | |
|---|---|---|---|---|
| Mean age (years) | 58.5 ± 10.8 | 58.0 ± 12.0 | 58.6 ± 10.7 | 0.629 |
| Sex | ||||
| M | 934 (68.2) | 50 (49.5) | 884 (69.7) | <0.001 |
| F | 435 (31.8) | 51 (50.5) | 384 (30.3) | |
| Tumor location | ||||
| U | 197 (14.4) | 8 (7.9) | 189 (14.9) | 0.081 |
| M | 226 (16.5) | 22 (21.8) | 204 (16.1) | |
| L | 946 (69.1) | 71 (70.3) | 875 (69.0) | |
| Differentiation | ||||
| Differentiated | 932 (68.1) | 61 (60.4) | 871 (68.7) | 0.085 |
| Undifferntiated | 437 (31.9) | 40 (39.6) | 397 (31.3) | |
| Depth | ||||
| M | 1060 (77.4) | 62 (61.4) | 998 (78.7) | <0.001 |
| SM | 309 (22.6) | 39 (38.6) | 270 (21.3) | |
| Tumor size | ||||
| ≤10 mm | 476 (34.8) | 25 (24.8) | 451 (35.6) | 0.071 |
| ≤20 mm | 628 (45.9) | 51 (50.5) | 577 (45.5) | |
| >20 mm | 265 (19.4) | 25 (24.8) | 240 (18.9) | |
| Ulcer finding | ||||
| Absence | 1259 (92.0) | 96 (95.0) | 1163 (91.7) | 0.236 |
| Presence | 110 (8.0) | 5 (5.0) | 105 (8.3) | |
| Nerve invasion | ||||
| Absence | 1358 (99.2) | 96 (95.0) | 1262 (99.5) | <0.001 |
| Presence | 11 (0.8) | 5 (5.0) | 6 (0.5) | |
| Lymph node metastasis | ||||
| Absence | 1310 (95.7) | 57 (56.4) | 1253 (98.8) | <0.001 |
| Presence | 59 (4.3) | 44 (43.6) | 15 (1.2) | |
| N stage | ||||
| N0 | 1040 (92.9) | 36 (37.5) | 1004 (98.1) | <0.001 |
| N1 | 55 (4.9) | 41 (42.7) | 14 (1.4) | |
| N2 | 18 (1.6) | 15 (15.6) | 3 (0.3) | |
| N3 | 6 (0.5) | 4 (4.2) | 2 (0.2) | |
| Dissection | ||||
| D1/D1+ | 673 (49.2) | 38 (37.6) | 633 (49.9) | 0.017 |
| D2 | 696 (50.8) | 63 (62.4) | 635 (50.1) | |
| Reconstruction | ||||
| Billroth-I | 433 (31.6) | 29 (28.7) | 404 (31.9) | 0.795 |
| Billroth-II | 138 (10.1) | 11 (10.9) | 127 (10.0) | |
| Billroth-II with Braun | 273 (19.9) | 26 (25.7) | 247 (19.5) | |
| Roux-en-Y after distal gastrectomy | 198 (14.5) | 15 (14.9) | 183 (14.4) | |
| Roux-en-Y after total gastrectomy | 177 (12.9) | 10 (9.9) | 167 (13.2) | |
| Esophagogastrostomy after proximal gastrectomy | 103 (7.5) | 7 (6.9) | 96 (7.6) | |
| Double-tract after proximal gastrectomy | 47 (3.4) | 3 (3.0) | 44 (3.5) |
| Total (%) | LVI-Positive | LVI-Negative | p Value | |
|---|---|---|---|---|
| Overall complication | 225 (16.4) | 23 (23.0) | 202 (15.9) | 0.074 |
| Surgical-related | ||||
| Wound problem | 22 (1.6) | 2 (2.0) | 20 (1.6) | 0.757 |
| Postoperative bleeding | 35 (2.6) | 3 (3.0) | 32 (2.5) | 0.784 |
| Anastomotic leakage | 25 (1.8) | 2 (2.0) | 23 (1.8) | 0.904 |
| Abdominal infection | 16 (1.2) | 1 (1.0) | 15 (1.2) | 0.862 |
| Intestinal obstruction | 4 (0.3) | 0 (0) | 4 (0.3) | 0.572 |
| Stenosis | 6 (0.4) | 1 (1.0) | 5 (0.4) | 0.383 |
| Gastric stasis | 7 (0.5) | 1 (1.0) | 6 (0.4) | 0.483 |
| Lymphatic leakage | 10 (0.7) | 1 (1.0) | 9 (0.7) | 0.750 |
| Non-surgical-related | ||||
| Pulmonary infection | 17 (1.2) | 1 (1.0) | 16 (1.3) | 0.812 |
| Pleural effusion | 31 (2.2) | 4 (4.0) | 27 (2.1) | 0.234 |
| Cardiovascular system | 9 (0.7) | 1 (1.0) | 8 (0.6) | 0.667 |
| Cerebrovascular disease | 5 (0.4) | 0 (0) | 5 (0.4) | 0.527 |
| Urinary problem | 7 (0.5) | 1 (1.0) | 6 (0.4) | 0.488 |
| Hepatic problem | 10 (0.7) | 2 (2.0) | 8 (0.6) | 0.128 |
| Others | 21 (1.5) | 3 (3.0) | 18 (1.4) | 0.223 |
| Operative mortablity | 2 (0.1) | 0 (0) | 2 (0.2) | 0.69 |
| RFS | OS | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | ||||||||
| ≥70 vs. <70 | 3.6 (2.0–6.4) | <0.001 | 3.4 (1.9–6.1) | <0.001 | 3.0 (1.5–5.9) | <0.001 | 2.9 (1.5–5.8) | 0.002 |
| Sex | ||||||||
| M vs. F | 1.2 (0.7–2.2) | 0.485 | 1.2 (0.6–2.4) | 0.517 | ||||
| Tumor location | ||||||||
| M vs. U | 1.0 (0.5–2.1) | 0.991 | 1.4 (0.6–3.1) | 0.416 | ||||
| L vs. U | 0.8 (0.4–1.7) | 0.559 | 0.9 (0.4–2.1) | 0.821 | ||||
| Differentiation | ||||||||
| Undifferntiated vs. Differentiated | 0.6 (0.3–1.1) | 0.126 | 0.6 (0.3–1.2) | 0.163 | ||||
| Depth | ||||||||
| SM1 vs. M | 1.0 (0.5–2.0) | 0.931 | 0.9 (0.4–1.9) | 0.720 | ||||
| Tumor size | ||||||||
| >20 mm vs. ≤20 mm | 1.5 (0.8–2.9) | 0.221 | 1.8 (0.9–3.7) | 0.106 | ||||
| Ulcer finding | ||||||||
| Presence vs. Absence | 1.3 (0.6–3.0) | 0.535 | 1.6 (0.7–3.7) | 0.313 | ||||
| Lymph node metastasis | ||||||||
| Presence vs. Absence | 6.2 (3.2–12.2) | <0.001 | —— | —— | 5.2 (2.4–11.2) | <0.001 | —— | —— |
| Lymphovascular invasion | ||||||||
| Presence vs. Absence | 4.8 (2.6–8.9) | <0.001 | 4.5 (2.4–8.6) | <0.001 | 4.8 (2.4–9.6) | <0.001 | 4.7 (2.3–9.4) | <0.001 |
| Nerve Invasion | ||||||||
| Presence vs. Absence | 4.1 (1.0–16.9) | 0.050 | 2.7 (0.4–19.5) | 0.331 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, B.; Li, H.; Gu, X.; Cai, H. Prognostic Implication of Lymphovascular Invasion in Early Gastric Cancer Meeting Endoscopic Submucosal Dissection Criteria: Insights from Radical Surgery Outcomes. Cancers 2024, 16, 979. https://doi.org/10.3390/cancers16050979
Sun B, Li H, Gu X, Cai H. Prognostic Implication of Lymphovascular Invasion in Early Gastric Cancer Meeting Endoscopic Submucosal Dissection Criteria: Insights from Radical Surgery Outcomes. Cancers. 2024; 16(5):979. https://doi.org/10.3390/cancers16050979
Chicago/Turabian StyleSun, Bo, Huanhuan Li, Xiaodong Gu, and Hong Cai. 2024. "Prognostic Implication of Lymphovascular Invasion in Early Gastric Cancer Meeting Endoscopic Submucosal Dissection Criteria: Insights from Radical Surgery Outcomes" Cancers 16, no. 5: 979. https://doi.org/10.3390/cancers16050979