1. Introduction
The prognostic impact of tumor-infiltrating immune cell (TIIC) populations in cervical cancer is still debated, probably due to the fact that prognostic studies on TIICs in cervical cancer cases are limited [
1]. This is surprising because the cytotoxic activities of immune cells isolated from gynecologic malignant tumors (including uterine cervical cancers) against various fresh tumor cells were reported more than 30 years ago [
2].
In addition to immune cell quantification, major effort has been put into the isolation and characterization of TILs from cervical carcinomas in recent years [
3]. In order to define the anticancer-directed immune response in situ, the group of Höhn et al. characterized CD4(+) and CD8(+) T cells from peripheral blood lymphocytes, freshly harvested tumor tissue and immune cells from a patient with cervical cancer [
4]. The group of Santin et al. found that cervical cancer-infiltrating immune cells contain higher numbers of type 1 cytokine expressors and DR+ T cells compared with lymphocytes from tumor draining lymph nodes and peripheral blood [
5].
Additional research approaches include the immune concept of human papillomaviruses and related antigens in local cancer milieu of human cervical neoplasia [
6]. Immune cells in the tumor microenvironment may be functionally inhibited and lose the ability to clonally proliferate because of decreased expression of IL-2Rα [
6].
A more recent study on infiltrating immune cells characterization showed that tumor-infiltrating lymphocytes in cervical cancers contain a higher proportion of FoxP3(+) T lymphocytes [
7]. In addition, our own studies showed that high CCL22(+)-infiltrating cells, particularly M2-like macrophages, are associated with a poor outcome of cervical cancer patients [
8]. CCL22 expression is positively correlated with FoxP3 expression [
8], could polarize TAMs toward M2a macrophages [
9] and may represent a novel prognostic marker and therapeutic target for the treatment of cervical cancer.
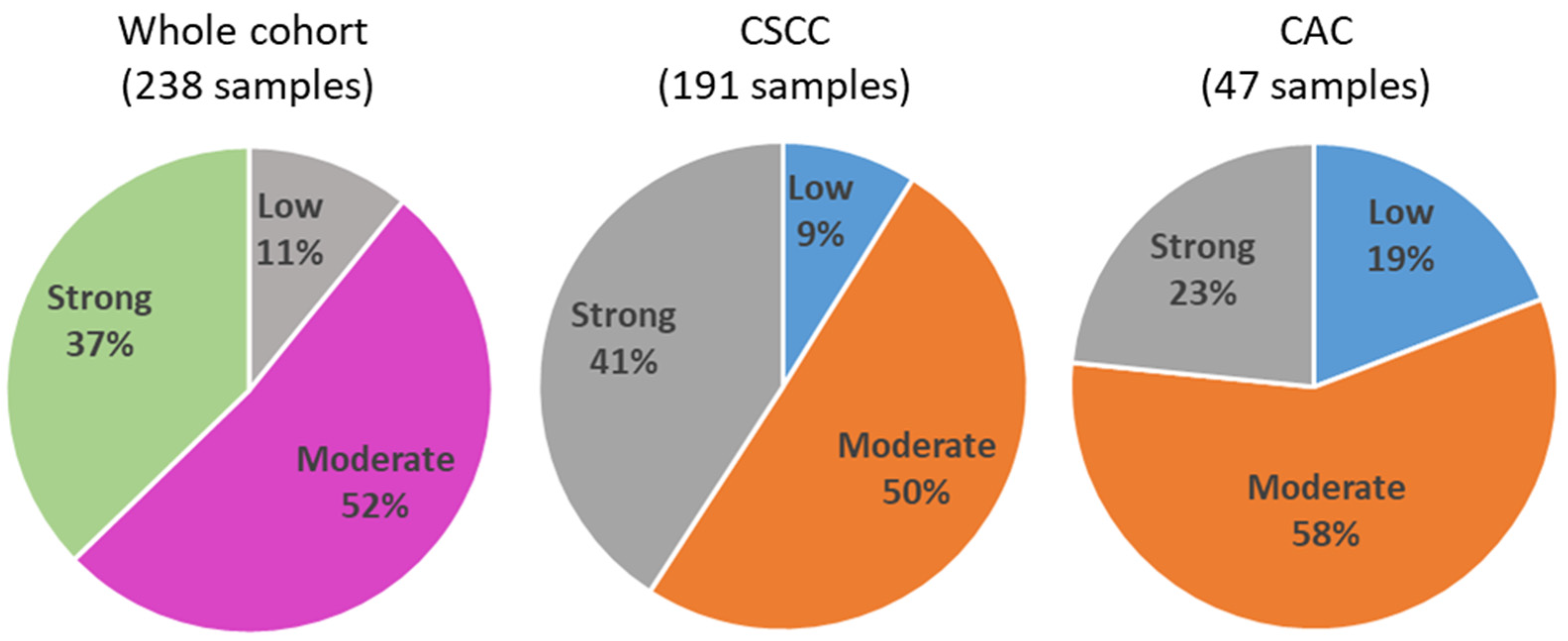
Because the link between cervical cancer histopathological subtypes, prognosis and immune infiltration is still unclear, the aim of this study was to quantify the stromal density of TIICs cells in a panel of 238 sporadic cervical cancers. Using this cohort, cells with lymphocyte or plasma cell morphology were assessed in three classes (low, moderate and strong infiltration), and we investigated the correlation with cervical cancer subtype and patient survival.
4. Discussion
Within this study, we analyzed the density of TIICs in a cohort of 238 cervical cancer cases in relation to the histological subtype and patient survival. This scoring of inflammatory cells was significantly enhanced in CSCC versus CAC. Survival analyses of our patient cohort showed that patients with CSCC had a significantly better OS than patients with CAC, this difference being observed only in the group of patients with low TIIC. This is in line with Chen et al., who describe a shorter OS for patients with less intraepithelial CD8+ lymphocyte counts [
18]. Interestingly, immune infiltration was an independent positive prognosticator for DFS in patients with CSCC.
Because survival rates are different in CSCC compared to CAC, we performed correlation analyses separately for both histological subtypes. In the group of CSCC, tumor infiltration by immune cells was negatively correlated with age, FIGO stage and the histone protein modification H3K4me3; the latter was analyzed in a recent study of our group [
6]. H3K4 methylation is a modification that occurs at the fourth lysine residue of the N-terminus of histone H3. It can be mono-, di- and trimethylated, which makes the analysis of its effects on the genome even more complex [
19,
20]. H3K4me3 is generally associated with transcriptional activation and has been proposed as a predictive factor of poor prognosis in several types of cancer, such as liver and cervical cancer [
15,
21]. In our former analyses, high expression of H3K4me3 was associated with reduced overall and recurrence-free survival; this is in accordance with our negative correlation results with TIIC infiltration. Within this study, we found that CSCC patients with strong TIIC infiltration showed the longest DFS time.
In the group of CAC patients, tumor infiltration by immune cells showed a positive correlation with p16 [
16] and with the glucocorticoid receptor (GR) [
14] and a negative correlation with MDM2 [
16]. The cell cycle regulation protein p16 is expressed at high levels in HPV-infected epithelial cells, which is why it acts as a marker for the diagnosis of an HPV-associated carcinoma [
22,
23]. The positive association of high TIIC rates and p16 expression has already been described in a variety of carcinomas, including oropharyngeal and hypopharyngeal [
24,
25], breast [
26], oropharynx squamous cell carcinomas [
27] and others, but not in cervical cancer cases and not in relation to histopathology. MDM2 promotes the ubiquitination and degradation of p53 [
28]. On the one hand, p53 is regulated by MDM2 oncoprotein through a negative feedback mechanism in non-carcinoma tissue. On the other hand, there is an association between MDM2 and p53 polymorphisms and the advancement of cervical carcinoma [
29]. Again, our findings are in agreement with another study on head and neck squamous cell carcinomas, showing that proliferative lymphocytes are vulnerable to MDM2 inhibition [
30]. This finding might explain that high expression of MDM2 is associated with low TIIC rates in the adenocarcinoma subtype of cervical cancer. Finally, we detected a positive correlation of TIIC with GR in CAC cases. Although this relationship has not been described before, triple-negative breast cancers with expression of glucocorticoid receptor in immune cells showed a better prognosis [
31]. Our former study showed the same result; an advanced GR expression went along with significantly better overall survival compared to low GR expression in cervical cancer cells [
14].
It has been long known that patients with CSCC have a significantly better OS than patients with CAC [
32,
33], and this was also confirmed with our collection of patients. Inclusion of TIIC revealed that this effect is determined only in the group of low TIIC infiltration. In addition, in that group, no patient with CSCC and low TIIC infiltration died. Although this concerns only a small group of patients (17 out of 191; 8.9%), this subgroup can be reassured about their OS rate.
In contrast, in CSCC cases, patients with low peritumoral inflammation showed a very short DFS time. Immune infiltration was an independent positive prognosticator for DFS in patients with CSCC. Patients with CSCC and low levels of TIIC showed the shortest DFS time whereas patients with CSCC and strong TIIC infiltration showed the longest DFS time. On first viewing, this seems to be contradictory with the OS rate of patients with low TIIC. In general, recurrence is not protective, and this was also true within our study group. We saw a strong correlation of recurrence and fatality rate in the whole cohort of squamous carcinoma cases (Correlation Coefficient = 0.451,
p < 0.001). Therefore, only the group of CSCC patients with low TIIC seemed to be not affected by a worse outcome in combination with early recurrence. In other tumor entities, such as oral squamous carcinomas (OSCC), TILs in the nonrecurrent group were significantly higher than those in the recurrent group [
34]. In addition, a high ratio of TILs was associated with an OS improvement in OSCC patients. This is in opposite to our findings on cervical cancer. On the other hand, low PD-L1 expression in TILs predicted local recurrence in oral squamous cell carcinomas [
35]. Although we did not investigate PD-L1 on TIICs, this could also be an explanation for our findings.
5. Limitations
This study has some limitations, considering its retrospective nature and the way TIICs were assessed. For instance, we herein only performed a global analysis of TIICs, and since these cells may be immunogenic or immune-suppressive, more precise methods based on immunohistochemical detection of the different lymphocyte subtypes (including cytotoxic and regulatory T cells, or B/plasma cells) would have been more informative. These points will be addressed in further studies, which are also needed to determine the prognostic value of checkpoint molecule expression on different TIIC populations.
Another limitation is the missing data for the kind of recurrence observed (local recurrence, metastasis to local lymph nodes or distant organs). In addition, individual groups, e.g., CAC with a low TIIC level, are very small, so that a check on another cohort should be performed before generalizing the results.




 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
](https://doi.org/10.5281/zenodo.8177051){kind=link}