
Robotic versus Laparoscopic Partial Nephrectomy in the New Era: Systematic Review
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Mining
2.3. Risk of Bias Assessment
2.4. Data Analysis
2.5. Data Synthesis
3. Results
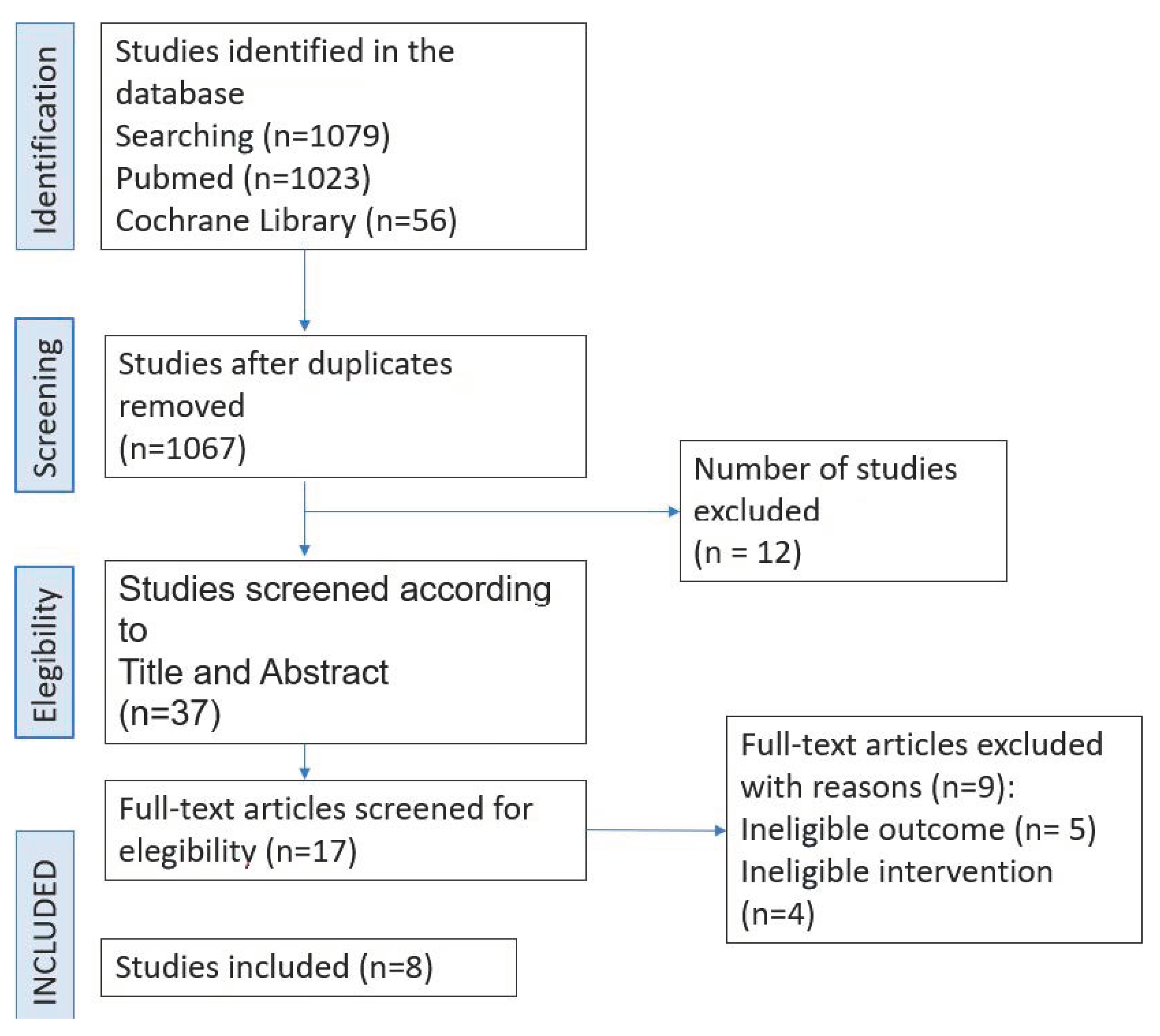
3.1. Selection of Studies
3.2. Analyzed Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chow, W.H.; Devesa, S.S.; Warren, J.L.; Fraumeni, J.F., Jr. Rising incidence of renal cell cancer in the United States. JAMA 1999, 281, 1628–1631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef]
- Thompson, R.H.; Lane, B.R.; Lohse, C.M.; Leibovich, B.C.; Fergany, A.; Frank, I.; Campbell, S.C. Renal function after partial ne-phrectomy: Effect of warm ischemia relative to quantity and quality of pre-served kidney. Urology 2012, 79, 356–360. [Google Scholar] [CrossRef]
- Gul, Z.G.; Tam, A.; Badani, K.K. Robotic partial nephrectomy: The current status. Indian J. Urol. 2020, 36, 16–20. [Google Scholar]
- Chen, K.; MBeeraka, N.; Zhang, J.; Reshetov, I.V.; Nikolenko, V.N.; Sinelnikov, M.Y.; Mikhaleva, L.M. Efficacy of da Vinci robot-assisted lymph node surgery than conventional axillary lymph node dissection in breast cancer-A comparative study. Int. J. Med. Robot. Comput. Assist. Surg. MRCAS 2021, 17, e2307. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, J.; Beeraka, N.M.; Sinelnikov, M.Y.; Zhang, X.; Cao, Y.; Lu, P. Robot-Assisted Minimally Invasive Breast Surgery: Recent Evidence with Comparative Clinical Outcomes. J. Clin. Med. 2022, 11, 1827. [Google Scholar] [CrossRef] [PubMed]
- Gettman, M.T.; Blute, M.L.; Chow, G.K.; Neururer, R.; Bartsch, G.; Peschel, R. Robotic-assisted laparoscopic partial nephrectomy: Technique and initial clinical ex-perience with daVinci robotic system. Urology 2004, 64, 914–918. [Google Scholar] [CrossRef]
- Amparore, D.; Piramide, F.; De Cillis, S.; Verri, P.; Piana, A.; Pecoraro, A.; Bur-gio, M.; Manfredi, M.; Carbonara, U.; Marchioni, M.; et al. Robotic partial nephrectomy in 3D virtual reconstructions era: Is the paradigm changed? World J. Urol. 2022, 40, 659–670. [Google Scholar] [CrossRef]
- Zhang, K.; Wang, L.; Sun, Y.; Wang, W.; Hao, S.; Li, H.; Lu, J.; O’Reilly, D.A.; Na, Y.; Zhu, G. Combination of holographic imaging with robotic partial nephrectomy for renal hilar tumor treatment. Int. Urol. Nephrol. 2022, 54, 1837–1844. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Zaid, H.B.; Parker, W.P.; Lohse, C.M.; Cheville, J.C.; Boorjian, S.A.; Leibo-vich, B.C.; Thompson, R.H. Patient factors associated with 30-day complications after partial nephrectomy: A contemporary update. Urol. Oncol. 2017, 35, 153.e1–153.e6. [Google Scholar] [CrossRef]
- Haseebuddin, M.; Benway, B.M.; Cabello, J.M.; Bhayani, S.B. Robot- assisted partial nephrectomy: Evaluation of learning curve for an experienced renal surgeon. J. Endourol. 2010, 24, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Ingels, A.; Duc, S.; Bensalah, K.; Bigot, P.; Paparel, P.; Beauval, J.B.; Salomon, L.; De La Taille, A.; Lang, H.; Nouhaud, F.X.; et al. Postoperative outcomes of elderly patients undergo-ing partial nephrectomy. Sci. Rep. 2021, 11, 17201. [Google Scholar] [CrossRef]
- Webb, C.M.; Kamel, M.; Eltahawy, E.; Faramawi, M.F.; Shera, A.L.; Davis, R.; Bissada, N.; Jadhav, S. A comparative study of open, laparoscopic and robotic partial ne-phrectomy in obese patients. Urol Ann. 2015, 7, 231–234. [Google Scholar] [PubMed]
- Porpiglia, F.; Mari, A.; Bertolo, R.; Antonelli, A.; Bianchi, G.; Fidanza, F.; Fiori, C.; Furlan, M.; Morgia, G.; Novara, G.; et al. Partial Nephrectomy in Clinical T1b Renal Tumors: Multi-center Comparative Study of Open, Laparoscopic and Robot-assisted Approach (the RECORd Project). Urology 2016, 89, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Kızılay, F.; Turna, B.; Apaydın, E.; Semerci, B. Comparison of long-term outcomes of laparoscopic and robot-assisted laparoscopic partial ne-phrectomy. Kaohsiung J. Med. Sci. 2019, 35, 238–243. [Google Scholar] [CrossRef]
- Würnschimmel, C.; Di Pierro, G.B.; Moschini, M.; Grande, P.; Baumeister, P.; Roth, M.; Mordasini, L.; Mattei, A. Robot-Assisted Laparoscopic Par-tial Nephrectomy Vs Conventional Laparoscopic Partial Nephrectomy: Func-tional and Surgical Outcomes of a Prospective Single Surgeon Randomized Study. J. Endourol. 2020, 34, 847–855. [Google Scholar] [CrossRef]
- Hinata, N.; Shiroki, R.; Tanabe, K.; Eto, M.; Takenaka, A.; Kawakita, M.; Hara, I.; Hongo, F.; Ibuki, N.; Nasu, Y.; et al. Robot-assisted partial nephrectomy versus standard laparoscopic partial nephrectomy for renal hilar tumor: A pro-spective multi-institutional study. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2021, 28, 382–389. [Google Scholar] [CrossRef]
- Bradshaw, A.W.; Autorino, R.; Simone, G.; Yang, B.; Uzzo, R.G.; Porpiglia, F.; Capi-tanio, U.; Porter, J.; Bertolo, R.; Minervini, A.; et al. Robotic partial nephrectomy vs. minimally invasive radical nephrectomy for clinical T2a renal mass: A pro-pensity score-matched comparison from the ROSULA (Robotic Surgery for Large Renal Mass) Collaborative Group. BJU Int. 2020, 126, 114–123. [Google Scholar] [CrossRef]
- Simone, G.; De Nunzio, C.; Ferriero, M.; Cindolo, L.; Brookman-May, S.; Papalia, R.; Sperduti, I.; Collura, D.; Leonardo, C.; Anceschi, U.; et al. Trends in the use of partial nephrectomy for cT1 renal tumors: Analysis of a 10-yr European multicenter dataset. Eur. J. Surg. Oncol. (EJSO) 2016, 42, 1729–1735. [Google Scholar] [CrossRef]
- Lavallée, L.T.; Desantis, D.; Kamal, F.; Blew, B.; Watterson, J.; Mallick, R.; Breau, R.H. The association between renal tumour scoring systems and ischemia time during open partial nephrectomy. Can. Urol. Assoc. J. 2012, 19, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayn, M.H.; Schwaab, T.; Underwood, W.; Kim, H.L. RENAL nephrometry score predicts surgical outcomes of laparoscopic partial nephrectomy. BJU Int. 2011, 108, 876–881. [Google Scholar] [CrossRef]
- Simone, G.; Capitanio, U.; Tuderti, G.; Presicce, F.; Leonardo, C.; Ferriero, M.; Leonardo, M.; Manuela, C.; Alessandro, L.; Francesco, M.; et al. On-clamp versus off-clamp partial nephrectomy: Propensity score-matched comparison of long-term functional outcomes. Int. J. Urol. 2019, 26, 985–991. [Google Scholar] [CrossRef]
- Bertolo, R.; Simone, G.; Garisto, J.; Nakhoul, G.; Armanyous, S.; Agudelo, J.; Costantini, M.; Tuderti, G.; Gallucci, M.; Kaouk, J. Off-clamp vs on-clamp robotic partial nephrectomy: Perioperative, functional and oncological outcomes from a propensity-score matching between two high-volume centers. Eur. J. Surg. Oncol. 2018, 45, 1232–1237. [Google Scholar] [CrossRef]
- Bylund, J.R.; Gayheart, D.; Fleming, T.; Venkatesh, R.; Preston, D.M.; Strup, S.E.; Crispen, P.L. Association of Tumor Size, Location, R.E.N.A.L., PADUA and Centrality Index Score with Perioperative Outcomes and Postoperative Renal Function. J. Urol. 2012, 188, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Rod, X.; Peyronnet, B.; Seisen, T.; Pradere, B.; Gomez, F.D.; Verhoest, G.; Roupret, M. Impact of ischaemia time on renal func-tion after partial nephrectomy: A systematic review. BJU Int. 2016, 118, 692–705. [Google Scholar] [CrossRef] [Green Version]
- Greco, F.; Autorino, R.; Altieri, V.; Campbell, S.; Ficarra, V.; Gill, I.; Kutikov, A.; Mottrie, A.; Mirone, V.; van Poppel, H. Ischemia techniques in nephron-sparing surgery: A systematic review and meta-analysis of surgical, oncological, and functional outcomes. Eur. Urol. 2019, 75, 477–491. [Google Scholar] [CrossRef]
- Anderson, B.G.; Potretzke, A.M.; Du, K.; Vetter, J.M.; Bergeron, K.; Paradis, A.G.; Figenshau, R.S. Comparing Off-clamp and On-clamp Robot-assisted Partial Nephrectomy: A Prospective Randomized Trial. Urology 2019, 126, 102–109. [Google Scholar] [CrossRef]
- Li, M.; Cheng, L.; Zhang, H.; Ma, L.; Wang, Y.; Niu, W.; Liu, Z.; Song, Y.; Liang, P.; Zhao, G.; et al. Laparoscopic and Robotic-Assisted Partial Nephrectomy: An Overview of Hot Issues. Urol. Int. 2020, 104, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Simone, G.; Tuderti, G.; Anceschi, U.; Ferriero, M.; Costantini, M.; Minisola, F.; Giulio, V.; Giuseppe, P.; Salvatore, G.; Leonardo, M.; et al. “Ride the Green Light”: Indocyanine Green–marked Off-clamp Robotic Partial Nephrectomy for Totally Endophytic Renal Masses. Eur. Urol. 2018, 75, 1008–1014. [Google Scholar] [CrossRef]
- Yang, Y.K.; Hsieh, M.L.; Chen, S.Y.; Liu, C.Y.; Lin, P.H.; Kan, H.C.; Pang, S.T.; Yu, K.J. Clinical Benefits of Indocyanine Green Fluorescence in Robot-Assisted Partial Nephrectomy. Cancers 2022, 14, 3032. [Google Scholar] [CrossRef]
- Brassetti, A.; Cacciamani, G.E.; Mari, A.; Garisto, J.D.; Bertolo, R.; Sundaram, C.P.; Derweesh, I.; Bindayi, A.; Dasgupta, P.; Porter, J.; et al. Off-Clamp Robot-Assisted Partial Nephrectomy for cT2 Renal Tumors: Retrospective Propensity-Score-Matched Multicenter Outcome Analysis. Cancers 2022, 14, 4431. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.D.; Koehne, E.L.; Gali, K.; Lanzotti, N.J.; Rac, G.; Desai, S.; Pahouja, G.; Quek, M.L.; Gupta, G.N. Robotic-assisted tumor enucleation versus stand-ard margin partial nephrectomy: Perioperative, renal functional, and oncologic outcomes for low and intermediate complexity renal masses. Urol. Oncol. 2022, 40, 347.e9–347.e16. [Google Scholar] [CrossRef] [PubMed]
- Bai, N.; Qi, M.; Shan, D.; Liu, S.; Na, T.; Chen, L. Trifecta achieve-ment in patients undergoing partial nephrectomy: A systematic review and meta-analysis of predictive factors. Int. Braz. J. Urol. Off. J. Braz. Soc. Urol. 2022, 48, 625–636. [Google Scholar] [CrossRef]
- Murphy, D.; Challacombe, B.; Khan, M.S.; Dasgupta, P. Robotic technology in urology. Postgrad. Med. J. 2006, 82, 743–747. [Google Scholar] [CrossRef] [Green Version]
- Takahara, K.; Ohno, Y.; Fukaya, K.; Matsukiyo, R.; Nukaya, T.; Takenaka, M.; Zennami, K.; Ichino, M.; Fukami, N.; Sasaki, H.; et al. Novel Intraoperative Navigation Using Ultra-High-Resolution CT in Robot-Assisted Partial Nephrectomy. Cancers 2022, 14, 2047. [Google Scholar] [CrossRef] [PubMed]
- Shirk, J.D.; Thiel, D.D.; Wallen, E.M.; Linehan, J.M.; White, W.M.; Badani, K.K.; Porter, J.R. Effect of 3-Dimensional Virtual Reality Models for Surgical Planning of Robotic-Assisted Partial. JAMA Netw. Open 2019, 2, e1911598. [Google Scholar] [CrossRef]


{kind=link}
| Studies | Level of Evidence | Design | No. of Centers | Recruitment Period | No. Surgeons | Coincidence | Follow-Up (Months) | Quality SCORE (NOS) |
|---|---|---|---|---|---|---|---|---|
| Porpiglia et al., 2015 [10] | 3 | RP | 19 | 2009–2012 | Multiple | 1, 2, 3, 4, 5, 6, 7, 10, 11, 12, 13, 14, 15, 16, 17, 19, 20, 21 | 3 | 8 |
| Webb et al., 2015 [14] | 3 | R | 1 | 2005–2011 | Multiple | 1, 2, 5, 6, 7, 10, 11, 12 | Perioperative | 7 |
| Kizilay et al., 2019 [15] | 3 | R | 1 | 2012–2018 | N/A | 1, 2, 3, 5, 6, 7, 9, 11, 12, 13, 14, 15, 16, 17, 18, 19, 21, 22 | 60 | 8 |
| Zaid et al., 2017 [16] | 3 | R | 1 | 2001–2012 | N/A | 1, 2, 3, 4, 5, 6, 7, 17, 19 | 1 | 6 |
| Ingels et al., 2021 [11] | 3 | RP | 15 | 2000–2016 | Multiple | 1, 2, 3, 4, 5, 6, 7, 8, 9.10, 11, 12, 13, 14, 15, 16, 19 | 3 | 8 |
| Würnschimmel et al., 2020 [13] | 2 | PRA | 1 | 2015–2019 | 1 | 1, 2, 3, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18 | 6 | 8 |
| Haseebuddin et al., 2010 [17] | 3 | R | 1 | 2007–2008 | 1 | 1, 7, 12, 13, 14, 16, 18 | Perioperative | 5 |
| Hinata et al., 2020 [12] | 2 | PRA | 22 | N/A | Multiple | 1, 2, 3, 6, 7, 9, 11, 12, 13, 14, 15, 17, 19 | 24 | 7 |
| Studies | N | OPN | LPN | RAPN | Sex | Average age (Years) Total OPN LPN RAPN | BMI (Kg/m2) OPN LPN RAPN | ECOG ≥1 (%) Total OPN LPN RAPN | LATERALITY Predominant Total OPN LPN RAPN | DIAMETER Total OPN LPN RAPN | LOCATION Predominant OPN LPN RAPN | GROWTH PATTERN Predominant OPN LPN RAPN | Hb before OPN LPN RAPN | Cr before (mg/dL) OPN LPN RAPN | EGFR before (ml/min/m2) Total OPN LPN RAPN | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M (%) Total OPN LPN RAPN | F (%) Total OPN LPN RAPN | |||||||||||||||
| Porpiglia et al., 2015 [10] | 285 | 133 | 57 | 95 | - 65.4 73.7 44.2 | - 34.6 26.3 55.8 | - 62.5 60 57.3 | - 26 25.6 25.8 | - 30.8 24.6 11.6 | - Right Right Right | - 5 5 5 | Superior Polar Mesorrenal Lower polar | Exophytic Exophytic Exofitico | 14 14 14 | 0.9 1 1 | - 87 86 |
| Webb et al., 2015 [14] | 66 | 21 | 31 | 14 | - 66.67 59.38 42.86 | - 33.3 46.62 57.14 | - 53.6 55.53 605 | - Left Left Same | - 4.22 2.7 2.9 | Exophytic Exophytic Exophytic | 0.95 0.9 0.8 | |||||
| Kizilay et al., 2019 [15] | 142 | - | 71 | 71 | - - 52.2 56.4 | - - 47.8 43.6 | - - 54.6 52.9 | - 23.8 24.5 | - - Left Right | - - 2.79 2.48 | - Exophytic Exophytic | - 0.88 0.92 | - - 84.9 82.6 | |||
| Zaid et al., 2017 [16] | 1773 | 1407 | 196 | 170 | 63 | 37 | 61 | 8 | ||||||||
| Ingels et al., 2021 [11] | 191 | 69 | 17 | 105 | 61.3 | 78.4 | 41.3 | 4.7 | 72.7 | |||||||
| Würnschimmel et al., 2020 [13] | 115 | - | 54 | 61 | - - 39 40 | - - 15 21 | - - 63.9 62.7 | - 28.5 29.5 | - Right Left | - 3.5 4.5 | - - 78.8 80.4 | |||||
| Haseebuddin et al., 2010 [17] | 38 | 38 | - - - 62 | - - - 3.3 (>2 cm) and 1.25 (<2 cm) | ||||||||||||
| Hinata et al., 2020 [12] | 105 | 105 | - - - 22 | - - - 62.6 | - - - 29.2 | - - - 3.2 | Hiliar | Endophytic | - - - 0.88 | - - - 69 | ||||||
| Studies | Total Operating Time (min) Total OPN LPN RAPN | Warm Ischemia Time (min) Total OPN LPN RAPN | Surgical Margins Positive (%) Total OPN LPN RAPN | Hospital Stay (days) Total OPN LPN RAPN | Blood Loss (cc) Total OPN LPN RAPN | Postoperative EGFR Difference Total OPN LPN RAPN | Death Total OPN LPN RAPN | Complications Postoperative (%) Total OPN LPN RAPN | Metastasis-Free Survival % Total OPN LPN RAPN | Recurrence-Free Survival (at 5 years) % Total OPN LPN RAPN |
|---|---|---|---|---|---|---|---|---|---|---|
| Porpiglia et al., 2015 [10] | - 135 129 155 | - 16 24 18 | - 6.8 1.9 2.5 | - | - 200 200 150 | - 8.7 7.3 1.6 | - 12.8 1.8 2.1 | |||
| Webb et al., 2015 [14] | - - 158 210 | - 30.69 24.07 28.01 | - 4 2 3 | - 300 100 150 | - 0 4.5 0 | |||||
| Kizilay et al., 2019 [15] | - - 158 176 | - - 24.39 18.81 | - - 3 2 | - - 3.5 3.2 | - - 240 210 | - - 12.39 11.38 | - - 68 69 | - - 61 64 | ||
| Zaid et al., 2017 [16] | 51 | 4 | 200 | 0.1 | 6.7 | |||||
| Ingels et al., 2021132021 [11] | 150 | 200 | 17 | |||||||
| Würnschimmel et al., 2020 [13] | - - 192.3 230.2 | - - 21.1 19.6 | - - 0 5 | - - 6.3 6.1 | - - 14 16 | - - 31 21 | ||||
| Haseebuddin et al., 2010 [17] | - - - 131.9 (<2 cm) 145.8 (>2 cm) | - - - 21 (<2 cm) 24.7 (>2 cm) | 2.5 | - - - 130.9 (<2 cm) 136.4 (>2 cm) | 13 | |||||
| Hinata et al., 2020 [12] | - - - 146 | - - - 20.2 | - - - 1.9 | - - - | - - - 138.6 | - - - 0.19 | - - - 63.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz Guerrero, E.; Claro, A.V.O.; Ledo Cepero, M.J.; Soto Delgado, M.; Álvarez-Ossorio Fernández, J.L. Robotic versus Laparoscopic Partial Nephrectomy in the New Era: Systematic Review. Cancers 2023, 15, 1793. https://doi.org/10.3390/cancers15061793
Ruiz Guerrero E, Claro AVO, Ledo Cepero MJ, Soto Delgado M, Álvarez-Ossorio Fernández JL. Robotic versus Laparoscopic Partial Nephrectomy in the New Era: Systematic Review. Cancers. 2023; 15(6):1793. https://doi.org/10.3390/cancers15061793
Chicago/Turabian StyleRuiz Guerrero, Estefanía, Ana Victoria Ojeda Claro, María José Ledo Cepero, Manuel Soto Delgado, and José Luis Álvarez-Ossorio Fernández. 2023. "Robotic versus Laparoscopic Partial Nephrectomy in the New Era: Systematic Review" Cancers 15, no. 6: 1793. https://doi.org/10.3390/cancers15061793