
Emerging Indications for Interventional Oncology: Expert Discussion on New Locoregional Treatments
 , , , , ,
, , , , ,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Spine, Skull, and Skull Base Tumors
2.1. Spinal Tumors
2.2. Desmoid Tumors
2.3. Ear, Nose, and Throat (ENT) Tumors
2.4. Intrasinusal Frontal Hemangioma
2.5. Palatine Nasopharyngeal Carcinoma
2.6. Glioblastoma
3. Deep Spaces of the Neck
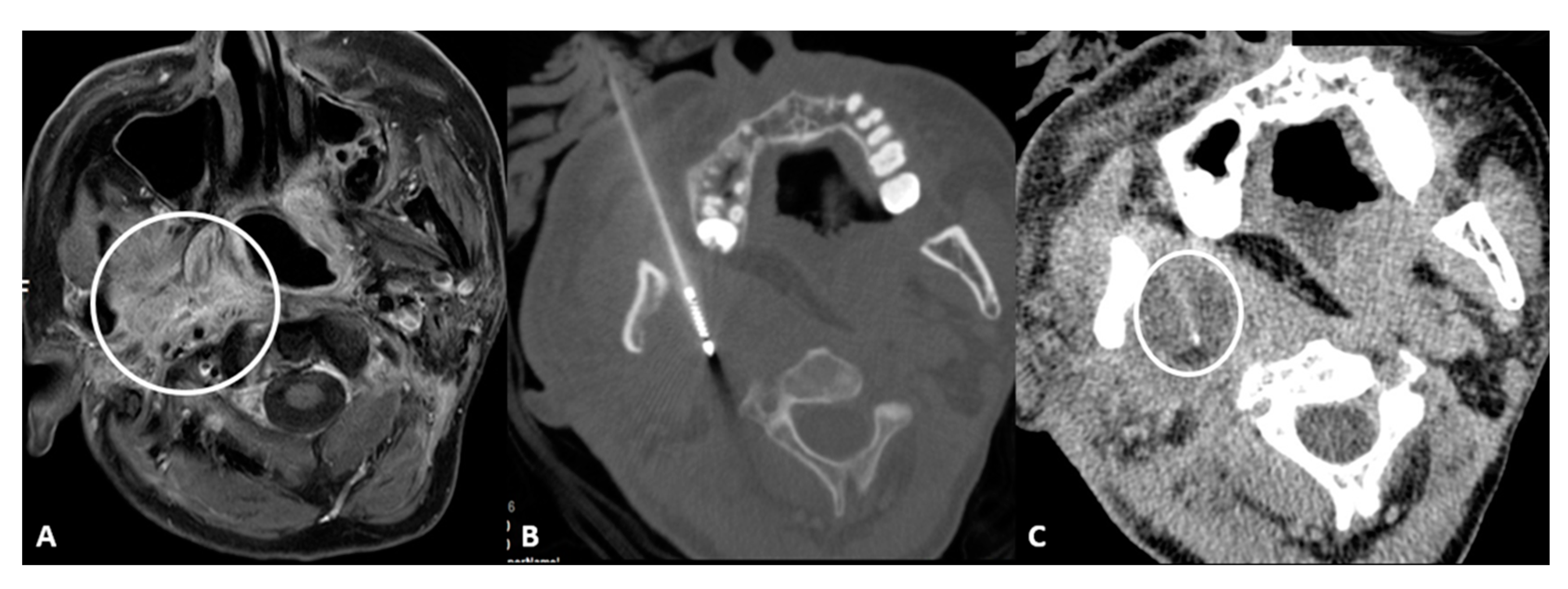
- Retromaxillary: In the case of a retromaxillary approach, the maxilla is used as a landmark. This approach is mostly used for lesions located in the masticatory space and the pharyngeal and laryngeal mucosa (Figure 1).

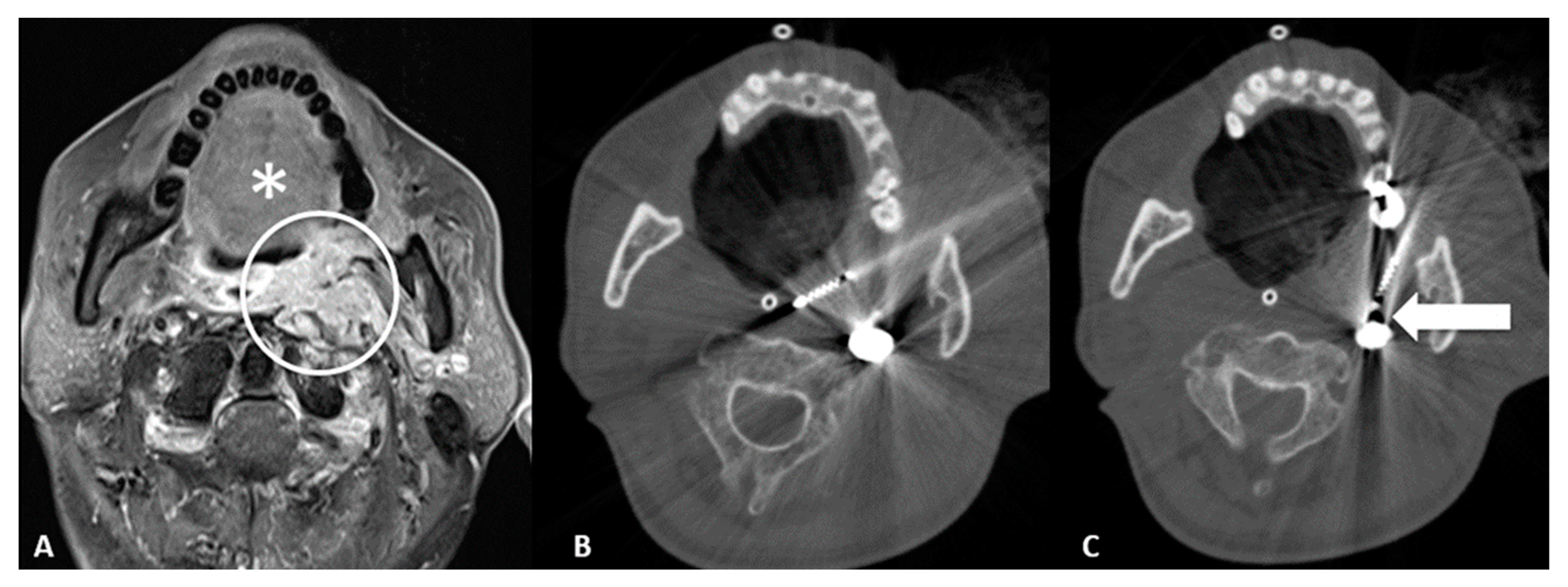
- Retromolar trigone: This is the space between the last molar and the mandibular condyle. It is a space without many vessels/nerves or vital structures; therefore, it represents a safe approach to treating pharyngeal and laryngeal lesions. Tongue positioning is mandatory, as it can flop backward against the ablation site resulting in frost injury: Forceps and a laryngoscope should be used to displace the tongue with gauze away from the ablation site to avoid this occurrence. In the case of tumors near the carotid artery, the patient can manifest severe hypotension and bradycardia during ablation. The presence of coils or metallic devices in a previously embolized carotid artery leads both to a loss of the cold-sink effect as well as a stimulation of the vagus nerve with thermal conduction down the carotid body (leading to the diving reflex). Cessation of cryoablation usually leads to spontaneous resolution (Figure 2).

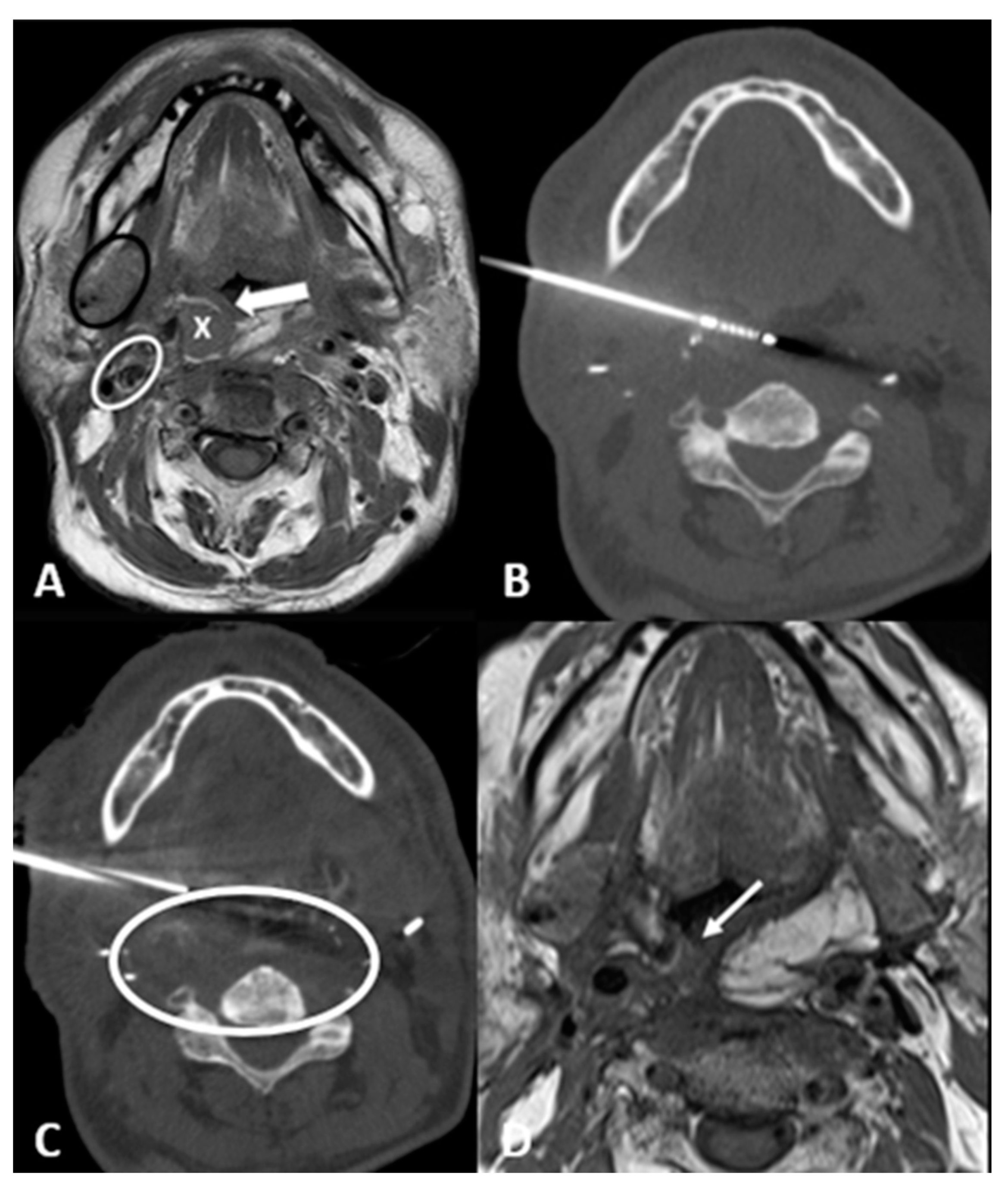
- Transglandular: This is a very useful approach in case of lesions in the pharyngeal space and prevertebral space, crossing the submandibular gland to reach these locations (Figure 3).

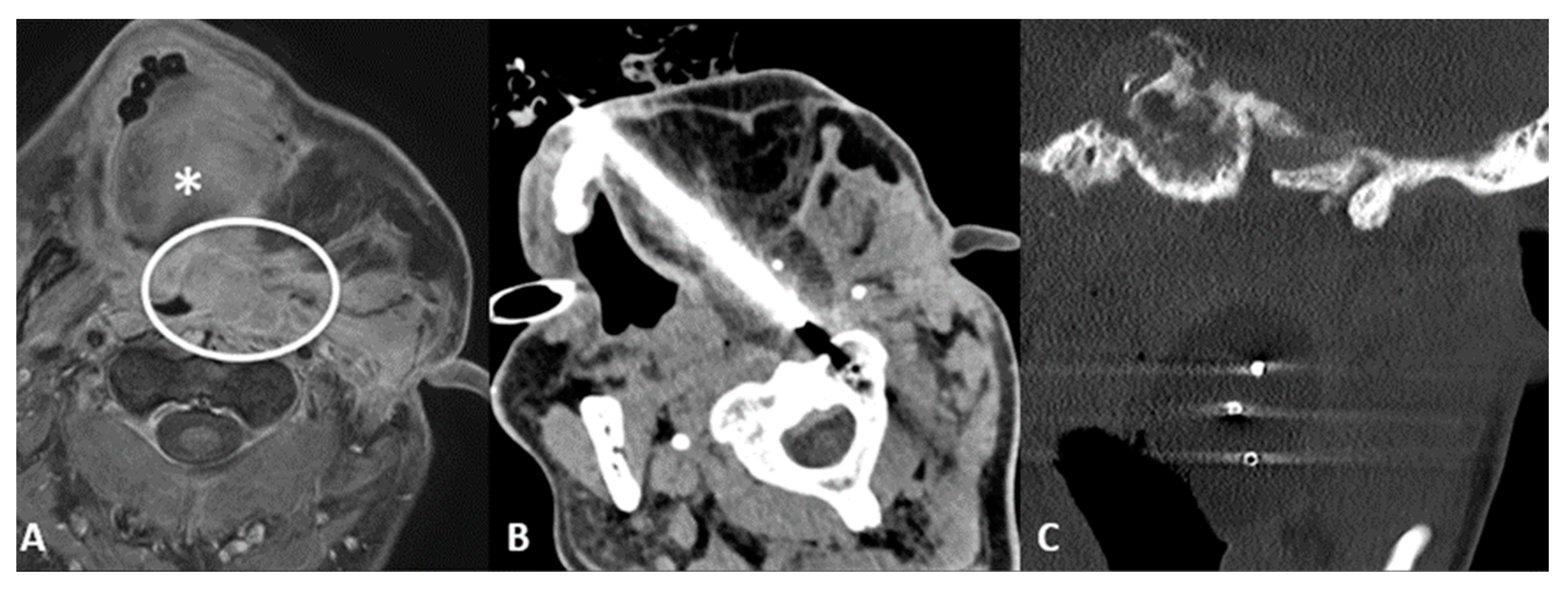
- Transflap: Useful in the case of early local tumor recurrence, in patients who underwent previous surgery, and myocutaneous flap reconstruction (Figure 4). The myocutaneous flap is usually devoid of significant vascularity and vital structures and presents a safe trajectory once it has been grafted [13].

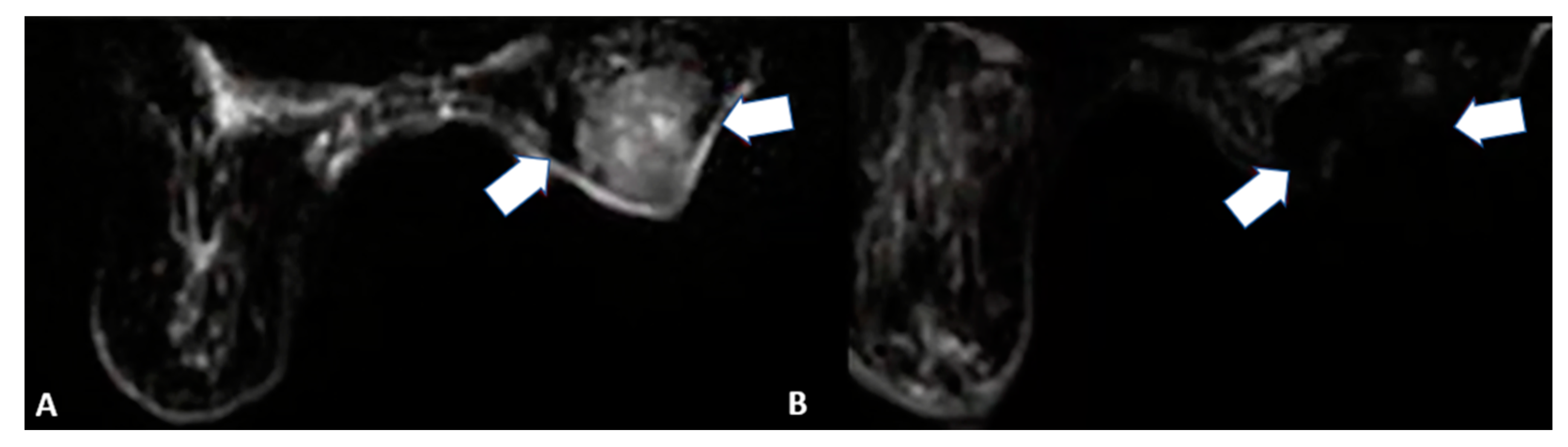
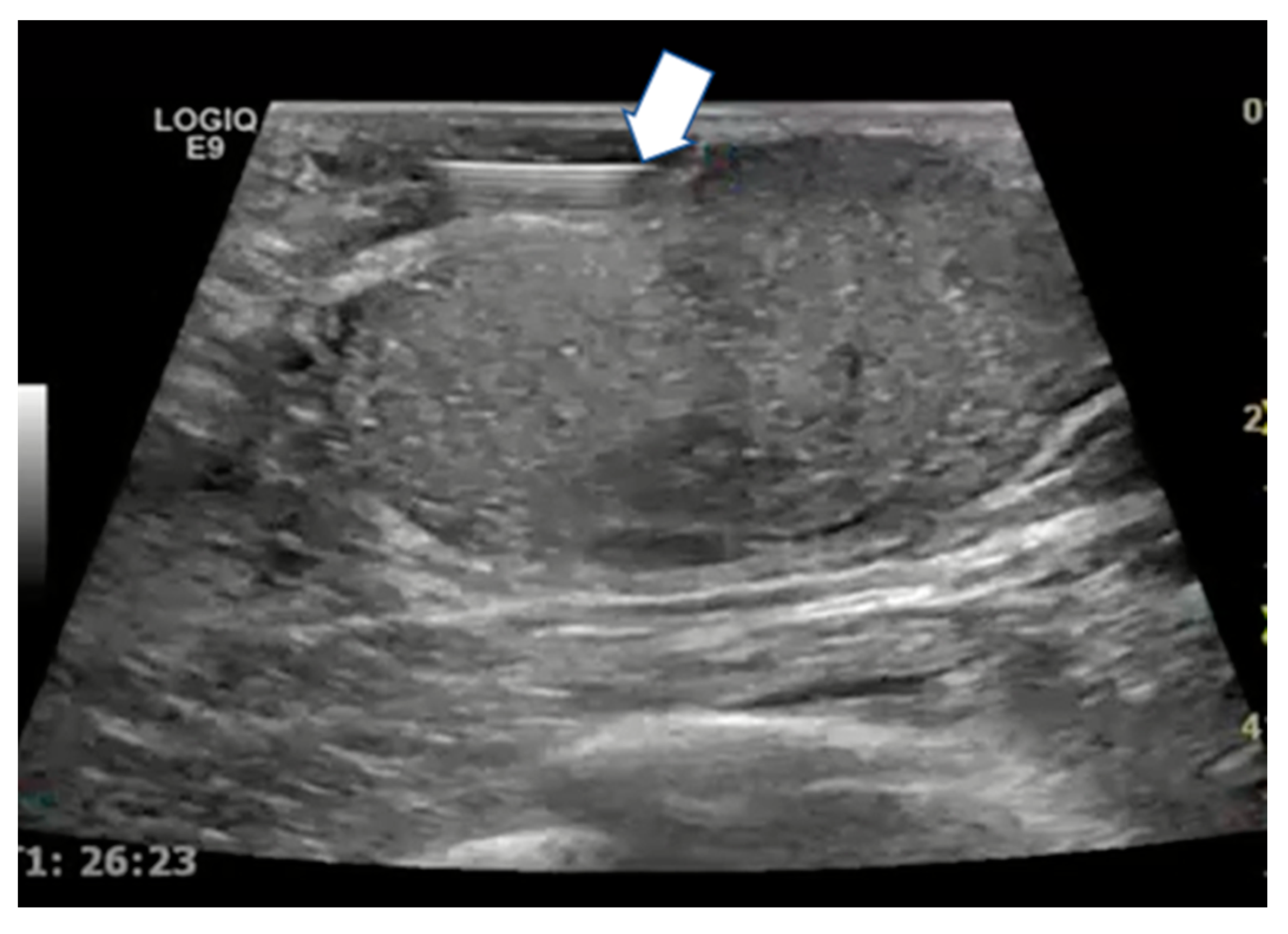
4. Breast Cancer
4.1. Locoregional Approaches
4.2. Key Points
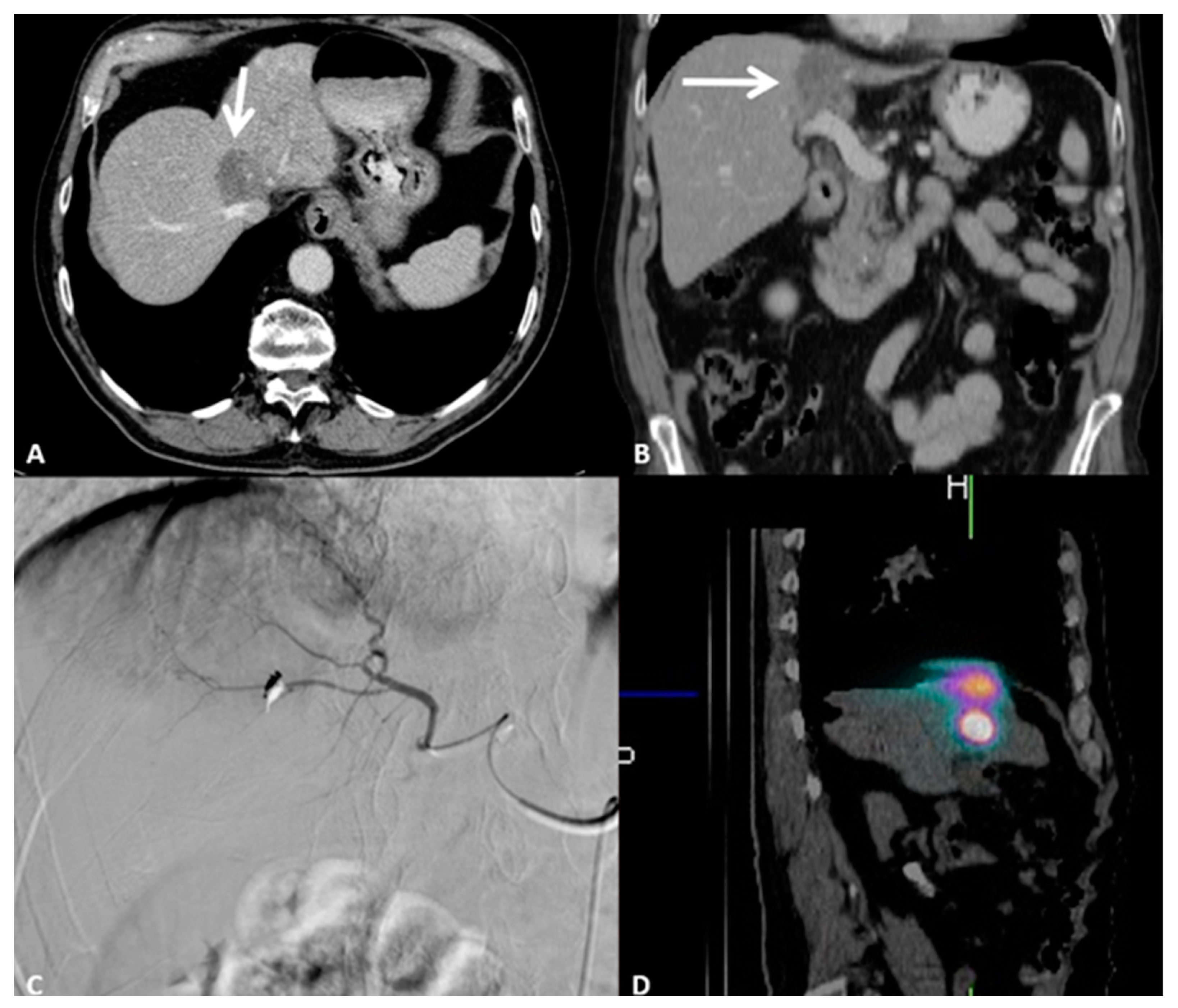
5. Intrahepatic Cholangiocellular Carcinoma
5.1. Locoregional Approaches
5.2. Key Points
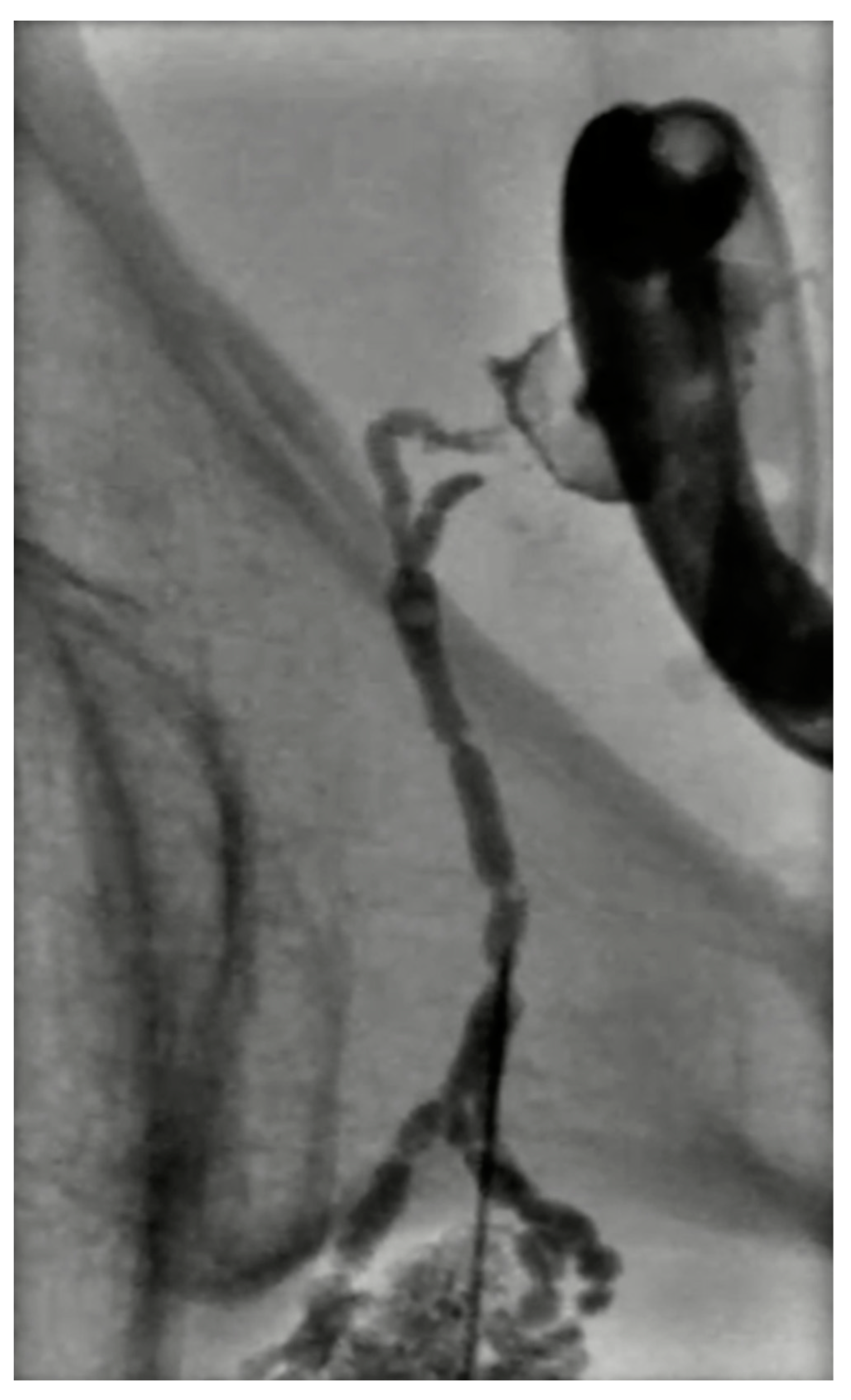
6. Lymphatics and Lymph Node Metastases
Locoregional Approaches
7. Bone Metastases
7.1. Locoregional Approaches
7.2. Key Points
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Helmberger, T. The evolution of interventional oncology in the 21st century. Br. J. Radiol. 2020, 93, 20200112. [Google Scholar] [CrossRef]
- Wilseck, Z.M.; Lin, L.; Gemmete, J.J.; Pandey, A.S.; Srinivasan, A.; Chaudhary, N. Skull Base Neurointerventional Techniques. Neuroimaging Clin. 2021, 31, 649–664. [Google Scholar] [CrossRef] [PubMed]
- Sagoo, N.S.; Haider, A.S.; Chen, A.L.; Vannabouathong, C.; Larsen, K.; Sharma, R.; Palmisciano, P.; Alamer, O.B.; Igbinigie, M.; Wells, D.B.; et al. Radiofrequency ablation for spinal osteoid osteoma: A systematic review of safety and treatment outcomes. Surg. Oncol. 2022, 41, 101747. [Google Scholar] [CrossRef]
- Koch, G.; Cazzato, R.L.; Gilkison, A.; Caudrelier, J.; Garnon, J.; Gangi, A. Percutaneous Treatments of Benign Bone Tumors. Semin. Interv. Radiol. 2018, 35, 324–332. [Google Scholar] [CrossRef]
- Auloge, P.; Garnon, J.; Robinson, J.M.; Thenint, M.A.; Koch, G.; Caudrelier, J.; Weiss, J.; Cazzato, R.L.; Kurtz, J.E.; Gangi, A. Percutaneous cryoablation for advanced and refractory extra-abdominal desmoid tumors. Int. J. Clin. Oncol. 2021, 26, 1147–1158. [Google Scholar] [CrossRef]
- Hashim, D.; Genden, E.; Posner, M.; Hashibe, M.; Boffetta, P. Head and neck cancer prevention: From primary prevention to impact of clinicians on reducing burden. Ann. Oncol. 2019, 30, 744–756. [Google Scholar] [CrossRef] [Green Version]
- Harar, R.P.; Wolfe, K.Q.; Kumar, S.; Gatland, D.J. Haemangioma of the frontal sinus. J. Laryngol. Otol. 2002, 116, 296–298. [Google Scholar] [CrossRef]
- Gangi, A.; Cebula, H.; Cazzato, R.L.; Ramamurthy, N.; Garnon, J.; Debry, C.; Proust, F. “Keeping a Cool Head”: Percutaneous Imaging-Guided Cryo-ablation as Salvage Therapy for Recurrent Glioblastoma and Head and Neck Tumours. Cardiovasc. Interv. Radiol. 2020, 43, 172–175. [Google Scholar] [CrossRef]
- Brook, A.L.; Gold, M.M.; Miller, T.S.; Gold, T.; Owen, R.P.; Sanchez, L.S.; Farinhas, J.M.; Shifteh, K.; Bello, J.A. CT-guided radiofrequency ablation in the palliative treatment of recurrent advanced head and neck malignancies. J. Vasc. Interv. Radiol. 2008, 19, 725–735. [Google Scholar] [CrossRef]
- Chokkappan, K.; Lim, M.Y.; Loke, S.C.; Karandikar, A.; Pua, U. Salvage Cryoablation of Recurrent Squamous Cell Carcinoma for Impending Airway Obstruction with Abscopal Effect. J. Vasc. Interv. Radiol. 2020, 31, 1939–1942. [Google Scholar] [CrossRef]
- Guenette, J.P.; Tuncali, K.; Himes, N.; Shyn, P.B.; Lee, T.C. Percutaneous Image-Guided Cryoablation of Head and Neck Tumors for Local Control, Preservation of Functional Status, and Pain Relief. AJR Am. J. Roentgenol. 2017, 208, 453–458. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.K.; Baek, J.H.; Lee, J.H.; Kim, W.B.; Kim, T.Y.; Shong, Y.K.; Hong, S.J. Efficacy and safety of radiofrequency ablation for treating locoregional recurrence from papillary thyroid cancer. Eur. Radiol. 2015, 25, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Quek, L.H.H.; Lim, M.Y.; Cheo, T.; Teo, H.L.; Pua, U. Percutaneous Management of Recurrent Head and Neck Cancer: Current Role and Evolving Principles in the Multidisciplinary Setting. Curr. Oncol. Rep. 2021, 23, 52. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Lei, S.; Zheng, R.; Zhang, S.; Wang, S.; Chen, R.; Sun, K.; Zeng, H.; Zhou, J.; Wei, W. Global patterns of breast cancer incidence and mortality: A population-based cancer registry data analysis from 2000 to 2020. Cancer Commun. 2021, 41, 1183–1194. [Google Scholar] [CrossRef]
- Lovelace, D.L.; McDaniel, L.R.; Golden, D. Long-Term Effects of Breast Cancer Surgery, Treatment, and Survivor Care. J. Midwifery Women’s Health 2019, 64, 713–724. [Google Scholar] [CrossRef]
- Bajaj, A.K.; Kon, P.S.; Oberg, K.C.; Miles, D.A. Aesthetic outcomes in patients undergoing breast conservation therapy for the treatment of localized breast cancer. Plast. Reconstr. Surg. 2004, 114, 1442–1449. [Google Scholar] [CrossRef]
- Wang, L.; Xu, J.; Yu, J.; Liang, P. Review of clinical tumor ablation advance in Asia. Int. J. Hyperth. 2021, 38, 1639–1649. [Google Scholar] [CrossRef]
- Yang, Q.; Li, H.; Chen, B.H.; He, G.Z.; Wu, X.P.; Wang, L.X.; Wu, H.; Dou, J.P.; Han, Z.Y.; Zhang, J.; et al. Ultrasound-guided percutaneous microwave ablation for 755 benign breast lesions: A prospective multicenter study. Eur. Radiol. 2020, 30, 5029–5038. [Google Scholar] [CrossRef]
- Yu, J.; Liang, P.; Yu, X.; Liu, F.; Chen, L.; Wang, Y. A comparison of microwave ablation and bipolar radiofrequency ablation both with an internally cooled probe: Results in ex vivo and in vivo porcine livers. Eur. J. Radiol. 2011, 79, 124–130. [Google Scholar] [CrossRef]
- Yu, J.; Han, Z.Y.; Li, T.; Feng, W.Z.; Yu, X.L.; Luo, Y.C.; Wu, H.; Jiang, J.; Wang, J.D.; Liang, P. Microwave Ablation Versus Nipple Sparing Mastectomy for Breast Cancer ≤ 5 cm: A Pilot Cohort Study. Front. Oncol. 2020, 10, 546883. [Google Scholar] [CrossRef]
- Cui, R.; Wu, H.; Xu, J.; Han, Z.; Zhang, J.; Li, Q.; Dou, J.; Yu, J.; Liang, P. Volume reduction for ≥ 2 cm benign breast lesions after ultrasound-guided microwave ablation with a minimum 12-month follow-up. Int. J. Hyperth. 2021, 38, 341–348. [Google Scholar] [CrossRef]
- Yu, J.; Chen, B.H.; Zhang, J.; Han, Z.Y.; Wu, H.; Huang, Y.; Mu, M.J.; Liang, P. Ultrasound guided percutaneous microwave ablation of benign breast lesions. Oncotarget 2017, 8, 79376–79386. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Wu, H.; Han, Z.; Zhang, J.; Li, Q.; Dou, J.; An, C.; Qi, E.; Yu, J.; Liang, P. Microwave ablation of benign breast tumors: A prospective study with minimum 12 months follow-up. Int. J. Hyperth. 2018, 35, 253–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhamija, E.; Singh, R.; Mishra, S.; Hari, S. Image-Guided Breast Interventions: Biopsy and Beyond. Indian J. Radiol. Imaging 2021, 31, 391–399. [Google Scholar] [CrossRef]
- Leylek, A.M.; Whitman, G.J.; Vilar, V.S.; Kisilevzky, N.; Faintuch, S. Radiofrequency ablation for breast cancer. Tech. Vasc. Interv. Radiol. 2013, 16, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Zha, X.; Liu, X.; Ding, Q.; Chen, L.; Ni, Y.; Zhang, Y.; Xu, Y.; Chen, L.; Zhao, Y.; et al. US-guided percutaneous microwave coagulation of small breast cancers: A clinical study. Radiology 2012, 263, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavros, M.N.; Economopoulos, K.P.; Alexiou, V.G.; Pawlik, T.M. Treatment and Prognosis for Patients With Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-analysis. JAMA Surg. 2014, 149, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Spolverato, G.; Kim, Y.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Clark Gamblin, T.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; et al. Management and Outcomes of Patients with Recurrent Intrahepatic Cholangiocarcinoma Following Previous Curative-Intent Surgical Resection. Ann. Surg. Oncol. 2016, 23, 235–243. [Google Scholar] [CrossRef]
- Wu, L.; Tsilimigras, D.I.; Paredes, A.Z.; Mehta, R.; Hyer, J.M.; Merath, K.; Sahara, K.; Bagante, F.; Beal, E.W.; Shen, F.; et al. Trends in the Incidence, Treatment and Outcomes of Patients with Intrahepatic Cholangiocarcinoma in the USA: Facility Type is Associated with Margin Status, Use of Lymphadenectomy and Overall Survival. World J. Surg. 2019, 43, 1777–1787. [Google Scholar] [CrossRef] [PubMed]
- Petrick, J.L.; Braunlin, M.; Laversanne, M.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in liver cancer incidence, overall and by histologic subtype, 1978-2007. Int. J. Cancer 2016, 139, 1534–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosconi, C.; Calandri, M.; Javle, M.; Odisio, B.C. Interventional radiology approaches for intra-hepatic cholangiocarcinoma. Chin. Clin. Oncol. 2020, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, R.; Acquafredda, F.; Ferraro, V.; Laera, L.; Surico, G.; Surgo, A.; Fiorentino, A.; Marini, S.; de’Angelis, N.; Memeo, R.; et al. Non-surgical treatment of hilar cholangiocarcinoma. World J. Gastrointest. Oncol. 2021, 13, 1696–1708. [Google Scholar] [CrossRef]
- Lucatelli, P.; Argirò, R.; Crocetti, L.; Rocco, B.; Bozzi, E.; Gasparrini, F.; Tanzilli, A.; Catalano, C.; Iezzi, R. Percutaneous Thermal Segmentectomy: Proof of Concept. Cardiovasc. Interv. Radiol. 2022, 45, 665–676. [Google Scholar] [CrossRef]
- Yousaf, A.; Kim, J.U.; Eliahoo, J.; Taylor-Robinson, S.D.; Khan, S.A. Ablative Therapy for Unresectable Intrahepatic Cholangiocarcinoma: A Systematic Review and Meta-Analysis. J. Clin. Exp. Hepatol. 2019, 9, 740–748. [Google Scholar] [CrossRef] [Green Version]
- Shindoh, J. Ablative therapies for intrahepatic cholangiocarcinoma. Hepatobiliary Surg. Nutr. 2017, 6, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Benson, A.B.; D’Angelica, M.I.; Abbott, D.E.; Anaya, D.A.; Anders, R.; Are, C.; Bachini, M.; Borad, M.; Brown, D.; Burgoyne, A.; et al. Hepatobiliary Cancers, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021, 19, 541–565. [Google Scholar] [CrossRef]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Han, K.; Ko, H.K.; Kim, K.W.; Won, H.J.; Shin, Y.M.; Kim, P.N. Radiofrequency ablation in the treatment of unresectable intrahepatic cholangiocarcinoma: Systematic review and meta-analysis. J. Vasc. Interv. Radiol. 2015, 26, 943–948. [Google Scholar] [CrossRef]
- Butros, S.R.; Shenoy-Bhangle, A.; Mueller, P.R.; Arellano, R.S. Radiofrequency ablation of intrahepatic cholangiocarcinoma: Feasability, local tumor control, and long-term outcome. Clin. Imaging 2014, 38, 490–494. [Google Scholar] [CrossRef]
- Rhim, H.; Dodd, G.D., 3rd; Chintapalli, K.N.; Wood, B.J.; Dupuy, D.E.; Hvizda, J.L.; Sewell, P.E.; Goldberg, S.N. Radiofrequency thermal ablation of abdominal tumors: Lessons learned from complications. Radiographics 2004, 24, 41–52. [Google Scholar] [CrossRef]
- McDermott, S.; Gervais, D.A. Radiofrequency ablation of liver tumors. Semin. Interv. Radiol. 2013, 30, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.; Brace, C.L.; Lee, F.T., Jr.; Goldberg, S.N. Principles of and advances in percutaneous ablation. Radiology 2011, 258, 351–369. [Google Scholar] [CrossRef]
- Slakey, D.P. Radiofrequency ablation of recurrent cholangiocarcinoma. Am. Surg. 2002, 68, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.A.; Liang, P.; Yu, X.L.; Cheng, Z.G.; Han, Z.Y.; Liu, F.Y.; Yu, J. Sonography-guided percutaneous microwave ablation of intrahepatic primary cholangiocarcinoma. Eur. J. Radiol. 2011, 80, 548–552. [Google Scholar] [CrossRef]
- Wright, A.S.; Sampson, L.A.; Warner, T.F.; Mahvi, D.M.; Lee, F.T., Jr. Radiofrequency versus microwave ablation in a hepatic porcine model. Radiology 2005, 236, 132–139. [Google Scholar] [CrossRef]
- Takahashi, E.A.; Kinsman, K.A.; Schmit, G.D.; Atwell, T.D.; Schmitz, J.J.; Welch, B.T.; Callstrom, M.R.; Geske, J.R.; Kurup, A.N. Thermal ablation of intrahepatic cholangiocarcinoma: Safety, efficacy, and factors affecting local tumor progression. Abdom. Radiol. 2018, 43, 3487–3492. [Google Scholar] [CrossRef]
- Kim, J.H.; Won, H.J.; Shin, Y.M.; Kim, K.A.; Kim, P.N. Radiofrequency ablation for the treatment of primary intrahepatic cholangiocarcinoma. AJR Am. J. Roentgenol. 2011, 196, W205–W209. [Google Scholar] [CrossRef]
- Carrafiello, G.; Laganà, D.; Cotta, E.; Mangini, M.; Fontana, F.; Bandiera, F.; Fugazzola, C. Radiofrequency ablation of intrahepatic cholangiocarcinoma: Preliminary experience. Cardiovasc. Interv. Radiol. 2010, 33, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Chiou, Y.Y.; Hwang, J.I.; Chou, Y.H.; Wang, H.K.; Chiang, J.H.; Chang, C.Y. Percutaneous ultrasound-guided radiofrequency ablation of intrahepatic cholangiocarcinoma. Kaohsiung J. Med. Sci. 2005, 21, 304–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercolani, G.; Vetrone, G.; Grazi, G.L.; Aramaki, O.; Cescon, M.; Ravaioli, M.; Serra, C.; Brandi, G.; Pinna, A.D. Intrahepatic cholangiocarcinoma: Primary liver resection and aggressive multimodal treatment of recurrence significantly prolong survival. Ann. Surg. 2010, 252, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.J.; Hu, P.; Wang, N.; Shen, Q.; Sun, A.X.; Kuang, M.; Qian, G.J. Thermal ablation versus repeated hepatic resection for recurrent intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2013, 20, 3596–3602. [Google Scholar] [CrossRef] [PubMed]
- Kishore, S.; Friedman, T.; Madoff, D.C. Update on Embolization Therapies for Hepatocellular Carcinoma. Curr. Oncol. Rep. 2017, 19, 40. [Google Scholar] [CrossRef]
- Koay, E.J.; Odisio, B.C.; Javle, M.; Vauthey, J.N.; Crane, C.H. Management of unresectable intrahepatic cholangiocarcinoma: How do we decide among the various liver-directed treatments? Hepatobiliary Surg. Nutr. 2017, 6, 105–116. [Google Scholar] [CrossRef] [Green Version]
- Vogl, T.J.; Naguib, N.N.; Nour-Eldin, N.E.; Bechstein, W.O.; Zeuzem, S.; Trojan, J.; Gruber-Rouh, T. Transarterial chemoembolization in the treatment of patients with unresectable cholangiocarcinoma: Results and prognostic factors governing treatment success. Int. J. Cancer 2012, 131, 733–740. [Google Scholar] [CrossRef]
- Stein, S.I.; Madoff, D.C. Balloon-Assisted Transarterial Chemoembolization Segmentectomy: An Alternative Strategy in the Treatment of Hypovascular Oligometastatic Liver Metastases. J. Vasc. Interv. Radiol. 2019, 30, 1143–1145. [Google Scholar] [CrossRef]
- Gyves, J.W.; Ziessman, H.A.; Ensminger, W.D.; Thrall, J.H.; Niederhuber, J.E.; Keyes, J.W., Jr.; Walker, S. Definition of hepatic tumor microcirculation by single photon emission computerized tomography (SPECT). J. Nucl. Med. 1984, 25, 972–977. [Google Scholar]
- Bierman, H.R.; Kelly, K.H.; Dod, K.S.; Byron, R.L., Jr. Studies on the blood supply of tumors in man. I. Fluorescence of cutaneous lesions. J. Natl. Cancer Inst. 1951, 11, 877–889. [Google Scholar]
- Poggi, G.; Amatu, A.; Montagna, B.; Quaretti, P.; Minoia, C.; Sottani, C.; Villani, L.; Tagliaferri, B.; Sottotetti, F.; Rossi, O.; et al. OEM-TACE: A new therapeutic approach in unresectable intrahepatic cholangiocarcinoma. Cardiovasc. Interv. Radiol. 2009, 32, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Rafi, S.; Piduru, S.M.; El-Rayes, B.; Kauh, J.S.; Kooby, D.A.; Sarmiento, J.M.; Kim, H.S. Yttrium-90 radioembolization for unresectable standard-chemorefractory intrahepatic cholangiocarcinoma: Survival, efficacy, and safety study. Cardiovasc. Interv. Radiol. 2013, 36, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Akinwande, O.; Shah, V.; Mills, A.; Noda, C.; Weiner, E.; Foltz, G.; Saad, N. Chemoembolization versus radioembolization for the treatment of unresectable intrahepatic cholangiocarcinoma in a single institution image-based efficacy and comparative toxicity. Hepat. Oncol. 2017, 4, 75–81. [Google Scholar] [CrossRef]
- Mosconi, C.; Solaini, L.; Vara, G.; Brandi, N.; Cappelli, A.; Modestino, F.; Cucchetti, A.; Golfieri, R. Transarterial Chemoembolization and Radioembolization for Unresectable Intrahepatic Cholangiocarcinoma-a Systemic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2021, 44, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Paz-Fumagalli, R.; Frey, G.; Sella, D.M.; McKinney, J.M.; Wang, W. Resin-based Yttrium-90 microspheres for unresectable and failed first-line chemotherapy intrahepatic cholangiocarcinoma: Preliminary results. J. Cancer Res. Clin. Oncol. 2017, 143, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Levillain, H.; Bagni, O.; Deroose, C.M.; Dieudonné, A.; Gnesin, S.; Grosser, O.S.; Kappadath, S.C.; Kennedy, A.; Kokabi, N.; Liu, D.M.; et al. International recommendations for personalised selective internal radiation therapy of primary and metastatic liver diseases with yttrium-90 resin microspheres. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1570–1584. [Google Scholar] [CrossRef]
- Wondergem, M.; Smits, M.L.; Elschot, M.; de Jong, H.W.; Verkooijen, H.M.; van den Bosch, M.A.; Nijsen, J.F.; Lam, M.G. 99mTc-macroaggregated albumin poorly predicts the intrahepatic distribution of 90Y resin microspheres in hepatic radioembolization. J. Nucl. Med. 2013, 54, 1294–1301. [Google Scholar] [CrossRef] [Green Version]
- Willowson, K.P.; Eslick, E.M.; Bailey, D.L. Individualised dosimetry and safety of SIRT for intrahepatic cholangiocarcinoma. EJNMMI Phys. 2021, 8, 65. [Google Scholar] [CrossRef]
- Hosseini Shabanan, S.; Nezami, N.; Abdelsalam, M.E.; Sheth, R.A.; Odisio, B.C.; Mahvash, A.; Habibollahi, P. Selective Internal Radiation Therapy with Yttrium-90 for Intrahepatic Cholangiocarcinoma: A Systematic Review on Post-Treatment Dosimetry and Concomitant Chemotherapy. Curr. Oncol. 2022, 29, 3825–3848. [Google Scholar] [CrossRef]
- Natale, G.; Bocci, G.; Ribatti, D. Scholars and scientists in the history of the lymphatic system. J. Anat. 2017, 231, 417–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shayan, R.; Achen, M.G.; Stacker, S.A. Lymphatic vessels in cancer metastasis: Bridging the gaps. Carcinogenesis 2006, 27, 1729–1738. [Google Scholar] [CrossRef] [PubMed]
- Willard-Mack, C.L. Normal structure, function, and histology of lymph nodes. Toxicol. Pathol. 2006, 34, 409–424. [Google Scholar] [CrossRef]
- Liao, S.; von der Weid, P.Y. Lymphatic system: An active pathway for immune protection. Semin. Cell Dev. Biol. 2015, 38, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guermazi, A.; Brice, P.; Hennequin, C.; Sarfati, E. Lymphography: An old technique retains its usefulness. Radiographics 2003, 23, 1541–1560. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.C.; Krementz, E.T. Lymphangiography by lymph-node injection. JAMA 1967, 202, 1136–1139. [Google Scholar] [CrossRef]
- Nadolski, G.J.; Itkin, M. Feasibility of ultrasound-guided intranodal lymphangiogram for thoracic duct embolization. J. Vasc. Interv. Radiol. 2012, 23, 613–616. [Google Scholar] [CrossRef]
- Gruber-Rouh, T.; Naguib, N.N.N.; Lehnert, T.; Harth, M.; Thalhammer, A.; Beeres, M.; Tsaur, I.; Hammersting, R.; Wichmann, J.L.; Vogl, T.J.; et al. Direct lymphangiography as treatment option of lymphatic leakage: Indications, outcomes and role in patient’s management. Eur. J. Radiol. 2014, 83, 2167–2171. [Google Scholar] [CrossRef]
- Yannes, M.; Shin, D.; McCluskey, K.; Varma, R.; Santos, E. Comparative Analysis of Intranodal Lymphangiography with Percutaneous Intervention for Postsurgical Chylous Effusions. J. Vasc. Interv. Radiol. 2017, 28, 704–711. [Google Scholar] [CrossRef]
- Alejandre-Lafont, E.; Krompiec, C.; Rau, W.S.; Krombach, G.A. Effectiveness of therapeutic lymphography on lymphatic leakage. Acta Radiol. 2011, 52, 305–311. [Google Scholar] [CrossRef]
- Pamarthi, V.; Stecker, M.S.; Schenker, M.P.; Baum, R.A.; Killoran, T.P.; Suzuki Han, A.; O’Horo, S.K.; Rabkin, D.J.; Fan, C.M. Thoracic duct embolization and disruption for treatment of chylous effusions: Experience with 105 patients. J. Vasc. Interv. Radiol. 2014, 25, 1398–1404. [Google Scholar] [CrossRef]
- Kato, S.; Takeda, K.; Sukhbaatar, A.; Sakamoto, M.; Mori, S.; Shiga, K.; Kodama, T. Intranodal pressure of a metastatic lymph node reflects the response to lymphatic drug delivery system. Cancer Sci. 2020, 111, 4232–4241. [Google Scholar] [CrossRef] [PubMed]
- Murthy, V.; Minehart, J.; Sterman, D.H. Local Immunotherapy of Cancer: Innovative Approaches to Harnessing Tumor-Specific Immune Responses. J. Natl. Cancer Inst. 2017, 109, djx097. [Google Scholar] [CrossRef]
- Kolstad, A.; Kumari, S.; Walczak, M.; Madsbu, U.; Hagtvedt, T.; Bogsrud, T.V.; Kvalheim, G.; Holte, H.; Aurlien, E.; Delabie, J.; et al. Sequential intranodal immunotherapy induces antitumor immunity and correlated regression of disseminated follicular lymphoma. Blood 2015, 125, 82–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodama, T.; Matsuki, D.; Tada, A.; Takeda, K.; Mori, S. New concept for the prevention and treatment of metastatic lymph nodes using chemotherapy administered via the lymphatic network. Sci. Rep. 2016, 6, 32506. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Chen, J.; Chen, Z.; Zeng, X.; Zheng, P.; Wang, X.; Cui, X.; Sang, L. Efficacy and Safety of Thermal Ablation for Treating Lymph Node Metastasis From Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Pan, T.; Xie, Q.K.; Lv, N.; Li, X.S.; Mu, L.W.; Wu, P.H.; Zhao, M. Percutaneous CT-guided Radiofrequency Ablation for Lymph Node Oligometastases from Hepatocellular Carcinoma: A Propensity Score-matching Analysis. Radiology 2017, 282, 259–270. [Google Scholar] [CrossRef]
- Papalexis, N.; Parmeggiani, A.; Peta, G.; Spinnato, P.; Miceli, M.; Facchini, G. Minimally Invasive Interventional Procedures for Metastatic Bone Disease: A Comprehensive Review. Curr. Oncol. 2022, 29, 4155–4177. [Google Scholar] [CrossRef]
- Saravana-Bawan, S.; David, E.; Sahgal, A.; Chow, E. Palliation of bone metastases-exploring options beyond radiotherapy. Ann Palliat Med 2019, 8, 168–177. [Google Scholar] [CrossRef]
- Amoretti, N.; Gallo, G.; Bertrand, A.S.; Bard, R.L.; Kelekis, A. Percutaneous Facet Screw Fixation in the Treatment of Symptomatic Recurrent Lumbar Facet Joint Cyst: A New Technique. Cardiovasc. Interv. Radiol. 2016, 39, 127–131. [Google Scholar] [CrossRef]
- Gangi, A.; Tsoumakidou, G.; Buy, X.; Quoix, E. Quality improvement guidelines for bone tumour management. Cardiovasc. Interv. Radiol. 2010, 33, 706–713. [Google Scholar] [CrossRef] [Green Version]
- Nakatsuka, A.; Yamakado, K.; Takaki, H.; Uraki, J.; Makita, M.; Oshima, F.; Takeda, K. Percutaneous radiofrequency ablation of painful spinal tumors adjacent to the spinal cord with real-time monitoring of spinal canal temperature: A prospective study. Cardiovasc. Interv. Radiol. 2009, 32, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Macedo, F.; Ladeira, K.; Pinho, F.; Saraiva, N.; Bonito, N.; Pinto, L.; Goncalves, F. Bone Metastases: An Overview. Oncol. Rev. 2017, 11, 321. [Google Scholar] [CrossRef] [PubMed]
- Tubiana-Hulin, M. Incidence, prevalence and distribution of bone metastases. Bone 1991, 12, S9–S10. [Google Scholar] [CrossRef] [PubMed]
- Auloge, P.; Cazzato, R.L.; Rousseau, C.; Caudrelier, J.; Koch, G.; Rao, P.; Chiang, J.B.; Garnon, J.; Gangi, A. Complications of Percutaneous Bone Tumor Cryoablation: A 10-year Experience. Radiology 2019, 291, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, F.; de Baere, T.; Hakime, A.; Pearson, E.; Farouil, G.; Teriitehau, C.; Tselikas, L. Percutaneous osteosynthesis in the pelvis in cancer patients. Eur. Radiol. 2016, 26, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.Y.; Latich, I.; Toombs, C.; Mungur, A.; Conway, D.; Alder, K.; Ibe, I.; Lindskog, D.; Friedlaender, G. Minimally Invasive Image-Guided Ablation, Osteoplasty, Reinforcement, and Internal Fixation (AORIF) for Osteolytic Lesions in the Pelvis and Periarticular Regions of Weight-Bearing Bones. J. Vasc. Interv. Radiol. 2020, 31, 649–658. [Google Scholar] [CrossRef]
- Fisher, C.G.; DiPaola, C.P.; Ryken, T.C.; Bilsky, M.H.; Shaffrey, C.I.; Berven, S.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; Chou, D.; et al. A novel classification system for spinal instability in neoplastic disease: An evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 2010, 35, E1221–E1229. [Google Scholar] [CrossRef] [Green Version]
- Pusceddu, C.; Fancellu, A.; Ballicu, N.; Fele, R.M.; Sotgia, B.; Melis, L. CT-guided percutaneous screw fixation plus cementoplasty in the treatment of painful bone metastases with fractures or a high risk of pathological fracture. Skelet. Radiol. 2017, 46, 539–545. [Google Scholar] [CrossRef]
- Tam, A.; Ahrar, K. Palliative interventions for pain in cancer patients. Semin. Interv. Radiol. 2007, 24, 419–429. [Google Scholar] [CrossRef] [Green Version]
- De Marini, P.; Cazzato, R.L.; Auloge, P.; Koch, G.; Dalili, D.; Garnon, J.; Gangi, A. Percutaneous image-guided thermal ablation of bone metastases: A retrospective propensity study comparing the safety profile of radio-frequency ablation and cryo-ablation. Int. J. Hyperth. 2020, 37, 1386–1394. [Google Scholar] [CrossRef]
- Cazzato, R.L.; Palussière, J.; Auloge, P.; Rousseau, C.; Koch, G.; Dalili, D.; Buy, X.; Garnon, J.; De Marini, P.; Gangi, A. Complications Following Percutaneous Image-guided Radiofrequency Ablation of Bone Tumors: A 10-year Dual-Center Experience. Radiology 2020, 296, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Cazzato, R.L.; De Marini, P.; Leonard-Lorant, I.; Dalili, D.; Koch, G.; Autrusseau, P.A.; Mayer, T.; Weiss, J.; Auloge, P.; Garnon, J.; et al. Percutaneous thermal ablation of sacral metastases: Assessment of pain relief and local tumor control. Diagn. Interv. Imaging 2021, 102, 355–361. [Google Scholar] [CrossRef]
- Cazzato, R.L.; Auloge, P.; De Marini, P.; Rousseau, C.; Chiang, J.B.; Koch, G.; Caudrelier, J.; Rao, P.; Garnon, J.; Gangi, A. Percutaneous image-guided ablation of bone metastases: Local tumor control in oligometastatic patients. Int. J. Hyperth. 2018, 35, 493–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, C.S.; Ensor, J.E.; Ahrar, K.; Huang, S.Y.; Sabir, S.H.; Tannir, N.M.; Lewis, V.O.; Tam, A.L. Cryoablation of Bone Metastases from Renal Cell Carcinoma for Local Tumor Control. J. Bone Joint. Surg. Am. 2017, 99, 1916–1926. [Google Scholar] [CrossRef]
- Barile, A.; Arrigoni, F.; Bruno, F.; Palumbo, P.; Floridi, C.; Cazzato, R.L.; Reginelli, A.; Zappia, M.; Brunese, L.; Zugaro, L.; et al. Present role and future perspectives of interventional radiology in the treatment of painful bone lesions. Future Oncol. 2018, 14, 2945–2955. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iezzi, R.; Gangi, A.; Posa, A.; Pua, U.; Liang, P.; Santos, E.; Kurup, A.N.; Tanzilli, A.; Tenore, L.; De Leoni, D.; et al. Emerging Indications for Interventional Oncology: Expert Discussion on New Locoregional Treatments. Cancers 2023, 15, 308. https://doi.org/10.3390/cancers15010308
Iezzi R, Gangi A, Posa A, Pua U, Liang P, Santos E, Kurup AN, Tanzilli A, Tenore L, De Leoni D, et al. Emerging Indications for Interventional Oncology: Expert Discussion on New Locoregional Treatments. Cancers. 2023; 15(1):308. https://doi.org/10.3390/cancers15010308
Chicago/Turabian StyleIezzi, Roberto, Afshin Gangi, Alessandro Posa, Uei Pua, Ping Liang, Ernesto Santos, Anil N. Kurup, Alessandro Tanzilli, Lorenzo Tenore, Davide De Leoni, and et al. 2023. "Emerging Indications for Interventional Oncology: Expert Discussion on New Locoregional Treatments" Cancers 15, no. 1: 308. https://doi.org/10.3390/cancers15010308