
Habitat Imaging Biomarkers for Diagnosis and Prognosis in Cancer Patients Infected with COVID-19
 ,
,  , , , , , , add
Show full author list
, , , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Overall Study Design
2.2. Patient Population

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Datasets Characteristics | Stony Brook (N = 275) | MD Anderson COVID-19 Positive (N = 252) |
|---|---|---|
| No. (%) | No. (%) | |
| Age (years) | ||
| <18 | - | 1 (0.4%) |
| 18–59 | 125 (45%) | 112 (44%) |
| 60–74 | 83 (30%) | 99 (39%) |
| 75–90 | 67 (24) | 37 (15%) |
| >90 | - | 3 (1%) |
| Sex | ||
| Male | 160 (58%) | 121 (48%) |
| Female | 106 (39%) | 131 (52%) |
| NA | 9 (3%) | - |
| BMI | ||
| >30 | 100 (36%) | 70 (28%) |
| <30 | 127 (46%) | 95 (38%) |
| NA | 48 (17%) | 87 (35%) |
| Smoking status | ||
| Current | 6 (2%) | 11 (5%) |
| Former | 63 (23%) | 90 (36%) |
| Never | 138 (50%) | 148 (59%) |
| NA | 68 (25%) | 3 (1%) |
| Major diseases | ||
| Malignancy | 25 (9%) | 240 (95%) |
| Hypertension | 105 (38%) | 136 (54%) |
| Diabetes | 54 (20%) | 105 (42%) |
| Coronary artery diseases | 33 (12%) | 50 (20%) |
| Chronic kidney disease | 19 (7%) | 75 (30%) |
| Chronic obstructive pulmonary disease | 18 (7%) | 15 (6%) |
| Other lung diseases | 39 (14%) | 22 (9%) |
| Symptoms at onset | ||
| Fever | 158 (57%) | 33 (13%) |
| Shortness of breath | 152 (55%) | 14 (6%) |
| Cough | 157 (57%) | 39 (15%) |
| Nausea | 49 (18%) | 17 (7%) |
| Vomiting | 29 (11%) | 9 (4%) |
| Diarrhea | 65 (24%) | 17 (7%) |
| Abdominal pain | 19 (7%) | 7 (3%) |
| Hospitalization status | ||
| Inpatient/admitted | 259 (94%) | 86 (34%) |
| Outpatient | - | 166 (66%) |
| Emergency Visit | 16 (6%) | - |
| ICU | ||
| TRUE | 83 (30%) | 42 (17%) |
| FALSE | 192 (70%) | 209 (83%) |
| Oxygen requirement | ||
| TRUE | 71 (26%) | 20 (8%) |
| FALSE | 204 (74%) | 232 (92%) |
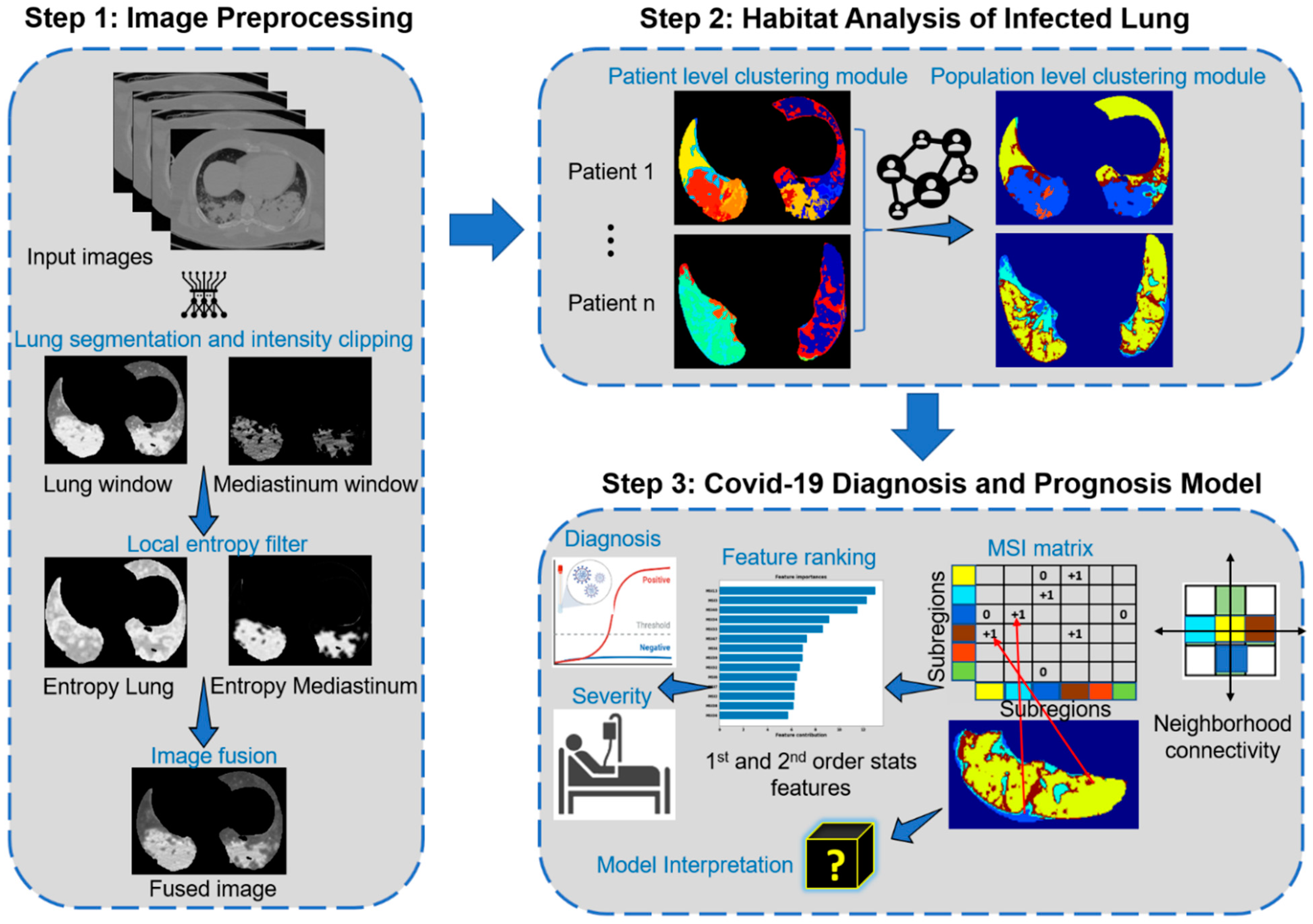
2.3. Imaging Preprocessing and Fusion
2.4. Habitat Image Pipeline
2.5. Habitat Imaging Based Machine Learning Model
2.6. Model Interpretation
2.7. Statistical Analysis
3. Results
3.1. Habitat Image Analysis
3.2. Habitat Models for COVID-19 Diagnosis
3.3. Comparison between Diagnostic Models of General Population and Cancer Population
3.4. Habitat Models for COVID-19 Prognosis and Severity Prediction
3.5. Habitat Models Interpretation
3.6. Comparison to Deep Learning Approach
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RT-PCR | Reverse Transcription Polymerase Chain Reaction |
| AI | artificial intelligence |
| GGO | ground glass opacities |
| MSI | multiregional spatial interaction |
| ROC | receiver operating characteristics |
| AUC | area under the curve |
References
- Pecoraro, V.; Negro, A.; Pirotti, T.; Trenti, T. Estimate false-negative RT-PCR rates for SARS-CoV-2. A systematic review and meta-analysis. Eur. J. Clin. Investig. 2022, 52, e13706. [Google Scholar] [CrossRef] [PubMed]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef]
- West, C.P.; Montori, V.M.; Sampathkumar, P. COVID-19 Testing: The Threat of False-Negative Results. Mayo Clin. Proc. 2020, 95, 1127–1129. [Google Scholar] [CrossRef] [PubMed]
- Elie, A.; Ivana, B.; Sally, Y.; Guy, F.; Roger, C.; John, A.; Mansoor, F.; Nicola, F.; Eveline, H.; Hussain, J.; et al. Use of Chest Imaging in the Diagnosis and Management of COVID-19: A WHO Rapid Advice Guide. Radiology 2020, 298, E63–E69. [Google Scholar] [CrossRef]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain 2020, 143, 3104–3120. [Google Scholar] [CrossRef]
- Chen, J.; Qi, T.; Liu, L.; Ling, Y.; Qian, Z.; Li, T.; Li, F.; Xu, Q.; Zhang, Y.; Xu, S.; et al. Clinical progression of patients with COVID-19 in Shanghai, China. J. Infect. 2020, 80, e1–e6. [Google Scholar] [CrossRef]
- Desai, A.; Mohammed, T.J.; Duma, N.; Garassino, M.C.; Hicks, L.K.; Kuderer, N.M.; Lyman, G.H.; Mishra, S.; Pinato, D.J.; Rini, B.I. COVID-19 and Cancer: A Review of the Registry-Based Pandemic Response. JAMA Oncol. 2021, 7, 1882–1890. [Google Scholar] [CrossRef]
- Zoabi, Y.; Deri-Rozov, S.; Shomron, N. Machine learning-based prediction of COVID-19 diagnosis based on symptoms. NPJ Digit. Med. 2021, 4, 3. [Google Scholar] [CrossRef]
- Imran, A.; Posokhova, I.; Qureshi, H.N.; Masood, U.; Riaz, M.S.; Ali, K.; John, C.N.; Hussain, M.I.; Nabeel, M. AI4COVID-19: AI enabled preliminary diagnosis for COVID-19 from cough samples via an app. Inform. Med. Unlocked 2020, 20, 100378. [Google Scholar] [CrossRef] [PubMed]
- Cabitza, F.; Campagner, A.; Ferrari, D.; Di Resta, C.; Ceriotti, D.; Sabetta, E.; Colombini, A.; De Vecchi, E.; Banfi, G.; Locatelli, M.; et al. Development, evaluation, and validation of machine learning models for COVID-19 detection based on routine blood tests. Clin. Chem. Lab. Med. (CCLM) 2021, 59, 421–431. [Google Scholar] [CrossRef]
- Soltan, A.A.; Yang, J.; Pattanshetty, R.; Novak, A.; Yang, Y.; Rohanian, O.; Beer, S.; Soltan, M.A.; Thickett, D.R.; Fairhead, R.; et al. Real-world evaluation of rapid and laboratory-free COVID-19 triage for emergency care: External validation and pilot deployment of artificial intelligence driven screening. Lancet Digit. Health 2022, 4, e266–e278. [Google Scholar] [CrossRef] [PubMed]
- Soltan, A.A.; Kouchaki, S.; Zhu, T.; Kiyasseh, D.; Taylor, T.; Hussain, Z.B.; Peto, T.; Brent, A.J.; Eyre, D.W.; Clifton, D.A. Rapid triage for COVID-19 using routine clinical data for patients attending hospital: Development and prospective validation of an artificial intelligence screening test. Lancet Digit. Health 2021, 3, e78–e87. [Google Scholar] [CrossRef] [PubMed]
- Mei, X.; Lee, H.C.; Diao, K.Y.; Huang, M.; Lin, B.; Liu, C.; Xie, Z.; Ma, Y.; Robson, P.M.; Chung, M.; et al. Artificial intelligence–enabled rapid diagnosis of patients with COVID-19. Nat. Med. 2020, 26, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Kurstjens, S.; Van Der Horst, A.; Herpers, R.; Geerits, M.W.; Kluiters-de Hingh, Y.C.; Göttgens, E.L.; Blaauw, M.J.; Thelen, M.H.; Elisen, M.G.; Kusters, R. Rapid identification of SARS-CoV-2-infected patients at the emergency department using routine testing. Clin. Chem. Lab. Med. (CCLM) 2020, 58, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Shamout, F.E.; Shen, Y.; Wu, N.; Kaku, A.; Park, J.; Makino, T.; Jastrzębski, S.; Witowski, J.; Wang, D.; Zhang, B.; et al. An artificial intelligence system for predicting the deterioration of COVID-19 patients in the emergency department. NPJ Digit. Med. 2021, 4, 80. [Google Scholar] [CrossRef]
- Heaven, W.D. Hundreds of AI tools have been built to catch covid. None of them helped. MIT Technol. Review. Retrieved Oct. 2021, 6, 2021. [Google Scholar]
- Zhang, Y.J.; Yang, W.J.; Liu, D.; Cao, Y.Q.; Zheng, Y.Y.; Han, Y.C.; Jin, R.S.; Han, Y.; Wang, X.Y.; Pan, A.S.; et al. COVID-19 and early-stage lung cancer both featuring ground-glass opacities: A propensity score-matched study. Transl. Lung Cancer Res. 2020, 9, 1516–1527. [Google Scholar] [CrossRef]
- Guarnera, A.; Santini, E.; Podda, P. COVID-19 Pneumonia and Lung Cancer: A Challenge for the Radiologist Review of the Main Radiological Features, Differential Diagnosis and Overlapping Pathologies. Tomography 2022, 8, 513–528. [Google Scholar] [CrossRef]
- Dingemans, A.M.C.; Soo, R.A.; Jazieh, A.R.; Rice, S.J.; Kim, Y.T.; Teo, L.L.; Warren, G.W.; Xiao, S.Y.; Smit, E.F.; Aerts, J.G.; et al. Treatment Guidance for Patients With Lung Cancer During the Coronavirus 2019 Pandemic. J. Thorac. Oncol. 2020, 15, 1119–1136. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Song, K.H.; Yao, Y.; Dong, X.R.; Li, L.J.; Wang, Q.; Yang, J.Y.; Hu, W.D.; Xie, Z.B.; Luo, Z.G.; et al. Individualized model for predicting COVID-19 deterioration in patients with cancer: A multicenter retrospective study. Cancer Sci. 2021, 112, 2522–2532. [Google Scholar] [CrossRef] [PubMed]
- Navlakha, S.; Morjaria, S.; Perez-Johnston, R.; Zhang, A.; Taur, Y. Projecting COVID-19 disease severity in cancer patients using purposefully-designed machine learning. BMC Infect. Dis. 2021, 21, 391. [Google Scholar] [CrossRef]
- Napel, S.; Mu, W.; Jardim-Perassi, B.V.; Aerts, H.; Gillies, R.J. Quantitative imaging of cancer in the postgenomic era: Radio(geno)mics, deep learning, and habitats. Cancer 2018, 124, 4633–4649. [Google Scholar] [CrossRef]
- Zhang, J.; Fujimoto, J.; Zhang, J.; Wedge, D.C.; Song, X.; Zhang, J.; Seth, S.; Chow, C.W.; Cao, Y.; Gumbs, C.; et al. Intratumor heterogeneity in localized lung adenocarcinomas delineated by multiregion sequencing. Science 2014, 346, 256–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Cao, G.; Sun, X.; Lee, J.; Rubin, D.L.; Napel, S.; Kurian, A.W.; Daniel, B.L.; Li, R. Intratumoral Spatial Heterogeneity at Perfusion MR Imaging Predicts Recurrence-free Survival in Locally Advanced Breast Cancer Treated with Neoadjuvant Chemotherapy. Radiology 2018, 288, 26–35. [Google Scholar] [CrossRef]
- Saltz, J. Stony Brook University COVID-19 Positive Cases. Cancer Imaging Arch. 2021. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Tsai, E.B.; Simpson, S.; Lungren, M.P.; Hershman, M.; Roshkovan, L.; Colak, E.; Erickson, B.J.; Shih, G.; Stein, A.; Kalpathy-Cramer, J.; et al. Data from medical imaging data resource center (MIDRC)-RSNA international covid radiology database (RICORD) release 1C—Chest X-ray, covid+(MIDRC-RICORD-1C). Cancer Imaging Arch. 2021, 6, 13. [Google Scholar] [CrossRef]
- Tsai, E.B.; Simpson, S.; Lungren, M.P.; Hershman, M.; Roshkovan, L.; Colak, E.; Erickson, B.J.; Shih, G.; Stein, A.; Kalpathy-Cramer, J.; et al. The RSNA international COVID-19 open radiology database (RICORD). Radiology 2021, 299, E204–E213. [Google Scholar] [CrossRef]
- Hofmanninger, J.; Prayer, F.; Pan, J.; Röhrich, S.; Prosch, H.; Langs, G. Automatic lung segmentation in routine imaging is primarily a data diversity problem, not a methodology problem. Eur. Radiol. Exp. 2020, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Gensheimer, M.F.; Dong, X.; Rubin, D.L.; Napel, S.; Diehn, M.; Loo, B.W., Jr.; Li, R. Robust intratumor partitioning to identify high-risk subregions in lung cancer: A pilot study. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1504–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Gensheimer, M.F.; Zhang, N.; Guo, M.; Liang, R.; Zhang, C.; Fischbein, N.; Pollom, E.L.; Beadle, B.; Le, Q.T. Tumor subregion evolution-based imaging features to assess early response and predict prognosis in oropharyngeal cancer. J. Nucl. Med. 2020, 61, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Achanta, R.; Shaji, A.; Smith, K.; Lucchi, A.; Fua, P.; Süsstrunk, S. SLIC superpixels compared to state-of-the-art superpixel methods. IEEE Trans. Pattern Anal. Mach. Intell. 2012, 34, 2274–2282. [Google Scholar] [CrossRef] [Green Version]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P. Radiological Society of North America expert consensus document on reporting chest CT findings related to COVID-19: Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA. Radiol. Cardiothorac. Imaging 2020, 2, e200152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, K.; Liu, X.; Shen, J.; Li, Z.; Sang, Y.; Wu, X.; Zha, Y.; Liang, W.; Wang, C.; Wang, K. Clinically applicable AI system for accurate diagnosis, quantitative measurements, and prognosis of COVID-19 pneumonia using computed tomography. Cell 2020, 181, 1423–1433.e1411. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Zhao, C.; Xu, Y.; He, Z.; Tang, J.; Zhang, Y.; Han, J.; Shi, Y.; Zhou, W. Lung segmentation and automatic detection of COVID-19 using radiomic features from chest CT images. Pattern Recognit. 2021, 119, 108071. [Google Scholar] [CrossRef]
- Bai, X.; Wang, H.; Ma, L.; Xu, Y.; Gan, J.; Fan, Z.; Yang, F.; Ma, K.; Yang, J.; Bai, S. Advancing COVID-19 diagnosis with privacy-preserving collaboration in artificial intelligence. Nat. Mach. Intell. 2021, 3, 1081–1089. [Google Scholar] [CrossRef]
- Fang, X.; Li, X.; Bian, Y.; Ji, X.; Lu, J. Radiomics nomogram for the prediction of 2019 novel coronavirus pneumonia caused by SARS-CoV-2. Eur. Radiol. 2020, 30, 6888–6901. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, L.; Lee, E.H.; Zheng, J.; Zhang, W.; Halabi, S.; Liu, C.; Deng, K.; Song, J.; Yeom, K.W. Decoding COVID-19 pneumonia: Comparison of deep learning and radiomics CT image signatures. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1478–1486. [Google Scholar] [CrossRef] [PubMed]
- Homayounieh, F.; Ebrahimian, S.; Babaei, R.; Mobin, H.K.; Zhang, E.; Bizzo, B.C.; Mohseni, I.; Digumarthy, S.R.; Kalra, M.K. CT radiomics, radiologists, and clinical information in predicting outcome of patients with COVID-19 pneumonia. Radiol. Cardiothorac. Imaging 2020, 2, e200322. [Google Scholar] [CrossRef] [PubMed]
- Saygılı, A. A new approach for computer-aided detection of coronavirus (COVID-19) from CT and X-ray images using machine learning methods. Appl. Soft Comput. 2021, 105, 107323. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Chen, W.; Cao, Y.; Xu, Z.; Tan, Z.; Zhang, X.; Deng, L.; Zheng, C.; Zhou, J.; Shi, H. Development and evaluation of an artificial intelligence system for COVID-19 diagnosis. Nat. Commun. 2020, 11, 5088. [Google Scholar] [CrossRef]
- Aminu, M.; Ahmad, N.A.; Noor, M.H.M. Covid-19 detection via deep neural network and occlusion sensitivity maps. Alex. Eng. J. 2021, 60, 4829–4855. [Google Scholar] [CrossRef]
- Song, Y.; Zheng, S.; Li, L.; Zhang, X.; Zhang, X.; Huang, Z.; Chen, J.; Wang, R.; Zhao, H.; Chong, Y. Deep learning enables accurate diagnosis of novel coronavirus (COVID-19) with CT images. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 18, 2775–2780. [Google Scholar] [CrossRef]
- Zhang, N.; Liang, R.; Gensheimer, M.F.; Guo, M.; Zhu, H.; Yu, J.; Diehn, M.; Loo, B.W., Jr.; Li, R.; Wu, J. Early response evaluation using primary tumor and nodal imaging features to predict progression-free survival of locally advanced non-small cell lung cancer. Theranostics 2020, 10, 11707–11718. [Google Scholar] [CrossRef]
- Noor, A.; Muhammad, A.; Mohd, N.M.H. Covid-19 detection via deep neural network and occlusion sensitivity maps. TechRxiv 2021. [Google Scholar] [CrossRef]






| Feature Name | Feature Description |
|---|---|
| MSI 1–MSI 4 | 2nd order statistics features |
| MSI 5–MSI 10 | absolute habitat subregions volume (SR1–SR6) |
| MSI 11–MSI 16 | interaction (absolute) between habitat subregions and border |
| MSI 17–MSI 21 | interaction (absolute) between SR1 and the remaining subregions, i.e., MSI 17 = SR1 SR2, MSI 18 = SR1 SR3, …, MSI 21 = SR1 SR6. |
| MSI 22–MSI 25 | interaction (absolute) between SR2 and SR3, SR4, SR5 and SR6, i.e., MSI 22 = SR2 SR3, MSI 23 = SR2 SR4, MSI 24 = SR2 SR5, MSI 25 = SR2 SR6. |
| MSI 26–MSI 28 | interaction (absolute) between SR3 and SR4, SR5 and SR6, i.e., MSI 26 = SR3 SR4, MSI 27 = SR3 SR5, MSI 28 = SR3 SR6. |
| MSI 29–MSI 30 | interaction (absolute) between SR4 and SR5 and SR6, i.e., MSI 29 = SR4 SR5, MSI 30 = SR4 SR6. |
| MSI 31 | interaction (absolute) between SR5 and SR6, i.e., MSI 30 = SR5 SR6. |
| MSI 32–MSI 37 | percentage of habitat subregions volume (SR1–SR6) |
| MSI 38–MSI 43 | normalized interaction (percentage) between habitat subregions and border |
| MSI 44–MSI 48 | normalized interaction (percentage) between SR1 and the remaining subregions, i.e., MSI 44 = SR1 SR2, MSI 45 = SR1 SR3, …, MSI 48 = SR1 SR6. |
| MSI 49–MSI 52 | normalized interaction (percentage) between SR2 and SR3, SR4, SR5 and SR6, i.e., MSI 49 = SR2 SR3, MSI 50 = SR2 SR4, MSI 51 = SR2 SR5, MSI 52 = SR2 SR6. |
| MSI 53–MSI 55 | normalized interaction (percentage) between SR3 and SR4, SR5 and SR6, i.e., MSI 53 = SR3 SR4, MSI 54 = SR3 SR5, MSI 55 = SR3 SR6. |
| MSI 56–MSI 57 | normalized interaction (percentage) between SR4 and SR5 and SR6, i.e., MSI 56 = SR4 SR5, MSI 57 = SR4 SR6. |
| MSI 58 | normalized interaction (percentage) between SR5 and SR6, i.e., MSI 58 = SR5 SR6. |
| Methods | Cohort | |||||||
|---|---|---|---|---|---|---|---|---|
| General | Cancer | |||||||
| Acc | Sen | Spe | AUC | Acc | Sen | Spe | AUC | |
| LR | 0.9944 | 1.0000 | 0.9928 | 0.9999 | 1.0000 | 1.0000 | 1.0000 | 1.0000 |
| RF | 0.9944 | 0.9914 | 0.9952 | 0.9998 | 0.9952 | 0.9878 | 1.0000 | 0.9998 |
| SVM | 0.9906 | 0.9912 | 0.9904 | 0.9998 | 0.9976 | 1.0000 | 0.9961 | 1.0000 |
| GAM | 0.9925 | 1.000 | 0.9904 | 0.9997 | 0.9952 | 0.9938 | 0.9961 | 1.0000 |
| Methods | All | |||
|---|---|---|---|---|
| Acc | Sen | Spe | AUC | |
| LR | 0.8738 | 0.9910 | 0.8317 | 0.9807 |
| RF | 0.8548 | 1.0000 | 0.8088 | 0.9178 |
| SVM | 0.8548 | 1.0000 | 0.8088 | 0.9586 |
| GAM | 0.9000 | 0.9918 | 0.8624 | 0.9202 |
| Methods | Cohort | |||||||
|---|---|---|---|---|---|---|---|---|
| General | Cancer | |||||||
| Acc | Sen | Spe | AUC | Acc | Sen | Spe | AUC | |
| LR | 0.9616 | 0.9796 | 0.9457 | 0.9961 | 0.9912 | 1.0000 | 0.9821 | 1.0000 |
| RF | 0.9161 | 1.0000 | 0.8589 | 0.9949 | 0.9580 | 1.0000 | 0.9205 | 1.0000 |
| SVM | 0.9928 | 1.0000 | 0.9861 | 1.0000 | 0.9757 | 1.0000 | 0.9524 | 1.0000 |
| GAM | 0.9161 | 1.0000 | 0.8589 | 0.9967 | 0.9867 | 1.0000 | 0.9735 | 1.0000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aminu, M.; Yadav, D.; Hong, L.; Young, E.; Edelkamp, P., Jr.; Saad, M.; Salehjahromi, M.; Chen, P.; Sujit, S.J.; Chen, M.M.; et al. Habitat Imaging Biomarkers for Diagnosis and Prognosis in Cancer Patients Infected with COVID-19. Cancers 2023, 15, 275. https://doi.org/10.3390/cancers15010275
Aminu M, Yadav D, Hong L, Young E, Edelkamp P Jr., Saad M, Salehjahromi M, Chen P, Sujit SJ, Chen MM, et al. Habitat Imaging Biomarkers for Diagnosis and Prognosis in Cancer Patients Infected with COVID-19. Cancers. 2023; 15(1):275. https://doi.org/10.3390/cancers15010275
Chicago/Turabian StyleAminu, Muhammad, Divya Yadav, Lingzhi Hong, Elliana Young, Paul Edelkamp, Jr., Maliazurina Saad, Morteza Salehjahromi, Pingjun Chen, Sheeba J. Sujit, Melissa M. Chen, and et al. 2023. "Habitat Imaging Biomarkers for Diagnosis and Prognosis in Cancer Patients Infected with COVID-19" Cancers 15, no. 1: 275. https://doi.org/10.3390/cancers15010275