
Molecular Targets in Lung Cancer: Study of the Evolution of Biomarkers Associated with Treatment with Tyrosine Kinase Inhibitors—Has NF1 Tumor Suppressor a Key Role in Acquired Resistance?

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Extraction of cfDNA from Plasma Samples for EGFR Mutation Analysis
2.3. Molecular Characterization of EGFR in cfDNA
2.4. Extraction of cfDNA from Plasma Samples for NGS Analysis
2.5. Validation and Molecular Characterization of NSCLC in FFPE and cfDNA Samples
2.6. Library Preparation and Sequencing
2.7. Variant Calling and Data Analysis
2.8. Statistical Analysis
3. Results
3.1. EGFR Mutations Detected in Tissue and Plasma Samples
3.1.1. Characteristics of Patient Cohort and Presence of Initial EGFR Mutation
3.1.2. EGFR Mutations Detected in Plasma Samples
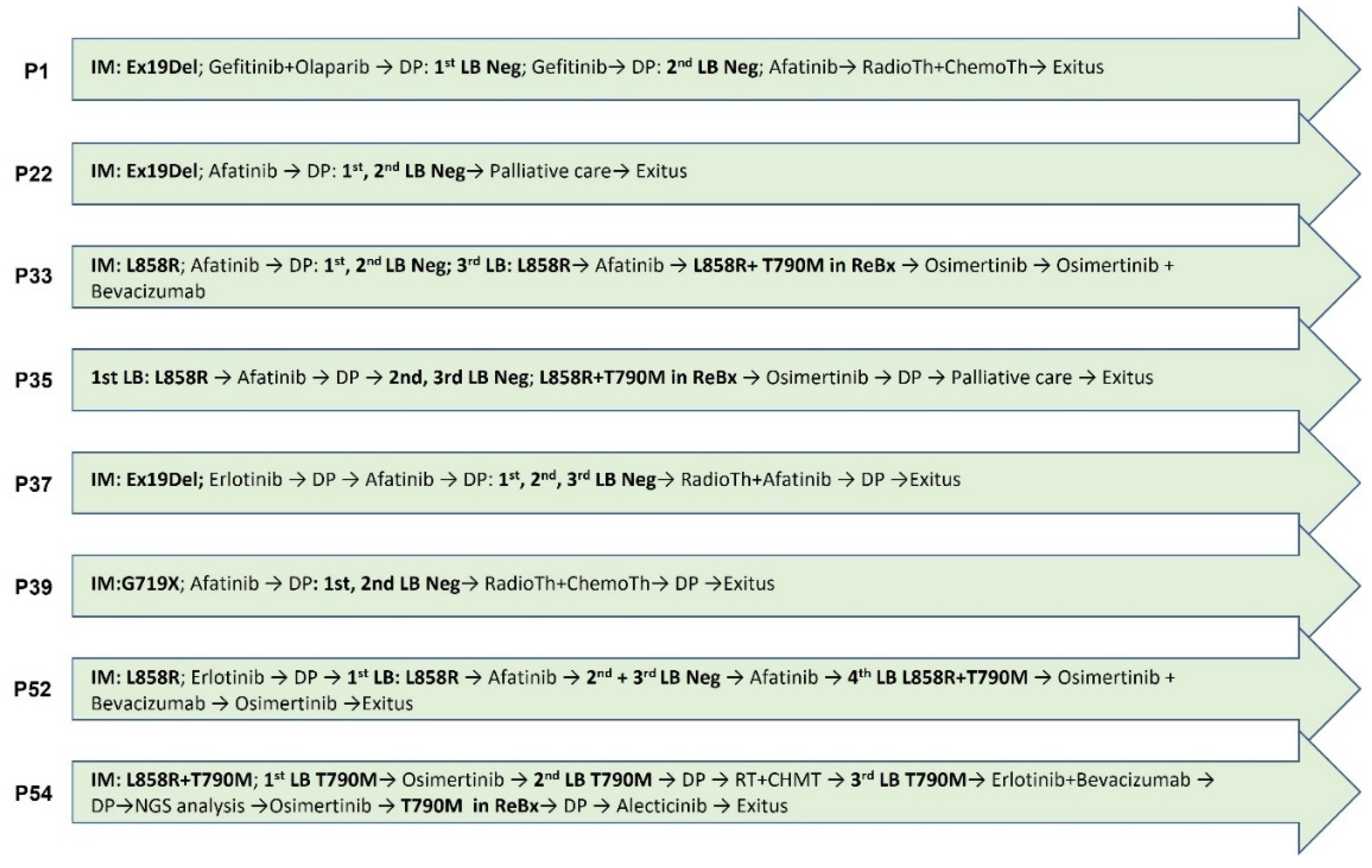
3.1.3. Patients Undergoing Rebiopsy
3.1.4. Correlation between Mutations
3.2. Liquid Biopsy as a Disease Monitor. Response to TKIs
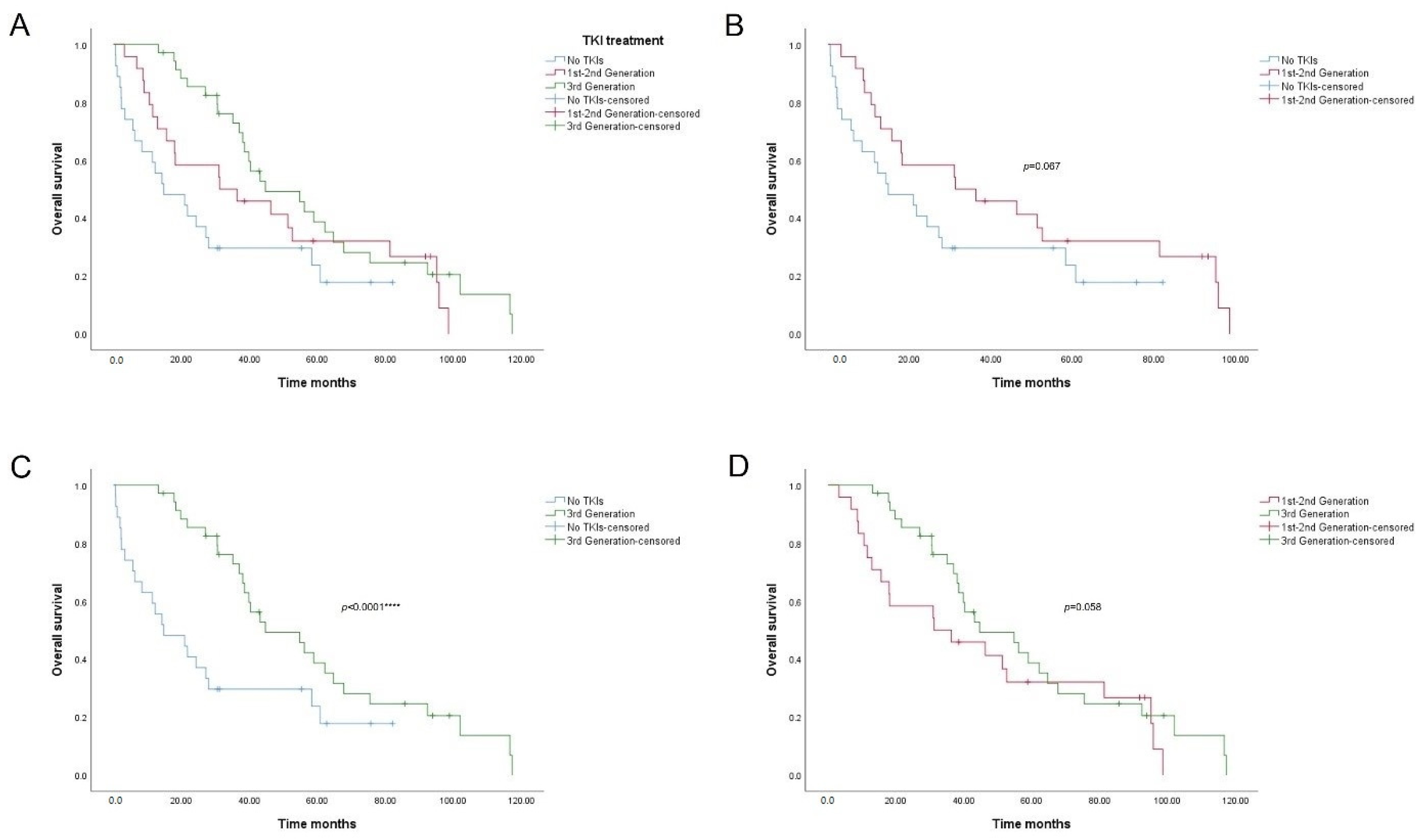
3.3. Prognostic Significance of the T790M EGFR Mutation and TKI Treatment
3.4. Validation of EGFR Results in Tissue and Plasma Samples
3.5. NGS Analysis of Patients with Discordant Progression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hirsch, F.R.; Scagliotti, G.V.; Mulshine, J.L.; Kwon, R.; Curran, W.J., Jr.; Wu, Y.-L.; Paz-Ares, L. Lung cancer: Current therapies and new targeted treatments. Lancet 2017, 389, 299–311. [Google Scholar] [CrossRef]
- Zhao, H.; Wu, L.; Yan, G.; Chen, Y.; Zhou, M.; Wu, Y.; Li, Y. Inflammation and tumor progression: Signaling pathways and targeted intervention. Signal Transduct. Target Ther. 2021, 6, 263. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Jadhav, H.R. Targeting non-small cell lung cancer with small-molecule EGFR tyrosine kinase inhibitors. Drug Discov. Today 2018, 23, 745–753. [Google Scholar] [CrossRef]
- Rosell, R.; Morán, T.; Carcereny, E.; Quiroga, V.; Molina, M.A.; Costa, C.; Tarón, M. Non-small-cell lung cancer harbouring mutations in the EGFR kinase domain. Clin. Transl. Oncol. 2010, 12, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Zhou, C.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated molecular testing guideline for the selection of Lung Cancer patients for treatment with targeted tyrosine kinase inhibitors: Guideline from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; Yang, B.; An, Q.; Assaraf, Y.G.; Cao, X.; Xia, J. Acquired resistance to third-generation EGFR-TKIs and emerging next-generation EGFR inhibitors. Innovation 2021, 2, 100103. [Google Scholar] [CrossRef]
- Wu, S.-G.; Shih, J.-Y. Management of acquired resistance to EGFR TKI–targeted therapy in advanced non-small cell lung cancer. Mol. Cancer 2018, 17, 1–14. [Google Scholar] [CrossRef]
- Socinski, M.A.; Villaruz, L.C.; Ross, J. Understanding mechanisms of resistance in the epithelial growth factor receptor in non-small cell lung cancer and the role of biopsy at progression. Oncologist 2017, 22, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Yun, C.-H.; Mengwasser, K.E.; Toms, A.V.; Woo, M.S.; Greulich, H.; Wong, K.-K.; Meyerson, M.; Eck, M.J. The T790M mutation in EGFR kinase causes drug resistance by increasing the affinity for ATP. Proc. Natl. Acad. Sci. USA 2008, 105, 2070–2075. [Google Scholar] [CrossRef] [Green Version]
- Santarpia, M.; Liguori, A.; D’Aveni, A.; Karachaliou, N.; Gonzalez-Cao, M.; Daffinà, M.G.; Lazzari, C.; Altavilla, G.; Rosell, R. Liquid biopsy for lung cancer early detection. J. Thorac. Dis. 2018, 10, S882–S897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morán, T.; Felip, E.; Bosch-Barrera, J.; de Aguirre, I.; Ramirez, J.L.; Mesia, C.; Carcereny, E.; Roa, D.; Sais, E.; García, Y.; et al. Monitoring EGFR-T790M mutation in serum/plasma for prediction of response to third-generation EGFR inhibitors in patients with lung cancer. Oncotarget 2018, 9, 27074–27086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.-L.; Chen, Y.-L.; Yang, S.-C.; Ho, C.-L.; Wei, F.; Wong, D.T.; Su, W.C.; Lin, C.-C. Liquid biopsy genotyping in lung cancer: Ready for clinical utility? Oncotarget 2017, 8, 18590–18608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolfo, C.; Mack, P.C.; Scagliotti, G.V.; Baas, P.; Barlesi, F.; Bivona, T.G.; Herbst, R.S.; Mok, T.S.; Peled, N.; Pirker, R.; et al. Liquid biopsy for advanced non-small cell lung cancer (NSCLC): A statement paper from the IASLC. J. Thorac. Oncol. 2018, 13, 1248–1268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remon, J.; García-Campelo, R.; de Álava, E.; Vera, R.; Rodríguez-Peralto, J.L.; Rodríguez-Lescure, Á.; Bellosillo, B.; Garrido, P.; Rojo, F.; Álvarez-Alegret, R. Liquid biopsy in oncology: A consensus statement of the Spanish Society of Pathology and the Spanish Society of Medical Oncology. Clin. Transl. Oncol. 2020, 22, 823–834. [Google Scholar] [CrossRef] [Green Version]
- Duffy, M.J.; Crown, J. Use of circulating tumour DNA (ctDNA) for measurement of therapy predictive biomarkers in patients with cancer. J. Pers. Med. 2022, 12, 99. [Google Scholar] [CrossRef]
- Thress, K.S.; Paweletz, C.P.; Felip, E.; Cho, B.C.; Stetson, D.; Dougherty, B.; Lai, Z.; Markovets, A.; Vivancos, A.; Kuang, Y.; et al. Acquired EGFR C797S mutation mediates resistance to AZD9291 in non-small cell lung cancer harboring EGFR T790M. Nat. Med. 2015, 21, 560–562. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Loriot, Y.; André, F.; Gobert, A.; Auger, N.; Lacroix, L.; Soria, J.C. EGFR-independent mechanisms of acquired resistance to AZD9291 in EGFR T790M-positive NSCLC patients. Ann. Oncol. 2015, 26, 2073–2078. [Google Scholar] [CrossRef]
- Dono, M.; De Luca, G.; Lastraioli, S.; Anselmi, G.; Dal Bello, M.G.; Coco, S.; Vanni, I.; Grossi, F.; Vigani, A.; Genova, C.; et al. Tag-based next generation sequencing: A feasible and reliable assay for EGFR T790M mutation detection in circulating tumor DNA of non-small cell lung cancer patients. Mol. Med. 2019, 25, 15. [Google Scholar] [CrossRef]
- Chang, Y.-S.; Tu, S.-J.; Chen, Y.-C.; Liu, T.-Y.; Lee, Y.-T.; Yen, J.-C.; Fang, H.-Y.; Chang, J.-G. Mutation profile of non-small cell lung cancer revealed by next generation sequencing. Respir. Res. 2021, 22, 3. [Google Scholar] [CrossRef]
- Rami-Porta, R.; Asamura, H.; Travis, W.D.; Rusch, V.W. Lung cancer—major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 138–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Q.; Zhu, Y.; Bai, Y.; Wei, X.; Zheng, X.; Mao, M.; Zheng, G. Detection of epidermal growth factor receptor mutation in lung cancer by droplet digital polymerase chain reaction. Onco. Targets Ther. 2015, 8, 1533–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, N.; Azuma, K.; Sakai, K.; Hattori, S.; Kawahara, A.; Ishii, H.; Tokito, T.; Kinoshita, T.; Yamada, K.; Nishio, K.; et al. Association of EGFR Exon 19 deletion and EGFR-TKI treatment duration with frequency of T790M mutation in EGFR-mutant lung cancer patients. Sci. Rep. 2016, 6, 36458. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Miao, S.; Wang, F.; Fang, W.; Chen, G.; Chen, X.; Yan, F.; Huang, X.; Wu, M.; Huang, Y.; et al. The efficacy and toxicity of afatinib in advanced EGFR-positive non-small-cell lung cancer patients after failure of first-generation tyrosine kinase inhibitors: A systematic review and meta-analysis. J. Thorac. Dis. 2017, 9, 1980–1987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Li, J. Second-generation EGFR and ErbB tyrosine kinase inhibitors as first-line treatments for non-small cell lung cancer. Onco Targets Ther. 2019, 12, 6535–6548. [Google Scholar] [CrossRef] [PubMed]
- EER. SEER Cancer Statistics Review 1975–2016. Available online: https://seer.cancer.gov/csr/1975_2016/index.html (accessed on 23 March 2022).
- Nasim, F.; Sabath, B.F.; Eapen, G.A. Lung cancer. Med. Clin. 2019, 103, 463–473. [Google Scholar] [CrossRef]
- Lee, T.; Lee, B.; Choi, Y.-L.; Han, J.; Ahn, M.-J.; Um, S.-W. Non-small cell lung cancer with concomitant EGFR, KRAS, and ALK mutation: Clinicopathologic features of 12 cases. J. Pathol. Transl. Med. 2016, 50, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Serna-Blasco, R.; Sánchez-Herrero, E.; Sanz-Moreno, S.; Rodriguez-Festa, A.; García-Veros, E.; Casarrubios, M.; Sierra-Rodero, B.; Laza-Briviesca, R.; Cruz-Bermúdez, A.; Mielgo-Rubio, X.; et al. KRAS p.G12C mutation occurs in 1% of EGFR-mutated advanced non-small-cell lung cancer patients progressing on a first-line treatment with a tyrosine kinase inhibitor. ESMO Open 2021, 6, 100279. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [Green Version]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and guidelines for the interpretation and reporting of sequence variants in cancer: A joint consensus recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Hu, H.; Pan, Y.; Wang, R.; Li, Y.; Shen, L.; Yu, Y.; Li, H.; Cai, D.; Sun, Y.; et al. PIK3CA mutations frequently coexist with EGFR/KRAS mutations in non-small cell lung cancer and suggest poor prognosis in EGFR/KRAS wildtype subgroup. PLoS ONE 2014, 9, e88291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redig, A.J.; Capelletti, M.; Dahlberg, S.E.; Sholl, L.M.; Mach, S.; Fontes, C.; Shi, Y.; Chalasani, P.; Jänne, P.A. Clinical and molecular characteristics of NF1-mutant lung cancer. Clin. Cancer Res. 2016, 22, 3148–3156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; García-Gómez, R.; Pallares, C.; Sánchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [Green Version]
- Sequist, L.V.; Waltman, B.A.; Dias-Santagata, D.; Digumarthy, S.; Turke, A.B.; Fidias, P.; Bergethon, K.; Shaw, A.T.; Gettinger, S.; Cosper, A.K.; et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci. Transl. Med. 2011, 3, ra26–ra75. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.A.; Arcila, M.E.; Rekhtman, N.; Sima, C.S.; Zakowski, M.F.; Pao, W.; Kris, M.G.; Miller, V.A.; Ladanyi, M.; Riely, G.J. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin. Cancer Res. 2013, 19, 2240–2247. [Google Scholar] [CrossRef] [Green Version]
- Cross, D.A.E.; Ashton, S.E.; Ghiorghiu, S.; Eberlein, C.; Nebhan, C.A.; Spitzler, P.J.; Orme, J.P.; Raymond, M.; Finlay, V.; Ward, R.A.; et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014, 4, 1046–1061. [Google Scholar] [CrossRef] [Green Version]
- Leonetti, A.; Sharma, S.; Minari, R.; Perego, P.; Giovannetti, E.; Tiseo, M. Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Br. J. Cancer 2019, 121, 725–737. [Google Scholar] [CrossRef]
- Zhu, S.-J.; Zhao, P.; Yang, J.; Ma, R.; Yan, X.-E.; Yang, S.-Y.; Yang, J.-W.; Yun, C.-H. Structural insights into drug development strategy targeting EGFR T790M/C797S. Oncotarget 2018, 9, 13652–13665. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.J.; Shaw, A.T. Resisting resistance: Targeted therapies in lung cancer. Trends Cancer 2016, 2, 350–364. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Wang, J.; Zeng, Y.; Zhang, X.; Hu, Q.; Zheng, J.; Chen, B.; Xie, B.; Zhang, W.-M. Implication of epithelial-mesenchymal transition in IGF1R-induced resistance to EGFR-TKIs in advanced non-small cell lung cancer. Oncotarget 2015, 6, 44332–44345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santoni-Rugiu, E.; Melchior, L.C.; Urbanska, E.M.; Jakobsen, J.N.; Stricker, K.; Grauslund, M.; Sørensen, J.B. Intrinsic resistance to EGFR-Tyrosine Kinase Inhibitors in EGFR-Mutant Non-Small Cell Lung Cancer: Differences and Similarities with Acquired Resistance. Cancers 2019, 11, 923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellanos, E.; Feld, E.; Horn, L. Driven by mutations: The predictive value of mutation subtype in EGFR-mutated non-small cell lung cancer. J. Thorac. Oncol. 2017, 12, 612–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, C.; Sousa, C.; Machado, F.; Serino, M.; Santos, V.; Cruz-Martins, N.; Teixeira, A.; Cunha, A.; Pereira, T.; Oliveira, H.P.; et al. The role of liquid biopsy in early diagnosis of lung cancer. Front. Oncol. 2021, 11, 634316. [Google Scholar] [CrossRef]
- Lettig, L.; Sahnane, N.; Pepe, F.; Cerutti, R.; Albeni, C.; Franzi, F.; Veronesi, G.; Ogliari, F.; Pastore, A.; Tuzi, A.; et al. EGFR T790M detection rate in lung adenocarcinomas at baseline using droplet digital PCR and validation by ultra-deep next generation sequencing. Transl. Lung Cancer Res. 2019, 8, 584–592. [Google Scholar] [CrossRef]
- Saarenheimo, J.; Andersen, H.; Eigeliene, N.; Jekunen, A.P. Current challenges in applying gene-driven therapies in clinical lung cancer practice. World J. Clin. Oncol. 2021, 12, 656–663. [Google Scholar] [CrossRef]
- Liang, H.; Li, C.; Zhao, Y.; Zhao, S.; Huang, J.; Cai, X.; Cheng, B.; Xiong, S.; Li, J.; Wang, W.; et al. Concomitant mutations in EGFR 19Del/L858R mutation and their association with response to EGFR-TKIs in NSCLC patients. Cancer Manag. Res. 2020, 12, 8653–8662. [Google Scholar] [CrossRef]
- Inukai, M.; Toyooka, S.; Ito, S.; Asano, H.; Ichihara, S.; Soh, J.; Suehisa, H.; Ouchida, M.; Aoe, K.; Aoe, M.; et al. Presence of epidermal growth factor receptor gene T790M mutation as a minor clone in non-small cell lung cancer. Cancer Res. 2006, 66, 7854–7858. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, S.S.; Yang, J.C.-H.; Lee, C.K.; Kurata, T.; Kim, D.-W.; John, T.; Nogami, N.; Ohe, Y.; Mann, H.; Rukazenkov, Y.; et al. Osimertinib as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer. J. Clin. Oncol. 2018, 36, 841–849. [Google Scholar] [CrossRef] [Green Version]
- Ohe, Y.; Imamura, F.; Nogami, N.; Okamoto, I.; Kurata, T.; Kato, T.; Sugawara, S.; Ramalingam, S.S.; Uchida, H.; Hodge, R.; et al. Osimertinib versus standard-of-care EGFR-TKI as first-line treatment for EGFRm advanced NSCLC: FLAURA Japanese subset. Jpn. J. Clin. Oncol. 2019, 49, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Boyer, M.J.; Lee, J.-S.; Dechaphunkul, A.; Cheema, P.K.; Takahashi, T.; Gray, J.E.; Tiseo, M.; Ramalingam, S.S.; Todd, A.; et al. Postprogression outcomes for osimertinib versus standard-of-care EGFR-TKI in patients with previously untreated EGFR-mutated advanced non-small cell lung cancer. Clin. Cancer Res. 2019, 25, 2058–2063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, T.F.; Borghaei, H.; Ramalingam, S.S.; Mok, T.S.; Peters, S. Targeting KRAS-mutant non-small-cell lung cancer: One mutation at a time, with a focus on KRAS G12C mutations. J. Clin. Oncol. 2020, 38, 4208–4218. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhao, J. KRAS oncogene may be another target conquered in non-small cell lung cancer (NSCLC). Thorac. Cancer 2020, 11, 3425–3435. [Google Scholar] [CrossRef] [PubMed]
- Blair, H.A. Sotorasib: First Approval. Drugs 2021, 81, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.D.; Alexandrov, A.; Kim, J.; Wala, J.; Berger, A.H.; Pedamallu, C.S.; Shukla, S.A.; Guo, G.; Brooks, A.N.; Murray, B.A.; et al. Distinct patterns of somatic genome alterations in lung adenocarcinomas and squamous cell carcinomas. Nat. Genet. 2016, 48, 607–616. [Google Scholar] [CrossRef] [Green Version]
- Jamal-Hanjani, M.; Wilson, G.A.; McGranahan, N.; Birkbak, N.J.; Watkins, T.B.K.; Veeriah, S.; Shafi, S.; Johnson, D.H.; Mitter, R.; Rosenthal, R.; et al. Tracking the evolution of non-small-cell lung cancer. N. Engl. J. Med. 2017, 376, 2109–2121. [Google Scholar] [CrossRef] [Green Version]
- Morcos, P.; Thapar, N.; Tusneem, N.; Stacey, D.; Tamanoi, F. Identification of neurofibromin mutants that exhibit allele specificity or increased Ras affinity resulting in suppression of activated ras alleles. Mol. Cell. Biol. 1996, 16, 2496–2503. [Google Scholar] [CrossRef] [Green Version]
- Kastnerova, L.; Martinek, P.; Grossmann, P.; Steiner, P.; Vanecek, T.; Kyclova, J.; Ferak, I.; Zalud, R.; Slehobr, O.; Svajdler, P.; et al. A clinicopathological study of 29 spitzoid melanocytic lesions with ALK fusions, including novel fusion variants, accompanied by fluorescence in situ hybridization analysis for chromosomal copy number changes, and both TERT promoter and next-generation sequencing mutation analysis. Am. J. Dermatopathol. 2020, 42, 578–592. [Google Scholar] [CrossRef]
- Hillen, U.; Grabellus, F.; Franklin, C.; Sucker, A.; Schadendorf, D.; Schilling, B. Oncogene status of an interdigitating dendritic cell sarcoma: Recurrent mutations in NF1, TP53, and ARID2 shared with melanoma: Recurrent mutations in NF1, TP53, and ARID2 shared with melanoma. Am. J. Surg. Pathol. 2016, 40, 1721–1723. [Google Scholar] [CrossRef]
- Pivovarcikova, K.; Agaimy, A.; Martinek, P.; Alaghehbandan, R.; Perez-Montiel, D.; Alvarado-Cabrero, I.; Rogala, J.; Kuroda, N.; Rychly, B.; Gasparov, S.; et al. Primary renal well-differentiated neuroendocrine tumour (carcinoid): Next-generation sequencing study of 11 cases: Next-generation sequencing of renal carcinoid. Histopathology 2019, 75, 104–117. [Google Scholar] [CrossRef]
- Tlemsani, C.; Pécuchet, N.; Gruber, A.; Laurendeau, I.; Danel, C.; Riquet, M.; Le Pimpec-Barthes, F.; Fabre, E.; Mansuet-Lupo, A.; Damotte, D.; et al. NF1 mutations identify molecular and clinical subtypes of lung adenocarcinomas. Cancer Med. 2019, 8, 4330–4337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruin, E.C.; Cowell, C.; Warne, P.H.; Jiang, M.; Saunders, R.E.; Melnick, M.A.; Gettinger, S.; Walther, Z.; Wurtz, A.; Heynen, G.J.; et al. Reduced NF1 expression confers resistance to EGFR inhibition in lung cancer. Cancer Discov. 2014, 4, 606–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No. | % | Variables | No. | % |
|---|---|---|---|---|---|
| Patients | 86 | Pathological stage | |||
| Male | 35 | 40.70 | I | 2 | 2.33 |
| Female | 51 | 59.30 | III | 6 | 6.98 |
| Age (yr) | IV | 77 | 89.53 | ||
| Mean (range) | 66.45 (36–89) | ND | 1 | 1.16 | |
| Histology | Smoking | ||||
| Adenocarcinoma | 74 | 86.05 | No | 38 | 44.19 |
| Squamous cell carcinoma | 3 | 3.49 | Former smoker | 28 | 32.56 |
| Other NSCLC | 9 | 10.47 | Yes | 16 | 18.60 |
| ND | 4 | 4.65 | |||
| No. | Initial EGFR Mutation | Rebiopsy 1 | Rebiopsy 2 | LB1 | LB2 | LB3 | LB4 | LB5 | LB6 | LB7 | No. | Initial EGFR Mutation | Rebiopsy 1 | LB1 | LB2 | LB3 | LB4 | LB5 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ex19Del | NMD | NMD | 43 | Ex19Del | Ex19Del | ||||||||||||
| 5 | Ex19Del | T790M | NMD | 44 | L858R | NMD | L858R | NMD | NMD | |||||||||
| 6 | Ex19Del | Ex19Del | Ex19Del T790M | 46 | L858R | L858R | ||||||||||||
| 7 | Ex19Del | NMD | NMD | NMD | NMD | NMD | NMD | Ex19Del | Ex19Del | 47 | S768I | NMD | NMD | |||||
| 8 | Ex19Del | Ex19Del | Ex19Del T790M | 50 | Ex19Del | Ex19Del T790M | ||||||||||||
| 9 | Ex19Del | NMD | Ex19Del T790M | 52 | L858R | L858R | NMD | NMD | L858R T790M | |||||||||
| 10 | L858R | L858R | 53 | Ex19Del | NMD | Ex19Del T790M | Ex19Del T790M | |||||||||||
| 11 | L858R | NMD | L858R | L858R | 54 | L858R T790M | L858R T790M | T790M | T790M | T790M | ||||||||
| 13 | Ex19Del | NMD | Ex19Del | Ex19Del T790M | 55 | L858R | L858R T790M | NMD | L858R | |||||||||
| 15 | Ex19Del | Ex19Del T790M | 56 | L858R | L858R | L858R | ||||||||||||
| 20 | S768I, L858R | S768I | NMD | S768I L858R T790M | 59 | L858R | L858R T790M | L858R | INV | L858R | L858R | |||||||
| 22 | Ex19Del | Ex19Del | NMD | NMD | NMD | 60 | L858R | NMD | L858R T790M | |||||||||
| 23 | Ex19Del | NMD | Ex19Del T790M | Ex19Del | Ex19Del T790M | 62 | Ex19Del | NMD | ||||||||||
| 24 | Ex20Ins | NMD | 63 | Ex19Del | NMD | NMD | NMD | NMD | NMD | |||||||||
| 27 | L858R | L858R T790M | 65 | Ex19Del | NMD | NMD | NMD | |||||||||||
| 28 | ND | INV | Ex19Del | Ex19Del | 66 | ND | Ex19Del T790M | Ex19Del | Ex19Del | |||||||||
| 30 | L858R | L858R | L858R | L858R | INV | INV | 67 | L858R | NMD | |||||||||
| 31 | L858R | L858R | 69 | G719X S768I | NMD | |||||||||||||
| 32 | Ex19Del | Ex19Del T790M | 70 | Ex19Del | Ex19Del T790M | Ex19Del | ||||||||||||
| 33 | L858R | L858R T790M | NMD | NMD | L858R | 73 | Ex19Del | NMD | ||||||||||
| 34 | Ex19Del | Ex19Del T790M | 74 | ND | Ex19Del | NMD | ||||||||||||
| 35 | ND | L858R T790M | L858R | NMD | NMD | 79 | Ex19Del | NMD | NMD | NMD | ||||||||
| 36 | Ex19Del | Ex19Del | 80 | L858R | L858R T790M | L858R | NMD | NMD | ||||||||||
| 37 | Ex19Del | NMD | NMD | NMD | 81 | Ex19Del | T790M | |||||||||||
| 38 | L858R | L858R | 82 | L858R | NMD | |||||||||||||
| 39 | G719X | NMD | NMD | 83 | Ex19Del | Ex19Del T790M | ||||||||||||
| 40 | L858R | L858R T790M | NMD | L858R | 84 | ND | L858R | L858R | ||||||||||
| 41 | Ex19Del | NMD | NMD | INV | NMD | NMD | NMD | NMD | NMD | 85 | ND | L858R | ||||||
| 42 | Ex19Del | Ex19Del T790M | Ex19Del | NMD | NMD | 86 | L858R | L858R T790M |
| Ex19Del IM | L858R IM | Ex19Del LB | L858R LB | T790M LB | Ex19Del ReBx | L858R ReBx | T790M ReBx | |
|---|---|---|---|---|---|---|---|---|
| Ex19Del IM | φ: −0.385 *** | φ: 0.637 *** | φ: −0.385 *** | φ: 0.329 ** | φ: 0.110 ns | φ: −0.217 * | φ: −0.011 ns | |
| L858R IM | φ: −0.292 ** | φ: 0.811 *** | φ: 0.107 ns | φ: −0.156 ns | φ: 0.470 *** | φ: 0.300 ** | ||
| Ex19Del LB | φ: −0.292 ** | φ: 0.438 *** | φ: 0.308 ** | φ: −0.165 ns | φ: 0.081 ns | |||
| L858R LB | φ: 0.107 ns | φ: −0.156 ns | φ: 0.470 *** | φ: 0.216 * | ||||
| T790M LB | φ: −0.191 ns | φ: −0.066 ns | φ: −0.097 ns | |||||
| Ex19Del ReBx | φ: −0.088 ns | φ: 0.328 ** | ||||||
| L858R ReBx | φ: 0.633 *** | |||||||
| T790M ReBx |
| No. | Months | 1st LB | TKI Treat | Months | Subsequent LBs | TKI Treat | Rebiopsy | Exitus | No. | Months | 1st LB | TKI Treat | Months | Subsequent LBs | TKI Treat | Rebiopsy | Exitus |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 37.2 | 0 | 1 | 4.2 | 0 | 1 | 5.3 | 44 | 4.9 | 0 | 1 | 50.7 | 1 | 1 | |||
| 5 | 20.0 | 0 | 3 | T790M | 10.5 | 46 | 5.6 | 1 | 1 | 4.8 | |||||||
| 7 | 5.7 | 0 | 3 | 27.1 | 1 | 1 | NMD | 2.3 | 47 | 32.9 | 0 | 0 | 31 | 0 | 3 | 11.1 | |
| 8 | 35.8 | 1 | 1 | 0.2 | 1 | 0 | 0.3 | 50 | 31.7 | 2 | 3 | ||||||
| 9 | 14.9 | 0 | 1 | 0.2 | 2 | 2 | 22.4 | 52 | 17.1 | 0 | 1 | 21.4 | 2 | 3 | 37.2 | ||
| 10 | 1.8 | 1 | 1 | 1.0 | 53 | 21.8 | 0 | 1 | 32.5 | 2 | 2 | 3.6 | |||||
| 11 | 4.0 | 0 | 1 | 5.6 | 1 | 1 | 0.6 | 56 | 8.6 | 1 | 2 | 2.2 | 1 | 2 | 1.4 | ||
| 13 | 15.7 | 0 | 1 | 14.3 | 2 | 3 | 38.1 | 59 | 26.2 | 1 | 1 | 3.0 | 1 | 2 | L858R T790M | 15.5 | |
| 15 | 8.0 | 2 | 1 | 0.5 | 60 | 8.9 | 0 | 1 | 3.1 | 2 | 2 | 24.8 | |||||
| 20 | 11.0 | 0 | 1 | 16.4 | 2 | 2 | 27.2 | 62 | 17.5 | 0 | 2 | 2.2 | |||||
| 23 | 11.9 | 0 | 1 | 35.9 | 2 | 2 | 6.6 | 63 | 5.3 | 0 | 1 | 22.1 | 0 | 2 | |||
| 27 | 11.7 | 2 | 3 | 14.5 | 65 | 37.4 | 0 | 1 | 10.2 | 0 | 1 | NMD | 5.0 | ||||
| 30 | 9.5 | 1 | 1 | 5.0 | 1 | 0 | L858R | 0.7 | 67 | 13.9 | 0 | 1 | 3.7 | ||||
| 31 | 4.87 | 1 | 2 | 2.0 | 69 | 11.8 | 0 | 1 | 21.8 | ||||||||
| 32 | 10.0 | 2 | 3 | 7.8 | 70 | 9.2 | 1 | 2 | Ex19Del T790M | 12.2 | |||||||
| 33 | 38.4 | 1 | 1 | 19.9 | 1 | 2 | L858R T790M | 79 | 62.1 | 0 | 1 | 20.3 | 0 | 1 | |||
| 36 | 9.2 | 1 | 1 | 3.3 | 80 | 57.1 | 1 | 1 | 0.5 | 0 | 2 | L858R T790M | |||||
| 37 | 20.5 | 0 | 1 | 0.5 | 0 | 0 | 7.9 | 81 | 21.0 | 2 | 3 | ||||||
| 38 | 15.1 | 1 | 1 | 3.03 | 82 | 12.2 | 0 | 0 | |||||||||
| 39 | 2.0 | 0 | 1 | 6.2 | 83 | 16.7 | 2 | 3 | 13.8 | ||||||||
| 43 | 2.0 | 1 | 1 | 1.3 | 86 | 18.3 | 2 | 2 |
| A | Censored | B | Censored | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mut Status | N Total | N Exitus | N | % | Mut Status | N Total | N Exitus | N | % |
| Wild Type | 28 | 23 | 5 | 17.9% | T790M- | 58 | 45 | 13 | 22.4% |
| EGFR+ | 58 | 45 | 13 | 22.4% | T790M+ | 28 | 23 | 5 | 17.9% |
| Global | 86 | 68 | 18 | 20.9% | Global | 86 | 68 | 18 | 20.9% |
| Censored | ||||
|---|---|---|---|---|
| Mut Status | N Total | N Exitus | N | % |
| No TKIs | 27 | 21 | 6 | 22.2% |
| 1st–2nd Generation | 24 | 20 | 4 | 16.7% |
| 3rd Generation | 35 | 27 | 8 | 22.9% |
| Global | 86 | 68 | 18 | 20.9% |
| No. | Type of Sample | Pan Lung Cancer Panel | cobas EGFR Mutation Test |
|---|---|---|---|
| Mutation Detected | Mutation Detected | ||
| 1 | Liquid biopsy | Negative | Negative |
| 5 | Rebiopsy | T790M | T790M |
| 7 | Rebiopsy | KRAS G12A/V/R/G13C * | Negative |
| 22 | Liquid biopsy | Negative | Negative |
| 30 | Rebiopsy | L858R | L858R |
| 31 | Liquid biopsy | L858R | L858R |
| 33 | Rebiopsy | L858R T790M | L858R T790M |
| 35 | Liquid biopsy | Negative | Negative |
| 37 | Liquid biopsy | Negative | Negative |
| 54 | Rebiopsy | L858R T790M | L858R T790M |
| 56 | Liquid biopsy | Negative | Negative |
| 65 | Rebiopsy | KRAS G12C * | Negative |
| 70 | Rebiopsy | Ex19Del T790M | Ex19Del T790M |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alen, B.O.; Estévez-Pérez, L.S.; Hermida-Romero, M.T.; Reguera-Arias, A.; García-Campelo, R.; de la Torre-Bravos, M.; Concha, Á. Molecular Targets in Lung Cancer: Study of the Evolution of Biomarkers Associated with Treatment with Tyrosine Kinase Inhibitors—Has NF1 Tumor Suppressor a Key Role in Acquired Resistance? Cancers 2022, 14, 3323. https://doi.org/10.3390/cancers14143323
Alen BO, Estévez-Pérez LS, Hermida-Romero MT, Reguera-Arias A, García-Campelo R, de la Torre-Bravos M, Concha Á. Molecular Targets in Lung Cancer: Study of the Evolution of Biomarkers Associated with Treatment with Tyrosine Kinase Inhibitors—Has NF1 Tumor Suppressor a Key Role in Acquired Resistance? Cancers. 2022; 14(14):3323. https://doi.org/10.3390/cancers14143323
Chicago/Turabian StyleAlen, Begoña O., Lara S. Estévez-Pérez, María Teresa Hermida-Romero, Ana Reguera-Arias, Rosario García-Campelo, Mercedes de la Torre-Bravos, and Ángel Concha. 2022. "Molecular Targets in Lung Cancer: Study of the Evolution of Biomarkers Associated with Treatment with Tyrosine Kinase Inhibitors—Has NF1 Tumor Suppressor a Key Role in Acquired Resistance?" Cancers 14, no. 14: 3323. https://doi.org/10.3390/cancers14143323