
Diffusion Microstructure Imaging to Analyze Perilesional T2 Signal Changes in Brain Metastases and Glioblastomas

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
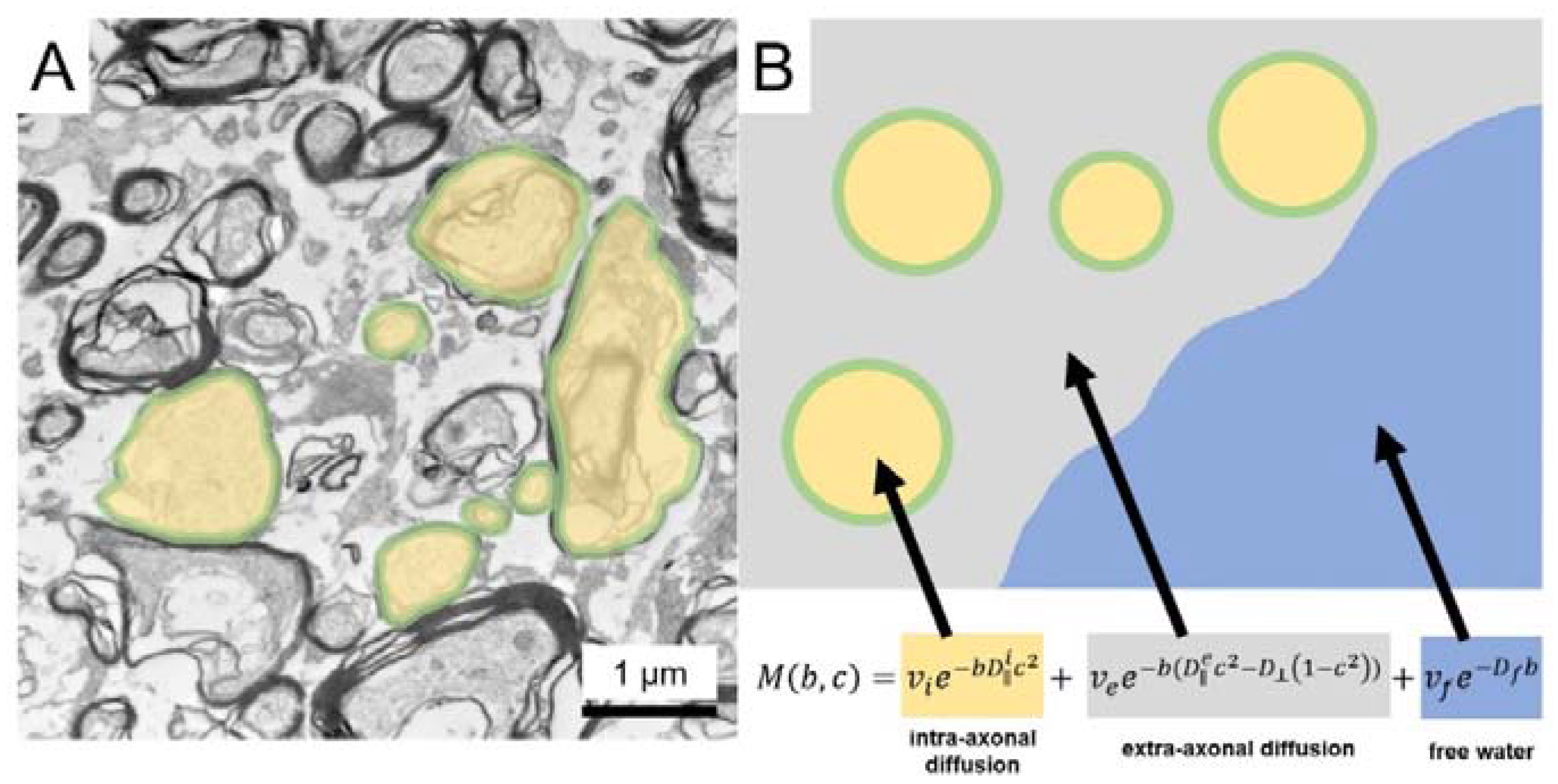
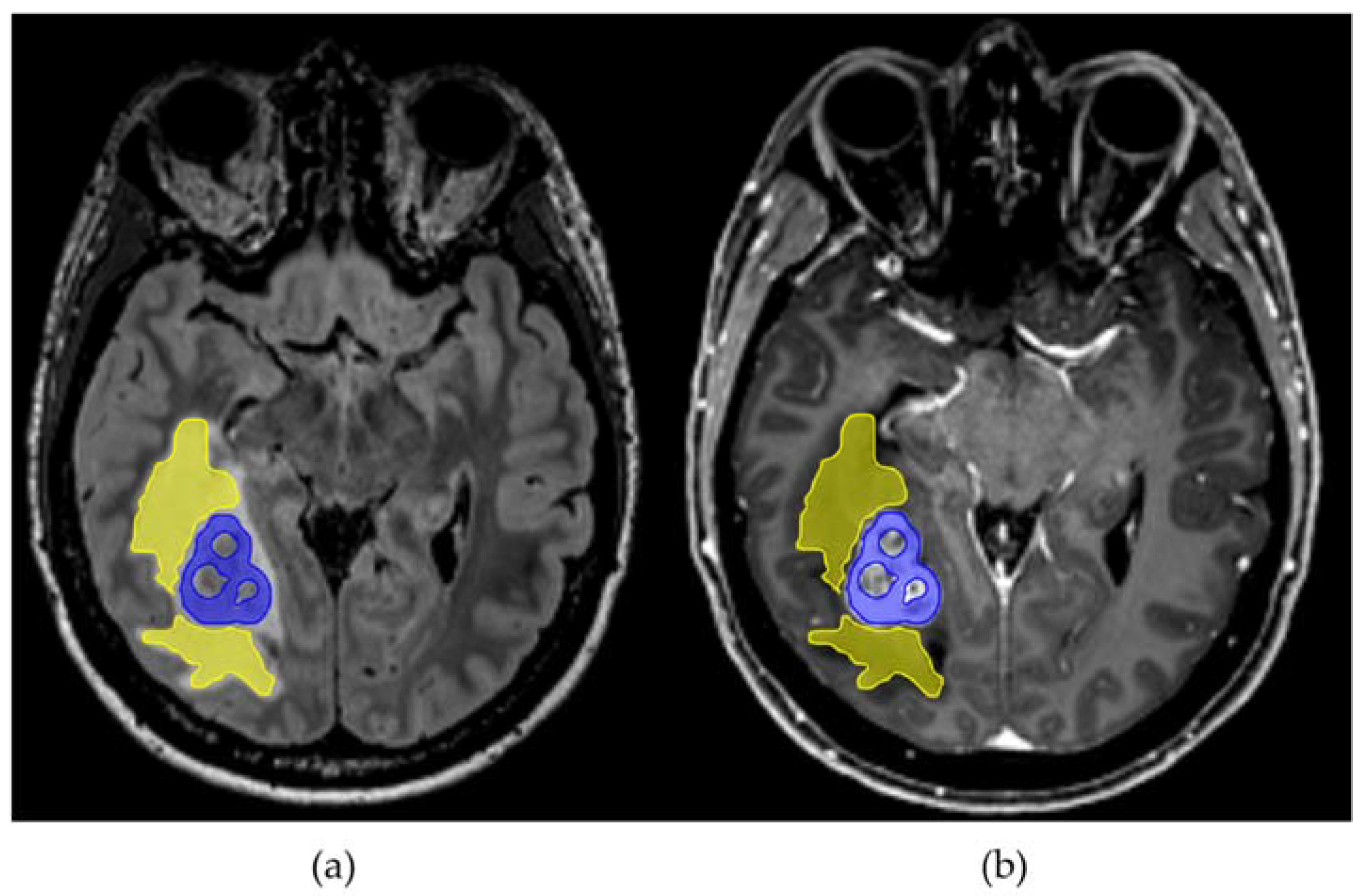
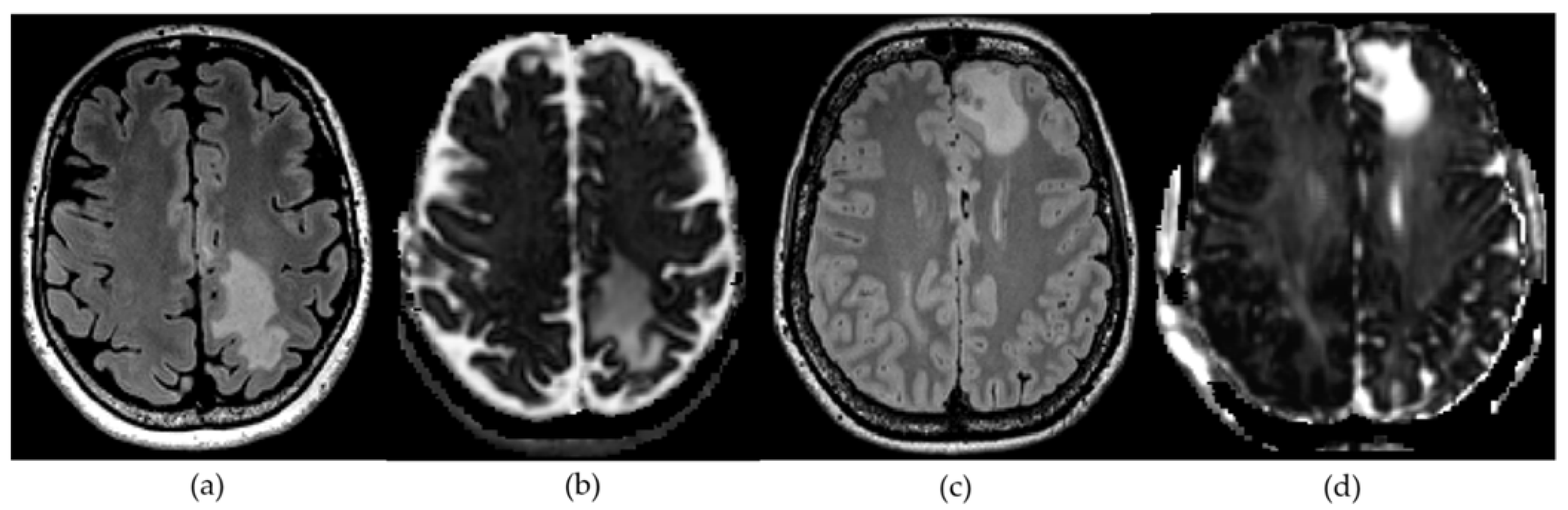
2.2. Diffusion Microstructure Imaging (DMI) and ROI Based Analysis
2.3. Histopathology
Statistical Analysis
3. Results
3.1. Study Population
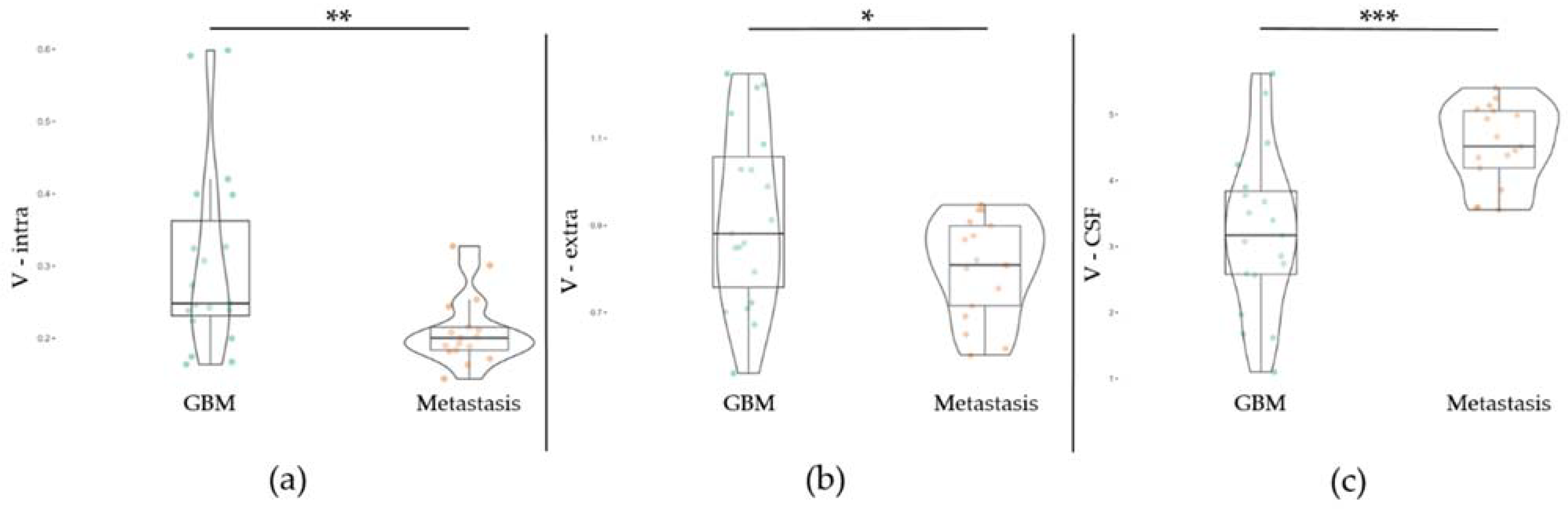
3.2. Diffusion Metrics in Brain Metastasis and GBM
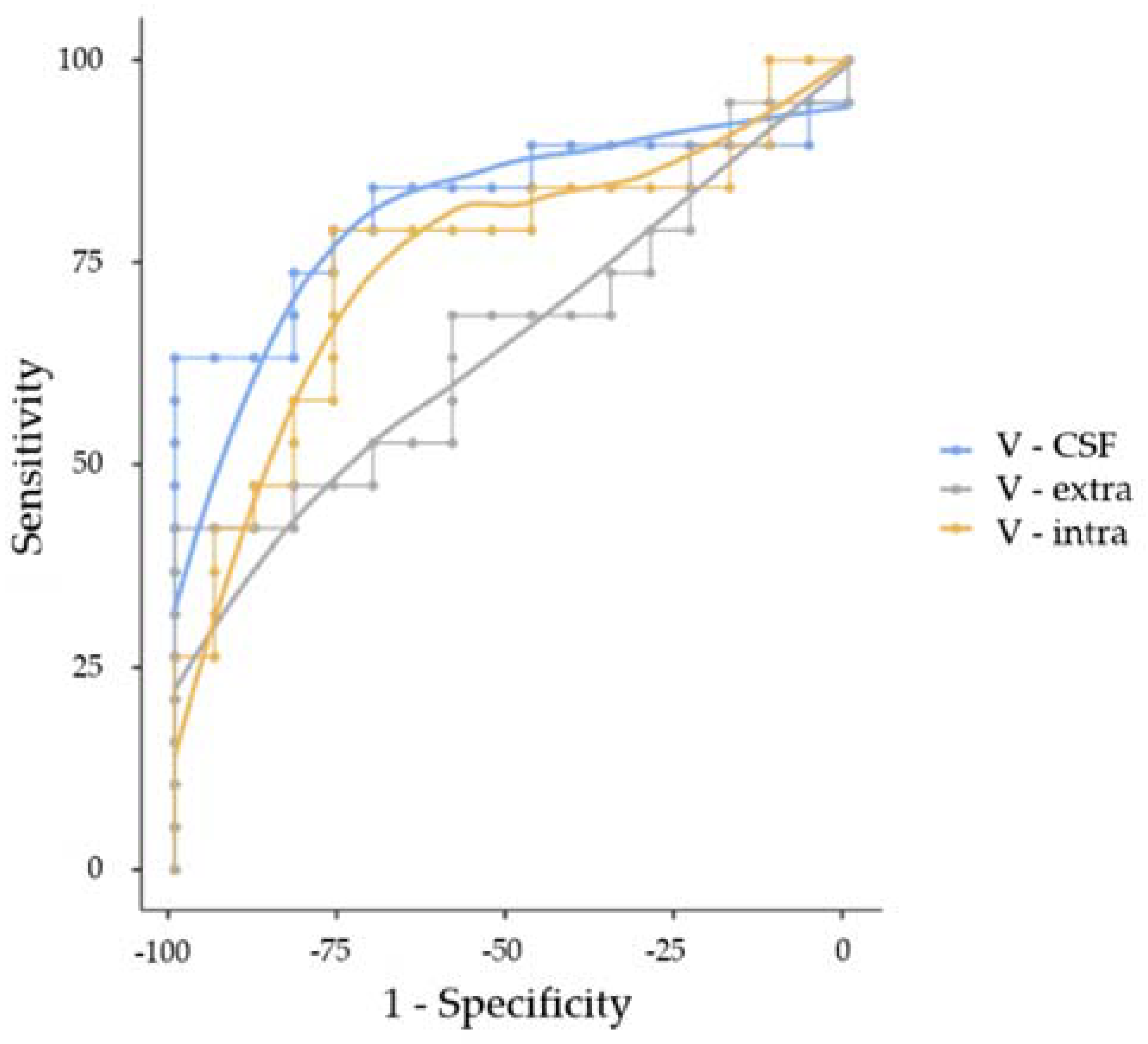
3.3. Correlation and ROC Analysis
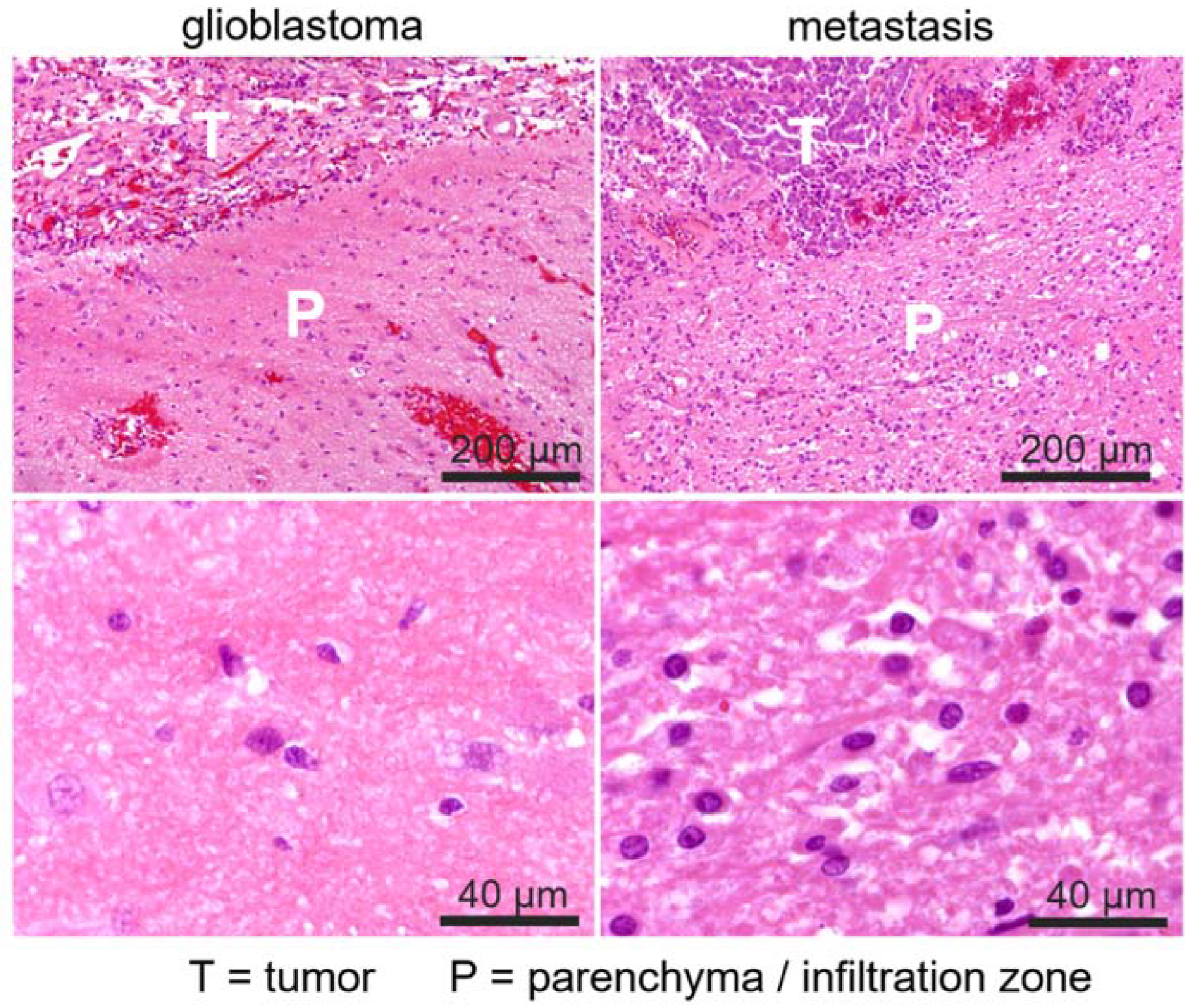
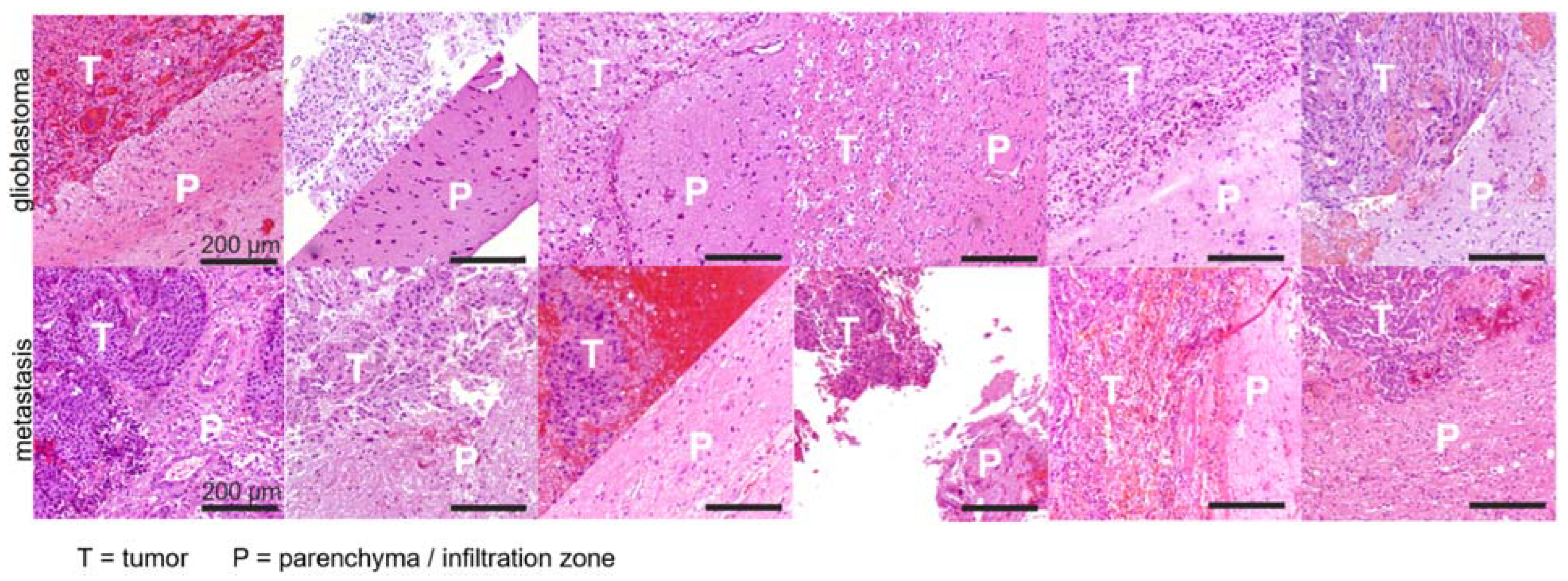
3.4. Histopathology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro-Oncology 2021, 23, iii1–iii105. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Bette, S.; Barz, M.; Huber, T.; Straube, C.; Schmidt-Graf, F.; Combs, S.E.; Delbridge, C.; Gerhardt, J.; Zimmer, C.; Meyer, B.; et al. Retrospective Analysis of Radiological Recurrence Patterns in Glioblastoma, Their Prognostic Value And Association to Postoperative Infarct Volume. Sci. Rep. 2018, 8, 4561. [Google Scholar] [CrossRef]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of Brain Metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef]
- Malone, H.; Yang, J.; Hershman, D.L.; Wright, J.D.; Bruce, J.N.; Neugut, A.I. Complications Following Stereotactic Needle Biopsy of Intracranial Tumors. World Neurosurg. 2015, 84, 1084–1089. [Google Scholar] [CrossRef]
- Kepes, J.J. Pitfalls and Problems in the Histopathologic Evaluation of Stereotactic Needle Biopsy Specimens. Neurosurg. Clin. N. Am. 1994, 5, 19–33. [Google Scholar] [CrossRef]
- Zhang, H.; Schneider, T.; Wheeler-Kingshott, C.A.; Alexander, D.C. NODDI: Practical in Vivo Neurite Orientation Dispersion and Density Imaging of the Human Brain. NeuroImage 2012, 61, 1000–1016. [Google Scholar] [CrossRef]
- Reisert, M.; Kellner, E.; Dhital, B.; Hennig, J.; Kiselev, V.G. Disentangling Micro from Mesostructure by Diffusion MRI: A Bayesian Approach. NeuroImage 2017, 147, 964–975. [Google Scholar] [CrossRef] [Green Version]
- Sternberg, E.J.; Lipton, M.L.; Burns, J. Utility of Diffusion Tensor Imaging in Evaluation of the Peritumoral Region in Patients with Primary and Metastatic Brain Tumors. AJNR Am. J. Neuroradiol. 2014, 35, 439–444. [Google Scholar] [CrossRef] [Green Version]
- Jiang, R.; Du, F.-Z.; He, C.; Gu, M.; Ke, Z.-W.; Li, J.-H. The Value of Diffusion Tensor Imaging in Differentiating High-Grade Gliomas from Brain Metastases: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e112550. [Google Scholar] [CrossRef]
- Wang, W.; Steward, C.E.; Desmond, P.M. Diffusion Tensor Imaging in Glioblastoma Multiforme and Brain Metastases: The Role of p, q, L, and Fractional Anisotropy. AJNR Am. J. Neuroradiol. 2009, 30, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.M.; Suki, D.; Hess, K.; Sawaya, R. The Influence of Maximum Safe Resection of Glioblastoma on Survival in 1229 Patients: Can We Do Better than Gross-Total Resection? J. Neurosurg. 2016, 124, 977–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, P.J.; Daumas-Duport, C.; Scheithauer, B.W.; Kall, B.A.; Kispert, D.B. Stereotactic Histologic Correlations of Computed Tomography- and Magnetic Resonance Imaging-Defined Abnormalities in Patients with Glial Neoplasms. Mayo Clin. Proc. 1987, 62, 450–459. [Google Scholar] [CrossRef]
- Caravan, I.; Ciortea, C.A.; Contis, A.; Lebovici, A. Diagnostic Value of Apparent Diffusion Coefficient in Differentiating between High-Grade Gliomas and Brain Metastases. Acta Radiol. Stockh. Swed. 1987 2018, 59, 599–605. [Google Scholar] [CrossRef]
- Van Westen, D.; Lätt, J.; Englund, E.; Brockstedt, S.; Larsson, E.M. Tumor Extension in High-Grade Gliomas Assessed with Diffusion Magnetic Resonance Imaging: Values and Lesion-to-Brain Ratios of Apparent Diffusion Coefficient and Fractional Anisotropy. Acta Radiol. Stockh. Swed. 1987 2006, 47, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Zeng, W.; Zhang, Q.; Yang, Z.; Yan, X.; Zhang, H.; Wang, M.; Yang, G.; Zhou, M.; Shen, J. Differentiation between High-Grade Gliomas and Solitary Brain Metastases: A Comparison of Five Diffusion-Weighted MRI Models. BMC Med. Imaging 2020, 20, 124. [Google Scholar] [CrossRef]
- Novikov, D.S.; Veraart, J.; Jelescu, I.O.; Fieremans, E. Rotationally-Invariant Mapping of Scalar and Orientational Metrics of Neuronal Microstructure with Diffusion MRI. NeuroImage 2018, 174, 518–538. [Google Scholar] [CrossRef]
- Rau, A.; Reisert, M.; Kellner, E.; Hosp, J.A.; Urbach, H.; Demerath, T. Increased Interstitial Fluid in Periventricular and Deep White Matter Hyperintensities in Patients with Suspected Idiopathic Normal Pressure Hydrocephalus. Sci. Rep. 2021, 11, 19552. [Google Scholar] [CrossRef]
- Demerath, T.; Donkels, C.; Reisert, M.; Heers, M.; Rau, A.; Schröter, N.; Schulze-Bonhage, A.; Reinacher, P.; Scheiwe, C.; Shah, M.J.; et al. Gray-White Matter Blurring of the Temporal Pole Associated With Hippocampal Sclerosis: A Microstructural Study Involving 3 T MRI and Ultrastructural Histopathology. Cereb. Cortex 2021, bhab320. [Google Scholar] [CrossRef]
- Veraart, J.; Novikov, D.S.; Christiaens, D.; Ades-Aron, B.; Sijbers, J.; Fieremans, E. Denoising of Diffusion MRI Using Random Matrix Theory. NeuroImage 2016, 142, 394–406. [Google Scholar] [CrossRef] [Green Version]
- Kellner, E.; Dhital, B.; Kiselev, V.G.; Reisert, M. Gibbs-Ringing Artifact Removal Based on Local Subvoxel-Shifts. Magn. Reson. Med. 2016, 76, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, E.; Leila, M.C.C.; Brian, H.; James, S.L. Neuropathology: A Reference Text of CNS Pathology, 3rd ed.; Get Full Access and More at ExpertConsult.Com; Ellison, D., Ed.; Elsevier: Edinburgh, UK, 2013; ISBN 978-0-7234-3515-0. [Google Scholar]
- Pekmezci, M.; Perry, A. Neuropathology of Brain Metastases. Surg. Neurol. Int. 2013, 4, S245–S255. [Google Scholar] [CrossRef]
- Eidel, O.; Burth, S.; Neumann, J.-O.; Kieslich, P.J.; Sahm, F.; Jungk, C.; Kickingereder, P.; Bickelhaupt, S.; Mundiyanapurath, S.; Bäumer, P.; et al. Tumor Infiltration in Enhancing and Non-Enhancing Parts of Glioblastoma: A Correlation with Histopathology. PLoS ONE 2017, 12, e0169292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, S.; Ahn, D.; Johnson, G.; Law, M.; Zagzag, D.; Grossman, R.I. Diffusion-Tensor MR Imaging of Intracranial Neoplasia and Associated Peritumoral Edema: Introduction of the Tumor Infiltration Index. Radiology 2004, 232, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Bette, S.; Huber, T.; Wiestler, B.; Boeckh-Behrens, T.; Gempt, J.; Ringel, F.; Meyer, B.; Zimmer, C.; Kirschke, J.S. Analysis of Fractional Anisotropy Facilitates Differentiation of Glioblastoma and Brain Metastases in a Clinical Setting. Eur. J. Radiol. 2016, 85, 2182–2187. [Google Scholar] [CrossRef]
- Machein, M.R.; Plate, K.H. VEGF in Brain Tumors. J. Neurooncol. 2000, 50, 109–120. [Google Scholar] [CrossRef]
- Pietsch, T.; Valter, M.M.; Wolf, H.K.; von Deimling, A.; Huang, H.J.; Cavenee, W.K.; Wiestler, O.D. Expression and Distribution of Vascular Endothelial Growth Factor Protein in Human Brain Tumors. Acta Neuropathol. 1997, 93, 109–117. [Google Scholar] [CrossRef]
- Strugar, J.G.; Criscuolo, G.R.; Rothbart, D.; Harrington, W.N. Vascular Endothelial Growth/Permeability Factor Expression in Human Glioma Specimens: Correlation with Vasogenic Brain Edema and Tumor-Associated Cysts. J. Neurosurg. 1995, 83, 682–689. [Google Scholar] [CrossRef] [Green Version]
- Nghiemphu, P.L.; Liu, W.; Lee, Y.; Than, T.; Graham, C.; Lai, A.; Green, R.M.; Pope, W.B.; Liau, L.M.; Mischel, P.S.; et al. Bevacizumab and Chemotherapy for Recurrent Glioblastoma: A Single-Institution Experience. Neurology 2009, 72, 1217–1222. [Google Scholar] [CrossRef] [Green Version]
- Seidel, C.; Dörner, N.; Osswald, M.; Wick, A.; Platten, M.; Bendszus, M.; Wick, W. Does Age Matter?—A MRI Study on Peritumoral Edema in Newly Diagnosed Primary Glioblastoma. BMC Cancer 2011, 11, 127. [Google Scholar] [CrossRef] [Green Version]
- Sahm, F.; Capper, D.; Jeibmann, A.; Habel, A.; Paulus, W.; Troost, D.; von Deimling, A. Addressing Diffuse Glioma as a Systemic Brain Disease with Single-Cell Analysis. Arch. Neurol. 2012, 69, 523–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuoco, J.A.; Klein, B.J.; Busch, C.M.; Guilliams, E.L.; Olasunkanmi, A.L.; Entwistle, J.J. Corticosteroid-Induced Regression of Glioblastoma: A Radiographic Conundrum. Front. Oncol. 2019, 9, 1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Heading | GBM | Metastasis | p-Value |
|---|---|---|---|
| n | 19 | 17 | |
| Sex (m/f) | 10/9 | 9/8 | |
| Age (years) (SD) | 66.4 (14.1) | 63.5 (11.8) | p = 0.509 |
| Perifocal T2 volume (ml) (IQR) | 20.7 (22.1) | 19.5 (35.1) | p = 0.925 |
| Presurgical steroid treatment | 7/19 (36.8%) | 6/17 (35.3%) | |
| V-intra (IQR) | 0.25 (0.13) | 0.20 (0.03) | p = 0.006 |
| V-extra (IQR) | 0.88 (0.30) | 0.81 (0.18) | p = 0.024 |
| V-CSF (IQR) | 3.17 (1.26) | 4.52 (0.86) | p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Würtemberger, U.; Diebold, M.; Erny, D.; Hosp, J.A.; Schnell, O.; Reinacher, P.C.; Rau, A.; Kellner, E.; Reisert, M.; Urbach, H.; et al. Diffusion Microstructure Imaging to Analyze Perilesional T2 Signal Changes in Brain Metastases and Glioblastomas. Cancers 2022, 14, 1155. https://doi.org/10.3390/cancers14051155
Würtemberger U, Diebold M, Erny D, Hosp JA, Schnell O, Reinacher PC, Rau A, Kellner E, Reisert M, Urbach H, et al. Diffusion Microstructure Imaging to Analyze Perilesional T2 Signal Changes in Brain Metastases and Glioblastomas. Cancers. 2022; 14(5):1155. https://doi.org/10.3390/cancers14051155
Chicago/Turabian StyleWürtemberger, Urs, Martin Diebold, Daniel Erny, Jonas A. Hosp, Oliver Schnell, Peter C. Reinacher, Alexander Rau, Elias Kellner, Marco Reisert, Horst Urbach, and et al. 2022. "Diffusion Microstructure Imaging to Analyze Perilesional T2 Signal Changes in Brain Metastases and Glioblastomas" Cancers 14, no. 5: 1155. https://doi.org/10.3390/cancers14051155