
Management of Synchronous Extrathoracic Oligometastatic Non-Small Cell Lung Cancer

 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Management of Patients with Oligometastatic Disease
2.3. Outcomes and Statistical Analysis
3. Results
3.1. Patients, Tumor Characteristics, and Treatment Details
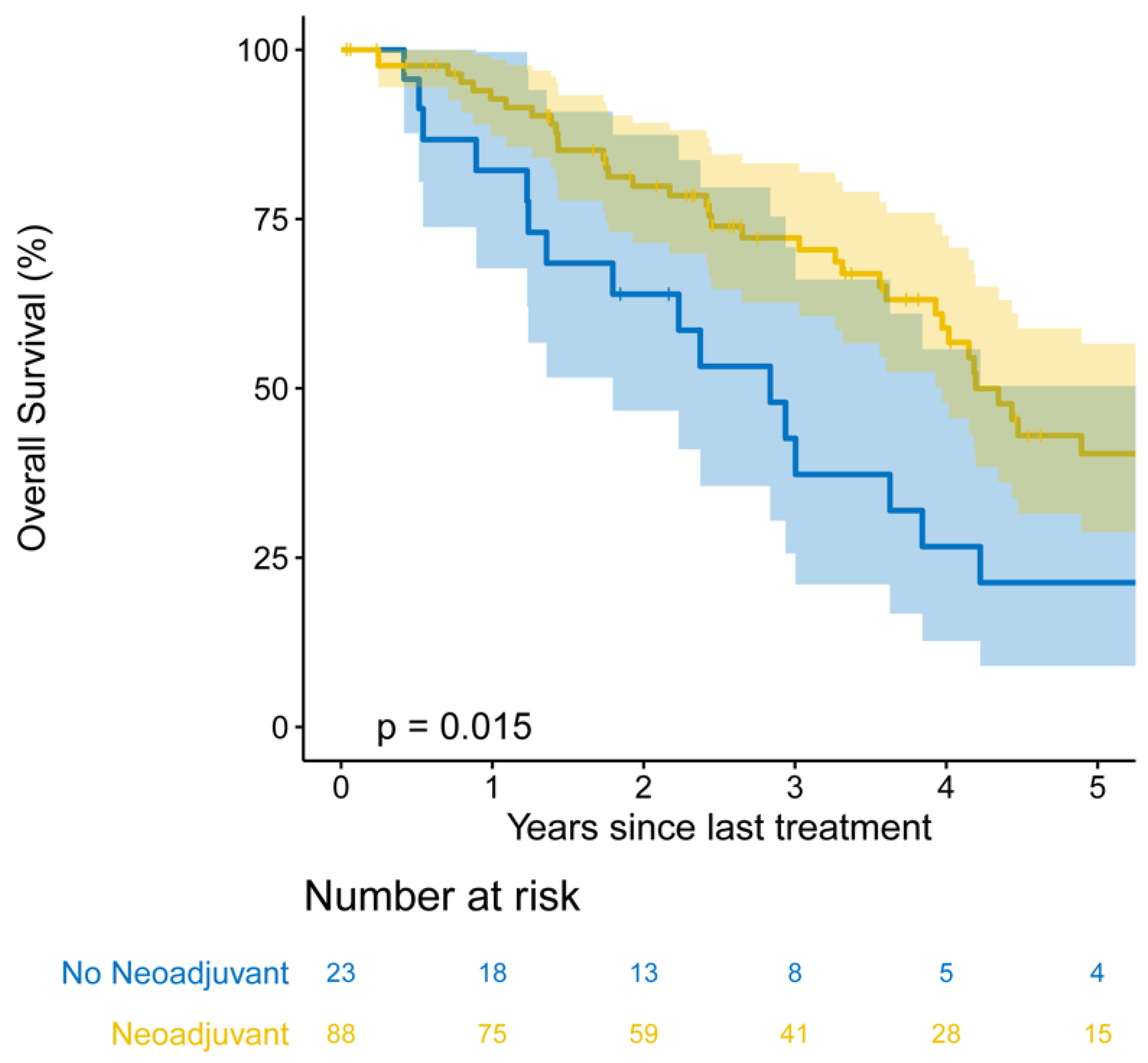
3.2. Follow-Up and Survival
3.3. Patterns of Treatment Failure
3.4. Factors Associated with EFS and OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Little, A.G.; Gay, E.G.; Gaspar, L.E.; Stewart, A.K. National survey of non-small cell lung cancer in the United States: Epidemiology, pathology and patterns of care. Lung Cancer 2007, 57, 253–260. [Google Scholar] [CrossRef]
- Li, D.; Zhu, X.; Wang, H.; Qiu, M.; Li, N. Should aggressive thoracic therapy be performed in patients with synchronous oligometastatic non-small cell lung cancer? A meta-analysis. J. Thorac. Dis. 2017, 9, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dingemans, A.-M.C.; Hendriks, L.E.; Berghmans, T.; Levy, A.; Hasan, B.; Faivre-Finn, C.; Giaj-Levra, M.; Giaj-Levra, N.; Girard, N.; Greillier, L.; et al. Definition of Synchronous Oligometastatic Non–Small Cell Lung Cancer—A Consensus Report. J. Thorac. Oncol. 2019, 14, 2109–2119. [Google Scholar] [CrossRef] [PubMed]
- Parikh, R.B.; Cronin, A.M.; Kozono, D.E.; Oxnard, G.R.; Mak, R.H.; Jackman, D.M.; Lo, P.C.; Baldini, E.H.; Johnson, B.E.; Chen, A.B. Definitive Primary Therapy in Patients Presenting With Oligometastatic Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. 2014, 89, 880–887. [Google Scholar] [CrossRef]
- Loi, M.; Mazzella, A.; Mansuet-Lupo, A.; Bobbio, A.; Canny, E.; Magdeleinat, P.; Régnard, J.-F.; Damotte, D.; Trédaniel, J.; Alifano, M. Synchronous Oligometastatic Lung Cancer Deserves a Dedicated Management. Ann. Thorac. Surg. 2019, 107, 1053–1059. [Google Scholar] [CrossRef]
- Bartlett, E.K.; Simmons, K.D.; Wachtel, H.; Roses, R.E.; Fraker, D.L.; Kelz, R.R.; Karakousis, G.C. The rise in metastasectomy across cancer types over the past decade. Cancer 2014, 121, 747–757. [Google Scholar] [CrossRef]
- Gomez, D.R.; Blumenschein, G.R.; Lee, J.J.; Hernandez, M.; Ye, R.; Camidge, D.R.; Doebele, R.C.; Skoulidis, F.; E Gaspar, L.; Gibbons, D.L.; et al. Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: A multicentre, randomised, controlled, phase 2 study. Lancet Oncol. 2016, 17, 1672–1682. [Google Scholar] [CrossRef] [Green Version]
- Gomez, D.R.; Tang, C.; Zhang, J.; Jr, G.R.B.; Hernandez, M.; Lee, J.J.; Ye, R.; Palma, D.A.; Louie, A.V.; Camidge, D.R.; et al. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients With Oligometastatic Non–Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study. J. Clin. Oncol. 2019, 37, 1558–1565. [Google Scholar] [CrossRef]
- Iyengar, P.; Wardak, Z.; Gerber, D.E.; Tumati, V.; Ahn, C.; Hughes, R.S.; Dowell, J.E.; Cheedella, N.; Nedzi, L.; Westover, K.D.; et al. Consolidative Radiotherapy for Limited Metastatic Non–Small-Cell Lung Cancer. JAMA Oncol. 2018, 4, e173501. [Google Scholar] [CrossRef]
- A Palma, D.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- David, E.A.; Canter, R.J.; Chen, Y.; Cooke, D.T.; Cress, R.D. Surgical Management of Advanced Non-Small Cell Lung Cancer Is Decreasing But Is Associated With Improved Survival. Ann. Thorac. Surg. 2016, 102, 1101–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.C.; Alex, D.; Bott, M.; Tan, K.S.; Seshan, V.; Golden, A.; Sauter, J.L.; Buonocore, D.J.; Vanderbilt, C.M.; Gupta, S.; et al. Comprehensive Next-Generation Sequencing Unambiguously Distinguishes Separate Primary Lung Carcinomas From Intrapulmonary Metastases: Comparison with Standard Histopathologic Approach. Clin. Cancer Res. 2019, 25, 7113–7125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettinger, D.S.; Wood, D.E.; Aggarwal, C.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; et al. NCCN Guidelines Insights: Non–Small Cell Lung Cancer, Version 1.2020. J. Natl. Compr. Cancer Netw. 2019, 17, 1464–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Shuster, J.J. Median follow-up in clinical trials. J. Clin. Oncol. 1991, 9, 191–192. [Google Scholar] [CrossRef]
- Opitz, I.; Patella, M.; Payrard, L.; Perentes, J.Y.; Inderbitzi, R.; Gelpke, H.; Schulte, S.; Diezi, M.; Gonzalez, M.; Krueger, T.; et al. Prognostic factors of oligometastatic non-small-cell lung cancer following radical therapy: A multicentre analysis. Eur. J. Cardio-Thorac. Surg. 2020, 57, 1166–1172. [Google Scholar] [CrossRef]
- Mitchell, K.G.; Farooqi, A.; Ludmir, E.B.; Corsini, E.M.; Sepesi, B.; Gomez, D.R.; Antonoff, M.B.; Vaporciyan, A.A.; Swisher, S.G.; Heymach, J.V.; et al. Pulmonary resection is associated with long-term survival and should remain a therapeutic option in oligometastatic lung cancer. J. Thorac. Cardiovasc. Surg. 2021, 161, 1497–1504.e2. [Google Scholar] [CrossRef]
- Mitchell, K.G.; Farooqi, A.; Ludmir, E.B.; Corsini, E.M.; Zhang, J.; Sepesi, B.; Vaporciyan, A.A.; Swisher, S.G.; Heymach, J.V.; Zhang, J.; et al. Improved Overall Survival With Comprehensive Local Consolidative Therapy in Synchronous Oligometastatic Non–Small-Cell Lung Cancer. Clin. Lung Cancer 2020, 21, 37–46.e7. [Google Scholar] [CrossRef] [Green Version]
- Mordant, P.; Arame, A.; De Dominicis, F.; Pricopi, C.; Foucault, C.; Dujon, A.; Le Pimpec-Barthes, F.; Riquet, M. Which metastasis management allows long-term survival of synchronous solitary M1b non-small cell lung cancer? Eur. J. Cardio-Thorac. Surg. 2012, 41, 617–622. [Google Scholar] [CrossRef] [Green Version]
- Albain, K.S.; Crowley, J.J.; Leblanc, M.; Livingston, R.B. Survival determinants in extensive-stage non-small-cell lung cancer: The Southwest Oncology Group experience. J. Clin. Oncol. 1991, 9, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- McMahon, M.; Barbiere, J.M.; Greenberg, D.C.; A Wright, K.; Lyratzopoulos, G. Population-based trends in use of surgery for non-small cell lung cancer in a UK region, 1995–2006. Thorax 2011, 66, 453–455. [Google Scholar] [CrossRef] [Green Version]
- Collaud, S.; Stahel, R.; Inci, I.; Hillinger, S.; Schneiter, D.; Kestenholz, P.; Weder, W. Survival of patients treated surgically for synchronous single-organ metastatic NSCLC and advanced pathologic TN stage. Lung Cancer 2012, 78, 234–238. [Google Scholar] [CrossRef]
- Tamura, T.; Kurishima, K.; Watanabe, H.; Shiozawa, T.; Nakazawa, K.; Ishikawa, H.; Satoh, H.; Hizawa, N. Characteristics of clinical N0 metastatic non-small cell lung cancer. Lung Cancer 2015, 89, 71–75. [Google Scholar] [CrossRef]
- Ashworth, A.B.; Senan, S.; Palma, D.A.; Riquet, M.; Ahn, Y.C.; Ricardi, U.; Congedo, M.T.; Gomez, D.R.; Wright, G.M.; Melloni, G.; et al. An Individual Patient Data Metaanalysis of Outcomes and Prognostic Factors After Treatment of Oligometastatic Non–Small-Cell Lung Cancer. Clin. Lung Cancer 2014, 15, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Griffioen, G.H.; Toguri, D.; Dahele, M.; Warner, A.; de Haan, P.F.; Rodrigues, G.B.; Slotman, B.J.; Yaremko, B.P.; Senan, S.; Palma, D.A. Radical treatment of synchronous oligometastatic non-small cell lung carcinoma (NSCLC): Patient outcomes and prognostic factors. Lung Cancer 2013, 82, 95–102. [Google Scholar] [CrossRef]
- Gibson, A.J.W.; Li, H.; D’Silva, A.; Tudor, R.A.; Elegbede, A.A.; Otsuka, S.M.; Bebb, D.G.; Cheung, W.Y. Impact of number versus location of metastases on survival in stage IV M1b non-small cell lung cancer. Med. Oncol. 2018, 35, 117. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | No. (%) or Median (IQR) |
|---|---|
| Age at surgery, years | 62 (53–69) |
| Sex | |
| Female | 65 (59) |
| Male | 46 (41) |
| Smoking status | |
| Never | 21 (19) |
| Ever | 90 (81) |
| Pack-years | 30 (4.5–48) |
| Radiologic primary tumor size, cm (n = 102) | 3.3 (2.0–4.6) |
| Primary tumor SUVmax (n = 87) | 9.6 (6.3–15) |
| FEV1, % (n = 103) | 91 (79–101) |
| DLCO, % (n = 103) | 82 (67–94) |
| Extrathoracic metastatic site at diagnosis | |
| Adrenal | 6 (5) |
| Bone | 21 (19) |
| Brain | 57 (51) |
| Liver | 8 (7) |
| Other a | 9 (8) |
| Multiple | 10 (9) |
| Total metastatic sites | |
| 1 | 101 (91) |
| 2 | 8 (7) |
| 3 | 2 (2) |
| Total metastatic lesions | |
| 1 | 87 (78) |
| 2 | 15 (14) |
| 3 | 7 (6) |
| 4 | 1 (1) |
| 5 | 1 (1) |
| Local consolidative therapy for metastasis | |
| No | 18 (16) |
| Yes | 93 (84) |
| Neoadjuvant therapy | |
| None | 23 (21) |
| Systemic therapy only b | 77 (69) |
| Chemoradiotherapy | 11 (10) |
| Operative approach to primary tumor | |
| Open | 70 (63) |
| VATS | 41 (37) |
| Primary tumor resection type | |
| Lobectomy | 85 (77) |
| Segmentectomy | 26 (23) |
| Histologic subtype | |
| Lepidic | 0 (0) |
| Acinar/papillary | 30 (27) |
| Micropapillary/solid | 14 (13) |
| Unknown | 67 (60) |
| Final pathologic diagnosis | |
| Adenocarcinoma | 80 (72) |
| Squamous cell carcinoma | 6 (5) |
| Other | 14 (13) |
| No viable tumor | 11 (10) |
| Lymphovascular invasion | |
| No | 45 (41) |
| Yes | 60 (54) |
| Unknown | 6 (5) |
| Visceral pleural invasion | |
| No | 62 (56) |
| Yes | 45 (41) |
| Unknown | 4 (4) |
| Pathologic primary tumor size, cm | 2.5 (1.6–3.6) |
| Pathologic stage (AJCC 8th edition) c | |
| I | 5 (5) |
| II | 2 (2) |
| III | 2 (2) |
| IV | 102 (92) |
| Adjuvant therapy | |
| None | 67 (60) |
| Systemic therapy only b | 31 (28) |
| Radiotherapy only | 8 (7) |
| Chemoradiotherapy | 5 (5) |
| Outcome, Variable | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Event-free survival | ||||
| Pathologic primary tumor size, cm | 1.15 (1.03–1.28) | 0.013 | 1.15 (1.03–1.29) | 0.014 |
| Lymphovascular invasion | 1.85 (1.16–2.96) | 0.010 | 1.73 (1.06–2.84) | 0.029 |
| Overall survival | ||||
| Receipt of neoadjuvant therapy | 0.52 (0.30–0.89) | 0.018 | 0.43 (0.24–0.77) | 0.004 |
| Pathologic primary tumor size, cm | 1.21 (1.06–1.38) | 0.004 | 1.18 (1.02–1.35) | 0.023 |
| Pathologic N1 or N2 disease (vs. N0) | 2.05 (1.18–3.56) | 0.010 | 1.83 (1.05–3.20) | 0.033 |
| Visceral pleural invasion | 2.45 (1.42–4.21) | 0.001 | 1.93 (1.10–3.40) | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, G.D.; Lengel, H.B.; Hsu, M.; Tan, K.S.; Caso, R.; Ghanie, A.; Connolly, J.G.; Bains, M.S.; Rusch, V.W.; Huang, J.; et al. Management of Synchronous Extrathoracic Oligometastatic Non-Small Cell Lung Cancer. Cancers 2021, 13, 1893. https://doi.org/10.3390/cancers13081893
Jones GD, Lengel HB, Hsu M, Tan KS, Caso R, Ghanie A, Connolly JG, Bains MS, Rusch VW, Huang J, et al. Management of Synchronous Extrathoracic Oligometastatic Non-Small Cell Lung Cancer. Cancers. 2021; 13(8):1893. https://doi.org/10.3390/cancers13081893
Chicago/Turabian StyleJones, Gregory D., Harry B. Lengel, Meier Hsu, Kay See Tan, Raul Caso, Amanda Ghanie, James G. Connolly, Manjit S. Bains, Valerie W. Rusch, James Huang, and et al. 2021. "Management of Synchronous Extrathoracic Oligometastatic Non-Small Cell Lung Cancer" Cancers 13, no. 8: 1893. https://doi.org/10.3390/cancers13081893