Effectiveness and Safety of Immune Checkpoint Inhibitors for Patients with Advanced Non Small-Cell Lung Cancer in Real-World: Review and Meta-Analysis

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
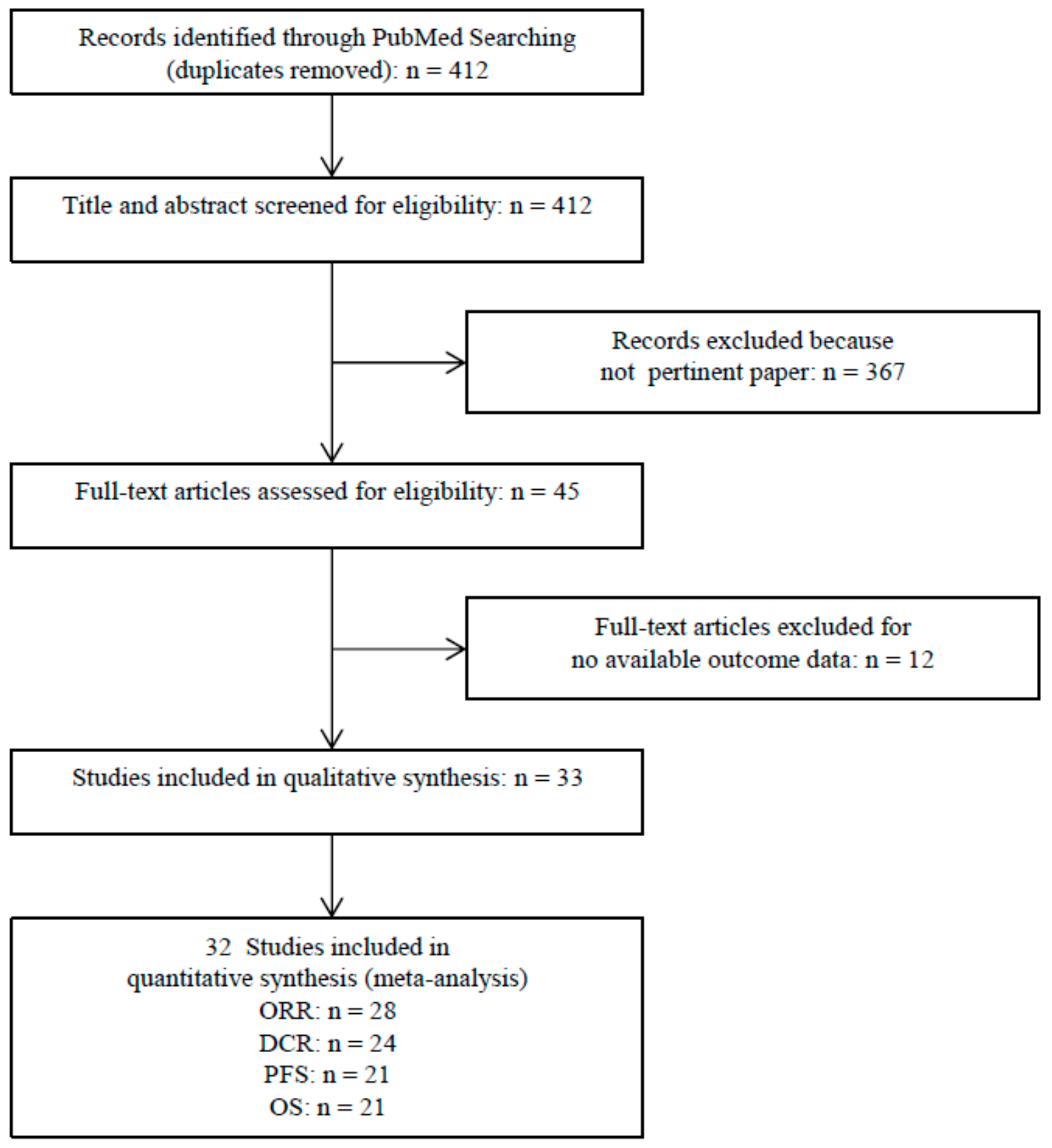
2.1. Search Strategy and Inclusion Criteria
2.2. Eligibility Criteria
2.3. Data Extraction
3. Statistical Analysis
4. Results
4.1. Study Characteristics
4.2. Meta-Analysis
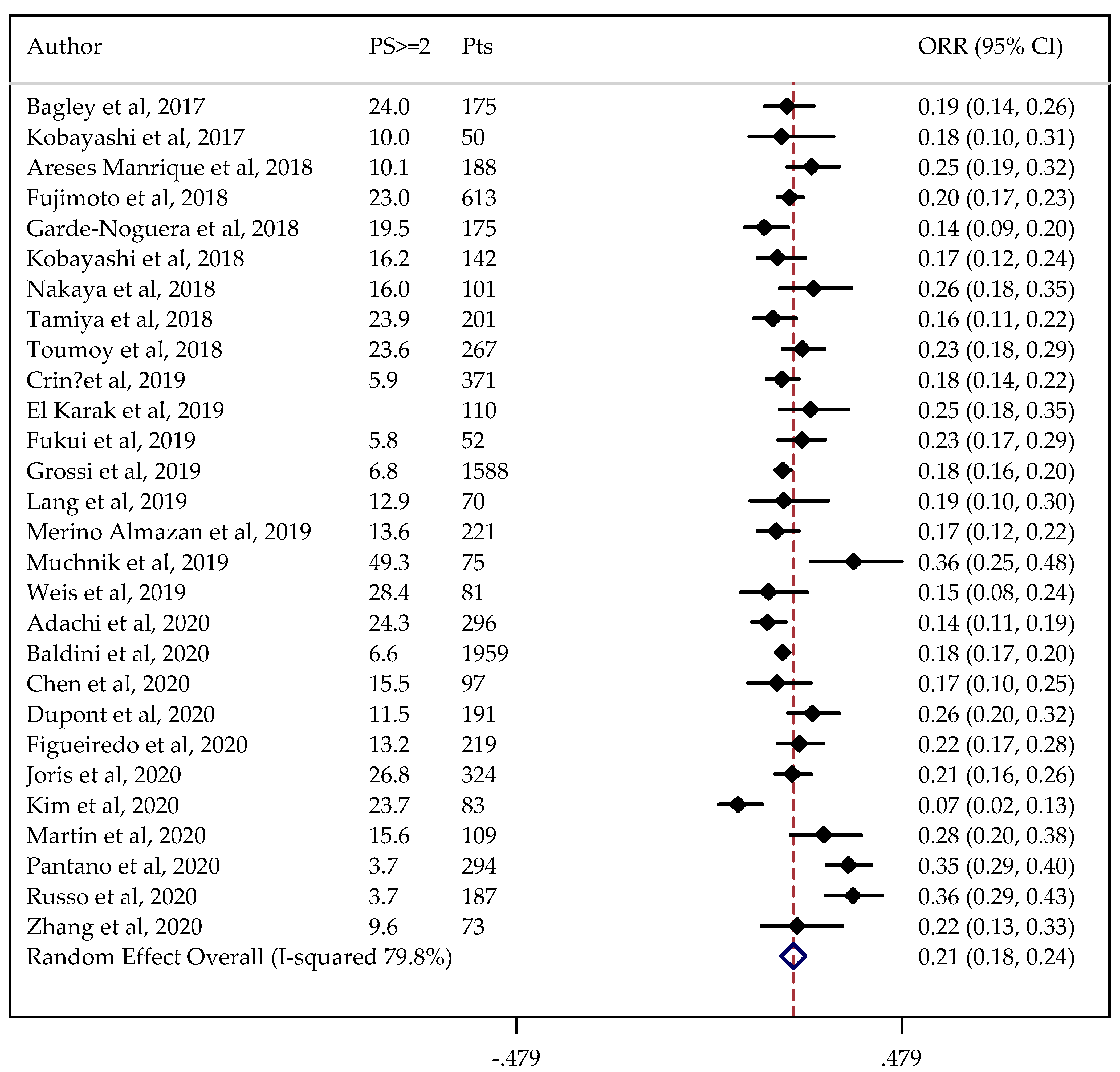
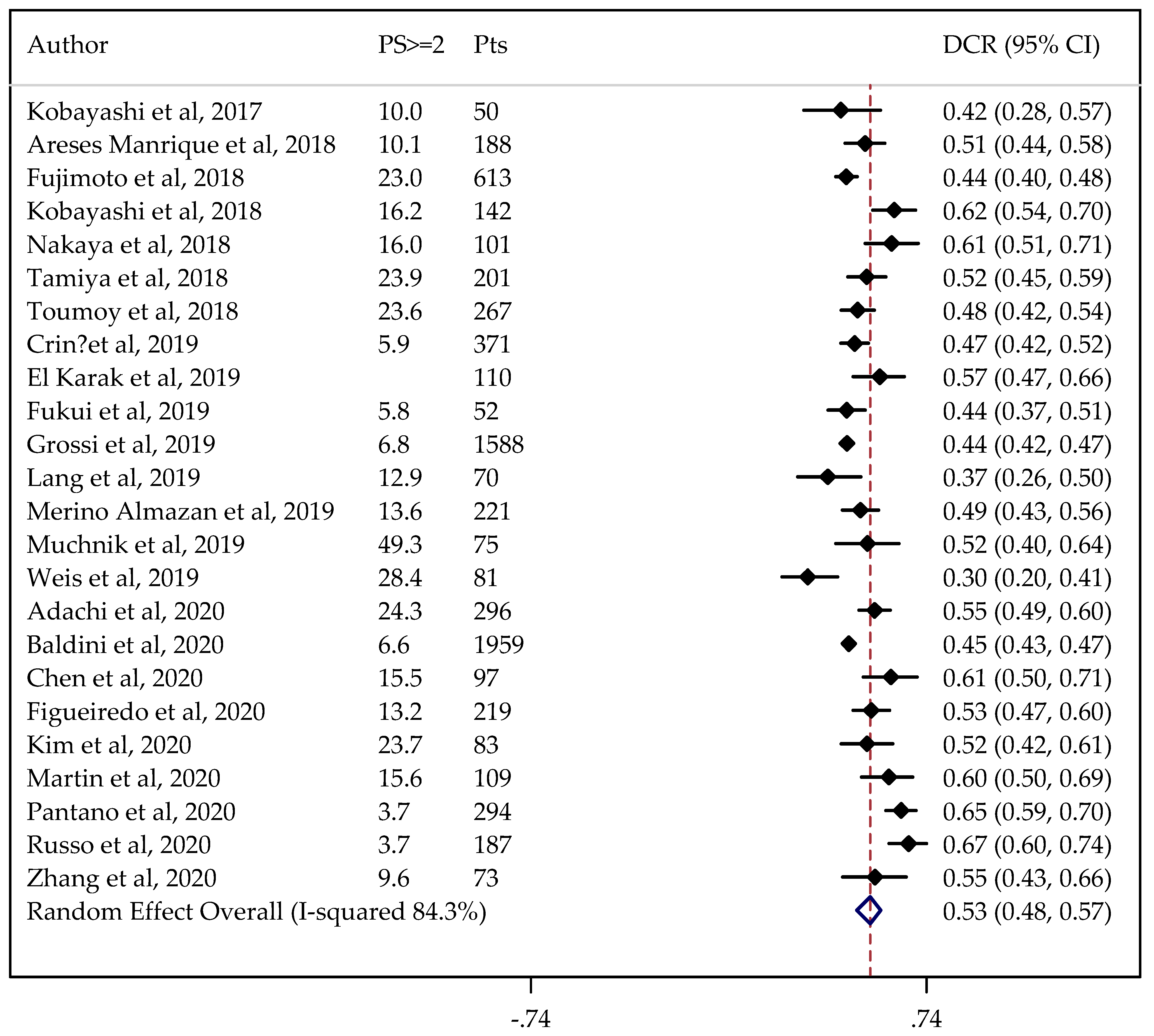
Pooled Analysis of ORR and DCR
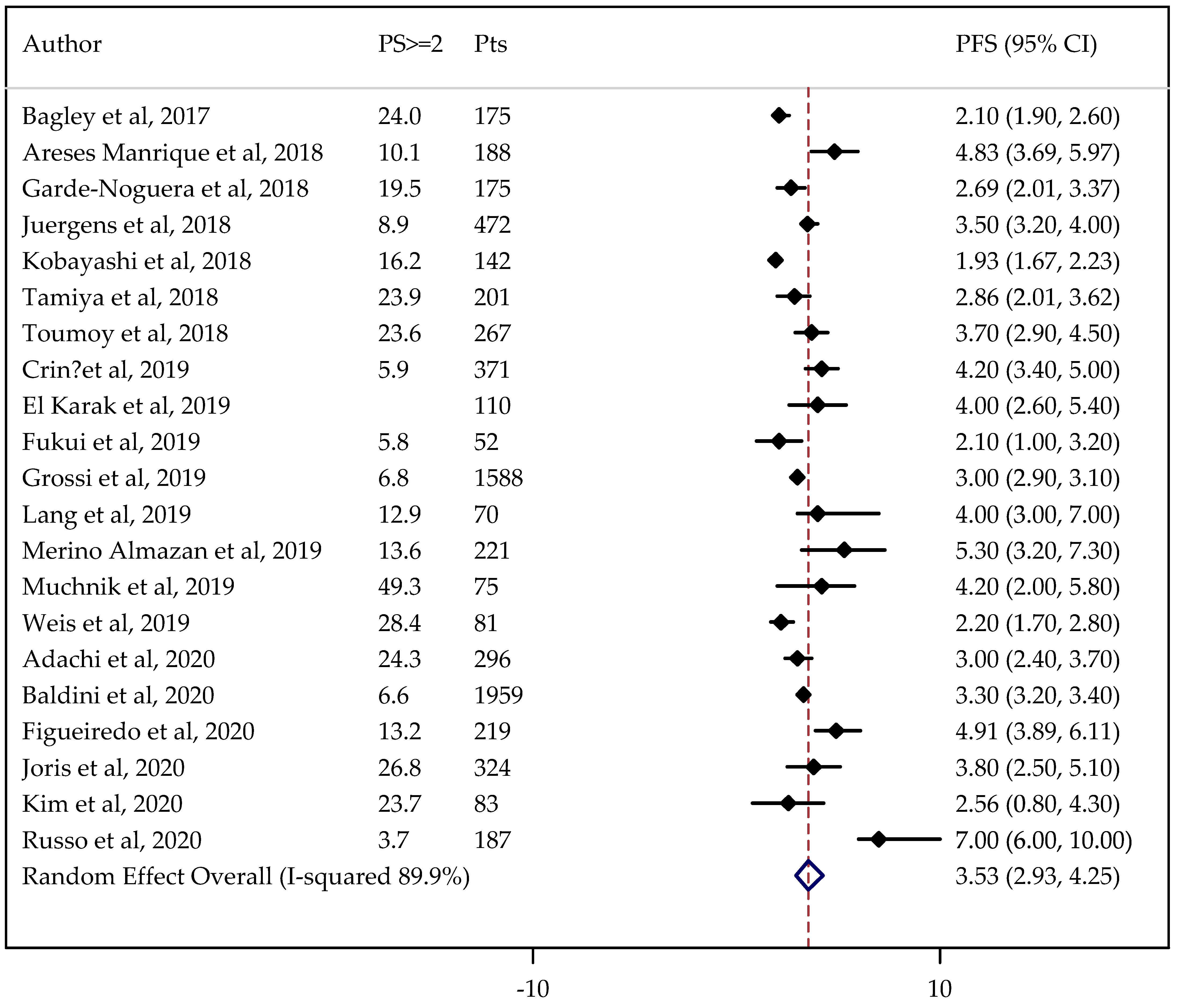
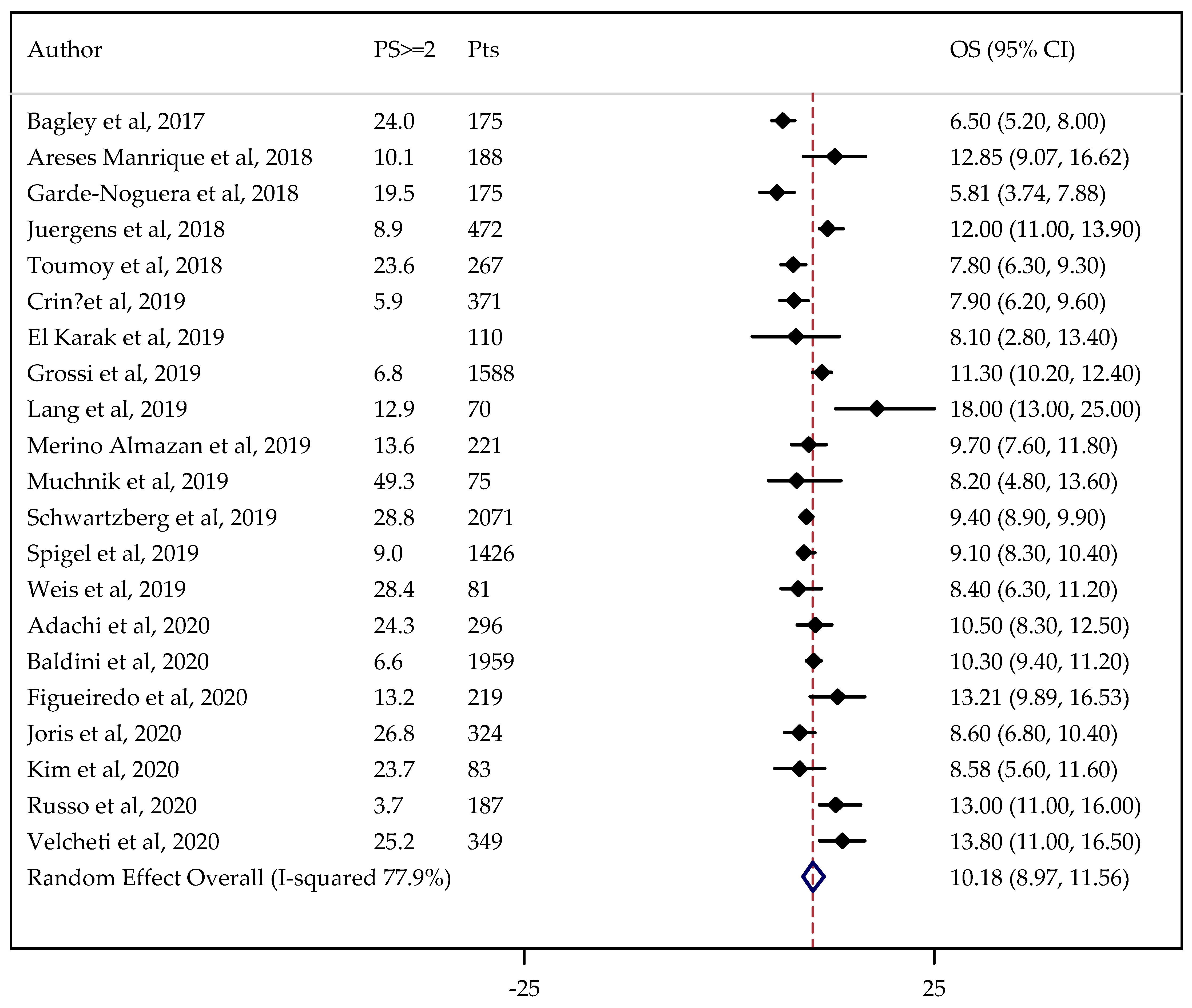
4.3. Pooled Analysis of PFS and OS
5. Discussion
5.1. Quantitative Analysis
5.2. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raphael, J.; Batra, A.; Boldt, G.; Shah, P.S.; Blanchette, P.; Rodrigues, G.; Vincent, M.D. Predictors of Survival Benefit from Immune Checkpoint Inhibitors in Patients With Advanced Non-small-cell Lung Cancer: A Systematic Review and Meta-analysis. Clin. Lung Cancer 2020, 21, 106–113. [Google Scholar] [CrossRef]
- Pinheiro, F.D.; Teixeira, A.F.; de Brito, B.B.; da Silva, F.A.F.; Santos, M.L.C.; de Melo, F.F. Immunotherapy—New perspective in lung cancer. World J. Clin. Oncol. 2020, 11, 250–259. [Google Scholar] [CrossRef]
- Rossi, A. Immunotherapy and NSCLC: The Long and Winding Road. Cancers 2020, 12, 2512. [Google Scholar] [CrossRef]
- Wagner, G.; Stollenwerk, H.K.; Klerings, I.; Pecherstorfer, M.; Gartlehner, G.; Singer, J. Efficacy and safety of immune checkpoint inhibitors in patients with advanced non-small cell lung cancer (NSCLC): A systematic literature review. Oncoimmunology 2020, 9, 1774314. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Antonia, S.; Borghaei, H.; Ramalingam, S.; Horn, L.; De Castro Carpeño, J.; Pluzanski, A.; Burgio, M.A.; Garassino, M.; Chow, L.Q.M.; Gettinger, S.; et al. Four-year survival with nivolumab in patients with previously treated advanced non-small-cell lung cancer: A pooled analysis. Lancet Oncol. 2019, 20, 1395–1408. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Dubos Arvis, C.; Ahn, M.J.; et al. Pembrolizumab versusdocetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; von Pawel, J.; Park, K.; Rittmeyer, A.; Gandara, D.R.; Ponce Aix, S.; Han, J.Y.; Gadgeel, S.M.; Hida, T.; Cortinovis, D.L.; et al. Updated Efficacy Analysis Including Secondary Population Results for OAK: A Randomized Phase III Study of Atezolizumab versus Docetaxel in Patients with Previously Treated Advanced Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2018, 13, 1156–1170. [Google Scholar] [CrossRef] [Green Version]
- Rashdan, S.; Gerber, D.E. Immunotherapy for non-small cell lung cancer: From clinical trials to real-world practice. Transl. Lung Cancer Res. 2019, 8, 202–207. [Google Scholar] [CrossRef]
- Zauderer, M.G. Practical Application of Real-World Evidence in Developing Cancer Therapies. JCO Clin. Cancer Inform. 2019, 3, 1–2. [Google Scholar] [CrossRef]
- Pasello, G.; Pavan, A.; Attili, I.; Bortolami, A.; Bonanno, L.; Menis, J.; Conte, P.; Guarneri, V. Real world data in the era of Immune Checkpoint Inhibitors (ICIs): Increasing evidence and future applications in lung cancer. Cancer Treat. Rev. 2020, 87, 102031. [Google Scholar] [CrossRef] [PubMed]
- Sherman, R.E.; Anderson, S.A.; Dal Pan, G.J.; Gray, G.W.; Gross, T.; Hunter, N.L.; LaVange, L.; Marinac-Dabic, D.; Marks, P.W.; Robb, M.A.; et al. Real-World Evidence—What Is It and What Can It Tell Us? N. Engl. J. Med. 2016, 375, 2293–2297. [Google Scholar] [CrossRef] [Green Version]
- Hendriks, L.E.L.; Henon, C.; Auclin, E.; Mezquita, L.; Ferrara, R.; Audigier-Valette, C.; Mazieres, J.; Lefebvre, C.; Rabeau, A.; Le Moulec, S.; et al. Outcome of Patients with Non-Small Cell Lung Cancer and Brain Metastases Treated with Checkpoint Inhibitors. J. Thorac. Oncol. 2019, 14, 1244–1254. [Google Scholar] [CrossRef]
- Song, P.; Zhang, J.; Shang, C.; Zhang, L. Author Correction: Real-world evidence and clinical observations of the treatment of advanced nonsmall cell lung cancer with PD-1/PD-L1 inhibitors. Sci. Rep. 2020, 10, 1525. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Contr. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Knapp, G.; Hartung, J. Improved tests for a random effects meta-regression with a single covariate. Stat. Med. 2003, 22, 2693–2710. [Google Scholar] [CrossRef]
- Egger, M.; Smith, J.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adachi, Y.; Tamiya, A.; Taniguchi, Y.; Enomoto, T.; Azuma, K.; Kouno, S.; Inagaki, Y.; Saijo, N.; Okishio, K.; Atagi, S. Predictive factors for progression-free survival in non-mall cell lung cancer patients receiving nivolumab based on performance status. Cancer Med. 2020, 9, 1383–1391. [Google Scholar] [CrossRef]
- Chen, M.; Li, Q.; Xu, Y.; Zhao, J.; Zhang, L.; Wei, L.; Zhong, W.; Wang, M. Immunotherapy as second-line treatment and beyond for non-small cell lung cancer in a single center of China: Outcomes, toxicities, and clinical predictive factors from a real-world retrospective analysis. Thorac. Cancer 2020, 11, 1955–1962. [Google Scholar] [CrossRef]
- Dupont, R.; Bérard, E.; Puisset, F.; Comont, T.; Delord, J.P.; Guimbaud, R.; Meyer, N.; Mazieres, J.; Alric, L. The prognostic impact of immune-related adverse events during anti-PD1 treatment in melanoma and non-small-cell lung cancer: A real-life retrospective study. Oncoimmunology 2019, 9, 1682383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiredo, A.; Almeida, M.A.; Almodovar, M.; Alves, P.; Araújo, A.; Araújo, D.; Barata, F.; Barradas, F.; Barroso, A.; Brito, U.; et al. Real-world data from the Portuguese Nivolumab Expanded Access Program (EAP) in previously treated Non Small Cell Lung Cancer (NSCLC). Pulmonology 2020, 26, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Joris, S.; Pieters, T.; Sibille, A.; Bustin, F.; Jacqmin, L.; Kalantari, H.R.; Surmont, V.; Goeminne, J.-C.; Clinckart, F.; Pat, K.; et al. Real life safety and effectiveness of nivolumab in older patients with non-small cell lung cancer: Results from the Belgian compassionate use program. J. Geriatr. Oncol. 2020, 11, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Lupinacci, L.; Perazzo, F.; Bas, C.; Carranza, O.; Puparelli, C.; Kowalyszyn, R.; Magri, I.; Varela, M.; Richardet, E.; et al. Efficacy and Safety of Nivolumab in Previously Treated Patients with Non-Small-cell Lung Cancer: Real World Experience in Argentina. Clin. Lung Cancer 2020, 21, e380–e387. [Google Scholar] [CrossRef] [PubMed]
- Pantano, F.; Russano, M.; Berruti, A.; Mansueto, G.; Migliorino, M.R.; Adamo, V.; Aprile, G.; Gelibter, A.; Ficorella, C.; Falcone, A.; et al. Prognostic clinical factors in patients affected by non-small-cell lung cancer receiving Nivolumab. Expert Opin. Biol. Ther. 2020, 20, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Russano, M.; Franchina, T.; Migliorino, M.R.; Aprile, G.; Mansueto, G.; Berruti, A.; Falcone, A.; Aieta, M.; Gelibter, A.; et al. Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Outcomes with Nivolumab in Pretreated Non-Small Cell Lung Cancer (NSCLC): A Large Retrospective Multicenter Study. Adv. Ther. 2020, 37, 1145–1155. [Google Scholar] [CrossRef]
- Velcheti, V.; Chandwani, S.; Chen, X.; Piperdi, B.; Burke, T. Pembrolizumab for Previously Treated, PD-L1-expressing Advanced NSCLC: Real-world Time on Treatment and Overall Survival. Clin. Lung Cancer 2020, 21, e445–e455. [Google Scholar] [CrossRef]
- Kim, S.H.; Choi, C.M.; Lee, D.H.; Kim, S.W.; Yoon, S.; Kim, W.S.; Ji, W.; Lee, J.C. Clinical outcomes of nivolumab in patients with advanced non-small cell lung cancer in real-world practice, with an emphasis on hyper-progressive disease. J. Cancer Res. Clin. Oncol. 2020, 146, 3025–3036. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Cheng, R.; Wang, H.; Zhang, Y.; Yan, X.; Li, P.; Zhang, M.; Zhang, X.; Yang, J.; Niu, Y.; et al. Comparable outcomes of nivolumab in patients with advanced NSCLC presenting with or without brain metastases: A retrospective cohort study. Cancer Immunol. Immunother. 2020, 69, 399–405. [Google Scholar] [CrossRef]
- Baldini, E.; Lunghi, A.; Cortesi, E.; Turci, D.; Signorelli, D.; Stati, V.; Melotti, B.; Ricciuti, B.; Frassoldati, A.; Romano, G.; et al. Immune-related adverse events correlate with clinical outcomes in NSCLC patients treated with nivolumab: The Italian NSCLC expanded access program. Lung Cancer 2020, 140, 59–64. [Google Scholar] [CrossRef]
- Crinò, L.; Bidoli, P.; Delmonte, A.; Grossi, F.; De Marinis, F.; Ardizzoni, A.; Vitiello, F.; Lo Russo, G.; Soto Parra, H.; Cortesi, E.; et al. Italian Cohort of Nivolumab Expanded Access Program in Squamous Non-Small Cell Lung Cancer: Results from a Real-World Population. Oncologist 2019, 24, e1165–e1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, T.; Okuma, Y.; Nakahara, Y.; Otani, S.; Igawa, S.; Katagiri, M.; Mitsufuji, H.; Kubota, M.; Hiyoshi, Y.; Ishihara, M.; et al. Activity of Nivolumab and Utility of Neutrophil-to-Lymphocyte Ratio as a Predictive Biomarker for Advanced Non-Small-Cell Lung Cancer: A Prospective Observational Study. Clin. Lung Cancer 2019, 20, 208–214. [Google Scholar] [CrossRef]
- Grossi, F.; Genova, C.; Crinò, L.; Delmonte, A.; Turci, D.; Signorelli, D.; Passaro, A.; Soto Parra, H.; Catino, A.; Landi, L.; et al. Real-life results from the overall population and key subgroups within the Italian cohort of nivolumab expanded access program in non-squamous non-small cell lung cancer. Eur. J. Cancer. 2019, 123, 72–80. [Google Scholar] [CrossRef]
- Lang, D.; Huemer, F.; Rinnerthaler, G.; Horner, A.; Wass, R.; Brehm, E.; Akbari, K.; Granitz, M.; Hutarew, G.; Kaiser, B.; et al. Therapy Line and Associated Predictors of Response to PD-1/PD-L1-Inhibitor Monotherapy in Advanced Non-small-Cell Lung Cancer: A Retrospective Bi-centric Cohort Study. Target. Oncol. 2019, 14, 707–717. [Google Scholar] [CrossRef] [Green Version]
- Merino Almazán, M.; Duarte Pérez, J.M.; Marín Pozo, J.F.; Ortega Granados, A.L.; De Muros Fuentes, B.; Quesada Sanz, P.; Gago Sánchez, A.I.; Rodríguez Gómez, P.; Jurado García, J.M.; Artime Rodríguez-Hermida, F.; et al. A multicentre observational study of the effectiveness, safety and economic impact of nivolumab on non-small-cell lung cancer in real clinical practice. Int. J. Clin. Pharm. 2019, 41, 272–279. [Google Scholar] [CrossRef]
- Muchnik, E.; Loh, K.P.; Strawderman, M.; Magnuson, A.; Mohile, S.G.; Estrah, V.; Maggiore, R.J. Immune Checkpoint Inhibitors in Real-World Treatment of Older Adults with Non-Small Cell Lung Cancer. J. Am. Geriatr. Soc. 2019, 67, 905–912. [Google Scholar] [CrossRef]
- Weis, T.M.; Hough, S.; Reddy, H.G.; Daignault-Newton, S.; Kalemkerian, G.P. Real-world comparison of immune checkpoint inhibitors in non-small cell lung cancer following platinum-based chemotherapy. J. Oncol. Pharm. Pract. 2020, 26, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Schwartzberg, L.; Korytowsky, B.; Penrod, J.R.; Zhang, Y.; Le, T.K.; Batenchuk, C.; Krug, L. Real-World Clinical Impact of Immune Checkpoint Inhibitors in Patients with Advanced/Metastatic Non-Small Cell Lung Cancer After Platinum Chemotherapy. Clin. Lung Cancer 2019, 20, 287–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Karak, F.; Haddad, F.G.; Eid, R.; Al Ghor, M.; El Rassy, E.; Ahmadieh, N.; Choullamy, T.; Halim, N.A.; Tfayli, A.; Farhat, F.; et al. Lung cancer and immunotherapy: A real-life experience from second line and beyond. Future Oncol. 2019, 15, 3025–3032. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; McCleod, M.; Jotte, R.M.; Einhorn, L.; Horn, L.; Waterhouse, D.M.; Creelan, B.; Babu, S.; Leighl, N.B.; Chandler, J.C.; et al. Safety, Efficacy, and Patient-Reported Health-Related Quality of Life and Symptom Burden with Nivolumab in Patients with Advanced Non-Small Cell Lung Cancer, Including Patients Aged 70 Years or Older or with Poor Performance Status (CheckMate 153). J. Thorac. Oncol. 2019, 14, 1628–1639. [Google Scholar] [CrossRef]
- Areses Manrique, M.C.; Mosquera Martínez, J.; García González, J.; Afonso Afonso, F.J.; Lázaro Quintela, M.; Fernández Núñez, N.; Azpitarte Raposeiras, C.; Amenedo Gancedo, M.; Santomé Couto, L.; García Campelo, M.R.; et al. Real world data of nivolumab for previously treated non-small cell lung cancer patients: A Galician lung cancer group clinical experience. Transl. Lung Cancer Res. 2018, 7, 404–415. [Google Scholar] [CrossRef]
- Garde-Noguera, J.; Martin-Martorell, P.; De Julián, M.; Perez-Altozano, J.; Salvador-Coloma, C.; García-Sanchez, J.; Insa-Molla, A.; Martín, M.; Mielgo-Rubio, X.; Marin-Liebana, S.; et al. Predictive and prognostic clinical and pathological factors of nivolumab efficacy in non-small-cell lung cancer patients. Clin. Transl. Oncol. 2018, 20, 1072–1079. [Google Scholar] [CrossRef]
- Fujimoto, D.; Yoshioka, H.; Kataoka, Y.; Morimoto, T.; Kim, Y.H.; Tomii, K.; Ishida, T.; Hirabayashi, M.; Hara, S.; Ishitoko, M.; et al. Efficacy and safety of nivolumab in previously treated patients with non-small cell lung cancer: A multicenter retrospective cohort study. Lung Cancer 2018, 119, 14–20. [Google Scholar] [CrossRef]
- Juergens, R.; Mariano, C.; Jolivet, J.; Finn, N.; Rothenstein, J.; Reaume, M.N.; Faghih, A.; Labbé, C.; Owen, S.; Shepherd, F.A.; et al. Real-world benefit of nivolumab in a Canadian non-small-cell lung cancer cohort. Curr. Oncol. 2018, 25, 384–392. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, K.; Nakachi, I.; Naoki, K.; Satomi, R.; Nakamura, M.; Inoue, T.; Tateno, H.; Sakamaki, F.; Sayama, K.; Terashima, T.; et al. Real-world Efficacy and Safety of Nivolumab for Advanced Non-Small-Cell Lung Cancer: A retrospective multicenter analysis. Clin. Lung Cancer 2018, 19, e349–e358. [Google Scholar] [CrossRef]
- Nakaya, A.; Kurata, T.; Yoshioka, H.; Takeyasu, Y.; Niki, M.; Kibata, K.; Satsutani, N.; Ogata, M.; Miyara, T.; Nomura, S. Neutrophil-to-lymphocyte ratio as an early marker of outcomes in patients with advanced non-small-cell lung cancer treated with nivolumab. Int. J. Clin. Oncol. 2018, 23, 634–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamiya, M.; Tamiya, A.; Inoue, T.; Kimura, M.; Kunimasa, K.; Nakahama, K.; Taniguchi, Y.; Shiroyama, T.; Isa, S.; Nishino, K.; et al. Metastatic site as a predictor of nivolumab efficacy in patients with advanced non-small cell lung cancer: A retrospective multicenter trial. PLoS ONE 2018, 13, e0192227. [Google Scholar] [CrossRef]
- Tournoy, K.G.; Thomeer, M.; Germonpré, P.; Derijcke, S.; De Pauw, R.; Galdermans, D.; Govaert, K.; Govaerts, E.; Schildermans, R.; Declercq, I.; et al. Does nivolumab for progressed metastatic lung cancer fulfill its promises? An efficacy and safety analysis in 20 general hospitals. Lung Cancer 2018, 115, 49–55. [Google Scholar] [CrossRef]
- Bagley, S.J.; Kothari, S.; Aggarwal, C.; Bauml, J.M.; Alley, E.W.; Evans, T.L.; Kosteva, J.A.; Ciunci, C.A.; Gabriel, P.E.; Thompson, J.C.; et al. Pretreatment neutrophil-to-lymphocyte ratio as a marker of outcomes in nivolumab-treated patients with advanced non-small-cell lung cancer. Lung Cancer 2017, 106, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Brustugun, O.T.; Sprauten, M.; Helland, Å. Real-world data on nivolumab treatment of non-small cell lung cancer. Acta Oncol. 2016, 56, 438–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, H.; Omori, S.; Nakashima, K.; Wakuda, K.; Ono, A.; Kenmotsu, H.; Naito, T.; Murakami, H.; Endo, M.; Takahashi, T. Response to the treatment immediately before nivolumab monotherapy may predict clinical response to nivolumab in patients with non-small cell lung cancer. Int. J. Clin. Oncol. 2017, 22, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Yi, F.; Yu, D.; Xu, J.; Wei, Y.; Zhang, W. Nivolumab provides improved effectiveness and safety compared with docetaxel as a second-line treatment for advanced non-small cell lung cancer: A systematic review and meta-analysis. Cancer Med. 2019, 8, 629–642. [Google Scholar] [CrossRef]
- Li, X.; Huang, C.; Xie, X.; Wu, Z.; Tian, X.; Wu, Y.; Du, X.; Shi, L. The impact of smoking status on the progression-free survival of non-small cell lung cancer patients receiving molecularly target therapy or immunotherapy versus chemotherapy: A meta-analysis. J. Clin. Pharm. Ther. 2021, 46, 256–266. [Google Scholar] [CrossRef] [PubMed]
- El-Osta, H.; Jafri, S. Predictors for clinical benefit of immune checkpoint inhibitors in advanced non-small-cell lung cancer: A meta-analysis. Immunotherapy 2019, 11, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Felip, E.; Ardizzoni, A.; Ciuleanu, T.; Cobo, M.; Laktionov, K.; Szilasi, M.; Califano, R.; Carcereny, E.; Griffiths, R.; Paz-Ares, L.; et al. CheckMate 171: A phase 2 trial of nivolumab in patients with previously treated advanced squamous non-small cell lung cancer, including ECOG PS 2 and elderly populations. Eur. J. Cancer 2020, 127, 160–172. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Hu, B.; Li, H. A meta-analysis of nivolumab for the treatment of advanced non-small-cell lung cancer. OncoTargets Ther. 2018, 11, 7691–7697. [Google Scholar] [CrossRef] [Green Version]
- Liang, J.; Li, M.; Sui, Q.; Hu, Z.; Bian, Y.; Huang, Y.; Zhan, C.; Jiang, W.; Wang, Q.; Tan, L. Compare the efficacy and safety of programmed cell death-1 (PD-1) and programmed cell death ligand-1 (PD-L1) inhibitors for advanced non-small cell lung cancer: A Bayesian analysis. Transl. Lung Cancer Res. 2020, 9, 1302–1323. [Google Scholar] [CrossRef]
- Stewart, M.; Norden, A.D.; Dreyer, N.; Henk, H.J.; Abernethy, A.P.; Chrischilles, E.; Kushi, L.; Mansfield, A.S.; Khozin, S.; Sharon, E.; et al. An Exploratory Analysis of Real-World End Points for Assessing Outcomes Among Immunotherapy-Treated Patients with Advanced Non-Small-Cell Lung Cancer. JCO Clin. Cancer Inform. 2019, 3, 1–15. [Google Scholar] [CrossRef]
- Knetki-Wróblewska, M.; Kowalski, D.M.; Krzakowski, M. Nivolumab for Previously Treated Patients with Non-Small-Cell Lung Cancer—Daily Practice versus Clinical Trials. J. Clin. Med. 2020, 9, 2273. [Google Scholar] [CrossRef]
- Passiglia, F.; Pilotto, S.; Facchinetti, F.; Bertolaccini, L.; Del Re, M.; Ferrara, R.; Franchina, T.; Malapelle, U.; Menis, J.; Passaro, A.; et al. Treatment of advanced non-small-cell lung cancer: The 2019 AIOM (Italian Association of Medical Oncology) clinical practice guidelines. Crit. Rev. Oncol. Hematol. 2020, 146, 102858. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab Versus Docetaxel in Previously Treated Patients with Advanced Non–Small-Cell Lung Cancer: Two-Year Outcomes from Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Zhang, W.; Yu, D.; Xu, J.; Wei, Y. The benefit and risk of nivolumab in non-small-cell lung cancer: A single-arm meta-analysis of noncomparative clinical studies and randomized controlled trials. Cancer Med. 2018, 7, 1642–1659. [Google Scholar] [CrossRef]
- Vokes, E.E.; Ready, N.; Felip, E.; Horn, L.; Burgio, M.A.; Antonia, S.J.; Arén Frontera, O.; Gettinger, S.; Holgado, E.; Spigel, D.; et al. Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (CheckMate 017 and CheckMate 057): 3-year update and outcomes in patients with liver metastases. Ann. Oncol. 2018, 29, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- National Heart Lung and Blood Institute. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 24 May 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | N Patients | Age Median (Range) | Male % | Smoker % | Histology % | Stage % | PS % | Prior RT % | Metastases % | Cycles ICIs % | Line % |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Adachi et al., 2020 [19] | 296 n | 70 (IQR: 64–76) | 70 | 80 | ADC: 62 Sq: 27 Other: 10 | nr | 0: 14 1: 61 2: 18 3: 5 4: 2 | 21 | Brain: 26 Liver: 14 | nr | 2: 49 3: 23 4: 13 >4: 15 |
| Chen et al., 2020 [20] | 97 62 n 35 p | 64 (IQR: 57–69) ≥65: 49 | 67 | 59 | Non sq: 60 Sq: 40 | III: 23 IV: 77 | 0–1: 84 ≥2: 15 | 28 | nr | nr | 2: 74 ≥3: 26 |
| Dupont et al., 2020 [21] | 191 n | 63 (IQR: 56–68) | 63 | 90 | ADC:71 Sq: 23 Other: 6 | III: 9 IV: 91 | 0: 19 1: 69 2: 8 3: 3 4: 0.5 | nr | Brain: 23 | nr | 2: 48 3: 38 >3: 14 |
| Figueiredo et al., 2020 [22] | 219 n | 64 (37–83) ≥75:15 | 70 | 69 | Non sq: 88 Sq: 12 | IIIB: 8 IV: 92 | 0: 12 1: 75 2: 13 | nr | Brain: 0 | 14 (1–52) | 2: 32 3: 38 ≥4: 29 |
| Joris et al., 2020 [23] | 324 n | 65 (28–86) ≥70: 33 ≥75: 14 | 65 | 85 | Non sq: 66 Sq: 28 Other: 6 | nr | 0–1: 69 ≥2: 27 Nos: 4 | nr | nr | nr | 2: 52 3: 28 >3: 20 |
| Martin et al., 2020 [24] | 109 n | Mean 65 (56–72) | 58 | 75 | Non sq: 78 Sq: 20 Nos: 2 | IV:100 | 0–1: 83 2–3: 16 Nos: 2 | 61 | nr | 10 (IQR: 3–18) | Median before: 2 (1–4) |
| Pantano et al., 2020 [25] | 294 n | 67 (34–90) | 68 | 86 | ADC: 54 Sq: 42 Other:4 | I-II: 11 * III: 23 IV: 65 | 0: 52 1: 44 2: 4 | 36 | Brain: 14 Liver: 12 | nr | 2: 65 3: 23 >3: 12 |
| Russo et al., 2020 [26] | 187 n | 67 (34–83) | 73 | 90 | Non sq: 54 Sq: 46 | IIIB or IV | 0: 45 1: 51 2: 4 | nr | nr | nr | Median 2 (2–8) |
| Velcheti et al., 2020 [27] | 349 p | 68 (37–84) ≥75:25 | 57 | 92 | Non sq: 58 Sq: 37 NSCLC nos: 4 | IIIB-IV: 86 | 0: 26 1: 49 2: 18 3: 7 | nr | Brain: 9 | nr | 2: 92 3: 7 ≥4: 1 |
| Kim et al., 2020 [28] | 83 n | 60 (IQR: 53–68) | 66 | 63 | Non sq: 70 Sq: 30 | IV:100 | 0–1: 76 ≥2: 24 | nr | CNS: 34 | nr | 2: 43 ≥3: 57 |
| Zhang et al., 2020 [29] | 73 n | nr | 75 | nr | ADC: 57 Non sq: 37 Other: 5 | III: 4 IV: 96 | 0–1: 90 ≥2: 10 | nr | Brain: 44 | nr | 2: 82 ≥3: 19 |
| Baldini et al., 2020 [30] | 1959 n | 66 (27–91) | 68 | 73 | Non sq: 81 Sq: 19 | nr | 0: 40 1: 52 2: 7 | nr | Brain: 23 Liver: 20 | 7 (1–55) | 2: 40 3: 29 ≥4: 30 |
| Crinò et al., 2019 [31] | 371 n | 68 (31–91) ≥75: 19 | 80 | 83 | Sq: 100 | ≥IIIB | 0: 36 1: 58 2: 6 | nr | CNS: 10 Liver: 17 | Mean: 6 (1–22) | 2: 44 3: 32 ≥4: 24 |
| Fukui et al., 2019 [32] | 52 n | 69 (46–83) ≥75:21 | 71 | 82 | ADC: 63 Sq: 31 Nos: 6 | III: 25 IV:75 | 0: 37 1: 58 2: 4 3: 2 | nr | Brain 15 Liver: 19 | 4 (1–43) | 2: 42 3: 29 ≥4: 29 |
| Grossi et al., 2019 [33] | 1588 n | 66 (27–89) | 65 | 71 | Non sq: 100 | IIIb or IV | 0: 41 1: 51 2: 7 | nr | CNS: 26 Liver: 21 | 7 (1–55) | 2: 24 3: 35 ≥4: 40 |
| Lang et al., 2019 [34] | 70 37 n 26 p 7 a | mean 66 (39–85) | 60 | 80 | ADC: 79 Sq: 30 | III: 4 IV: 96 | 0: 24 1: 63 2: 13 | nr | CNS: 23 | nr | 2: 100 |
| Merino Almazan et al., 2019 [35] | 221 n | Mean 64 >70: 27 | 84 | 69 | Non sq: 38 Sq: 60 | I-II: 8 * III: 38 IV: 54 | 0:28 1: 57 2: 14 | 9 | Brain: 10 Liver: 19 | Mean 9.7 (1–48) | 2: 65 3: 28 ≥4: 7 |
| Muchnik et al., 2019 [36] | 75 65 n 6 p 4 other | Mean 74 (70–92) | 52 | nr | ADC: 68 Other: 32 | IIIB: 3 IV: 97 | 0: 4 1: 47 2: 45 3: 4 | nr | nr | nr | 2: 16 3: 69 ≥4: 15 |
| Weis et al., 2019 [37] | 81 n | 64 | 48 | 85 | Non sq:60 Sq: 32 Other: 7 | IV: 100 | 0: 17 1: 54 ≥2: 28 | nr | nr | 3 (1–18) | 2: 64 ≥3: 36 |
| A 43 | 67 | 53 | 81 | Non sq: 67 Sq: 28 Other: 5 | IV:100 | 0: 16 1: 63 ≥: 21 | nr | nr | 4 (1–36) | 2: 74 ≥3: 26 | |
| Schwartzberg et al., 2019 [38] | 2071 1842 n 186 p 38 a | Mean 68 ≥75: 27 | 56 | 92 | Non sq: 64 Sq: 31 Nos: 5 | I-IIIA: 16 * IIIB-IV: 83 Nos: 2 | 0: 21 1: 50 2: 24 ≥3: 5 | nr | nr | nr | 2: 91 3: 9 |
| El Karak et al., 2019 [39] | 110 55 n 55 p | 66 | 75 | 88 | ADC: 57 Sq: 30 Nos: 13 | IV: 100 | Nr | nr | Brain: 17 Liver: 15 | nr | 2: 68 3: 24 ≥4: 8 |
| Spigel et al., 2019 [40] | 1426 n | 67 (23–93) ≥70: 9 | 54 | 87 | Non sq: 71 Sq: 28 Nos: 1 | IIIB: 8 IV: 91 | 0: 23 1: 66 2: 9 | nr | nr | nr | 2: 39 3: 28 ≥4: 32 |
| Areses Manrique et al., 2018 [41] | 188 n | 58 (45–81) ≥70: 7 | 77 | 91 | ADC: 60 Sq: 35 Nos: 5 | IIIB: 31 IV: 67 | 0: 8 1: 82 2: 10 | nr | CNS: 22 | 6 (1–34) | 2: 62 3: 24 ≥4: 14 |
| Garde-Noguera et al., 2018 [42] | 175 n | 61.5 ≥70: 26.8 | 73 | 91 | Non sq: 77 Sq: 23 | III: 13 IV: 87 | 0–1: 81 2: 19 | 17 | Brain: 22 Liver: 23 | 2: 37 3: 38 ≥4: 25 | |
| Fujimoto et al., 2018 [43] | 613 n | Mean 66.9 | 71 | 79 | ADC: 67 Sq: 22 Other: 10 | IIIB: 6 IV: 94 | 0–1: 77 2: 15 3–4: 8 | nr | nr | nr | 2: 33 3: 25 ≥4: 42 |
| Juergens et al., 2018 [44] | 472 n | 66 (36–92) >75: 13 | 43 | 54 | Non sq: 73 Sq: 26 Other: 1 | nr | 0–1: 86 ≥2: 9 Nos: 5 | nr | Brain: 13 | nr | 2: 44 3: 29 ≥4: 26 |
| Kobayashi et al., 2018 [45] | 142 n | 67 (34–85) ≥75: 27 | 75 | 80 | ADC: 58 Sq: 29 Other: 13 | IIIA: 13 IIIB: 15 IV: 60 | 0: 30 1: 53 2: 11 3: 6 | 32 | CNS: 19 | nr | 2: 40 ≥3: 60 |
| Nakaya et al., 2018 [46] | 101 n | 69 (45–84) | 77 | 84 | Non sq: 63 Sq: 37 | nr | 0–1: 84 ≥2: 16 | nr | nr | nr | 2: 18 3: 28 ≥4: 55 |
| Tamiya et al., 2018 [47] | 201 n | 68 (27–87) | 67 | 78 | ADC: 71 Sq: 21 Other: 8 | IV:100 | 0: 16 1: 60 2: 16 ≥3: 7 | nr | Brain: 25 Liver: 14 | nr | ≤3: 61 ≥4: 39 |
| Toumoy et al., 2018 [48] | 267 n | 66 (41–86) | 72 | 92 | Non sq: 73 Sq: 27 | III: 4 IV: 96 | 0: 16 1: 60 2: 24 | 52 | Brain: 17 Liver: 21 | 6 (1–43) | 2: 52 3: 33 ≥4: 16 |
| Bagley et al., 2017 [49] | 175 n | 68 (33–88) ≥75: 25 | 46 | 84 | Non sq: 76 Sq: 24 | nr | 0: 17 1: 58 2: 22 3: 3 | nr | CNS: 31 Liver: 23 | 5 (1–24) | 2: 54 3: 25 ≥4: 21 |
| Brustugun et al., ** 2017 [50] | 58 n | 65 (32–88) | 48 | nr | ADC: 55 Sq: 41 Other: 3 | I-II: 14 III: 42 IV: 62 | 0: 19 1: 57 2: 17 3: 7 | nr | Brain: 0 | 8.5 (1–32) | 2: 34 3: 47 ≥4:18 |
| Kobayashi et al., 2017 [51] | 50 n | 65 (39–76) | 60 | 62 | Non sq: 88 Sq: 12 | III: 20 IV: 58 rec: 22 | 0: 26 1: 64 2: 10 | 32 | nr | 4 (1–20) | 2: 20 3: 18 ≥4: 62 |
| Author | Follow-Up Months | Response % (95%CI) | PFS Months (95%CI) | OS Months (95%CI) | Adverse Event % |
|---|---|---|---|---|---|
| Adachi et al., 2020 [19] | 26.6 | ORR: 14 DCR: 55 CR: 1 PR: 13 SD: 40 | 3.0 (2.4–3.7) | 10.5 (8.3–12.5) | nr |
| Chen et al., 2020 [20] | 8.0 | ORR: 17 DCR: 61 PR: 16 SD: 44 | 5.0 | 18 | irAE any grade: 46 grade 3–4: 9 |
| Dupont et al., 2020 [21] | 24 (IQR: 20–29) | ORR: 26 | 2.8 (IQR: 1.6–10.4) | 9.1 (IQR: 3.6–28.9) | any grade: 30 grade 3–4: 5 |
| Figueiredo et al., 2020 [22] | 17.1 (1–34.1) | ORR: 22 DCR: 53 CR: 1 PR: 21 SD: 31 | 4.9 (3.9–6.1) | 13.2 (9.9–16.5) | any grade: 62 |
| Joris et al., 2020 [23] | Nr | ORR: 21 CR: 4 PR: 17 | 3.8 (2.5–5.1) | 8.6 (6.8–10.4) | any grade: 57 grade 3–4: 17 |
| Martin et al., 2020 [24] | 8.83 (0.2–33.7) | ORR: 29 DCR: 60 CR: 2 PR: 27 SD: 31 | 6.1 (range 2.4–13.1) | nr | any grade: 79 grade 2–3: 28 |
| Pantano et al., 2020 [25] | nr | ORR: 34 DCR: 65 CR: 1 PR: 34 SD: 30 | DSS: 14 (range 1-nr) | nr | any grade: 36 grade ≥ 3: 9 |
| Russo et al., 2020 [26] | nr | ORR: 36 DCR: 67 PR: 36 SD: 31 | 7.0 (6–10) | 13 (11–16) | nr |
| Velcheti et al., 2020 [27] | 8.1 (0.01–39.2) | nr | nr | 13.8 (11.0–16.5) | nr |
| Kim et al., 2020 [28] | nr | ORR: 7 DCR: 52 PR: 7 SD: 45 | 2.6 (0.8–4.3) | 8.6 (5.6–11.6) | any grade: 32 grade 3–4: 8 |
| Zhang et al., 2020 [29] | 8 | ORR: 22 DCR: 55 PR: 22 SD: 33 | 3.6 | 14.8 | nr |
| Baldini et al., 2020 [30] | 16.4 | ORR: 18 DCR: 45 CR:1 PR: 17 SD: 27 | 3.3 (3.2–3.4) | 10.3 (9.4–11.2) | irAE any grade: 7 |
| Crinò et al., 2019 [31] | 7.1 (0.1–16.4) | ORR: 18 DCR: 47 CR:1 PR:17 SD: 29 | 4.2 (3.4–5.0) | 7.9 (6.2–9.6) | any grade: 29 grade 3–4: 6 |
| Fukui et al., 2019 [32] | 10.9 (IQ: 5.6–16.4) | ORR: 23 DCR: 44 PR: 23 SD: 21 | 2.1 (1.0–3.2) | 1-year: 59.9 | all any grade: 88 grade 3–4: 25 irAE any grade: 44 grade 3–4: 10 |
| Grossi et al., 2019 [33] | 8.1 (1–27.4) | ORR: 18 DCR: 44 CR: 1 PR: 18 SD: 26 | 3.0 (2.9–3.1) | 11.3 (10.2–12.4) | any grade: 33 grade 3–4: 6 |
| Lang et al., 2019 [34] | nr | ORR: 19 DCR: 37 CR: 1 PR: 17 SD: 19 | 4 (3–7) | 18 (13–nr) | nr |
| Merino Almazan et al., 2019 [35] | nr | ORR: 17 DCR: 49 CR: 1 PR: 16 SD: 33 | 5.3 (3.2–7.3) | 9.7 (7.6–11.8) | any grade: 71 |
| Muchnik et al., 2019 [36] | nr | ORR: 36 DCR: 52 PR: 36 SD: 16 | TTF 4.2 (2.0–5.8) | 8.2 (4.8–13.6) | irAE any grade: 37 grade 3–4: 8 |
| Weis et al., 2019 [37] | 7.5 (0.5–35.4) | ORR: 15 DCR: 30 PR: 15 SD: 15 | 2.2 (1.7–2.8) | 8.4 (6.3–11.2) | any grade: 70 |
| 4.9 (0.6–13.5) | ORR: 14 DCR: 26 PR: 14 SD: 11 | 2.0 (1.8–2.7) | 6.5 (4.7–nr) | any grade: 65 | |
| Schwartzberg et al., 2019 [38] | 5.7 (0.03–32.5) | nr | nr | 9.4 (8.9–9.9) | nr |
| El Karak et al., 2019 [39] | nr | ORR: 25 DCR: 57 CR: 3 PR: 22 SD: 31 | 4 (2.6–5.4) | 8.1 (2.8–13.4) | irAE any grade: 18 |
| Spigel et al., 2019 [40] | 7.9 | nr | nr | 9.1 (8.3–10.4) | Total AE any gr:62 gr 3–4:15 irAE any gr:37 grade 3–4:6 |
| Areses Manrique et al., 2018 [41] | nr | ORR: 25 DCR: 51 CR: 2 PR: 24 SD: 25 | 4.8 (3.7–6.0) | 12.8 (9.1–16.6) | any grade: 78 grade 3–4: 5 |
| Garde-Noguera et al., 2018 [42] | nr | ORR: 14 | 2.7 (2.0–3.4) | 5.8 (3.7–7.9) | grade 3–4: 11 |
| Fujimoto et al., 2018 [43] | nr | ORR: 20 DCR: 44 CR: 1 PR: 19 SD: 4 | 1-year: 18% | 1-year: 54% | irAE grade ≥3: 11 |
| Juergens et al., 2018 [44] | 9.3 (0.03–24.5) | nr | 3.5 (3.2–4.0) | 12.0 (11–13.9) | Nr |
| Kobayashi et al., 2018 [45] | nr | ORR: 17 (12–24) DCR: 62 (54–70) PR: 17 SD: 45 | 1.9 (1.7–2.2) | nr | any grade: 45 grade 3–4: 13 grade 5: 1 |
| Nakaya et al., 2018 [46] | 8.9 | ORR: 26 DCR: 61 PR: 25 SD: 35 | 3.2 | 17.0 | all any grade: 60 irAE any grade: 40 |
| Tamiya et al., 2018 [47] | 12 | ORR: 16 DCR: 52 | 2.9 (2.0–3.6) | nr | nr |
| Toumoy et al., 2018 [48] | nr | ORR: 23 DCR: 48 CR: 17 PR: 22 SD: 25 | 3.7 (2.9–4.5) | 7.8 (6.3–9.3) | grade 3–4: 21 |
| Bagley et al., 2017 [49] | nr | ORR: 19.4 | 2.1 (1.9–2.6) | 6.5 (5.2–8.0) | irAE any grade: 16 grade 3–4: 3 |
| Brustugun et al., 2017 [50] * | 14 | nr | 4 | 12 | any grade: 31 grade ≥3: 5 |
| Kobayashi et al., 2017 [51] | nr | ORR: 18 DCR: 42 PR: 18 SD: 24 | 2.1 | nr | nr |
| Outcome | Age | Liver Metastases | CNS Metastases | |||
|---|---|---|---|---|---|---|
| N | N | N | ||||
| ORR | 22 | 0.21 (0.18–0.24) | 12 | 0.20 (0.16–0.23) | 19 | 0.20 (0.17–0.23) |
| DCR | 18 | 0.52 (0.48–0.57) | 10 | 0.47 (0.46–0.49) | 16 | 0.51 (0.47–0.55) |
| PFS | 18 | 3.25 (2.73–3.87) | 11 | 3.11 (2.61–3.72) | 17 | 3.15 (2.75–3.60) |
| OS | 17 | 9.77 (8.53–11.20) | 9 | 8.65 (7.23–10.36) | 15 | 9.96 (8.43–11.76) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mencoboni, M.; Ceppi, M.; Bruzzone, M.; Taveggia, P.; Cavo, A.; Scordamaglia, F.; Gualco, M.; Filiberti, R.A. Effectiveness and Safety of Immune Checkpoint Inhibitors for Patients with Advanced Non Small-Cell Lung Cancer in Real-World: Review and Meta-Analysis. Cancers 2021, 13, 1388. https://doi.org/10.3390/cancers13061388
Mencoboni M, Ceppi M, Bruzzone M, Taveggia P, Cavo A, Scordamaglia F, Gualco M, Filiberti RA. Effectiveness and Safety of Immune Checkpoint Inhibitors for Patients with Advanced Non Small-Cell Lung Cancer in Real-World: Review and Meta-Analysis. Cancers. 2021; 13(6):1388. https://doi.org/10.3390/cancers13061388
Chicago/Turabian StyleMencoboni, Manlio, Marcello Ceppi, Marco Bruzzone, Paola Taveggia, Alessia Cavo, Francesca Scordamaglia, Marina Gualco, and Rosa Angela Filiberti. 2021. "Effectiveness and Safety of Immune Checkpoint Inhibitors for Patients with Advanced Non Small-Cell Lung Cancer in Real-World: Review and Meta-Analysis" Cancers 13, no. 6: 1388. https://doi.org/10.3390/cancers13061388