
The Underlying Biology and Therapeutic Vulnerabilities of Leptomeningeal Metastases in Adult Solid Cancers

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
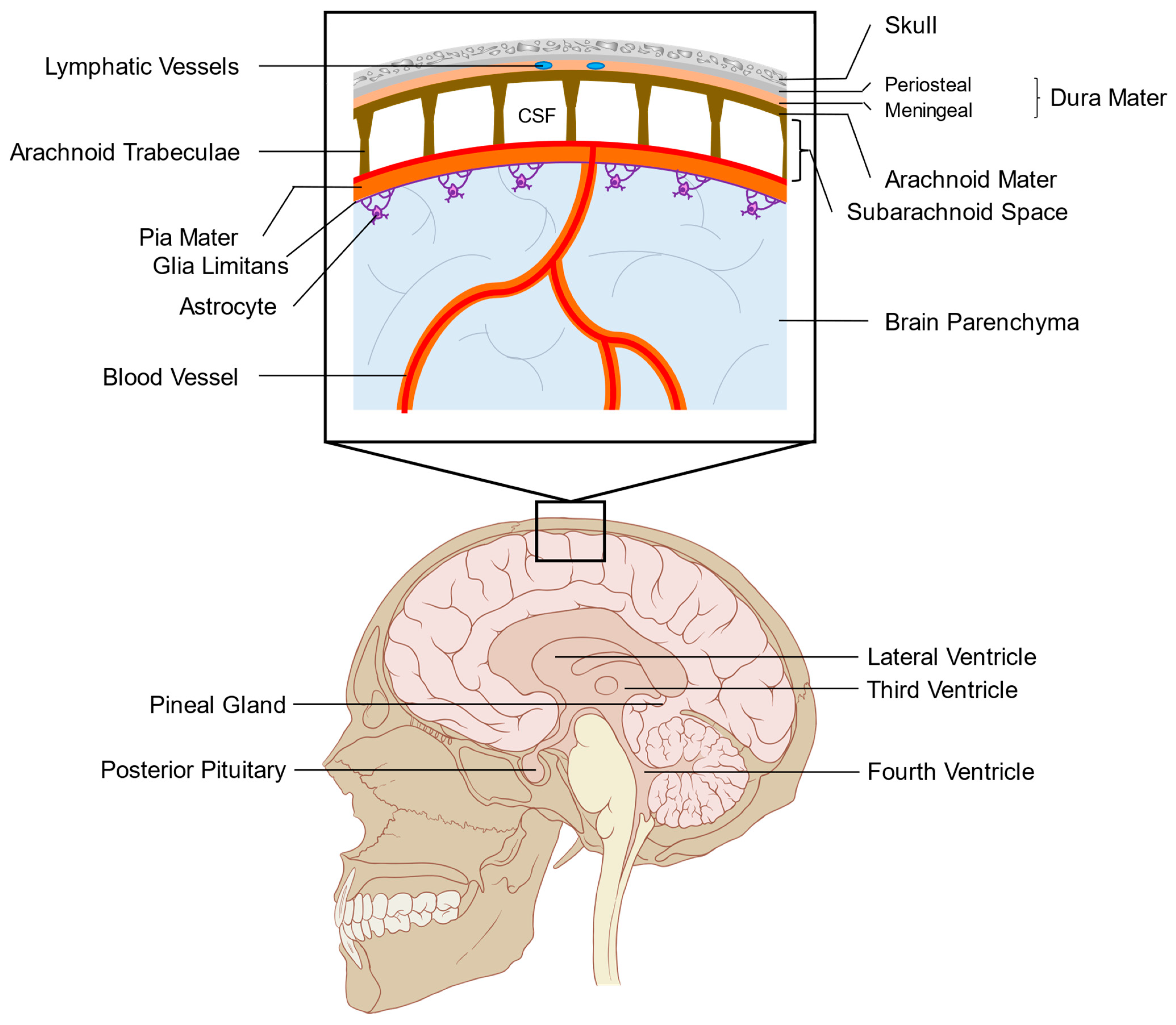
2. Anatomy and Function of the Leptomeninges
3. Defining LM by the Route of Entry
4. Diagnosis of LM
4.1. Neurological Evaluation
4.2. CSF Cytology
4.3. Imaging-Based Approaches
5. Treatment Approaches for LM
5.1. Systemic and Intrathecal Therapies
5.2. Radiation Therapies
6. Applying Pre-Clinical Animal Models of LM to Study Its Underlying Biology
7. Avenues of Future Investigation and Conclusions
8. Conclusions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Graber, J.; Kesari, S. Leptomeningeal Metastases. Curr. Treat. Opt. Oncol. 2018, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Waki, F.; Ando, M.; Takashima, A.; Yonemori, K.; Nokihara, H.; Miyake, M.; Tateishi, U.; Tsuta, K.; Shimada, Y.; Fujiwara, Y.; et al. Prognostic factors and clinical outcomes in patients with leptomeningeal metastasis from solid tumors. J. Neuro-Oncol. 2009, 93, 205–212. [Google Scholar] [CrossRef]
- Seute, T.; Leffers, P.; Velde, G.P.M.T.; Twijnstra, A. Leptomeningeal metastases from small cell lung carcinoma. Cancer 2005, 104, 1700–1705. [Google Scholar] [CrossRef]
- Brufsky, A.M.; Mayer, M.; Rugo, H.S.; Kaufman, P.A.; Tan-Chiu, E.; Tripathy, D.; Tudor, I.C.; Wang, L.I.; Brammer, M.G.; Shing, M.; et al. Central Nervous System Metastases in Patients with HER2-Positive Metastatic Breast Cancer: Incidence, Treatment, and Survival in Patients from registHER. Clin. Cancer Res. 2011, 17, 4834–4843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellerino, A.; Bertero, L.; Rudà, R.; Soffietti, R. Neoplastic meningitis in solid tumors: From diagnosis to personalized treatments. Ther. Adv. Neurol. Disord. 2018, 11, 1756286418759618. [Google Scholar] [CrossRef]
- Harstad, L.; Hess, K.R.; Groves, M.D. Prognostic factors and outcomes in patients with leptomeningeal melanomatosis. Neuro-Oncology 2008, 10, 1010–1018. [Google Scholar] [CrossRef] [Green Version]
- Rudnicka, H.; Niwińska, A.; Murawska, M. Breast cancer leptomeningeal metastasis--the role of multimodality treatment. J. Neurooncol. 2007, 84, 57–62. [Google Scholar] [CrossRef]
- Lee, S.J.; Lee, J.I.; Nam, D.-H.; Ahn, Y.C.; Han, J.H.; Sun, J.-M.; Ahn, J.S.; Park, K.; Ahn, M.-J. Leptomeningeal Carcinomatosis in Non–Small-Cell Lung Cancer Patients: Impact on Survival and Correlated Prognostic Factors. J. Thorac. Oncol. 2013, 8, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Foppen, M.H.G.; Brandsma, D.; Blank, C.U.; Van Thienen, J.V.; Haanen, J.B.; Boogerd, W. Targeted treatment and immunotherapy in leptomeningeal metastases from melanoma. Ann. Oncol. 2016, 27, 1138–1142. [Google Scholar] [CrossRef]
- Gwak, H.-S.; Joo, J.; Kim, S.; Yoo, H.; Shin, S.H.; Han, J.-Y.; Kim, H.T.; Lee, S.H.; Lee, S.H. Analysis of Treatment Outcomes of Intraventricular Chemotherapy in 105 Patients for Leptomeningeal Carcinomatosis from Non–Small-Cell Lung Cancer. J. Thorac. Oncol. 2013, 8, 599–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Rhun, E.; Taillibert, S.; Zairi, F.; Kotecki, N.; Devos, P.; Mailliez, A.; Servent, V.; Vanlemmens, L.; Vennin, P.; Boulanger, T.; et al. A retrospective case series of 103 consecutive patients with leptomeningeal metastasis and breast cancer. J. Neuro-Oncol. 2013, 113, 83–92. [Google Scholar] [CrossRef]
- De Azevedo, C.R.; Cruz, M.R.; Chinen, L.T.; Peres, S.V.; Peterlevitz, M.A.; de Azevedo Pereira, A.E.; Fanelli, M.F.; Gimenes, D.L. Meningeal carcinomatosis in breast cancer: Prognostic factors and outcome. J. Neurooncol. 2011, 104, 565–572. [Google Scholar] [CrossRef]
- Boire, A.; Zou, Y.; Shieh, J.; Macalinao, D.G.; Pentsova, E.; Massagué, J. Complement Component 3 Adapts the Cerebrospinal Fluid for Leptomeningeal Metastasis. Cell 2017, 168, 1101–1113. [Google Scholar] [CrossRef] [Green Version]
- Norris, L.K.; Grossman, S.A.; Olivi, A. Neoplastic meningitis following surgical resection of isolated cerebellar metastasis: A potentially preventable complication. J. Neuro-Oncol. 1997, 32, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.H.; Lee, S.H.; Kim, S.; Joo, J.; Yoo, H.; Lee, S.H.; Shin, S.H.; Gwak, H.-S. Risk for leptomeningeal seeding after resection for brain metastases: Implication of tumor location with mode of resection. J. Neurosurg. 2012, 116, 984–993. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.P.; Keles, G.E.; Waite, M.; Temkin, N.; Berger, M.S. Ventricular entry during resection of malignant gliomas: Effect on intracranial cerebrospinal fluid tumor dissemination. J. Neurosurg. 1994, 80, 834–839. [Google Scholar] [CrossRef]
- Suki, D.; Hatiboglu, M.A.; Patel, A.J.; Weinberg, J.S.; Groves, M.D.; Mahajan, A.; Sawaya, R. Comparative risk of leptomeningeal dissemination of cancer after surgery or stereotactic radiosurgery for a single supratentorial solid tumor metastasis. Neurosurgery 2009, 64, 664–676. [Google Scholar] [CrossRef] [PubMed]
- van der Ree, T.C.; Dippel, D.W.; Avezaat, C.J.; Smitt, P.S.; Vecht, C.J.; van den Bent, M.J. Leptomeningeal metastasis after surgical resection of brain metastases. J. Neurol. Neurosurg. Psychiatry 1999, 66, 225–227. [Google Scholar] [CrossRef] [Green Version]
- Abouharb, S.; Ensor, J.; Loghin, M.E.; Katz, R.L.; Moulder, S.L.; Esteva, F.J.; Smith, B.D.; Valero, V.; Hortobagyi, G.N.; Melhem-Bertrandt, A. Leptomeningeal disease and breast cancer: The importance of tumor subtype. Breast Cancer Res. Treat. 2014, 146, 477–486. [Google Scholar] [CrossRef]
- Niwińska, A.; Rudnicka, H.; Murawska, M. Breast cancer leptomeningeal metastasis: Propensity of breast cancer subtypes for leptomeninges and the analysis of factors influencing survival. Med. Oncol. 2013, 30, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Liao, B.-C.; Lee, J.-H.; Lin, C.-C.; Chen, Y.-F.; Chang, C.-H.; Ho, C.-C.; Shih, J.-Y.; Yu, C.-J.; Yang, J.C.-H. Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors for Non–Small-Cell Lung Cancer Patients with Leptomeningeal Carcinomatosis. J. Thorac. Oncol. 2015, 10, 1754–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gainor, J.F.; Ou, S.-H.I.; Logan, J.; Borges, L.F.; Shaw, A.T. The Central Nervous System as a Sanctuary Site in ALK-Positive Non–Small-Cell Lung Cancer. J. Thorac. Oncol. 2013, 8, 1570–1573. [Google Scholar] [CrossRef] [Green Version]
- Smedby, K.E.; Brandt, L.; Bäcklund, M.L.; Blomqvist, P. Brain metastases admissions in Sweden between 1987 and 2006. Br. J. Cancer 2009, 101, 1919–1924. [Google Scholar] [CrossRef] [Green Version]
- Deeken, J.F.; Löscher, W. The Blood-Brain Barrier and Cancer: Transporters, Treatment, and Trojan Horses. Clin. Cancer Res. 2007, 13, 1663–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Q.; Balasubramanian, K.; Fan, M.; Kim, S.-J.; Guo, L.; Wang, H.; Bar-Eli, M.; Aldape, K.D.; Fidler, I.J. Reactive Astrocytes Protect Melanoma Cells from Chemotherapy by Sequestering Intracellular Calcium through Gap Junction Communication Channels1. Neoplasia 2010, 12, 748–754. [Google Scholar] [CrossRef] [Green Version]
- Weller, R.O.; Sharp, M.M.; Christodoulides, M.; Carare, R.O.; Møllgård, K. The meninges as barriers and facilitators for the movement of fluid, cells and pathogens related to the rodent and human CNS. Acta Neuropathol. 2018, 135, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Louveau, A.; Smirnov, I.; Keyes, T.J.; Eccles, J.D.; Rouhani, S.J.; Peske, J.D.; Derecki, N.C.; Castle, D.; Mandell, J.W.; Lee, K.S.; et al. Structural and functional features of central nervous system lymphatic vessels. Nat. Cell Biol. 2015, 523, 337–341. [Google Scholar] [CrossRef]
- Mastorakos, P.; McGAVERN, D.B. The anatomy and immunology of vasculature in the central nervous system. Sci. Immunol. 2019, 4, eaav0492. [Google Scholar] [CrossRef] [PubMed]
- Oda, Y.; Nakanishi, I. Ultrastructure of the mouse leptomeninx. J. Comp. Neurol. 1984, 225, 448–457. [Google Scholar] [CrossRef]
- Alcolado, R.; Weller, R.O.; Parrish, E.P.; Garrod, D. The Cranial Arachnoid and Pia Mater in Man: Anatomical and Ultrastructural Observations. Neuropathol. Appl. Neurobiol. 1988, 14, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.W.J.; Sharp, M.M.; Albargothy, N.J.; Fernandes, R.; Hawkes, C.A.; Verma, A.; Weller, R.O.; Carare, R.O. Vascular basement membranes as pathways for the passage of fluid into and out of the brain. Acta Neuropathol. 2016, 131, 725–736. [Google Scholar] [CrossRef] [Green Version]
- Bentivoglio, M.; Kristensson, K.; Rottenberg, M.E. Circumventricular Organs and Parasite Neurotropism: Neglected Gates to the Brain? Front. Immunol. 2018, 9, 2877. [Google Scholar] [CrossRef]
- Spector, R.; Snodgrass, S.R.; Johanson, C.E. A balanced view of the cerebrospinal fluid composition and functions: Focus on adult humans. Exp. Neurol. 2015, 273, 57–68. [Google Scholar] [CrossRef] [Green Version]
- Redzic, Z.B.; Segal, M.B. The structure of the choroid plexus and the physiology of the choroid plexus epithelium. Adv. Drug Deliv. Rev. 2004, 56, 1695–1716. [Google Scholar] [CrossRef]
- Kaur, C.; Rathnasamy, G.; Ling, E.-A. The Choroid Plexus in Healthy and Diseased Brain. J. Neuropathol. Exp. Neurol. 2016, 75, 198–213. [Google Scholar] [CrossRef] [PubMed]
- Da Mesquita, S.; Louveau, A.; Vaccari, A.; Smirnov, I.; Cornelison, R.C.; Kingsmore, K.M.; Contarino, C.; Onengut-Gumuscu, S.; Farber, E.; Raper, D.; et al. Functional aspects of meningeal lymphatics in ageing and Alzheimer’s disease. Nat. Cell Biol. 2018, 560, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Smalley, I.; Law, V.; Wyatt, C.; Evernden, B.R.; Fang, B.; Koomen, J.M.; Welsh, E.A.; Macaulay, R.J.; Forsyth, P.A.; Smalley, K.S. Proteomic Analysis of CSF from Patients with Leptomeningeal Melanoma Metastases Identifies Signatures Associated with Disease Progression and Therapeutic Resistance. Clin. Cancer Res. 2020, 26, 2163–2175. [Google Scholar] [CrossRef] [Green Version]
- Chi, Y.; Remsik, J.; Kiseliovas, V.; Derderian, C.; Sener, U.; Alghader, M.; Saadeh, F.; Nikishina, K.; Bale, T.; Iacobuzio-Donahue, C.; et al. Cancer cells deploy lipocalin-2 to collect limiting iron in leptomeningeal metastasis. Science 2020, 369, 276–282. [Google Scholar] [PubMed]
- Bos, P.D.; Zhang, X.H.-F.; Nadal, C.; Shu, W.; Gomis, R.R.; Nguyen, D.X.; Minn, A.J.; Van De Vijver, M.J.; Gerald, W.L.; Foekens, J.A.; et al. Genes that mediate breast cancer metastasis to the brain. Nat. Cell Biol. 2009, 459, 1005–1009. [Google Scholar] [CrossRef]
- Kokkoris, C.P. Leptomeningeal carcinomatosis: How does cancer reach the pia-arachnoid? Cancer 1983, 51, 154–160. [Google Scholar] [CrossRef]
- Boyle, R.; Thomas, M.; Adams, J.H. Diffuse involvement of the leptomeninges by tumour--a clinical and pathological study of 63 cases. Postgrad. Med. J. 1980, 56, 149–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, H.; Price, T.T.; Cantelli, G.; Ngo, B.; Warner, M.J.; Olivere, L.; Ridge, S.M.; Jablonski, E.M.; Therrien, J.; Tannheimer, S.; et al. Leukaemia hijacks a neural mechanism to invade the central nervous system. Nat. Cell Biol. 2018, 560, 55–60. [Google Scholar] [CrossRef]
- Clarke, J.L.; Perez, H.R.; Jacks, L.M.; Panageas, K.S.; DeAngelis, L.M. Leptomeningeal metastases in the MRI era. Neurology 2010, 74, 1449–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.E.; Patel, A.S.; Prabhu, V.V.; Dicker, D.T.; Sheehan, J.M.; Glantz, M.; El-Deiry, W.S. COX-2 Drives Metastatic Breast Cells from Brain Lesions into the Cerebrospinal Fluid and Systemic Circulation. Cancer Res. 2014, 74, 2385–2390. [Google Scholar] [CrossRef] [Green Version]
- Dankner, M.; Caron, M.; Al-Saadi, T.; Yu, W.; Ouellet, V.; Ezzeddine, R.; Maritan, S.M.; Annis, M.G.; Le, P.U.; Nadaf, J.; et al. Invasive growth associated with Cold-Inducible RNA-Binding Protein expression drives recurrence of surgically resected brain metastases. Neuro-Oncology 2021. [Google Scholar] [CrossRef]
- Kienast, Y.; Von Baumgarten, L.; Fuhrmann, M.; Klinkert, W.E.F.; Goldbrunner, R.; Herms, J.; Winkler, F. Real-time imaging reveals the single steps of brain metastasis formation. Nat. Med. 2010, 16, 116–122. [Google Scholar] [CrossRef]
- Ahn, J.H.; Cho, H.; Kim, J.-H.; Kim, S.H.; Ham, J.-S.; Park, I.; Suh, S.H.; Hong, S.P.; Song, J.-H.; Hong, Y.-K.; et al. Meningeal lymphatic vessels at the skull base drain cerebrospinal fluid. Nat. Cell Biol. 2019, 572, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Shayan, R.; Achen, M.G.; Stacker, S.A. Lymphatic vessels in cancer metastasis: Bridging the gaps. Carcinogenesis 2006, 27, 1729–1738. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, R.S.; Turner, B.E.; Asher, A.L.; Marcrom, S.R.; Fiveash, J.B.; Foreman, P.M.; Press, R.H.; Patel, K.R.; Curran, W.J.; Breen, W.G.; et al. A multi-institutional analysis of presentation and outcomes for leptomeningeal disease recurrence after surgical resection and radiosurgery for brain metastases. Neuro-Oncology 2019, 21, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Devos, P.; Weller, J.; Seystahl, K.; Mo, F.; Compter, A.; Berghoff, A.S.; Jongen, J.L.; Wolpert, F.; Rudà, R.; et al. Prognostic validation and clinical implications of the EANO ESMO classification of leptomeningeal metastasis from solid tumors. Neuro-Oncology 2020. [Google Scholar] [CrossRef]
- Le Rhun, E.; Weller, M.; Brandsma, D.; Bent, M.V.D.; De Azambuja, E.; Henriksson, R.; Boulanger, T.; Peters, S.; Watts, C.; Wick, W.; et al. EANO–ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with leptomeningeal metastasis from solid tumours. Ann. Oncol. 2017, 28, iv84–iv99. [Google Scholar] [CrossRef] [PubMed]
- Nayar, G.; Ejikeme, T.; Chongsathidkiet, P.; Elsamadicy, A.A.; Blackwell, K.L.; Clarke, J.M.; Lad, S.P.; Fecci, P.E. Leptomeningeal disease: Current diagnostic and therapeutic strategies. Oncotarget 2017, 8, 73312–73328. [Google Scholar] [CrossRef] [Green Version]
- van Bussel, M.T.; Pluim, D.; Bol, M.; Beijnen, J.H.; Schellens, J.H.; Brandsma, D. EpCAM-based assays for epithelial tumor cell detection in cerebrospinal fluid. J. Neurooncol. 2018, 137, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cordone, I.; Masi, S.; Summa, V.; Carosi, M.; Vidiri, A.; Fabi, A.; Pasquale, A.; Conti, L.; Rosito, I.; Carapella, C.M.; et al. Overexpression of syndecan-1, MUC-1, and putative stem cell markers in breast cancer leptomeningeal metastasis: A cerebrospinal fluid flow cytometry study. Breast Cancer Res. 2017, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Tu, Q.; Bittencourt, M.D.C.; Farre, I.; Mortier, L.; Cai, H.; Kohler, C.; Faure, G.C. Detection and quantification of CSF malignant cells by the CellSearch® technology in patients with melanoma leptomeningeal metastasis. Med. Oncol. 2013, 30, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Fleisher, M.; Rosenblum, M.; Lin, O.; Boire, A.; Briggs, S.; Bensman, Y.; Hurtado, B.; Shagabayeva, L.; DeAngelis, L.M.; et al. Cerebrospinal fluid circulating tumor cells: A novel tool to diagnose leptomeningeal metastases from epithelial tumors. Neuro-Oncology 2017, 19, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Torre, M.; Lee, E.Q.; Chukwueke, U.N.; Nayak, L.; Cibas, E.S.; Lowe, A.C. Integration of rare cell capture technology into cytologic evaluation of cerebrospinal fluid specimens from patients with solid tumors and suspected leptomeningeal metastasis. J. Am. Soc. Cytopathol. 2020, 9, 45–54. [Google Scholar] [CrossRef] [PubMed]
- van Bussel, M.T.; Pluim, D.; Kerklaan, B.M.; Bol, M.; Sikorska, K.; Linders, D.T.; van den Broek, D.; Beijnen, J.H.; Schellens, J.H.; Brandsma, D. Circulating epithelial tumor cell analysis in CSF in patients with leptomeningeal metastases. Neurology 2020, 94, e521–e528. [Google Scholar] [CrossRef]
- Malani, R.; Fleisher, M.; Kumthekar, P.; Lin, X.; Omuro, A.; Groves, M.D.; Lin, N.U.; Melisko, M.; Lassman, A.B.; Jeyapalan, S.; et al. Cerebrospinal fluid circulating tumor cells as a quantifiable measurement of leptomeningeal metastases in patients with HER2 positive cancer. J. Neuro-Oncol. 2020, 148, 599–606. [Google Scholar] [CrossRef]
- Ying, S.; Ke, H.; Ding, Y.; Liu, Y.; Tang, X.; Yang, D.; Li, M.; Liu, J.; Yu, B.; Xiang, J.; et al. Unique genomic profiles obtained from cerebrospinal fluid cell-free DNA of non-small cell lung cancer patients with leptomeningeal metastases. Cancer Biol. Ther. 2019, 20, 562–570. [Google Scholar] [CrossRef]
- Pan, Z.; Yang, G.; He, H.; Gao, P.; Jiang, T.; Chen, Y.; Zhao, G. Identification of Cerebrospinal Fluid MicroRNAs Associated with Leptomeningeal Metastasis From Lung Adenocarcinoma. Front. Oncol. 2020, 10, 387. [Google Scholar] [CrossRef]
- Suryavanshi, M.; Jaipuria, J.; Panigrahi, M.K.; Goyal, N.; Singal, R.; Mehta, A.; Batra, U.; Doval, D.; Talwar, V. CSF cell-free DNA EGFR testing using DdPCR holds promise over conventional modalities for diagnosing leptomeningeal involvement in patients with non-small cell lung cancer. Lung Cancer 2020, 148, 33–39. [Google Scholar] [CrossRef]
- Boire, A.; Brandsma, D.; Brastianos, P.K.; Le Rhun, E.; Ahluwalia, M.; Junck, L.; Glantz, M.; Groves, M.D.; Lee, E.Q.; Lin, N.; et al. Liquid biopsy in central nervous system metastases: A RANO review and proposals for clinical applications. Neuro-Oncology 2019, 21, 571–584. [Google Scholar] [CrossRef] [Green Version]
- Le Rhun, E.; Devos, P.; Boulanger, T.; Smits, M.; Brandsma, D.; Rudà, R.; Furtner, J.; Hempel, J.-M.; Postma, T.J.; Roth, P.; et al. The RANO Leptomeningeal Metastasis Group proposal to assess response to treatment: Lack of feasibility and clinical utility and a revised proposal. Neuro-Oncology 2019, 21, 648–658. [Google Scholar] [CrossRef]
- Chamberlain, M.C.; Junck, L.; Brandsma, D.; Soffietti, R.; Rudà, R.; Raizer, J.; Boogerd, W.; Taillibert, S.; Groves, M.D.; Le Rhun, E.; et al. Leptomeningeal metastases: A RANO proposal for response criteria. Neuro-Oncology 2016, 19, 484–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, B.E.; Prabhu, R.S.; Burri, S.H.; Brown, P.D.; Pollom, E.L.; Milano, M.T.; Weiss, S.E.; Iv, M.; Fischbein, N.; Soliman, H.; et al. Nodular Leptomeningeal Disease—A Distinct Pattern of Recurrence After Postresection Stereotactic Radiosurgery for Brain Metastases: A Multi-institutional Study of Interobserver Reliability. Int. J. Radiat. Oncol. 2020, 106, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.K.; Sahgal, A.; Detsky, J.; Atenafu, E.G.; Myrehaug, S.; Tseng, C.-L.; Husain, Z.; Heyn, C.; Maralani, P.; Ruschin, M.; et al. Predictors of leptomeningeal disease following hypofractionated stereotactic radiotherapy for intact and resected brain metastases. Neuro-Oncology 2020, 22, 84–93. [Google Scholar] [CrossRef]
- Cagney, D.N.; Lamba, N.; Sinha, S.; Catalano, P.J.; Bi, W.L.; Alexander, B.M.; Aizer, A.A. Association of Neurosurgical Resection with Development of Pachymeningeal Seeding in Patients with Brain Metastases. JAMA Oncol. 2019, 5, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, A.; Jordan, L.; Rozner, R.; Patil, S.; Boire, A.; Pentsova, E.; Seidman, A.D. Characteristics and Outcomes of Patients with Breast Cancer with Leptomeningeal Metastasis. Clin. Breast Cancer 2017, 17, 23–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, M.; Soffietti, R.; Raizer, J.; Rudà, R.; Brandsma, D.; Boogerd, W.; Taillibert, S.; Groves, M.D.; Le Rhun, E.; Junck, L.; et al. Leptomeningeal metastasis: A Response Assessment in Neuro-Oncology critical review of endpoints and response criteria of published randomized clinical trials. Neuro-Oncology 2014, 16, 1176–1185. [Google Scholar] [CrossRef] [Green Version]
- Hitchins, R.N.; Bell, D.R.; Woods, R.L.; Levi, J.A. A prospective randomized trial of single-agent versus combination chemotherapy in meningeal carcinomatosis. J. Clin. Oncol. 1987, 5, 1655–1662. [Google Scholar] [CrossRef]
- Grossman, S.A.; Finkelstein, D.M.; Ruckdeschel, J.C.; Trump, D.L.; Moynihan, T.; Ettinger, D.S. Randomized prospective comparison of intraventricular methotrexate and thiotepa in patients with previously untreated neoplastic meningitis. Eastern Cooperative Oncology Group. J. Clin. Oncol. 1993, 11, 561–569. [Google Scholar] [CrossRef]
- Boogerd, W.; Bent, M.V.D.; Koehler, P.; Heimans, J.; Van Der Sande, J.; Aaronson, N.; Hart, A.; Benraadt, J.; Vecht, C. The relevance of intraventricular chemotherapy for leptomeningeal metastasis in breast cancer: A randomised study. Eur. J. Cancer 2004, 40, 2726–2733. [Google Scholar] [CrossRef]
- Groves, M.D.; Glantz, M.J.; Chamberlain, M.C.; Baumgartner, K.E.; Conrad, C.A.; Hsu, S.; Wefel, J.S.; Gilbert, M.R.; Ictech, S.; Hunter, K.U.; et al. A multicenter phase II trial of intrathecal topotecan in patients with meningeal malignancies. Neuro-Oncology 2008, 10, 208–215. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, W.R.; Schmid, M.; Glantz, M.; Miller, J.J. A randomized phase III/IV study to determine benefit and safety of cytarabine liposome injection for treatment of neoplastic meningitis. J. Clin. Oncol. 2006, 24, 1528. [Google Scholar] [CrossRef]
- Pan, Z.; Yang, G.; Cui, J.; Li, W.; Li, Y.; Gao, P.; Jiang, T.; Sun, Y.; Dong, L.; Song, Y.; et al. A Pilot Phase 1 Study of Intrathecal Pemetrexed for Refractory Leptomeningeal Metastases from Non-small-cell Lung Cancer. Front. Oncol. 2019, 9, 838. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Lee, E.Q.; Cohen, J.V.; Tolaney, S.M.; Lin, N.U.; Wang, N.; Chukwueke, U.; White, M.D.; Nayyar, N.; Kim, A.; et al. Single-arm, open-label phase 2 trial of pembrolizumab in patients with leptomeningeal carcinomatosis. Nat. Med. 2020, 26, 1280–1284. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Kim, S.-W.; Kim, D.-W.; Lee, J.-S.; Cho, B.C.; Ahn, J.-S.; Lee, D.H.; Kim, T.M.; Goldman, J.W.; Natale, R.B.; et al. Osimertinib in Patients with Epidermal Growth Factor Receptor Mutation–Positive Non–Small-Cell Lung Cancer and Leptomeningeal Metastases: The BLOOM Study. J. Clin. Oncol. 2020, 38, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Mrugala, M.M.; Kim, B.; Sharma, A.; Johnson, N.; Graham, C.; Kurland, B.F.; Gralow, J. Phase II Study of Systemic High-dose Methotrexate and Intrathecal Liposomal Cytarabine for Treatment of Leptomeningeal Carcinomatosis From Breast Cancer. Clin. Breast Cancer 2019, 19, 311–316. [Google Scholar] [CrossRef]
- Melisko, M.; Assefa, M.; Hwang, J.; DeLuca, A.; Park, J.W.; Rugo, H.S. Phase II study of irinotecan and temozolomide in breast cancer patients with progressing central nervous system disease. Breast Cancer Res. Treat. 2019, 177, 401–408. [Google Scholar] [CrossRef]
- Yang, T.J.; Wijetunga, N.A.; Yamada, J.; Wolden, S.; Mehallow, M.; Goldman, D.A.; Zhang, Z.; Young, R.J.; Kris, M.G.; Yu, H.A.; et al. Clinical trial of proton craniospinal irradiation for leptomeningeal metastases. Neuro-Oncology 2021, 23, 134–143. [Google Scholar] [CrossRef]
- Offin, M.; Luo, J.; Guo, R.; Lyo, J.K.; Falcon, C.; Dienstag, J.; Wilkins, O.; Chang, J.; Rudin, C.M.; Riely, G.; et al. CNS Metastases in Patients with MET Exon 14–Altered Lung Cancers and Outcomes with Crizotinib. JCO Precis. Oncol. 2020, 871–876. [Google Scholar] [CrossRef]
- Tolaney, S.M.; Sahebjam, S.; Le Rhun, E.; Bachelot, T.; Kabos, P.; Awada, A.; Yardley, D.; Chan, A.; Conte, P.; Diéras, V.; et al. A Phase II Study of Abemaciclib in Patients with Brain Metastases Secondary to Hormone Receptor–Positive Breast Cancer. Clin. Cancer Res. 2020. [Google Scholar] [CrossRef]
- Pan, Z.; Yang, G.; He, H.; Cui, J.; Li, W.; Yuan, T.; Chen, K.; Jiang, T.; Gao, P.; Sun, Y.; et al. Intrathecal pemetrexed combined with involved-field radiotherapy as a first-line intra-CSF therapy for leptomeningeal metastases from solid tumors: A phase I/II study. Ther. Adv. Med. Oncol. 2020, 12, 1758835920937953. [Google Scholar] [CrossRef]
- Nosaki, K.; Yamanaka, T.; Hamada, A.; Shiraishi, Y.; Harada, T.; Himeji, D.; Kitazaki, T.; Ebi, N.; Shimose, T.; Seto, T.; et al. Erlotinib for Non-Small Cell Lung Cancer with Leptomeningeal Metastases: A Phase II Study (LOGIK1101). Oncologist 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, M.-H.; Seong, M.; Kim, S.; Kang, J.-H.; Cho, B.; Lee, K.; Cho, E.; Sun, J.-M.; Lee, S.-H.; et al. A phase II, multicenter, two cohort study of 160 mg osimertinib in EGFR T790M-positive non-small-cell lung cancer patients with brain metastases or leptomeningeal disease who progressed on prior EGFR TKI therapy. Ann. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Jaeckle, K.A.; Dixon, J.G.; Anderson, S.K.; Moreno-Aspitia, A.; Colon-Otero, G.; Hebenstreit, K.; Patel, T.A.; Reddy, S.L.; Perez, E.A. Intra-CSF topotecan in treatment of breast cancer patients with leptomeningeal metastases. Cancer Med. 2020, 9, 7935–7942. [Google Scholar] [CrossRef] [PubMed]
- Kumthekar, P.; Tang, S.-C.; Brenner, A.J.; Kesari, S.; Piccioni, D.E.; Anders, C.K.; Carrillo, J.A.; Chalasani, P.; Kabos, P.; Puhalla, S.L.; et al. ANG1005, a Brain-Penetrating Peptide–Drug Conjugate, Shows Activity in Patients with Breast Cancer with Leptomeningeal Carcinomatosis and Recurrent Brain Metastases. Clin. Cancer Res. 2020, 26, 2789–2799. [Google Scholar] [CrossRef] [Green Version]
- Le Rhun, E.; Wallet, J.; Mailliez, A.; Le Deley, M.C.; Rodrigues, I.; Boulanger, T.; Lorgis, V.; Barrière, J.; Robin, Y.M.; Weller, M.; et al. Intrathecal liposomal cytarabine plus systemic therapy versus systemic chemotherapy alone for newly diagnosed leptomeningeal metastasis from breast cancer. Neuro-Oncology 2019, 22, 524–538. [Google Scholar] [CrossRef]
- Glantz, M.J.; Jaeckle, K.A.; Chamberlain, M.C.; Phuphanich, S.; Recht, L.; Swinnen, L.J.; Maria, B.; LaFollette, S.; Schumann, G.B.; Cole, B.F.; et al. A randomized controlled trial comparing intrathecal sustained-release cytarabine (DepoCyt) to intrathecal methotrexate in patients with neoplastic meningitis from solid tumors. Clin. Cancer Res. 1999, 5, 3394–3402. [Google Scholar]
- Glitza, I.C.; Phillips, S.; Brown, C.; Haymaker, C.L.; Bassett, R.L.; Lee, J.J.; Rohlfs, M.L.; Richard, J.; Iqbal, M.; John, I.; et al. Single-center phase I/Ib study of concurrent intrathecal (IT) and intravenous (IV) nivolumab (N) for metastatic melanoma (MM) patients (pts) with leptomeningeal disease (LMD). J. Clin. Oncol. 2020, 38, 10008. [Google Scholar] [CrossRef]
- Zagouri, F.; Zoumpourlis, P.; Le Rhun, E.; Bartsch, R.; Zografos, E.; Apostolidou, K.; Dimopoulos, M.-A.; Preusser, M. Intrathecal administration of anti-HER2 treatment for the treatment of meningeal carcinomatosis in breast cancer: A metanalysis with meta-regression. Cancer Treat. Rev. 2020, 88, 102046. [Google Scholar] [CrossRef]
- Figura, N.B.; Long, W.; Yu, M.; Robinson, T.J.; Mokhtari, S.; Etame, A.B.; Tran, N.D.; Diaz, R.; Soliman, H.; Han, H.S.; et al. Intrathecal trastuzumab in the management of HER2+ breast leptomeningeal disease: A single institution experience. Breast Cancer Res. Treat. 2018, 169, 391–396. [Google Scholar] [CrossRef]
- Bonneau, C.; Paintaud, G.; Trédan, O.; Dubot, C.; Desvignes, C.; Diéras, V.; Taillibert, S.; Tresca, P.; Turbiez, I.; Li, J.; et al. Phase I feasibility study for intrathecal administration of trastuzumab in patients with HER2 positive breast carcinomatous meningitis. Eur. J. Cancer 2018, 95, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Khozin, S.; Blumenthal, G.M.; Zhang, L.; Tang, S.; Brower, M.; Fox, E.; Helms, W.; Leong, R.; Song, P.; Pan, Y.; et al. FDA Approval: Ceritinib for the Treatment of Metastatic Anaplastic Lymphoma Kinase–Positive Non–Small Cell Lung Cancer. Clin. Cancer Res. 2015, 21, 2436–2439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkins, E.; Blumenthal, G.M.; Chen, H.; He, K.; Agarwal, R.; Gieser, G.; Stephens, O.; Zahalka, E.; Ringgold, K.; Helms, W.; et al. FDA Approval: Alectinib for the Treatment of Metastatic, ALK-Positive Non–Small Cell Lung Cancer Following Crizotinib. Clin. Cancer Res. 2016, 22, 5171–5176. [Google Scholar] [CrossRef] [Green Version]
- Taggart, D.; Andreou, T.; Scott, K.J.; Williams, J.; Rippaus, N.; Brownlie, R.J.; Ilett, E.J.; Salmond, R.J.; Melcher, A.; Lorger, M. Anti–PD-1/anti–CTLA-4 efficacy in melanoma brain metastases depends on extracranial disease and augmentation of CD8+ T cell trafficking. Proc. Natl. Acad. Sci. USA 2018, 115, E1540–E1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, M.C. Radioisotope CSF flow studies in leptomeningeal metastases. J. Neuro-Oncol. 1998, 38, 135–140. [Google Scholar] [CrossRef]
- Zhen, J.; Wen, L.; Lai, M.; Zhou, Z.; Shan, C.; Li, S.; Lin, T.; Wu, J.; Wang, W.; Xu, S.; et al. Whole brain radiotherapy (WBRT) for leptomeningeal metastasis from NSCLC in the era of targeted therapy: A retrospective study. Radiat. Oncol. 2020, 15, 1–8. [Google Scholar] [CrossRef]
- Morris, P.G.; Reiner, A.S.; Szenberg, O.R.; Clarke, J.L.; Panageas, K.S.; Perez, H.R.; Kris, M.G.; Chan, T.A.; DeAngelis, L.M.; Omuro, A. Leptomeningeal Metastasis from Non-small Cell Lung Cancer: Survival and the Impact of Whole Brain Radiotherapy. J. Thorac. Oncol. 2012, 7, 382–385. [Google Scholar] [CrossRef] [Green Version]
- Dankner, M.; Issa-Chergui, B.; Bouganim, N. Post-mortem tissue donation programs as platforms to accelerate cancer research. J. Pathol. Clin. Res. 2020, 6, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Reijneveld, J.C.; Taphoorn, M.J.B.; Voest, E.E. A Simple Mouse Model for Leptomeningeal Metastases and Repeated Intrathecal Therapy. J. Neuro-Oncol. 1999, 42, 137–142. [Google Scholar] [CrossRef]
- Schackert, G.; Fidler, I.J. Site-specific metastasis of mouse melanomas and a fibrosarcoma in the brain or meninges of syngeneic animals. Cancer Res. 1988, 48, 3478–3484. [Google Scholar] [PubMed]
- Schackert, G.; Price, J.E.; Zhang, R.D.; Bucana, C.D.; Itoh, K.; Fidler, I.J. Regional growth of different human melanomas as metastases in the brain of nude mice. Am. J. Pathol. 1990, 136, 95–102. [Google Scholar]
- Nanjo, S.; Ebi, H.; Arai, S.; Takeuchi, S.; Yamada, T.; Mochizuki, S.; Okada, Y.; Nakada, M.; Murakami, T.; Yano, S. High efficacy of third generation EGFR inhibitor AZD9291 in a leptomeningeal carcinomatosis model with EGFR-mutant lung cancer cells. Oncotarget 2015, 7, 3847–3856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saboundji, K.; Auliac, J.B.; Pérol, M.; François, G.; Janicot, H.; Marcq, M.; Dubos-Arvis, C.; Renault, A.; Guisier, F.; Odier, L.; et al. Efficacy of Osimertinib in EGFR-Mutated Non-Small Cell Lung Cancer with Leptomeningeal Metastases Pretreated with EGFR-Tyrosine Kinase Inhibitors. Target. Oncol. 2018, 13, 501–507. [Google Scholar] [CrossRef]
- Nanjo, S.; Arai, S.; Wang, W.; Takeuchi, S.; Yamada, T.; Hata, A.; Katakami, N.; Okada, Y.; Yano, S. MET Copy Number Gain Is Associated with Gefitinib Resistance in Leptomeningeal Carcinomatosis of EGFR-mutant Lung Cancer. Mol. Cancer Ther. 2017, 16, 506–515. [Google Scholar] [CrossRef] [Green Version]
- Remsik, J.; Chi, Y.; Tong, X.; Sener, U.; Derderian, C.; Park, A.; Saadeh, F.; Bale, T.; Boire, A. Leptomeningeal metastatic cells adopt two phenotypic states. Cancer Rep. 2020, e1236. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, D.; Bronder, J.L.; Herring, J.M.; Yoneda, T.; Weil, R.J.; Stark, A.M.; Kurek, R.; Vega-Valle, E.; Feigenbaum, L.; Halverson, D.; et al. Her-2 Overexpression Increases the Metastatic Outgrowth of Breast Cancer Cells in the Brain. Cancer Res. 2007, 67, 4190–4198. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dankner, M.; Lam, S.; Degenhard, T.; Garzia, L.; Guiot, M.-C.; Petrecca, K.; Siegel, P.M. The Underlying Biology and Therapeutic Vulnerabilities of Leptomeningeal Metastases in Adult Solid Cancers. Cancers 2021, 13, 732. https://doi.org/10.3390/cancers13040732
Dankner M, Lam S, Degenhard T, Garzia L, Guiot M-C, Petrecca K, Siegel PM. The Underlying Biology and Therapeutic Vulnerabilities of Leptomeningeal Metastases in Adult Solid Cancers. Cancers. 2021; 13(4):732. https://doi.org/10.3390/cancers13040732
Chicago/Turabian StyleDankner, Matthew, Stephanie Lam, Theresa Degenhard, Livia Garzia, Marie-Christine Guiot, Kevin Petrecca, and Peter M. Siegel. 2021. "The Underlying Biology and Therapeutic Vulnerabilities of Leptomeningeal Metastases in Adult Solid Cancers" Cancers 13, no. 4: 732. https://doi.org/10.3390/cancers13040732