
Postoperative Trends and Prognostic Values of Inflammatory and Nutritional Biomarkers after Liver Transplantation for Hepatocellular Carcinoma

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
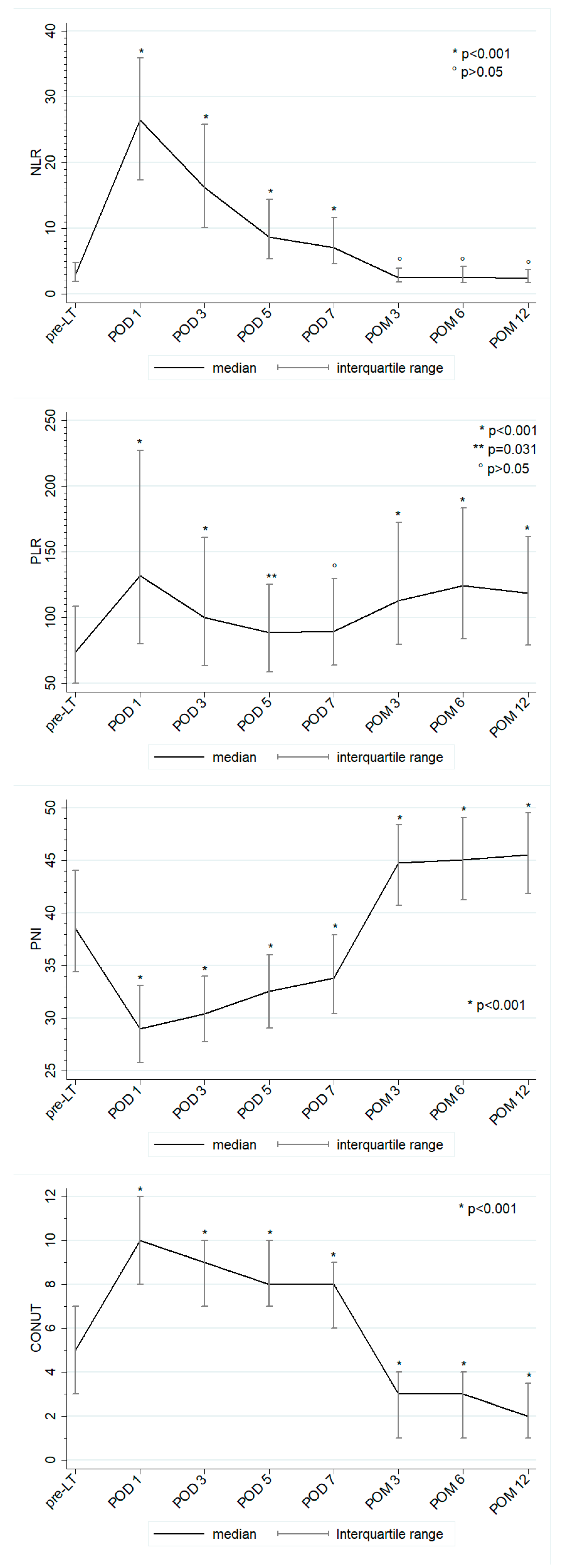
3.1. Post-Transplant Trend of Inflammatory and Nutritional Biomarkers
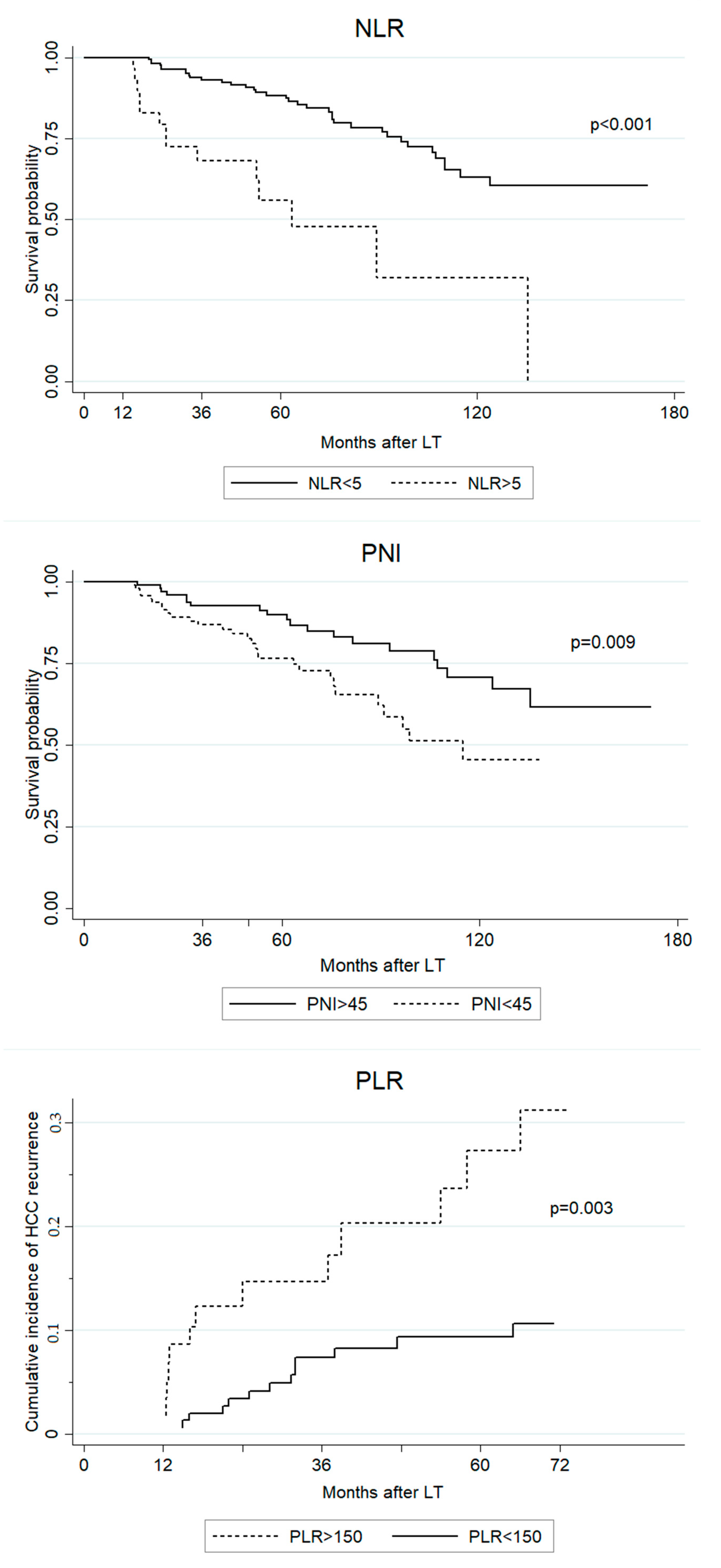
3.2. Overall Survival
3.3. HCC Recurrence
3.4. Late (>1 Year Post-LT) Outcomes
3.5. Predictive Factors of Pre-LT and 1 Year Post-LT Inflammatory and Nutritional Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Citores, M.J.; Lucena, J.L.; De La Fuente, S.; Cuervas-Mons, V. Serum biomarkers and risk of hepatocellular carcinoma recurrence after liver transplantation. World J. Hepatol. 2019, 11, 50–64. [Google Scholar] [CrossRef] [PubMed]
- Lai, Q.; Melandro, F.; Laureiro, Z.L.; Giovanardi, F.; Corradini, S.G.; Ferri, F.; Hassan, R.; Rossi, M.; Mennini, G. Platelet-to-lymphocyte ratio in the setting of liver transplantation for hepatocellu-lar cancer: A systematic review and meta-analysis. World J. Gastroenterol. 2018, 24, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: A Meta-Analysis and Systematic Review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.; Moon, Y.; Jung, K.; Park, Y.; Jun, I.; Kim, S.; Song, J.-G.; Hwang, G. Neutrophil-to-lymphocyte ratio is a predictor of early graft dysfunction following living donor liver transplantation. Liver Int. 2019, 39, 1545–1556. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systemat-ic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Šeruga, B.; Ocana, A.; Tannock, I.F.; Amir, E. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic re-view and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [Green Version]
- Lai, Q.; Santa, E.C.; Juri, J.M.R.; Pinheiro, R.S.N.; Lerut, J. Neutrophil and platelet-to-lymphocyte ratio as new predictors of dropout and recurrence after liver transplantation for hepatocellular cancer. Transpl. Int. 2014, 27, 32–41. [Google Scholar] [CrossRef]
- Sun, X.-D.; Shi, X.-J.; Chen, Y.-G.; Wang, C.-L.; Ma, Q.; Lv, G.-Y. Elevated Preoperative Neutrophil-Lymphocyte Ratio Is Associated with Poor Prognosis in Hepatocellular Carcinoma Patients Treated with Liver Transplantation: A Meta-Analysis. Gastroenterol. Res. Pr. 2016, 2016, 4743808. [Google Scholar] [CrossRef] [Green Version]
- Takagi, K.; Domagala, P.; Polak, W.G.; Buettner, S.; Ijzermans, J.N.M. Prognostic significance of the controlling nutritional status (CONUT) score in patients undergoing hepatectomy for hepatocellular carcinoma: A systematic review and meta-analysis. BMC Gastroenterol. 2019, 19, 211. [Google Scholar] [CrossRef] [Green Version]
- Pravisani, R.; Mocchegiani, F.; Isola, M.; Lorenzin, D.; Adani, G.L.; Cherchi, V.; Righi, E.; Terrosu, G.; Vivarelli, M.; Risaliti, A.; et al. Controlling Nutritional Status score does not predict patients’ overall survival or hepatocellular carcinoma recurrence after deceased donor liver transplantation. Clin. Transplant. 2020, 34, e13786. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Wang, P. The prognostic value of prognostic nutritional index in hepatocellular carcinoma patients: A me-ta-analysis of observational studies. PLoS ONE 2018, 13, e0202987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Man, Z.; Pang, Q.; Zhou, L.; Wang, Y.; Hu, X.; Yang, S.; Jin, H.; Liu, H. Prognostic significance of preoperative prognostic nutritional index in hepatocellular carcino-ma: A meta-analysis. HPB 2018, 20, 888–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McElroy, L.M.; Daud, A.; Davis, A.E.; Lapin, B.; Baker, T.; Abecassis, M.M.; Levitsky, J.; Holl, J.L.; Ladner, D.P. A meta-analysis of complications following deceased donor liver transplant. Am. J. Surg. 2014, 208, 605–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, H.; Takamura, H.; Ohbatake, Y.; Nakanuma, S.; Tajima, H.; Fushida, S.; Onishi, I.; Tani, T.; Shimizu, K.; Ohta, T. Postoperative changes in neutrophil-to-lymphocyte ratio and platelet count: A simple prognostic predictor for adult-to-adult living donor liver transplantation. Asian J. Surg. 2018, 41, 341–348. [Google Scholar] [CrossRef]
- Ismael, M.N.; Forde, J.J.; Milla, E.; Khan, W.; Cabrera, R. Utility of Inflammatory Markers in Predicting Hepatocellular Carcinoma Survival after Liver Transplantation. BioMed Res. Int. 2019, 2019, 7284040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pravisani, R.; Soyama, A.; Isola, M.; Sadykov, N.; Takatsuki, M.; Hidaka, M.; Adachi, T.; Ono, S.; Hara, T.; Hamada, T.; et al. Chronological changes in skeletal muscle mass following living-donor liver transplan-tation: An analysis of the predictive factors for long-term post-transplant low muscularity. Clin. Transplant. 2019, 33, e13495. [Google Scholar] [CrossRef]
- Thoefner, L.B.; Rostved, A.A.; Pommergaard, H.; Rasmussen, A. Risk factors for metabolic syndrome after liver transplantation: A systematic review and meta-analysis. Transplant. Rev. 2018, 32, 69–77. [Google Scholar] [CrossRef]
- Zheng, J.; Wang, W.-L. Risk factors of metabolic syndrome after liver transplantation. Hepatobiliary Pancreat. Dis. Int. 2015, 14, 582–587. [Google Scholar] [CrossRef]
- Anastácio, L.R.; Ferreira, S.C. Nutrition, dietary intake, and eating behavior after liver transplantation. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 381–387. [Google Scholar] [CrossRef]
- Zhang, X.; Li, C.; Wen, T.; Peng, W.; Yan, L.; Yang, J. Postoperative Prognostic Nutritional Index Predicts Survival of Patients with Hepatocellular Carcinoma within Milan Criteria and Hypersplenism. J. Gastrointest. Surg. 2017, 21, 1626–1634. [Google Scholar] [CrossRef]
- Peng, W.; Li, C.; Wen, T.; Yan, L.-N.; Li, B.; Wang, W.-T.; Yang, J.; Xu, M.-Q.; Information, P.E.K.F.C. Postoperative prognostic nutritional index change is an independent predictor of survival in patients with small hepatocellular carcinoma. Am. J. Surg. 2016, 212, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Parisi, I.; Tsochatzis, E.; Wijewantha, H.; Rodríguez-Perálvarez, M.; Luca, L.D.; Manousou, P.; Fatourou, E.; Pieri, G.; Papastergiou, V.; Davies, N.; et al. Inflammation-based scores do not predict post-transplant recurrence of hepato-cellular carcinoma in patients within Milan criteria. Liver Transpl. 2014, 20, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Azab, B.; Camacho-Rivera, M.; Taioli, E. Average values and racial differences of neutrophil lymphocyte ratio among a nation-ally representative sample of United States subjects. PLoS ONE 2014, 9, e112361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, X.; Chang, Q.; Liu, Y.; Chen, L.; Wei, G.; Yang, J.; Zheng, P.; He, F.; Wang, W.; Ming, L. Determinant roles of gender and age on SII, PLR, NLR, LMR and MLR and their reference intervals defining in Henan, China: A posteriori and big-data-based. J. Clin. Lab. Anal. 2018, 32, e22228. [Google Scholar] [CrossRef] [PubMed]
- Forget, P.; Khalifa, C.; Defour, J.P.; Latinne, D.; Van Pel, M.C.; De Kock, M. What is the normal value of the neutro-phil-to-lymphocyte ratio? BMC Res. Notes 2017, 10, 12. [Google Scholar]
- Luo, H.; He, L.; Zhang, G.; Yu, J.; Chen, Y.; Yin, H.; Goyal, H.; Zhang, G.-M.; Xiao, Y.; Gu, C.; et al. Normal Reference Intervals of Neutrophil-To-Lymphocyte Ratio, Platelet-To-Lymphocyte Ratio, Lymphocyte-To-Monocyte Ratio, and Systemic Immune Inflammation Index in Healthy Adults: A Large Multi-Center Study from Western China. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef]
- Angkananard, T.; Anothaisintawee, T.; McEvoy, M.; Attia, J.; Thakkinstian, A. Neutrophil Lymphocyte Ratio and Cardiovascular Disease Risk: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2018, 2018, 2703518. [Google Scholar] [CrossRef] [Green Version]
- Peng, W.; Li, C.; Zhu, W.-J.; Wen, T.; Yan, L.-N.; Li, B.; Wang, W.-T.; Yang, J. Prognostic value of the platelet to lymphocyte ratio change in liver cancer. J. Surg. Res. 2015, 194, 464–470. [Google Scholar] [CrossRef]
- Lai, Q.; Vitale, A.; Manzia, T.M.; Foschi, F.G.; Levi Sandri, G.B.; Gambato, M.; Melandro, F.; Russo, F.P.; Miele, L.; Viganò, L.; et al. AssociazioneItaliana per lo Studio del Fegato (AISF) HCC Special Interest Group. Platelets and Hepatocellular Cancer: Bridging the Bench to the Clinics. Cancers 2019, 11, 1568. [Google Scholar]
- Choi, J.; Bano, A.; Azzi, J. Biomarkers in Solid Organ Transplantation. Clin. Lab. Med. 2019, 39, 73–85. [Google Scholar] [CrossRef]
- Naesens, M.; Anglicheau, D. Precision Transplant Medicine: Biomarkers to the Rescue. J. Am. Soc. Nephrol. 2017, 29, 24–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Gender (M:F) | 291:33 |
| Age (years) | 58 (52–62) |
| BMI | 25.3 (23.2–28.1) |
| Pre-LT diabetes (%) | 54 (16.9%) |
| HIV positivity (%) | 29 (9.0%) |
| HCV positivity (%) | 180 (55.6%) |
| HBV positivity (%) | 70 (21.6%) |
| Alcohol abuse (%) | 96 (29.6%) |
| MELD score | 12 (9–16) |
| Child–Pugh score (%) | |
| - A | 139 (42.9%) |
| - B | 122 (37.6%) |
| - C | 62 (19.5%) |
| Pre-LT PLR | 74.2 (50.3–108.5) |
| 1 year post-LT PLR | 118.2 (79.1–161.5) |
| Pre-LT NLR | 2.9 (1.9–4.8) |
| 1 year post-LT NLR | 2.4 (1.7–3.7) |
| Pre-LT PNI | 38.6 (34.5–44.1) |
| 1 year post-LT PNI | 45.6 (41.9–49.5) |
| Pre-LT CONUT | 5 (3–7) |
| 1 year post-LT CONUT | 2 (1–3) |
| Pre-LT AFP, (ng/L) | 9.8 (4.6–40.2) |
| Donor age (years) | 61.4 (50.1–72.9) |
| Donor BMI | 25.8 (23.7–27.8) |
| Total ischemia time (min) | 470 (401–550) |
| Packed blood cells transfusion, (UI) | 3 (0–7) |
| Frozen fresh plasma transfusion, (mL) | 1000 (0–2000) |
| Tumor number | 2 (1–3) |
| Tumor max diameter (cm) | 2.3 (1.5–3) |
| Bilobar tumor distribution (%) | 82 (25.3%) |
| Edmonson–Steiner grading (%) | |
| - Complete necrosis | 12 (3.7%) |
| - G1 | 54 (16.6%) |
| - G2 | 172 (53.1%) |
| - G3 | 80 (24.7%) |
| - G4 | 6 (1.9%) |
| Microvascular invasion (%) | 50 (15.4%) |
| Mortality | HCC Recurrence | |||||
|---|---|---|---|---|---|---|
| Factors | HR | 95% Conf. Interval | p-Val | SHR | 95% Conf. Interval | p-Val |
| PLR | ||||||
| pre-LT | 1.004 | 1.002–1.006 | <0.001 | 1.005 | 1.002–1.007 | 0.001 |
| POD 1 | 1.001 | 0.999–1.002 | 0.399 | 1.001 | 0.999–1.003 | 0.196 |
| POD 3 | 1.001 | 0.998–1.003 | 0.354 | 1.001 | 0.998–1.004 | 0.384 |
| POD 5 | 1.001 | 0.998–1.004 | 0.295 | 0.999 | 0.996–1.003 | 0.982 |
| POD 7 | 1.003 | 1.001–1.005 | 0.012 | 0.999 | 0.996–1.002 | 0.769 |
| POM 3 | 1.003 | 1.001–1.005 | 0.003 | 1.001 | 0.998–1.003 | 0.333 |
| POM 6 | 1.005 | 1.004–1.008 | <0.001 | 1.003 | 1.001–1.006 | 0.018 |
| 1 year post-LT | 1.005 | 1.003–1.007 | <0.001 | 1.003 | 1.001–1.006 | 0.010 |
| NLR | ||||||
| pre-LT | 1.058 | 1.030–1.087 | <0.001 | 1.041 | 1.003–1.081 | 0.036 |
| POD 1 | 1.007 | 0.998–1.016 | 0.116 | 1.001 | 0.988–1.013 | 0.886 |
| POD 3 | 1.013 | 1.001–1.025 | 0.032 | 0.989 | 0.964–1.016 | 0.456 |
| POD 5 | 1.029 | 1.013–1.044 | <0.001 | 0.977 | 0.944–1.011 | 0.187 |
| POD 7 | 1.054 | 1.039–1.069 | <0.001 | 0.953 | 0.913–1.001 | 0.126 |
| POM 3 | 1.005 | 1.001–1.011 | 0.024 | 1.008 | 1.002–1.016 | 0.017 |
| POM 6 | 1.210 | 1.158–1.266 | <0.001 | 1.071 | 1.013–1.133 | 0.016 |
| 1 year post-LT | 1.058 | 1.030–1.087 | <0.001 | 1.157 | 1.007–1.331 | 0.040 |
| PNI | ||||||
| pre-LT | 0.988 | 0.962–1.014 | 0.382 | 1.018 | 0.982–1.057 | 0.315 |
| POD 1 | 0.952 | 0.915–1.000 | 0.145 | 1.029 | 0.975–1.086 | 0.288 |
| POD 3 | 0.984 | 0.942–1.027 | 0.473 | 0.999 | 0.943–1.058 | 0.977 |
| POD 5 | 0.980 | 0.941–1.020 | 0.326 | 1.006 | 0.944–1.072 | 0.840 |
| POD 7 | 0.956 | 0.916–0.998 | 0.044 | 1.009 | 0.948–1.073 | 0.776 |
| POM 3 | 0.943 | 0.911–0.976 | 0.001 | 1.005 | 0.954–1.059 | 0.834 |
| POM 6 | 0.911 | 0.874–0.949 | <0.001 | 1.008 | 0.963–1.054 | 0.722 |
| 1 year post-LT | 0.862 | 0.818–0.908 | <0.001 | 0.911 | 0.844–0.984 | 0.019 |
| CONUT | ||||||
| pre-LT | 0.956 | 0.876–1.044 | 0.326 | 0.936 | 0.837–1.047 | 0.251 |
| POD 1 | 1.071 | 0.944–1.216 | 0.282 | 0.850 | 0.719–1.005 | 0.158 |
| POD 3 | 1.003 | 0.910–1.106 | 0.944 | 0.970 | 0.850–1.108 | 0.662 |
| POD 5 | 1.006 | 0.902–1.122 | 0.904 | 1.001 | 0.833–1.204 | 0.987 |
| POD 7 | 1.158 | 1.017–1.319 | 0.026 | 0.959 | 0.812–1.133 | 0.628 |
| POM 3 | 1.211 | 1.075–1.365 | 0.002 | 1.002 | 0.832–1.207 | 0.980 |
| POM 6 | 1.335 | 1.195–1.493 | <0.001 | 0.951 | 0.797–1.135 | 0.582 |
| 1 year post-LT | 1.304 | 1.099–1.546 | 0.002 | 1.107 | 0.812–1.508 | 0.518 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Factors | HR | 95% Conf. Interval | p-Val | HR | 95% Conf. Interval | p-Val |
| Sex | ||||||
| - male | 1 | |||||
| - female | 0.850 | 0.340–2.123 | 0.728 | |||
| Age | 1.016 | 0.981–1.052 | 0.367 | |||
| Pre-LT BMI | 0.955 | 0.885–1.031 | 0.244 | |||
| Pre-transplant diabetes | 0.870 | 0.395–1.917 | 0.730 | |||
| HIV positivity | 1.115 | 0.481–2.590 | 0.798 | |||
| HCV positivity | 0.892 | 0.548–1.451 | 0.646 | |||
| HBV positivity | 0.870 | 0.4945–1.533 | 0.631 | |||
| Alcohol abuse | 1.523 | 0.915–2.533 | 0.105 | |||
| MELD score | 0.971 | 0.926–1.018 | 0.236 | |||
| Child–Pugh score | 0.839 | 0.585–1.205 | 0.343 | |||
| Donor age | 1.003 | 0.988–1.018 | 0.654 | |||
| Donor BMI | 0.987 | 0.925–1.054 | 0.706 | |||
| Total ischemia time | 1.001 | 0.999–1.003 | 0.303 | |||
| Packed blood cells transfusion | 1.044 | 1.004–1.085 | 0.029 | 1.058 | 1.004–1.117 | 0.040 |
| Frozen fresh plasma transfusion | 1.001 | 1.000–1.002 | 0.046 | |||
| Pre-LT AFP | 1.000 | 0.999–1.000 | 0.277 | |||
| HCC recurrence | 3.916 | 2.339–6.556 | <0.001 | 5.428 | 2.859–10.307 | <0.001 |
| 1 year post-LT PLR | 1.005 | 1.002–1.007 | <0.001 | |||
| 1 year post-LT NLR | 1.332 | 1.194–1.486 | <0.001 | 1.218 | 1.053–1.408 | 0.008 |
| 1 year post-LT PNI | 0.863 | 0.814–0.915 | <0.001 | 0.913 | 0.851–0.978 | 0.011 |
| 1 year post-LT CONUT | 1.286 | 1.067–1.550 | 0.008 | |||
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Factors | SHR | 95% Conf. Interval | p-Val | SHR | 95% Conf. Interval | p-Val |
| Sex | ||||||
| - male | 1 | |||||
| - female | 2.093 | 0.844–5.190 | 0.211 | |||
| Age | 1.009 | 0.969–1.059 | 0.702 | |||
| Pre-LT BMI | 0.952 | 0.864–1.051 | 0.334 | |||
| Pre-transplant diabetes | 0.336 | 0.081–1.403 | 0.135 | |||
| HIV positivity | 1.042 | 0.327–3.316 | 0.944 | |||
| HCV positivity | 0.565 | 0.286–1.119 | 0.202 | |||
| HBV positivity | 1.917 | 0.959–3.830 | 0.165 | |||
| Alcohol abuse | 1.042 | 0.502–2.163 | 0.911 | |||
| MELD score | 0.939 | 0.857–1.028 | 0.177 | |||
| Child–Pugh score | 0.587 | 0.346–1.995 | 0.148 | |||
| Donor age | 0.994 | 0.974–1.015 | 0.622 | |||
| Donor BMI | 0.931 | 0.847–1.024 | 0.143 | |||
| Total ischemia time | 1.001 | 0.998–1.003 | 0.530 | |||
| Packed blood cells transfusion | 0.994 | 0.925–1.070 | 0.891 | |||
| Frozen fresh plasma transfusion | 0.999 | 0.999–1.000 | 0.363 | |||
| Pre-LT AFP | 1.000 | 0.999–1.001 | 0.341 | |||
| 1 year post-LT PLR | 1.004 | 1.001–1.006 | 0.009 | 1.005 | 1.001–1.006 | 0.008 |
| 1 year post-LT NLR | 1.166 | 1.009–1.349 | 0.038 | |||
| 1 year post-LT PNI | 0.900 | 0.830–0.975 | 0.011 | |||
| 1 year post-LT CONUT | 1.165 | 0.838–1.619 | 0.364 | |||
| Tumor number | 1.407 | 1.203–1.646 | <0.001 | 1.504 | 1.26–1.795 | <0.001 |
| Tumor max diameter | 1.284 | 1.116–1.478 | 0.001 | 1.344 | 1.145–1.578 | <0.001 |
| Edmonson–Steiner grading | 2.250 | 1.372–3.687 | 0.001 | 2.030 | 1.045–3.945 | 0.037 |
| Microvascular invasion | 4.859 | 2.338–10.100 | <0.001 | 3.511 | 1.605–7.681 | 0.032 |
| Factors | Regression Coefficient | 95% Conf. Interval | p-Val | Regression Coefficient | 95% Conf. Interval | p-Val | |
|---|---|---|---|---|---|---|---|
| PLR | |||||||
| pre-LT | 1 year post-LT | ||||||
| MELD score | 0.255 | −0.959 to 1.471 | 0.679 | 0.656 | −1.144 to 2.457 | 0.473 | |
| Child–Pugh score | 7.635 | −3.347 to 18.619 | 0.172 | −4.916 | −20.333 to 10.501 | 0.530 | |
| Pre-LT AFP | 0.001 | −0.0136 to 0.016 | 0.845 | 0.032 | 0.013–0.050 | 0.001 | |
| Tumor number | 5.408 | 0.018 to 10.797 | 0.049 | 0.256 | −7.296 to 7.810 | 0.947 | |
| Tumor max diameter | 0.645 | −5.470 to 6.760 | 0.836 | 1.799 | −5.061 to 8.660 | 0.606 | |
| Edmonson–Steiner grading | 10.108 | 1.162 to 21.378 | 0.050 | 9.166 | −6.697 to 25.031 | 0.256 | |
| Microvascular invasion | 13.810 | −9.167 to 36.789 | 0.238 | 36.989 | 3.763 to 70.215 | 0.029 | |
| NLR | |||||||
| pre-LT | 1 year post-LT | ||||||
| MELD score | 0.196 | 0.115 to 0.277 | <0.001 | −0.005 | −0.053 to 0.041 | 0.816 | |
| Child–Pugh score | 2.095 | 1.368 to 2.822 | <0.001 | 0.071 | −0.344 to 0.486 | 0.736 | |
| Pre-LT AFP | −0.000 | −0.000 to.008 | 0.928 | 0.081 | 0.035 to 0.132 | 0.002 | |
| Tumor number | 0.172 | −0.205 to 0.549 | 0.370 | 0.054 | −0.146 to 0.255 | 0.595 | |
| Tumor max diameter | −0.367 | −0.790 to 0.055 | 0.089 | 0.185 | 0.007 to 0.364 | 0.042 | |
| Edmonson–Steiner grading | 0.836 | 0.051 to 1.621 | 0.037 | 0.286 | −0.128 to 0.701 | 0.175 | |
| Microvascular invasion | 0.887 | −0.728 to 2.503 | 0.281 | 1.125 | 0.252 to 1.999 | 0.012 | |
| PNI | |||||||
| 1 year post-LT | |||||||
| MELD score | −0.022 | −0.153 to 0.107 | 0.729 | ||||
| Child–Pugh score | −0.405 | −1.539 to 0.729 | 0.482 | ||||
| Pre-LT AFP | −0.000 | −0.002 to 0.000 | 0.226 | ||||
| Tumor number | −0.218 | −0.763 to 0.326 | 0.431 | ||||
| Tumor max diameter | −0.022 | −0.519 to 0.473 | 0.927 | ||||
| Edmonson–Steiner grading | −1.345 | −2.463 to −0.228 | 0.019 | ||||
| Microvascular invasion | −3.785 | −6.142 to −1.427 | 0.002 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pravisani, R.; Mocchegiani, F.; Isola, M.; Lorenzin, D.; Adani, G.L.; Cherchi, V.; De Martino, M.; Risaliti, A.; Lai, Q.; Vivarelli, M.; et al. Postoperative Trends and Prognostic Values of Inflammatory and Nutritional Biomarkers after Liver Transplantation for Hepatocellular Carcinoma. Cancers 2021, 13, 513. https://doi.org/10.3390/cancers13030513
Pravisani R, Mocchegiani F, Isola M, Lorenzin D, Adani GL, Cherchi V, De Martino M, Risaliti A, Lai Q, Vivarelli M, et al. Postoperative Trends and Prognostic Values of Inflammatory and Nutritional Biomarkers after Liver Transplantation for Hepatocellular Carcinoma. Cancers. 2021; 13(3):513. https://doi.org/10.3390/cancers13030513
Chicago/Turabian StylePravisani, Riccardo, Federico Mocchegiani, Miriam Isola, Dario Lorenzin, Gian Luigi Adani, Vittorio Cherchi, Maria De Martino, Andrea Risaliti, Quirino Lai, Marco Vivarelli, and et al. 2021. "Postoperative Trends and Prognostic Values of Inflammatory and Nutritional Biomarkers after Liver Transplantation for Hepatocellular Carcinoma" Cancers 13, no. 3: 513. https://doi.org/10.3390/cancers13030513