
Preoperative CTC-Detection by CellSearch® Is Associated with Early Distant Metastasis and Impaired Survival in Resected Pancreatic Cancer

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Group Characteristics
2.2. Distribution of CTCs and Site of First Recurrence
2.2.1. Recurrence and Survival Analysis
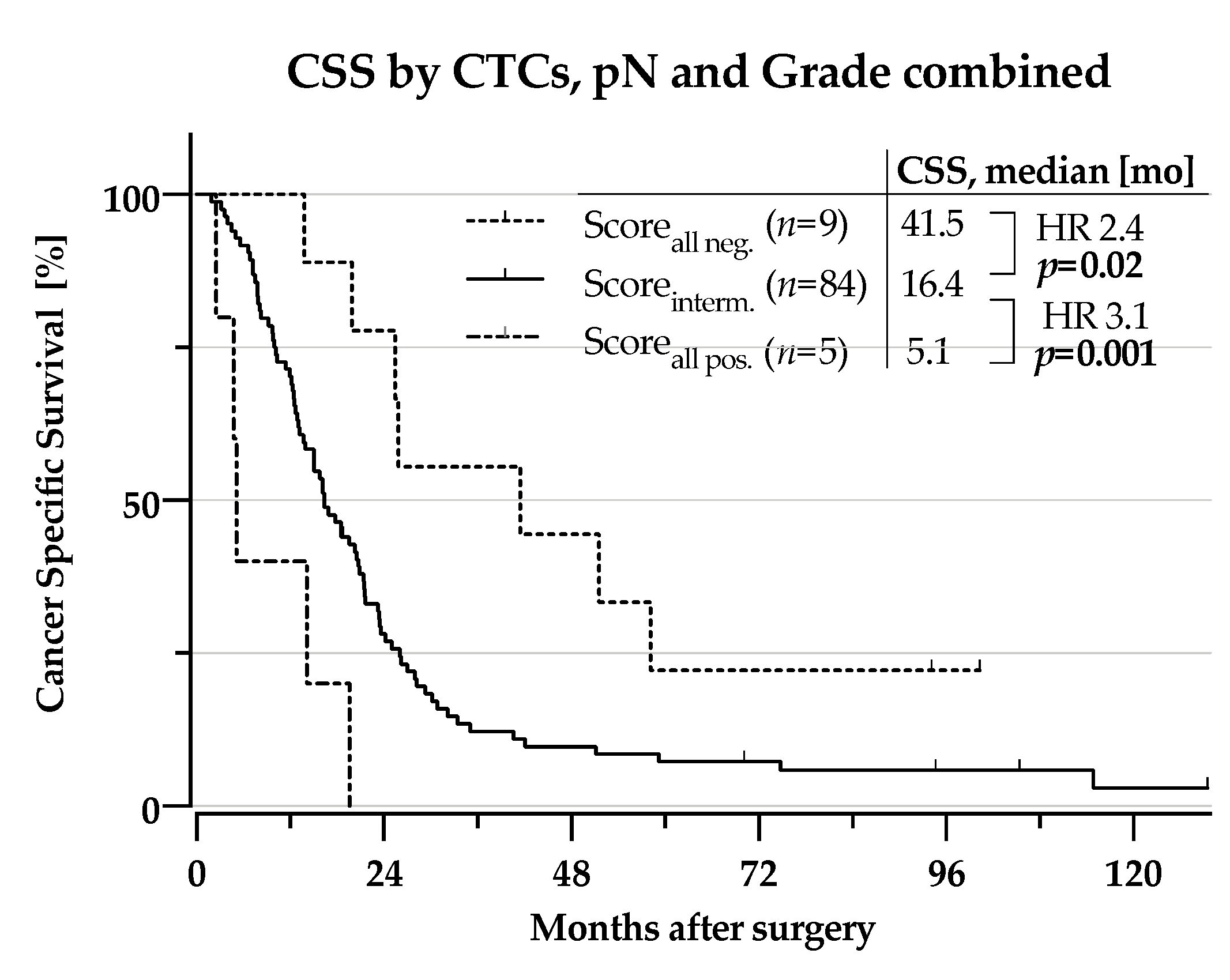
2.2.2. CSS According to Subgroups by Combining Risk-factors for Distant Metastasis
3. Discussion
4. Materials and Methods
4.1. Patients, Study Design and Follow-up
4.2. Characteristics of the Patient Cohort
4.3. CTC Detection
4.4. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Entire Cohort (n = 98) | Remission (n = 6) | ILR (n = 29) | DM (n = 58) | No Imaging (n = 4) | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age, median [years] | 68 (34–80) | 65 (57–75) | 68 (51–78) | 68 (34–79) | 74 (68–80) |
| Sex, male | 50 (51.0%) | 2 (33.3%) | 14 (48.3%) | 33 (59.0%) | 0 (0%) |
| Preoperative Risk Factors | |||||
| CTCs ≥ 1 | 7 (7.1%) | none | none | 7 (12.5%) | none |
| CA19-9 ≥ 200 kU/l | 31/74 (41.9%) 24 missing | 2/4 (50%) 2 missing | 10/25 (40%) 2 missing | 18/42 (42.9%) 14 missing | ½ (50%) 2 missing |
| Tumour size on imaging> 25 mm | 39/97 (40.2%) 1 missing | 2 (33.3%) | 15 (51.7%) | 21/57 (36.8%) 1 missing | 1 (25%) |
| Bilirubin > 50 µmol/L | 75/94 (79.8%) 4 missing | 5 (83.3%) | 20/27 (74.1%) 2 missing | 47/56 (82.4%) 1 missing | 2 (50%) |
| Treatment | |||||
| Neoadjuvant therapy: | |||||
| GEM | 3(3.0%) | None | 2(6.9%) | 1(1.7%) | None |
| FOLFIRINOX | 1 (1.0%) | none | none | 1(1.7%) | none |
| Operation: | |||||
| PPPD | 77 (78.6%) | 5 (83.3%) | 23 (79.3%) | 46 (79.3%) | 2 (50%) |
| PD | 13 (13.2%) | 1 (16.7%) | 4 (13.8%) | 7 (12.1%) | 1 (25%) |
| Tot. pancreatectomy | 8 (8.2%) | none | 2 (6.9%) | 5 (8.6%) | 1 (25%) |
| Venous resection | 36 (36.7%) | 3 (50%) | 16 (55.2%) | 15 (25.9%) | 1 (25%) |
| Adjuvant therapy: | |||||
| FLV | 53 (54.1%) | 5 (83.3%) | 14 (48.3%) | 31 (53.4%) | 2 (50%) |
| GEM | 6 (6.1%) | None | 3 (10.3%) | 3 (5.2%) | None |
| FLOX | 3 (3.1%) | None | 1 (3.4%) | 1 (1.7%) | None |
| none | 36 (36.7%) | 1 (16.7%) | 11 (37.9%) | 22 (37.9%) | 2 (50%) |
| Histopathologic results | |||||
| Pancreatobiliary type | 97 (99%) | 6 | 28 (96.6%) | 58 (100%) | 4 (100%) |
| Intestinal type | 1 (1%) | -100% | 1 (3.4%) | ||
| UICC-stage (V7): | |||||
| Ib | 2 (2.0%) | None | None | 1 (1.7%) | 0 (0%) |
| IIa | 23 (23.5%) | 4 (66.7%) | 9 (31.0%) | 8 (13.8%) | 2 (50%) |
| IIb | 73 (74.5%) | 2 (33.3%) | 20 (69.0%) | 49 (84.5%) | 2 (50%) |
| pN1-status | 73 (74,5%) | 2 (33.3%) | 20 (69.0%) | 49 (84.5%) | 2 (50%) |
| R1-status | 61 (62.2%) | 3 (50%) | 20 (69.0%) | 35 (60.3%) | 3 (75%) |
| Vascular infiltration | 64 (65.3%) | 2 (33.3%) | 17 (55.1%) | 42 (72.4%) | 3 (75%) |
| Perineural infiltration | 91 (92.9%) | 4 (66.7%) | 28 (96.6%) | 54 (93.1%) | 4 (100%) |
| Age | Sex | UICC-Stage | pT | pN | M | G | R | VI | PNI | CTCs/ 7.5 mL | CSS [mo] | DFS [mo] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 79 | m | St. IIb | 3 | 1 | 0 | 4 | 0 | 1 | 1 | 33 | 2.5 | 0.5 |
| 65 | m | St. IIb | 3 | 1 | 0 | 3 | 0 | 1 | 1 | 1 | 14.1 | 9.7 |
| 71 | m | St. IIb | 3 | 1 | 0 | 2 | 1 | 0 | 1 | 1 | 7.8 | 2.5 |
| 70 | m | St. IIb | 3 | 1 | 0 | 2 | 1 | 1 | 1 | 1 | 19.6 | 14.3 |
| 69 | m | St. IIb | 3 | 1 | 0 | 2 | 1 | 0 | 1 | 1 | 6.6 | 2.0 |
| 76 | f | St. IIb | 3 | 1 | 0 | 2 | 1 | 1 | 1 | 1 | 4.7 | 3.9 |
| 57 | m | St. IIb | 3 | 1 | 0 | 2 | 0 | 1 | 1 | 1 | 5.1 | 3.3 |
References
- Hariharan, D.; Saied, A.; Kocher, H.M. Analysis of mortality rates for pancreatic cancer across the world. HPB (Oxford) 2008, 10, 58–62. [Google Scholar] [CrossRef] [Green Version]
- Søreide, K.; Aagnes, B.; Møller, B.; Westgaard, A.; Bray, F. Epidemiology of pancreatic cancer in Norway: Trends in incidence, basis of diagnosis and survival 1965–2007. Scand. J. Gastroenterol. 2010, 45, 82–92. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Larsen, I.K.; Møller, B.; Robsahm, T.E.; Johannsessen, T.B.; Grimsrud, T.K.; Larønningen, S.; Jakobsen, E.; Ursin, G. Cancer in Norway 2018; Larsen, I.K., Ed.; Cancer Registry of Norway: Oslo, Norway, 2019. [Google Scholar]
- Van den Broeck, A.; Sergeant, G.; Ectors, N.; Van Steenbergen, W.; Aerts, R.; Topal, B. Patterns of recurrence after curative resection of pancreatic ductal adenocarcinoma. Eur. J. Surg. Oncol. 2009, 35, 600–604. [Google Scholar] [CrossRef]
- Sperti, C.; Pasquali, C.; Piccoli, A.; Pedrazzoli, S. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J. Surg. 1997, 21, 195–200. [Google Scholar] [CrossRef]
- Suto, H.; Okano, K.; Oshima, M.; Ando, Y.; Takahashi, S.; Shibata, T.; Kamada, H.; Kobara, H.; Masaki, T.; Suzuki, Y. The predictors and patterns of the early recurrence of pancreatic ductal adenocarcinoma after pancreatectomy: The influence of pre- and post- operative adjuvant therapy. BMC Surg. 2019, 19, 186–187. [Google Scholar] [CrossRef] [Green Version]
- Groot, V.P.; van Santvoort, H.C.; Rombouts, S.J.E.; Hagendoorn, J.; Borel Rinkes, I.H.M.; van Vulpen, M.; Herman, J.M.; Wolfgang, C.L.; Besselink, M.G.; Molenaar, I.Q. Systematic review on the treatment of isolated local recurrence of pancreatic cancer after surgery; re-resection, chemoradiotherapy and SBRT. HPB (Oxford) 2017, 19, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Oba, A.; Croce, C.; Hosokawa, P.; Meguid, C.; Torphy, R.J.; Al-Musawi, M.H.; Ahrendt, S.; Gleisner, A.; Schulick, R.D.; Del Chiaro, M. Prognosis Based Definition of Resectability in Pancreatic Cancer: A Road Map to New Guidelines. Ann. Surg. 2020. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Groot, V.P.; Rezaee, N.; Wu, W.; Cameron, J.L.; Fishman, E.K.; Hruban, R.H.; Weiss, M.J.; Zheng, L.; Wolfgang, C.L.; He, J. Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2018, 267, 936–945. [Google Scholar] [CrossRef]
- Honselmann, K.C.; Pergolini, I.; Castillo, C.F.-D.; Deshpande, V.; Ting, D.; Taylor, M.S.; Bolm, L.; Qadan, M.; Wellner, U.; Sandini, M.; et al. Timing but Not Patterns of Recurrence Is Different Between Node-negative and Node-positive Resected Pancreatic Cancer. Ann. Surg. 2019. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Riethdorf, S.; O’Flaherty, L.; Hille, C.; Pantel, K. Clinical applications of the CellSearch platform in cancer patients. Adv. Drug Deliv. Rev. 2018, 125, 102–121. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Mathiot, C.; Delaloge, S.; Brain, E.; Giachetti, S.; de Cremoux, P.; Marty, M.; Pierga, J.Y. Single circulating tumor cell detection and overall survival in nonmetastatic breast cancer. Ann. Oncol. 2010, 21, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Effenberger, K.E.; Schroeder, C.; Hanssen, A.; Wolter, S.; Eulenburg, C.; Tachezy, M.; Gebauer, F.; Izbicki, J.R.; Pantel, K.; Bockhorn, M. Improved Risk Stratification by Circulating Tumor Cell Counts in Pancreatic Cancer. Clin. Cancer Res. 2018, 24, 2844–2850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poruk, K.E.; Valero, V.; Saunders, T.; Blackford, A.L.; Griffin, J.F.; Poling, J.; Hruban, R.H.; Anders, R.A.; Herman, J.; Zheng, L.; et al. Circulating Tumor Cell Phenotype Predicts Recurrence and Survival in Pancreatic Adenocarcinoma. Ann. Surg. 2016, 264, 1073–1081. [Google Scholar] [CrossRef] [Green Version]
- Sergeant, G.; van Eijsden, R.; Roskams, T.; Van Duppen, V.; Topal, B. Pancreatic cancer circulating tumour cells express a cell motility gene signature that predicts survival after surgery. BMC Cancer 2012, 12, 527. [Google Scholar] [CrossRef] [Green Version]
- Hugenschmidt, H.; Labori, K.J.; Brunborg, C.; Verbeke, C.S.; Seeberg, L.T.; Schirmer, C.B.; Renolen, A.; Borgen, E.F.; Naume, B.; Wiedswang, G. Circulating Tumor Cells are an Independent Predictor of Shorter Survival in Patients Undergoing Resection for Pancreatic and Periampullary Adenocarcinoma. Ann. Surg. 2020, 271, 549–558. [Google Scholar] [CrossRef]
- Bissolati, M.; Sandri, M.T.; Burtulo, G.; Zorzino, L.; Balzano, G.; Braga, M. Portal vein-circulating tumor cells predict liver metastases in patients with resectable pancreatic cancer. Tumour. Biol. 2015, 36, 991–996. [Google Scholar] [CrossRef]
- Tien, Y.W.; Kuo, H.-C.; Ho, B.-I.; Chang, M.-C.; Chang, Y.-T.; Cheng, M.-F.; Chen, H.-L.; Liang, T.-Y.; Wang, C.-F.; Huang, C.-Y.; et al. A High Circulating Tumor Cell Count in Portal Vein Predicts Liver Metastasis from Periampullary or Pancreatic Cancer: A High Portal Venous CTC Count Predicts Liver Metastases. Medicine (Baltimore) 2016, 95, e3407. [Google Scholar] [CrossRef]
- Tao, L.; Su, L.; Yuan, C.; Ma, Z.; Zhang, L.; Bo, S.; Niu, Y.; Lu, S.; Xiu, D. Postoperative metastasis prediction based on portal vein circulating tumor cells detected by flow cytometry in periampullary or pancreatic cancer. Cancer Manag. Res. 2019, 11, 7405–7425. [Google Scholar] [CrossRef] [Green Version]
- Earl, J.; Garcia-Nieto, S.; Martinez-Avila, J.C.; Montans, J.; Sanjuanbenito, A.; Rodríguez-Garrote, M.; Lisa, E.; Mendía, E.; Lobo, E.; Malats, N.; et al. Circulating tumor cells (Ctc) and kras mutant circulating free Dna (cfdna) detection in peripheral blood as biomarkers in patients diagnosed with exocrine pancreatic cancer. BMC Cancer 2015, 15, 797. [Google Scholar] [CrossRef] [Green Version]
- Kurihara, T.; Itoi, T.; Sofuni, A.; Itokawa, F.; Tsuchiya, T.; Tsuji, S.; Ishii, K.; Ikeuchi, N.; Tsuchida, A.; Kasuya, K.; et al. Detection of circulating tumor cells in patients with pancreatic cancer: A preliminary result. J. Hepatobiliary Pancreat Surg. 2008, 15, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Khoja, L.; Backen, A.; Sloane, R.; Menasce, L.; Ryder, D.; Krebs, M.; Board, R.; Clack, G.; Hughes, A.; Blackhall, F.; et al. A pilot study to explore circulating tumour cells in pancreatic cancer as a novel biomarker. Br. J. Cancer 2012, 106, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Okubo, K.; Uenosono, Y.; Arigami, T.; Mataki, Y.; Matsushita, D.; Yanagita, S.; Kurahara, H.; Sakoda, M.; Kijima, Y.; Maemura, K.; et al. Clinical impact of circulating tumor cells and therapy response in pancreatic cancer. Eur. J. Surg. Oncol. 2017, 43, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.-C.; Michiels, S.; Riethdorf, S.; Mueller, V.; Esserman, L.J.; Lucci, A.; Naume, B.; Horiguchi, J.; Gisbert-Criado, R.; Sleijfer, S.; et al. Circulating Tumor Cells in Breast Cancer Patients Treated by Neoadjuvant Chemotherapy: A Meta-analysis. J. Natl. Cancer Inst. 2018, 110, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Terstappen, L.W.; Rao, C.; Gross, S.; Weiss, A.J. Peripheral blood tumor cell load reflects the clinical activity of the disease in patients with carcinoma of the breast. Int. J. Oncol. 2000, 17, 573–578. [Google Scholar] [CrossRef]
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.J.; Uhr, J.W.; Terstappen, L.W.M.M. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef] [Green Version]
- Rack, B.; Schindlbeck, C.; Jückstock, J.; Andergassen, U.; Hepp, P.; Zwingers, T.; Friedl, T.W.P.; Lorenz, R.; Tesch, H.; Fasching, P.A.; et al. Circulating Tumor Cells Predict Survival in Early Average-to-High Risk Breast Cancer Patients. J. Natl. Cancer Inst. 2014, 106, 793. [Google Scholar] [CrossRef]
- Janni, W.J.; Rack, B.; Terstappen, L.W.M.M.; Pierga, J.-Y.; Taran, F.-A.; Fehm, T.; Hall, C.; De Groot, M.R.; Bidard, F.-C.; Friedl, T.W.P.; et al. Pooled Analysis of the Prognostic Relevance of Circulating Tumor Cells in Primary Breast Cancer. Clin. Cancer Res. 2016, 22, 2583–2593. [Google Scholar] [CrossRef] [Green Version]
- van Dalum, G.; Stam, G.-J.; Scholten, L.F.A.; Mastboom, W.J.B.; Vermes, I.; Tibbe, A.G.J.; De Groot, M.R.; Terstappen, L.W.M.M. Importance of circulating tumor cells in newly diagnosed colorectal cancer. Int. J. Oncol. 2015, 46, 1361–1368. [Google Scholar] [CrossRef] [Green Version]
- Cabel, L.; Proudhon, C.; Gortais, H.; Loirat, D.; Coussy, F.; Pierga, J.-Y.; Bidard, F.-C. Circulating tumor cells: Clinical validity and utility. Int. J. Clin. Oncol. 2017, 22, 421–430. [Google Scholar] [CrossRef]
- Stoecklein, N.H.; Fischer, J.C.; Niederacher, D.; Terstappen, L.W.M.M. Challenges for CTC-based liquid biopsies: Low CTC frequency and diagnostic leukapheresis as a potential solution. Expert Rev. Mol. Diagn. 2016, 16, 147–164. [Google Scholar] [CrossRef] [PubMed]
- Brychta, N.; Drosch, M.; Driemel, C.; Fischer, J.C.; Neves, R.P.; Esposito, I.; Knoefel, W.; Möhlendick, B.; Hille, C.; Stresemann, A.; et al. Isolation of circulating tumor cells from pancreatic cancer by automated filtration. Oncotarget 2017, 8, 86143–86156. [Google Scholar] [CrossRef] [PubMed]
- Poruk, K.E.; Blackford, A.L.; Weiss, M.J.; Cameron, J.L.; He, J.; Goggins, M.; Rasheed, Z.A.; Wolfgang, C.L.; Wood, L.D. Circulating Tumor Cells Expressing Markers of Tumor-Initiating Cells Predict Poor Survival and Cancer Recurrence in Patients with Pancreatic Ductal Adenocarcinoma. Clin. Cancer Res. 2017, 23, 2681–2690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gemenetzis, G.; Groot, V.P.; Yu, J.; Ding, D.; Teinor, J.A.; Javed, A.A.; Wood, L.D.; Burkhart, R.A.; Cameron, J.L.; Makary, M.A.; et al. Circulating Tumor Cells Dynamics in Pancreatic Adenocarcinoma Correlate with Disease Status: Results of the Prospective CLUSTER Study. Ann. Surg. 2018, 268, 408–420. [Google Scholar] [CrossRef] [PubMed]
- de Albuquerque, A.; Kubisch, I.; Breier, G.; Stamminger, G.; Fersis, N.; Eichler, A.; Kaul, S.; Stölzel, U. Multimarker gene analysis of circulating tumor cells in pancreatic cancer patients: A feasibility study. Oncology 2012, 82, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephenson, D.; Nahm, C.; Chua, T.; Gill, A.; Mittal, A.; de Reuver, P.; Samra, J. Circulating and disseminated tumor cells in pancreatic cancer and their role in patient prognosis: A systematic review and meta-analysis. Oncotarget 2017, 8, 107223–107236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidard, F.C.; Huguet, F.; Louvet, C.; Mineur, L.; Bouché, O.; Chibaudel, B.; Artru, P.; Desseigne, F.; Bachet, J.B.; Mathiot, C.; et al. Circulating tumor cells in locally advanced pancreatic adenocarcinoma: The ancillary CirCe 07 study to the LAP 07 trial. Ann. Oncol. 2013, 24, 2057–2061. [Google Scholar] [CrossRef] [PubMed]
- Buscail, E.; Alix-Panabières, C.; Quincy, P.; Cauvin, T.; Chauvet, A.; Degrandi, O.; Caumont, C.; Verdon, S.; Lamrissi, I.; Moranvillier, I.; et al. High Clinical Value of Liquid Biopsy to Detect Circulating Tumor Cells and Tumor Exosomes in Pancreatic Ductal Adenocarcinoma Patients Eligible for Up-Front Surgery. Cancers 2019, 11, 1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Roessel, S.; Strijker, M.; Steyerberg, E.W.; Groen, J.V.; Mieog, J.S.; Groot, V.P.; He, J.; De Pastena, M.; Marchegiani, G.; Bassi, C.; et al. International validation and update of the Amsterdam model for prediction of survival after pancreatoduodenectomy for pancreatic cancer. Eur. J. Surg. Oncol. 2020, 46, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Tol, J.A.M.G.; Brosens, L.A.A.; van Dieren, S.; van Gulik, T.M.; Busch, O.R.C.; Besselink, M.G.H.; Gouma, D.J. Impact of lymph node ratio on survival in patients with pancreatic and periampullary cancer. Br. J. Surg. 2015, 102, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Turpin, A.; Amrani, E.M.; Bachet, J.-B.; Pietrasz, D.; Schwarz, L.; Hammel, P. Adjuvant Pancreatic Cancer Management: Towards New Perspectives in 2021. Cancers 2020, 12, 3866. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-S.; Rhee, T.-M.; Pietrasz, D.; Bachet, J.-B.; Laurent-Puig, P.; Kong, S.-Y.; Takai, E.; Yachida, S.; Shibata, T.; Lee, J.W.; et al. Circulating tumor DNA as a prognostic indicator in resectable pancreatic ductal adenocarcinoma: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 16971–16977. [Google Scholar] [CrossRef]
- Hadano, N.; Murakami, Y.; Uemura, K.; Hashimoto, Y.; Kondo, N.; Nakagawa, N.; Sueda, T.; Hiyama, E. Prognostic value of circulating tumour DNA in patients undergoing curative resection for pancreatic cancer. Br. J. Cancer 2016, 115, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Sausen, M.; Phallen, J.; Adleff, V.; Jones, S.; Leary, R.J.; Barrett, M.T.; Anagnostou, V.; Parpart-Li, S.; Murphy, D.; Kay Li, Q.; et al. Clinical implications of genomic alterations in the tumour and circulation of pancreatic cancer patients. Nat. Commun. 2015, 6, 7686. [Google Scholar] [CrossRef] [PubMed]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.; Zhang, H.; Chen, N.; Hao, J.; Jin, H.; Ma, X. Diagnostic value of various liquid biopsy methods for pancreatic cancer: A systematic review and meta-analysis. Medicine (Baltimore) 2020, 99, e18581. [Google Scholar] [CrossRef] [PubMed]
- Kulemann, B.; Pitman, M.B.; Liss, A.S.; Valsangkar, N.; Fernández-Del Castillo, C.; Lillemoe, K.D.; Hoeppner, J.; Mino-Kenudson, M.; Warshaw, A.L.; Thayer, S.P. Circulating tumor cells found in patients with localized and advanced pancreatic cancer. Pancreas 2015, 44, 547–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labori, K.J.; Katz, M.H.; Tzeng, C.W.; Bjørnbeth, B.A.; Cvancarova, M.; Edwin, B.; Kure, E.H.; Eide, T.J.; Dueland, S.; Buanes, T.; et al. Impact of early disease progression and surgical complications on adjuvant chemotherapy completion rates and survival in patients undergoing the surgery first approach for resectable pancreatic ductal adenocarcinoma—A population-based cohort study. Acta Oncol. 2016, 55, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Hugenschmidt, H.; Labori, K.J.; Brunborg, C.; Verbeke, C.S.; Seeberg, L.T.; Bendigtsen Schirmer, C.; Renolen, A.; Borgen, E.; Naume, B.; Wiedswang, G. Cytokeratin-positive cells in the bone marrow from patients with pancreatic, periampullary malignancy and benign pancreatic disease show no prognostic information. BMC Cancer 2020, 20, 1107–1113. [Google Scholar] [CrossRef]
- Nordby, T.; Hugenschmidt, H.; Fagerland, M.W.; Ikdahl, T.; Buanes, T.; Labori, K.J. Follow-up after curative surgery for pancreatic ductal adenocarcinoma: Asymptomatic recurrence is associated with improved survival. Eur. J. Surg. Oncol. 2013, 39, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Zhang, L.; Peng, Y.; Tao, M.; Li, L.; Xiu, D.; Yuan, C.; Ma, Z.; Jiang, B. Neutrophils assist the metastasis of circulating tumor cells in pancreatic ductal adenocarcinoma: A new hypothesis and a new predictor for distant metastasis. Medicine (Baltimore) 2016, 95, e4932. [Google Scholar] [CrossRef]
- Bonnetain, F.; Bonsing, B.; Conroy, T.; Dousseau, A.; Glimelius, B.; Haustermans, K.; Lacaine, F.; Van Laethem, J.-L.; Aparicio, T.; Aust, D.; et al. Guidelines for time-to-event end-point definitions in trials for pancreatic cancer. Results of the DATECAN initiative (Definition for the Assessment of Time-to-event End-points in CANcer trials). Eur. J. Cancer 2014, 50, 2983–2993. [Google Scholar] [CrossRef] [PubMed]





| Demographics | n | (%) |
|---|---|---|
| Age, median [years] | 68 | (34–80) |
| Sex, male | 50 | (51.0%) |
| Preoperative Risk Factors | ||
| CTCs ≥ 1/7.5 mL | 7 | (7.1%) |
| CA19–9 ≥ 200 kU/l | 31/74 | (41.9%) 24 missing |
| Tumour size on imaging> 25 mm | 39/97 | (40.2%) 1 missing |
| Bilirubin > 50 µmol/L | 75/94 | (79.8%) 4 missing |
| Treatment | ||
| Neoadjuvant chemotherapy: | ||
| GEM | 3 | (3.0%) |
| FOLFIRINOX | 1 | (1.0%) |
| Operation: | ||
| PPPD | 77 | (78.6%) |
| PD | 13 | (13.3%) |
| Total pancreatectomy | 8 | (8.2%) |
| Venous resection | 36 | (36.7%) |
| Adjuvant chemotherapy: | ||
| FLV | 53 | (54.1%) |
| GEM | 6 | (6.1%) |
| FLOX | 3 | (3.1%) |
| none | 36 | (36.7%) |
| Histopathologic results | ||
| Pancreatobiliary type | 97 | (99%) |
| Intestinal type | 1 | (1.0%) |
| UICC-stage (V7): | ||
| Ib | 2 | (2.0%) |
| IIa | 23 | (23.5%) |
| IIb | 73 | (74.5%) |
| pN1-status | 73 | (74,5%) |
| R1-status | 61 | (62.2%) |
| Vascular infiltration | 65 | (66.3%) |
| Perineural infiltration | 91 | (92.9%) |
| Potential Risk Factors | TDM | TILR | CSS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level | n | Univariate HR (95% CI) | p | Multivariable HR (95% CI) | p | Univariate HR (95% CI) | p | Multivariable HR (95% CI) | p | Univariate HR (95% CI) | p | Multivariable HR (95% CI) | p | |
| Age | ≤70 >70 | 58 40 | 1.2 (0.7–2.1) | 0.602 | 1.3 (0.6–2.8) | 0.449 | 1.4 (0.9–2.1) | 0.156 | ||||||
| Sex | Male female | 50 48 | 0.7 (0.4–1.2) | 0.127 | 0.8 (0.4–1.7) | 0.627 | 0.8 (0.5–1.2) | 196 | ||||||
| CA19–9(24 missing) | ≥200 <200 | 43 31 | 1.2 (0.6–2.2) | 0.623 | 1.0 (0.5–2.3) | 0.939 | 1.1 (0.7–1.8) | 0.601 | ||||||
| Tumour sizeon CT(1 missing) | ≥25 mm <25 mm | 39 58 | 1.4 (0.8–2.3) | 0.272 | 2.0 (1.0–4.) | 0.057 | 1.3 (0.8–2.0) | 0.241 | ||||||
| CTC | ≥1 none | 7 91 | 3.9 (1.7–8.8) | 0.001 | 2.9 (1.3–6.6) | 0.010 | All censored | 4.4 (2.0–9.8) | <0.001 | 0.001 | ||||
| Neoadjuvant chemotherapy | Yes no | 4 94 | 1.2 (0.3–5.0) | 0.928 | 2.0 0.5–8.7) | 0.333 | 1.0 (0.4–3.7) | 0.964 | ||||||
| Venous resection | yes no | 36 62 | 0.5 (0.3–0.9) | 0.017 | eliminated | 1.6 (0.8–3.3) | 0.209 | eliminated | 0.8 (0.5–1.2) | 0.326 | eliminated | |||
| Adjuvant chemotherapy | Yes no | 62 36 | 0.8 (0.5–1.4) | 0.466 | 0.9 (0.4–1.9) | 0.735 | 0.7 (0.7–1.1) | 0.124 | ||||||
| pT | 1,2 3,4 | 3 95 | 0.7 (0.2–2.7) | 0.557 | All censored | 0.5 (0.1–1.9) | 0.300 | |||||||
| pN | 1 0 | 73 25 | 3.6 (1.7–7.3) | 0.001 | 3.0 (1.5–6.3) | 0.003 | 1.6 (0.7–3.6) | 0.226 | eliminated | 2.1 (1.2–3.5) | 0.004 | 2.0 (1.2–3.4) | 0.009 | |
| Grade | G3,4 G1,2 | 28 70 | 2.1 (1.2–3.6) | 0.007 | 1.8 (1.1–3.1) | 0.030 | 0.6 (0.2–1.7) | 0.336 | eliminated | 1.4 (0.9–2.1) | 0.184 | eliminated | ||
| R | 1 0 | 61 37 | 1.4 (0.8–2.3) | 0.212 | eliminated | 2.3 (1.0–5.0) | 0.040 | 2.3 (1.0–5.0) | 0.040 | 1.4 (0.9–2.2) | 0.128 | eliminated | ||
| Vascular infiltration | 1 0 | 65 33 | 1.7 (0.9–3.1) | 0.075 | eliminated | 0.9 (0.4–1.9) | 0.790 | eliminated | 1.6 (1.0–2.6) | 0.034 | eliminated | |||
| Perineural infiltration | 1 0 | 91 7 | 1.3 (0.5–3.7) | 0.588 | 2.7 (0.4–19.7) | 0.334 | 1.8 (0.7–4.6) | 0.185 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hugenschmidt, H.; Labori, K.J.; Borgen, E.; Brunborg, C.; Schirmer, C.B.; Seeberg, L.T.; Naume, B.; Wiedswang, G. Preoperative CTC-Detection by CellSearch® Is Associated with Early Distant Metastasis and Impaired Survival in Resected Pancreatic Cancer. Cancers 2021, 13, 485. https://doi.org/10.3390/cancers13030485
Hugenschmidt H, Labori KJ, Borgen E, Brunborg C, Schirmer CB, Seeberg LT, Naume B, Wiedswang G. Preoperative CTC-Detection by CellSearch® Is Associated with Early Distant Metastasis and Impaired Survival in Resected Pancreatic Cancer. Cancers. 2021; 13(3):485. https://doi.org/10.3390/cancers13030485
Chicago/Turabian StyleHugenschmidt, Harald, Knut Jørgen Labori, Elin Borgen, Cathrine Brunborg, Cecilie Bendigtsen Schirmer, Lars Thomas Seeberg, Bjørn Naume, and Gro Wiedswang. 2021. "Preoperative CTC-Detection by CellSearch® Is Associated with Early Distant Metastasis and Impaired Survival in Resected Pancreatic Cancer" Cancers 13, no. 3: 485. https://doi.org/10.3390/cancers13030485