Update on the Management of Breast Cancer during Pregnancy

 , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Breast Cancer during Pregnancy: Prognosis and Biology
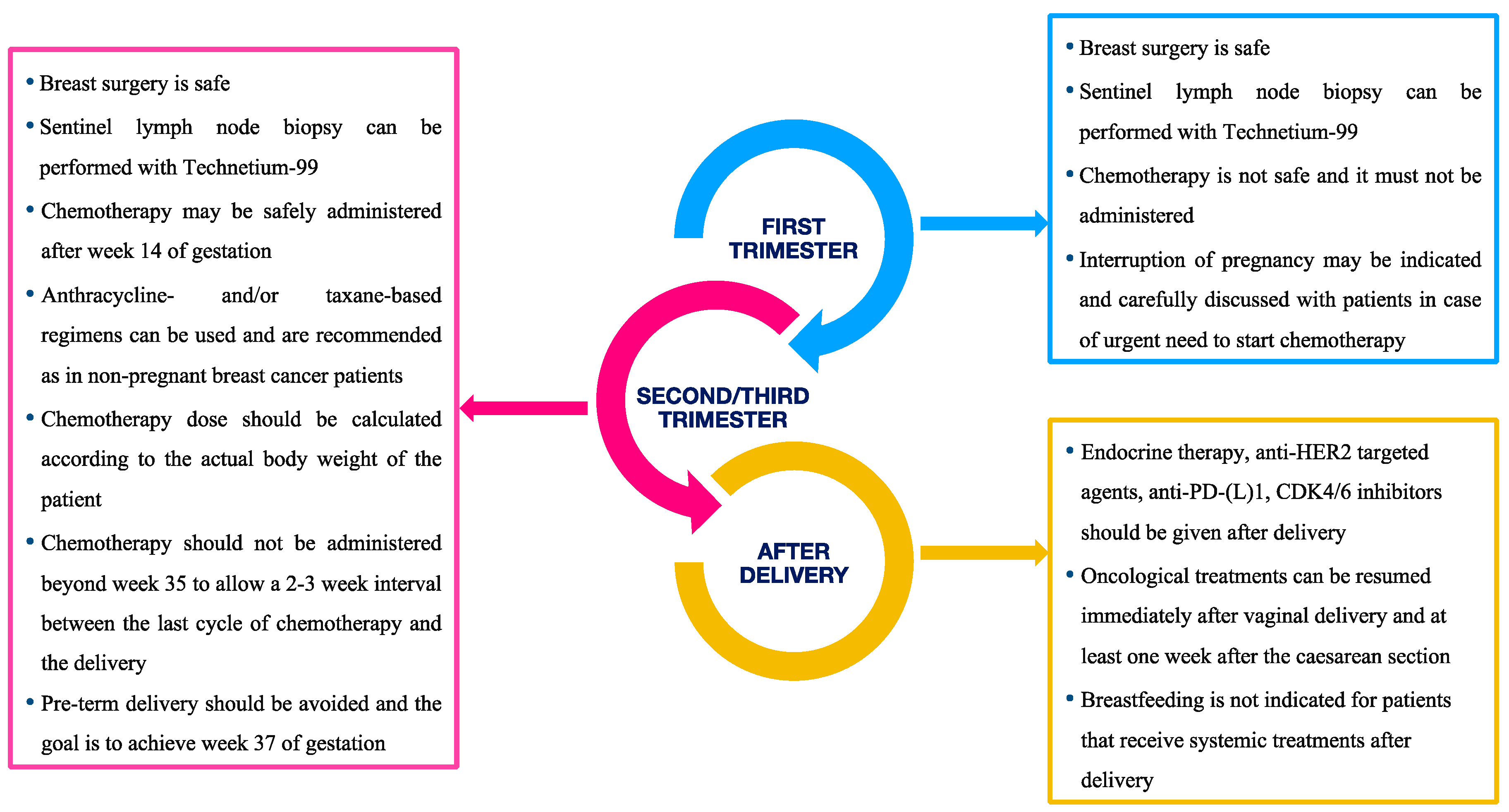
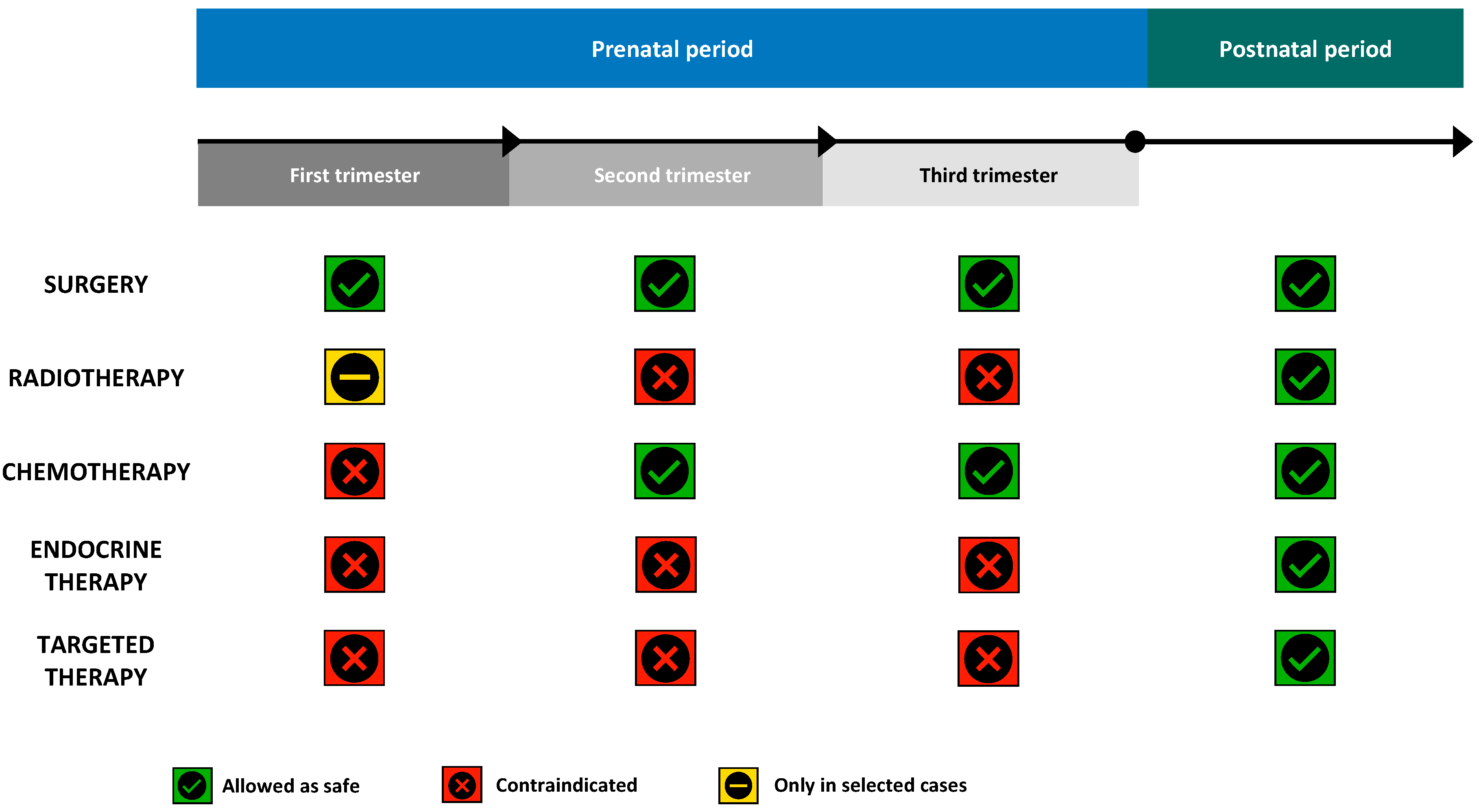
3. Anticancer Treatments during Pregnancy
3.1. Local therapy
3.2. Chemotherapy
3.3. Endocrine Therapy
3.4. Targeted Therapies
3.5. Supportive Care
3.6. Immunotherapy
4. Impact of Breast Cancer Treatment on Pregnancy Outcomes
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Dalmartello, M.; Negri, E.; La Vecchia, C.; Scarfone, G.; Buonomo, B.; Peccatori, F.A.; Parazzini, F. Frequency of Pregnancy-Associated Cancer: A Systematic Review of Population-Based Studies. Cancers 2020, 12, 1356. [Google Scholar] [CrossRef] [PubMed]
- Alfasi, A.; Ben-Aharon, I. Breast Cancer during Pregnancy—Current Paradigms, Paths to Explore. Cancers 2019, 11, 1669. [Google Scholar] [CrossRef] [Green Version]
- De Haan, J.; Verheecke, M.; Van Calsteren, K.; Van Calster, B.; Shmakov, R.G.; Mhallem Gziri, M.; Halaska, M.J.; Fruscio, R.; Lok, C.A.R.; Boere, I.A.; et al. Oncological management and obstetric and neonatal outcomes for women diagnosed with cancer during pregnancy: A 20-year international cohort study of 1170 patients. Lancet Oncol. 2018, 19, 337–346. [Google Scholar] [CrossRef]
- Silverstein, J.; Post, A.L.; Chien, A.J.; Olin, R.; Tsai, K.K.; Ngo, Z.; Van Loon, K. Multidisciplinary Management of Cancer During Pregnancy. JCO Oncol. Pract. 2020, 16, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Paluch-Shimon, S.; Cardoso, F.; Partridge, A.H.; Abulkhair, O.; Azim, H.A.; Bianchi-Micheli, G.; Cardoso, M.-J.; Curigliano, G.; Gelmon, K.A.; Harbeck, N.; et al. ESO–ESMO 4th International Consensus Guidelines for Breast Cancer in Young Women (BCY4). Ann. Oncol. 2020, 31, 674–696. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Schmidt, A.; Gentilini, O.; Kaufman, B.; Kuhl, C.; Denkert, C.; von Minckwitz, G.; Parokonnaya, A.; Stensheim, H.; Thomssen, C.; et al. Breast Cancer Diagnosed During Pregnancy: Adapting Recent Advances in Breast Cancer Care for Pregnant Patients. JAMA Oncol. 2015, 1, 1145. [Google Scholar] [CrossRef]
- Amant, F.; Loibl, S.; Neven, P.; Van Calsteren, K. Breast cancer in pregnancy. Lancet 2012, 379, 570–579. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Lambertini, M.; Scarfone, G.; Del Pup, L.; Codacci-Pisanelli, G. Biology, staging, and treatment of breast cancer during pregnancy: Reassessing the evidences. Cancer Biol. Med. 2018, 15, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Azim, H.A., Jr.; Botteri, E.; Renne, G.; Dell’Orto, P.; Rotmensz, N.; Gentilini, O.; Sangalli, C.; Pruneri, G.; Di Nubila, B.; Locatelli, M.; et al. The biological features and prognosis of breast cancer diagnosed during pregnancy: A case-control study. Acta Oncol. 2012, 51, 653–661. [Google Scholar] [CrossRef]
- Litton, J.K.; Warneke, C.L.; Hahn, K.M.; Palla, S.L.; Kuerer, H.M.; Perkins, G.H.; Mittendorf, E.A.; Barnett, C.; Gonzalez-Angulo, A.M.; Hortobágyi, G.N.; et al. Case control study of women treated with chemotherapy for breast cancer during pregnancy as compared with nonpregnant patients with breast cancer. Oncologist 2013, 18, 369–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amant, F.; von Minckwitz, G.; Han, S.N.; Bontenbal, M.; Ring, A.E.; Giermek, J.; Wildiers, H.; Fehm, T.; Linn, S.C.; Schlehe, B.; et al. Prognosis of Women With Primary Breast Cancer Diagnosed During Pregnancy: Results From an International Collaborative Study. JCO J. Clin. Oncol. 2013, 31, 2532–2539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, B.; Venet, D.; Azim, H.A.; Brown, D.; Desmedt, C.; Lambertini, M.; Majjaj, S.; Pruneri, G.; Peccatori, F.; Piccart, M.; et al. Breast cancer diagnosed during pregnancy is associated with enrichment of non-silent mutations, mismatch repair deficiency signature and mucin mutations. NPJ Breast Cancer 2018, 4, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, B.; Venet, D.; Lambertini, M.; Desmedt, C.; Salgado, R.; Horlings, H.M.; Rothé, F.; Sotiriou, C. Imprint of parity and age at first pregnancy on the genomic landscape of subsequent breast cancer. Breast Cancer Res. 2019, 21, 25. [Google Scholar] [CrossRef] [Green Version]
- Korakiti, A.-M.; Moutafi, M.; Zografos, E.; Dimopoulos, M.-A.; Zagouri, F. The Genomic Profile of Pregnancy-Associated Breast Cancer: A Systematic Review. Front. Oncol. 2020, 10, 1773. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Azim, H.A.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N.; Kesic, V.; Pentheroudakis, G. Cancer, pregnancy and fertility: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi160–vi170. [Google Scholar] [CrossRef]
- Toesca, A.; Gentilini, O.; Peccatori, F.; Azim, H.A.; Amant, F. Locoregional treatment of breast cancer during pregnancy. Gynecol. Surg. 2014, 11, 279–284. [Google Scholar] [CrossRef]
- Hershman, D.L.; Wang, X.; McBride, R.; Jacobson, J.S.; Grann, V.R.; Neugut, A.I. Delay in initiating adjuvant radiotherapy following breast conservation surgery and its impact on survival. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1353–1360. [Google Scholar] [CrossRef]
- Chen, Z.; King, W.; Pearcey, R.; Kerba, M.; Mackillop, W.J. The relationship between waiting time for radiotherapy and clinical outcomes: A systematic review of the literature. Radiother. Oncol. 2008, 87, 3–16. [Google Scholar] [CrossRef]
- Kuerer, H.M.; Gwyn, K.; Ames, F.C.; Theriault, R.L. Conservative surgery and chemotherapy for breast carcinoma during pregnancy. Surgery 2002, 131, 108–110. [Google Scholar] [CrossRef]
- Cohen-Kerem, R.; Railton, C.; Oren, D.; Lishner, M.; Koren, G. Pregnancy outcome following non-obstetric surgical intervention. Am. J. Surg. 2005, 190, 467–473. [Google Scholar] [CrossRef]
- Lyman, G.H.; Somerfield, M.R.; Bosserman, L.D.; Perkins, C.L.; Weaver, D.L.; Giuliano, A.E. Sentinel Lymph Node Biopsy for Patients with Early-Stage Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 561–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCCN Clinical Practice Guidelines in Oncology, Breast Cancer—Version 6.2020. Available online: www.nccn.org/patients (accessed on 1 October 2020).
- Azim, H.A., Jr. (Ed.) Managing Cancer during Pregnancy; Springer International Publishing: Cham, Switzerland, 2016; ISBN 978-3-319-28798-0. [Google Scholar]
- On Behalf of the International Network on Cancer, Infertility and Pregnancy; Han, S.N.; Amant, F.; Cardonick, E.H.; Loibl, S.; Peccatori, F.A.; Gheysens, O.; Sangalli, C.A.; Nekljudova, V.; Steffensen, K.D.; et al. Axillary staging for breast cancer during pregnancy: Feasibility and safety of sentinel lymph node biopsy. Breast Cancer Res. Treat. 2018, 168, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Leslie, K.K.; Koil, C.; Rayburn, W.F. Chemotherapeutic Drugs in Pregnancy. Obstet. Gynecol. Clin. N. Am. 2005, 32, 627–640. [Google Scholar] [CrossRef]
- Cardonick, E.; Iacobucci, A. Use of chemotherapy during human pregnancy. Lancet Oncol. 2004, 5, 283–291. [Google Scholar] [CrossRef]
- National Toxicology Program NTP Monograph. Developmental Effects and Pregnancy Outcomes Associated With Cancer Chemotherapy Use During Pregnancy. NTP Monogr. 2013, 2, i-214. [Google Scholar]
- Beadle, B.M.; Woodward, W.A.; Middleton, L.P.; Tereffe, W.; Strom, E.A.; Litton, J.K.; Meric-Bernstam, F.; Theriault, R.L.; Buchholz, T.A.; Perkins, G.H. The impact of pregnancy on breast cancer outcomes in women ≤35 years. Cancer 2009, 115, 1174–1184. [Google Scholar] [CrossRef] [Green Version]
- Van Calsteren, K.; Verbesselt, R.; Beijnen, J.; Devlieger, R.; De Catte, L.; Chai, D.C.; Van Bree, R.; Heyns, L.; de Hoon, J.; Amant, F. Transplacental transfer of anthracyclines, vinblastine, and 4-hydroxy-cyclophosphamide in a baboon model. Gynecol. Oncol. 2010, 119, 594–600. [Google Scholar] [CrossRef]
- Bar-Joseph, H.; Peccatori, F.A.; Goshen-Lago, T.; Cribiù, F.M.; Scarfone, G.; Miller, I.; Nemerovsky, L.; Levi, M.; Shalgi, R.; Ben-Aharon, I. Cancer During Pregnancy: The Role of Vascular Toxicity in Chemotherapy-Induced Placental Toxicity. Cancers 2020, 12, 1277. [Google Scholar] [CrossRef]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [Green Version]
- Denduluri, N.; Chavez-MacGregor, M.; Telli, M.L.; Eisen, A.; Graff, S.L.; Hassett, M.J.; Holloway, J.N.; Hurria, A.; King, T.A.; Lyman, G.H.; et al. Selection of Optimal Adjuvant Chemotherapy and Targeted Therapy for Early Breast Cancer: ASCO Clinical Practice Guideline Focused Update. JCO J. Clin. Oncol. 2018, 36, 2433–2443. [Google Scholar] [CrossRef] [PubMed]
- Poggio, F.; Bruzzone, M.; Ceppi, M.; Pondé, N.F.; La Valle, G.; Del Mastro, L.; de Azambuja, E.; Lambertini, M. Platinum-based neoadjuvant chemotherapy in triple-negative breast cancer: A systematic review and meta-analysis. Ann. Oncol. 2018, 29, 1497–1508. [Google Scholar] [CrossRef] [PubMed]
- Giacalone, P.L.; Laffargue, F.; Bénos, P. Chemotherapy for breast carcinoma during pregnancy: A French national survey. Cancer 1999, 86, 2266–2272. [Google Scholar] [CrossRef]
- Ring, A.E.; Smith, I.E.; Jones, A.; Shannon, C.; Galani, E.; Ellis, P.A. Chemotherapy for Breast Cancer During Pregnancy: An 18-Year Experience From Five London Teaching Hospitals. JCO J. Clin. Oncol. 2005, 23, 4192–4197. [Google Scholar] [CrossRef] [Green Version]
- Peccatori, F.A.; Azim, H.A.; Scarfone, G.; Gadducci, A.; Bonazzi, C.; Gentilini, O.; Galimberti, V.; Intra, M.; Locatelli, M.; Acaia, B.; et al. Weekly epirubicin in the treatment of gestational breast cancer (GBC). Breast Cancer Res. Treat. 2009, 115, 591–594. [Google Scholar] [CrossRef] [Green Version]
- García-Manero, M.; Royo, M.P.; Espinos, J.; Pina, L.; Alcazar, J.L.; López, G. Pregnancy associated breast cancer. Eur. J. Surg. Oncol. 2009, 35, 215–218. [Google Scholar] [CrossRef]
- Cardonick, E.; Dougherty, R.; Grana, G.; Gilmandyar, D.; Ghaffar, S.; Usmani, A. Breast Cancer During Pregnancy: Maternal and Fetal Outcomes. Cancer J. 2010, 16, 76–82. [Google Scholar] [CrossRef]
- Loibl, S.; Han, S.N.; von Minckwitz, G.; Bontenbal, M.; Ring, A.; Giermek, J.; Fehm, T.; Van Calsteren, K.; Linn, S.C.; Schlehe, B.; et al. Treatment of breast cancer during pregnancy: An observational study. Lancet Oncol. 2012, 13, 887–896. [Google Scholar] [CrossRef]
- Murthy, R.K.; Theriault, R.L.; Barnett, C.M.; Hodge, S.; Ramirez, M.M.; Milbourne, A.; Rimes, S.A.; Hortobagyi, G.N.; Valero, V.; Litton, J.K. Outcomes of children exposed in uteroto chemotherapy for breast cancer. Breast Cancer Res. 2014, 16, 500. [Google Scholar] [CrossRef] [Green Version]
- Safi, N.; Anazodo, A.; Dickinson, J.E.; Lui, K.; Wang, A.Y.; Li, Z.; Sullivan, E.A. In utero exposure to breast cancer treatment: A population-based perinatal outcome study. Br. J. Cancer 2019, 121, 719–721. [Google Scholar] [CrossRef]
- O’Laughlin, A.; So, S.; Fleischer, L.; Akoto, S.; Cardonick, E. Safety of Taxane Chemotherapy in Breast Cancer during Pregnancy [28O]. Obstet. Gynecol. 2019, 133, 169–170. [Google Scholar] [CrossRef]
- Tehrani, O.S. Systemic Treatments in Pregnancy-Associated Breast Cancer. In Diseases of the Breast during Pregnancy and Lactation; Alipour, S., Omranipour, R., Eds.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2020; Volume 1252, pp. 115–124. ISBN 978-3-030-41595-2. [Google Scholar]
- Del Mastro, L.; De Placido, S.; Bruzzi, P.; De Laurentiis, M.; Boni, C.; Cavazzini, G.; Durando, A.; Turletti, A.; Nisticò, C.; Valle, E.; et al. Fluorouracil and dose-dense chemotherapy in adjuvant treatment of patients with early-stage breast cancer: An open-label, 2 × 2 factorial, randomised phase 3 trial. Lancet 2015, 385, 1863–1872. [Google Scholar] [CrossRef]
- Gray, R.; Bradley, R.; Braybrooke, J.; Liu, Z.; Peto, R.; Davies, L.; Dodwell, D.; McGale, P.; Pan, H.; Taylor, C.; et al. Increasing the dose intensity of chemotherapy by more frequent administration or sequential scheduling: A patient-level meta-analysis of 37 298 women with early breast cancer in 26 randomised trials. Lancet 2019, 393, 1440–1452. [Google Scholar] [CrossRef] [Green Version]
- Lambertini, M.; Ceppi, M.; Cognetti, F.; Cavazzini, G.; De Laurentiis, M.; De Placido, S.; Michelotti, A.; Bisagni, G.; Durando, A.; Valle, E.; et al. Dose-dense adjuvant chemotherapy in premenopausal breast cancer patients: A pooled analysis of the MIG1 and GIM2 phase III studies. Eur. J. Cancer 2017, 71, 34–42. [Google Scholar] [CrossRef]
- Cardonick, E.; Gilmandyar, D.; Somer, R.A. Maternal and Neonatal Outcomes of Dose-Dense Chemotherapy for Breast Cancer in Pregnancy. Obstet. Gynecol. 2012, 120, 1267–1272. [Google Scholar] [CrossRef]
- Van Calsteren, K.; Verbesselt, R.; Ottevanger, N.; Halaska, M.; Heyns, L.; Van Bree, R.; de Bruijn, E.; Chai, D.; Delforge, M.; Noens, L.; et al. Pharmacokinetics of chemotherapeutic agents in pregnancy: A preclinical and clinical study. Acta Obstet. Gynecol. Scand. 2010, 89, 1338–1345. [Google Scholar] [CrossRef]
- Berveiller, P.; Mir, O.; Degrelle, S.A.; Tsatsaris, V.; Selleret, L.; Guibourdenche, J.; Evain-Brion, D.; Fournier, T.; Gil, S. Chemotherapy in pregnancy: Exploratory study of the effects of paclitaxel on the expression of placental drug transporters. Investig. New Drugs 2019, 37, 1075–1085. [Google Scholar] [CrossRef]
- Barthelmes, L.; Gateley, C.A. Tamoxifen and pregnancy. Breast 2004, 13, 446–451. [Google Scholar] [CrossRef]
- Halakivi-Clarke, L.; Cho, E.; Onojafe, I.; Liao, D.J.; Clarke, R. Maternal exposure to tamoxifen during pregnancy increases carcinogen-induced mammary tumorigenesis among female rat offspring. Clin. Cancer Res. 2000, 6, 305–308. [Google Scholar]
- Buonomo, B.; Brunello, A.; Noli, S.; Miglietta, L.; Del Mastro, L.; Lambertini, M.; Peccatori, F.A. Tamoxifen Exposure during Pregnancy: A Systematic Review and Three More Cases. Breast Care 2020, 15, 148–156. [Google Scholar] [CrossRef]
- Al Jishi, T.; Sergi, C. Current perspective of diethylstilbestrol (DES) exposure in mothers and offspring. Reprod. Toxicol. 2017, 71, 71–77. [Google Scholar] [CrossRef]
- Lambertini, M.; Peccatori, F.A.; Demeestere, I.; Amant, F.; Wyns, C.; Stukenborg, J.-B.; Paluch-Shimon, S.; Halaska, M.J.; Uzan, C.; Meissner, J.; et al. Fertility preservation and post-treatment pregnancies in post-pubertal cancer patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2020, 31, 1664–1678. [Google Scholar] [CrossRef] [PubMed]
- Tiboni, G.M. Aromatase inhibitors and teratogenesis. Fertil. Steril. 2004, 81, 1158–1159. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Peccatori, F.A.; Azim, H.A. Targeted agents for cancer treatment during pregnancy. Cancer Treat. Rev. 2015, 41, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Zagouri, F.; Sergentanis, T.N.; Chrysikos, D.; Papadimitriou, C.A.; Dimopoulos, M.-A.; Bartsch, R. Trastuzumab administration during pregnancy: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2013, 137, 349–357. [Google Scholar] [CrossRef]
- Goodyer, P.R.; Cybulsky, A.; Goodyer, C. Expression of the epidermal growth factor receptor in fetal kidney. Pediatr. Nephrol. 1993, 7, 612–615. [Google Scholar] [CrossRef]
- Pentšuk, N.; van der Laan, J.W. An interspecies comparison of placental antibody transfer: New insights into developmental toxicity testing of monoclonal antibodies. Birth Defects Res. B 2009, 86, 328–344. [Google Scholar] [CrossRef]
- Lambertini, M.; Di Maio, M.; Pagani, O.; Curigliano, G.; Poggio, F.; Del Mastro, L.; Paluch-Shimon, S.; Loibl, S.; Partridge, A.H.; Demeestere, I.; et al. The BCY3/BCC 2017 survey on physicians’ knowledge, attitudes and practice towards fertility and pregnancy-related issues in young breast cancer patients. Breast 2018, 42, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020. [Google Scholar] [CrossRef]
- Kelly, H.; Graham, M.; Humes, E.; Dorflinger, L.J.; Boggess, K.A.; O’Neil, B.H.; Harris, J.; Spector, N.L.; Dees, E.C. Delivery of a Healthy Baby After First-Trimester Maternal Exposure to Lapatinib. Clin. Breast Cancer 2006, 7, 339–341. [Google Scholar] [CrossRef]
- Lambertini, M.; Martel, S.; Campbell, C.; Guillaume, S.; Hilbers, F.S.; Schuehly, U.; Korde, L.; Azim, H.A.; Di Cosimo, S.; Tenglin, R.C.; et al. Pregnancies during and after trastuzumab and/or lapatinib in patients with human epidermal growth factor receptor 2-positive early breast cancer: Analysis from the NeoALTTO (BIG 1-06) and ALTTO (BIG 2-06) trials: Pregnancies in Women with HER2+ Breast Cancer. Cancer 2019, 125, 307–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, S.R.D.; Harbeck, N.; Hegg, R.; Toi, M.; Martin, M.; Shao, Z.M.; Zhang, Q.Y.; Martinez Rodriguez, J.L.; Campone, M.; Hamilton, E.; et al. Abemaciclib Combined with Endocrine Therapy for the Adjuvant Treatment of HR+, HER2−, Node-Positive, High-Risk, Early Breast Cancer (monarchE). JCO J. Clin. Oncol. 2020, 38, 3987–3998. [Google Scholar] [CrossRef] [PubMed]
- Pasternak, B.; Svanström, H.; Hviid, A. Ondansetron in Pregnancy and Risk of Adverse Fetal Outcomes. N. Engl. J. Med. 2013, 368, 814–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koren, G.; Madjunkova, S.; Maltepe, C. The protective effects of nausea and vomiting of pregnancy against adverse fetal outcome—A systematic review. Reprod. Toxicol. 2014, 47, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.E.; Van Bennekom, C.; Anderka, M.; Mitchell, A.A. Ondansetron for Treatment of Nausea and Vomiting of Pregnancy and the Risk of Specific Birth Defects. Obstet. Gynecol. 2018, 132, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, Y.C.; Richardson, J.L.; Keskin-Arslan, E.; Erol-Coskun, H.; Kennedy, D. Use of ondansetron during pregnancy and the risk of major congenital malformations: A systematic review and meta-analysis. Reprod. Toxicol. 2019, 86, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Picot, C.; Berard, A.; Grenet, G.; Ripoche, E.; Cucherat, M.; Cottin, J. Risk of malformation after ondansetron in pregnancy: An updated systematic review and meta-analysis. Birth Defects Res. 2020, 112, 996–1013. [Google Scholar] [CrossRef]
- Garbis, H.; Elefant, E.; Diavcitrin, O.; Mastroiacovo, P.; Schaefer, C.; Vial, T.; Clementi, M.; Valti, E.; Mcelhatton, P.; Smorlesi, C. Pregnancy outcome after exposure to ranitidine and other H2-blockersA collaborative study of the European Network of Teratology Information Services. Reprod. Toxicol. 2005, 19, 453–458. [Google Scholar] [CrossRef]
- Matthews, S.G. Antenatal glucocorticoids and the developing brain: Mechanisms of action. Semin. Neonatol. 2001, 6, 309–317. [Google Scholar] [CrossRef]
- Sloboda, D.; Challis, J.; Moss, T.; Newnham, J. Synthetic Glucocorticoids: Antenatal Administration and Long-term Implications. CPD Curr. Pharm. Des. 2005, 11, 1459–1472. [Google Scholar] [CrossRef] [Green Version]
- Alexander, N.; Rosenlöcher, F.; Stalder, T.; Linke, J.; Distler, W.; Morgner, J.; Kirschbaum, C. Impact of Antenatal Synthetic Glucocorticoid Exposure on Endocrine Stress Reactivity in Term-Born Children. J. Clin. Endocrinol. Metab. 2012, 97, 3538–3544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallensteen, L.; Zimmermann, M.; Thomsen Sandberg, M.; Gezelius, A.; Nordenström, A.; Hirvikoski, T.; Lajic, S. Sex-Dimorphic Effects of Prenatal Treatment With Dexamethasone. J. Clin. Endocrinol. Metab. 2016, 101, 3838–3846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowther, C.A.; Doyle, L.W.; Haslam, R.R.; Hiller, J.E.; Harding, J.E.; Robinson, J.S. Outcomes at 2 Years of Age after Repeat Doses of Antenatal Corticosteroids. N. Engl. J. Med. 2007, 357, 1179–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dale, D.C.; Cottle, T.E.; Fier, C.J.; Bolyard, A.A.; Bonilla, M.A.; Boxer, L.A.; Cham, B.; Freedman, M.H.; Kannourakis, G.; Kinsey, S.E.; et al. Severe chronic neutropenia: Treatment and follow-up of patients in the Severe Chronic Neutropenia International Registry. Am. J. Hematol. 2003, 72, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Boxer, L.A.; Bolyard, A.A.; Kelley, M.L.; Marrero, T.M.; Phan, L.; Bond, J.M.; Newburger, P.E.; Dale, D.C. Use of granulocyte colony-stimulating factor during pregnancy in women with chronic neutropenia. Obstet. Gynecol. 2015, 125, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Dieras, V.; Henschel, V.; Molinero, L.; Chui, S.Y.; et al. IMpassion130: Updated overall survival (OS) from a global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab (atezo) + nab- paclitaxel (nP) in previously untreated locally advanced or metastatic triple-negative breast cancer (mTNBC). JCO J. Clin. Oncol. 2019, 37, 1003. [Google Scholar] [CrossRef]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): A randomised, double-blind, phase 3 trial. Lancet 2020. [Google Scholar] [CrossRef]
- Luppi, P. How immune mechanisms are affected by pregnancy. Vaccine 2003, 21, 3352–3357. [Google Scholar] [CrossRef]
- Hepner, A.; Negrini, D.; Hase, E.A.; Exman, P.; Testa, L.; Trinconi, A.F.; Filassi, J.R.; Francisco, R.P.V.; Zugaib, M.; O’Connor, T.L.; et al. Cancer during Pregnancy: The Oncologist Overview. World J. Oncol. 2019, 10, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Lu, D.; Ludvigsson, J.F.; Smedby, K.E.; Fall, K.; Valdimarsdóttir, U.; Cnattingius, S.; Fang, F. Maternal Cancer During Pregnancy and Risks of Stillbirth and Infant Mortality. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 1522–1529. [Google Scholar] [CrossRef] [PubMed]
- Shechter Maor, G.; Czuzoj-Shulman, N.; Spence, A.R.; Abenhaim, H.A. Neonatal outcomes of pregnancy-associated breast cancer: Population-based study on 11 million births. Breast J. 2019, 25, 86–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, K.M.E.; Johnson, P.H.; Gordon, N.; Kuerer, H.; Middleton, L.; Ramirez, M.; Yang, W.; Perkins, G.; Hortobagyi, G.N.; Theriault, R.L. Treatment of pregnant breast cancer patients and outcomes of children exposed to chemotherapy in utero. Cancer 2006, 107, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Vandenbroucke, T.; Verheecke, M.; Fumagalli, M.; Halaska, M.J.; Boere, I.; Han, S.; Gziri, M.M.; Peccatori, F.; Rob, L.; et al. Pediatric Outcome after Maternal Cancer Diagnosed during Pregnancy. N. Engl. J. Med. 2015, 373, 1824–1834. [Google Scholar] [CrossRef]
- Cardonick, E.H.; Gringlas, M.B.; Hunter, K.; Greenspan, J. Development of children born to mothers with cancer during pregnancy: Comparing in utero chemotherapy-exposed children with nonexposed controls. Am. J. Obstet. Gynecol. 2015, 212, 658.e1–658.e8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study, Year | Patients Treated with Chemotherapy, N | Type of Regimen | Gestational Age at the Beginning of CT, Weeks | Gestational Age at Delivery, Weeks | Pregnancy Complications and Fetal Outcomes |
|---|---|---|---|---|---|
| Giacalone, 1996 [35] | 29 | FEC, FAC, EC, VEM, VA, FA | 26 | 34.7 | 35% obstetrical complications 10% spontaneous abortion 5% stillbirth No malformations |
| Ring, 2005 [36] | 28 | AC, EC | 20 | 37 | 19% obstetrical complications 4% spontaneous abortion No stillbirths 4% malformations |
| Peccatori, 2009 [37] | 20 | Weekly epirubicin | Not reported | 35 | 10% obstetrical complications No abortion No stillbirths 5% malformations |
| Garcia-Manero, 2009 [38] | 15 | A and Docetaxel, FAC | Not reported | Not reported | 27% obstetrical complications No spontaneous abortion, stillbirths and malformations |
| Cardonick, 2010 [39] | 104 | AC, FAC, EC, FEC, anthracycline followed by taxane | 20.4 | 35.8 | 24% obstetrical complications 5% spontaneous abortion 4% malformations Stillbirths not reported |
| Loibl, 2012 [40] | 197 | A, E, AC, EC, FAC, FEC, anthracycline followed by CMF. Anthracycline followed by taxane | 24 | 37 | 17% obstetrical complications 4% malformations 1% spontaneous abortion and stillbirth |
| Murthy, 2014 [41] | 81 | FAC | Not reported | 37 | 33% obstetrical complications 4% malformations Spontaneous abortion and stillbirths not reported |
| Safi, 2019 [42] | 18 | A, E, Docetaxel, Paclitaxel, | 20 weeks | 35.7 | 12% obstetrical complications No stillbirths and congenital malformations |
| O’Laughlin, 2019 [43] | 50 | AC plus taxane | Not reported | Not reported | Obstetrical complications were not significantly different as compared to patients treated with only anthracycline |
| Study, Year | Type of Mother’s Cancer | Type of Systemic Treatments | Results |
|---|---|---|---|
| Hahn, 2006 [86] | Breast cancer | 5′-fluorouracil, doxorubicin and cyclophosphamide | No stillbirths, miscarriages, or perinatal deaths 1 subarachnoid hemorrhage, 1 Down’s syndrome |
| Murthy, 2014 [41] | Breast cancer | 5′-fluorouracil, doxorubicin and cyclophosphamide | No significant impairment of baby health at delivery and up to childhood 3 babies with congenital abnormalities |
| Amant, 2015 [87] | Breast cancer, hematological malignancies, cervical cancer, ovarian cancer, brain tumor, colon cancer, gastric cancer, renal cell cancer, tongue cancer, lung cancer, thyroid cancer, melanoma, sarcoma | Anthracycline-based, anthracycline plus taxane, CMF, taxane-based, platinum-agents, vinca alkaloid, dacarbazine, temozolomide, mitoxantrone | Comparison with control group (babies from healthy women without in utero exposure to chemotherapy):
|
| Cardonick, 2015 [88] | Breast cancer, ovarian cancer, hematological malignancies | Anthracycline-based, anthracycline plus taxane, taxane-based | Comparison with control group (babies from women also diagnosed with a cancer during pregnancy, but without in utero exposure to chemotherapy):
|
| O’Laughlin, 2019 [43] | Breast cancer | Anthracycline plus taxane | Comparison with taxanes administration delayed to the postpartum period:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poggio, F.; Tagliamento, M.; Pirrone, C.; Soldato, D.; Conte, B.; Molinelli, C.; Cosso, M.; Fregatti, P.; Del Mastro, L.; Lambertini, M. Update on the Management of Breast Cancer during Pregnancy. Cancers 2020, 12, 3616. https://doi.org/10.3390/cancers12123616
Poggio F, Tagliamento M, Pirrone C, Soldato D, Conte B, Molinelli C, Cosso M, Fregatti P, Del Mastro L, Lambertini M. Update on the Management of Breast Cancer during Pregnancy. Cancers. 2020; 12(12):3616. https://doi.org/10.3390/cancers12123616
Chicago/Turabian StylePoggio, Francesca, Marco Tagliamento, Chiara Pirrone, Davide Soldato, Benedetta Conte, Chiara Molinelli, Maurizio Cosso, Piero Fregatti, Lucia Del Mastro, and Matteo Lambertini. 2020. "Update on the Management of Breast Cancer during Pregnancy" Cancers 12, no. 12: 3616. https://doi.org/10.3390/cancers12123616