Unraveling the Heterogeneity of Sarcoma Survivors’ Health-Related Quality of Life Regarding Primary Sarcoma Location: Results from the SURVSARC Study

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
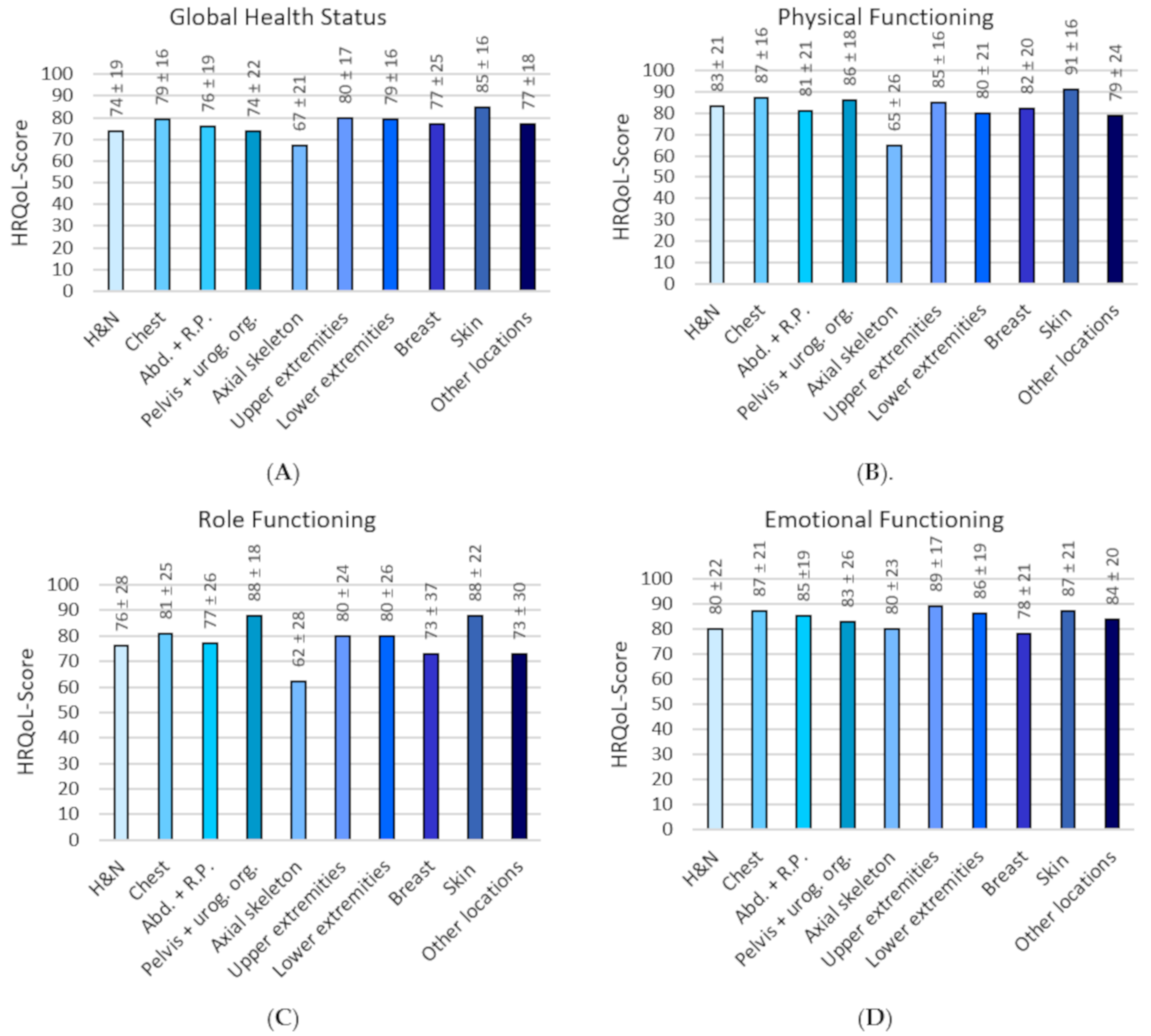
2.2. Mean HRQoL Scores for Each Domain of the EORTC-QLQ-C30
2.3. Influence of Location on HRQoL
2.4. Treatment-Specific HRQoL Issues per Sarcoma Location
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Recruitment and Data Collection
4.3. Socio-Demographic and Clinical Characteristics
4.4. HRQoL
4.5. Treatment-Specific HRQoL Issues
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours, WHO Classification of Tumour, 5th ed.; WHO Press: Geneva, Switzerland, 2020. [Google Scholar]
- Burningham, Z.; Hashibe, M.; Spector, L.G.; Schiffman, J.D. The Epidemiology of Sarcoma. Clin. Sarcoma Res. 2012, 2, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Information Network on Rare Cancers. Available online: http://www.rarecarenet.eu (accessed on 30 March 2020).
- Stiller, C.A.; Botta, L.; Brewster, D.; Ho, V.; Frezza, A.M.; Whelan, J.; Casali, P.G.; Trama, A.; Gatta, G. Survival of adults with cancers of bone or soft tissue in Europe—Report from the EUROCARE-5 study. Cancer Epidemiol. 2018, 56, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, A.C.; Gronchi, A.; Cardona, K. Soft-tissue sarcoma in adults: An update on the current state of histiotype-specific management in an era of personalized medicine. CA Cancer J. Clin. 2020, 70, 200–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, J.L.; Turner, S.P. Bone Cancer: Diagnosis and Treatment Principles. Am. Fam. Physician 2018, 98, 205–213. [Google Scholar]
- Frisch, S.; Timmermann, B. The Evolving Role of Proton Beam Therapy for Sarcomas. Clin. Oncol. 2017, 29, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Deroose, J.P.; Eggermont, A.M.; Van Geel, A.N.; Burger, J.W.; Bakker, M.A.D.; De Wilt, J.H.W.; Verhoef, C. Long-Term Results of Tumor Necrosis Factor α– and Melphalan-Based Isolated Limb Perfusion in Locally Advanced Extremity Soft Tissue Sarcomas. J. Clin. Oncol. 2011, 29, 4036–4044. [Google Scholar] [CrossRef]
- Linch, M.; Miah, A.B.; Thway, K.; Judson, I.; Benson, C. Systemic treatment of soft-tissue sarcoma—Gold standard and novel therapies. Nat. Rev. Clin. Oncol. 2014, 11, 187–202. [Google Scholar] [CrossRef]
- Kluetz, P.G.; Slagle, A.; Papadopoulos, E.J.; Johnson, L.L.; Donoghue, M.; Kwitkowski, V.E.; Chen, W.-H.; Sridhara, R.; Farrell, A.T.; Keegan, P.; et al. Focusing on Core Patient-Reported Outcomes in Cancer Clinical Trials: Symptomatic Adverse Events, Physical Function, and Disease-Related Symptoms. Clin. Cancer Res. 2016, 22, 1553–1558. [Google Scholar] [CrossRef] [Green Version]
- Di Maio, M.; Basch, E.; Bryce, J.; Perrone, F. Patient-reported outcomes in the evaluation of toxicity of anticancer treatments. Nat. Rev. Clin. Oncol. 2016, 13, 319–325. [Google Scholar] [CrossRef]
- McDonough, J.; Eliott, J.; Neuhaus, S.; Reid, J.; Butow, P. Health-related quality of life, psychosocial functioning, and unmet health needs in patients with sarcoma: A systematic review. Psycho Oncol. 2019, 28, 653–664. [Google Scholar] [CrossRef]
- Storey, L.; Fern, L.A.; Martins, A.; Wells, M.; Bennister, L.; Gerrand, C.; Onasanya, M.; Whelan, J.S.; Windsor, R.; Woodford, J.; et al. A Critical Review of the Impact of Sarcoma on Psychosocial Wellbeing. Sarcoma 2019, 2019, 9730867. [Google Scholar] [CrossRef] [PubMed]
- Winnette, R.; Hess, L.M.; Nicol, S.J.; Tai, D.F.; Copley-Merriman, C. The Patient Experience with Soft Tissue Sarcoma: A Systematic Review of the Literature. Patient 2016, 10, 153–162. [Google Scholar] [CrossRef] [PubMed]
- IKNL. Sarcomenzorg in Nederland: Overzicht van de Nederlandse Kankerregistratie over de Periode 2009–2018. June 2020. Available online:https://www.iknl.nl/getmedia/b2538482-8e79-40d5-a4ff-90e4b1e54838/Sarcomenzorg-in-Nederland-overzicht-NKR-2009-2018.pdf (accessed on 16 October 2020).
- Diaz, R.J.; Maggacis, N.; Zhang, S.; Cusimano, M.D. Determinants of quality of life in patients with skull base chordoma. J. Neurosurg. 2014, 120, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.H.; Pan, D.J.W.; Castle, D.J.; Choong, P. A Systematic Review of the Recent Quality of Life Studies in Adult Extremity Sarcoma Survivors. Sarcoma 2012, 2012, 171342. [Google Scholar] [CrossRef]
- Schreiber, D.; Bell, R.S.; Wunder, J.S.; O’Sullivan, B.; Turcotte, R.; Masri, B.A.; Davis, A.M. Evaluating Function and Health Related Quality of Life in Patients Treated for Extremity Soft Tissue Sarcoma. Qual. Life Res. 2006, 15, 1439–1446. [Google Scholar] [CrossRef]
- Soomers, V.L.M.N.; Husson, O.; Desar, I.; van de Sande, M.A.J.; de Haan, J.J.; Verhoef, C. Patient and diagnostic intervals of sarcoma survivors: Results from the SURVSARC study. Cancer 2020. [Google Scholar] [CrossRef]
- Cocks, K.; King, M.T.; Velikova, G.; St-James, M.M.; Fayers, P.M.; Brown, J.M. Evidence-Based Guidelines for Determination of Sample Size and Interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. J. Clin. Oncol. 2011, 29, 89–96. [Google Scholar] [CrossRef]
- Hoffmann, C.; Gosheger, G.; Gebert, C.; Jürgens, H.; Winkelmann, W. Functional Results and Quality of Life After Treatment of Pelvic Sarcomas Involving the Acetabulum. J. Bone Jt. Surg. Am. 2006, 88, 575–582. [Google Scholar] [CrossRef]
- Schwab, J.H.; Janssen, S.J.; Pereira, N.R.P.; Chen, Y.L.E.; Wain, J.C.; Delaney, T.F.; Hornicek, F.J. Quality of life after resection of a chordoma of the mobile spine. Bone Jt. J. 2017, 99, 979–986. [Google Scholar] [CrossRef]
- Kohlmeyer, J.; Steimle-Grauer, S.A.; Hein, R. Cutaneous sarcomas. J. Dtsch. Dermatol. Ges. 2017, 15, 630–648. [Google Scholar] [CrossRef] [Green Version]
- Luke, J.J.; Keohan, M.L. Advances in the Systemic Treatment of Cutaneous Sarcomas. Semin. Oncol. 2012, 39, 173–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, J.S.; Matthews, B.A.; Neuburg, M.; Smith, T.L.; Burzynski, M.; Nattinger, A.B. Skin Cancer and Quality of Life: Assessment with the Dermatology Life Quality Index. Dermatol. Surg. 2004, 30, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.; Kassam, Z.; Springer, A.N.; Gladdy, R.; Chung, P.; Ringash, J.; Catton, C. Long-Term Quality of Life of Retroperitoneal Sarcoma Patients Treated with Pre-Operative Radiotherapy and Surgery. Cureus 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callegaro, D.; Miceli, R.; Brunelli, C.; Colombo, C.; Sanfilippo, R.; Radaelli, S.; Casali, P.G.; Caraceni, A.; Gronchi, A.; Fiore, M. Long-term morbidity after multivisceral resection for retroperitoneal sarcoma. BJS 2015, 102, 1079–1087. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Courneya, K.S.; Robbins, K.T.; Rao, K.; Malone, J.; Seiz, A.; Reminger, S.; Markwell, S.J.; Burra, V. Factors associated with fatigue, sleep, and cognitive function among patients with head and neck cancer. Head Neck 2008, 30, 1310–1317. [Google Scholar] [CrossRef]
- Kuo, P.Y.; Yen, J.T.C.; Parker, G.M.; Chapman, S.; Kandikattu, S.; Sohanpal, I.; Barbachano, Y.; Williams, J.E. The Prevalence of Pain in Patients Attending Sarcoma Outpatient Clinics. Sarcoma 2011, 2011, 813483. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.; Kim, I.; Choi, E.; Im, Y.H.; Park, Y.H.; Ahn, J.S.; Lee, J.E.; Nam, S.J.; Lee, H.K.; Park, J.-H.; et al. Permanent Chemotherapy-Induced Alopecia in Patients with Breast Cancer: A 3-Year Prospective Cohort Study. Oncologist 2018, 24, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinoshita, T.; Nakayama, T.; Fukuma, E.; Inokuchi, M.; Ishiguro, H.; Ogo, E.; Kikuchi, M.; Jinno, H.; Yamazaki, N.; Toi, M. Efficacy of Scalp Cooling in Preventing and Recovering From Chemotherapy-Induced Alopecia in Breast Cancer Patients: The HOPE Study. Front. Oncol. 2019, 9, 733. [Google Scholar] [CrossRef] [Green Version]
- Martins, A.; Bennister, L.; Fern, L.A.; Gerrand, C.; Onasanya, M.; Storey, L.; Wells, M.; Whelan, J.S.; Windsor, R.; Woodford, J.; et al. Development of a patient-reported experience questionnaire for patients with sarcoma: The Sarcoma Assessment Measure (SAM). Qual. Life Res. 2020, 29, 2287–2297. [Google Scholar] [CrossRef]
- Husson, O.; Den Hollander, D.; Van Der Graaf, W.T.A. The complexity of assessing health-related quality of life among sarcoma patients. Qual. Life Res. 2020, 1–2. [Google Scholar] [CrossRef]
- Hudgens, S.; Forsythe, A.; Kontoudis, I.; D’Adamo, D.; Bird, A.; Gelderblom, H. Evaluation of Quality of Life at Progression in Patients with Soft Tissue Sarcoma. Sarcoma 2017, 2017, 2372135. [Google Scholar] [CrossRef] [Green Version]
- Netherlands Cancer Registry (NCR). Available online: https://www.iknl.nl/en/ncr (accessed on 5 April 2020).
- Fritz, A.G. International Classification of Diseases for Oncology: ICD-O, 3rd ed.; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Patient Reported Outcomes Following Initial treatment and Long-term Evaluation of Survivorship (PROFILES). Available online: https://www.profilesregistry.nl (accessed on 5 April 2020).
- Van De Poll-Franse, L.V.; Horevoorts, N.; Van Eenbergen, M.; Denollet, J.; Roukema, J.A.; Aaronson, N.K.; Vingerhoets, A.; Coebergh, J.W.; De Vries, J.; Essink-Bot, M.-L.; et al. The Patient Reported Outcomes Following Initial treatment and Long term Evaluation of Survivorship registry: Scope, rationale and design of an infrastructure for the study of physical and psychosocial outcomes in cancer survivorship cohorts. Eur. J. Cancer 2011, 47, 2188–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangha, O.; Stucki, G.; Liang, M.H.; Fossel, A.H.; Katz, J.N. The self-administered comorbidity questionnaire: A new method to assess comorbidity for clinical and health services research. Arthritis Rheum. 2003, 49, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; De Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Groenvold, M.; Aaronson, N.K.; Darlington, A.-S.E.; Fitzsimmons, D.; Greimel, E.; Holzner, B.; Reijneveld, J.C.; Tomaszewski, K.A.; Leeuw, I.V.-D.; Van De Poll-Franse, L.V. Focusing on Core Patient-Reported Outcomes in Cancer Clinical Trials—Letter. Clin. Cancer Res. 2016, 22, 5617. [Google Scholar] [CrossRef] [Green Version]
- Davis, A.M.; Wright, J.G.; Williams, J.I.; Bombardier, C.; Griffin, A.; Bell, R.S. Development of a measure of physical function for patients with bone and soft tissue sarcoma. Qual. Life Res. 1996, 5, 508–516. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total N = 1099 | H and N 1 N = 72 | Thorax N = 97 | Abd. and R.P. 2 N = 106 | Pelvis and Urogen. Org. 3 N = 28 | Axial Skel. 4 N = 57 | Upper Extr. 5 N = 116 | Lower Extr. 5 N = 405 | Breast N = 25 | Skin N = 110 | Other N = 83 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender, N (%), p < 0.001 | |||||||||||
| Male | 596 (54) | 41 (57) | 52 (54) | 57 (54) | 8 (29) | 35 (61) | 76 (66) | 218 (54) | 1 (4) | 64 (58) | 44 (53) |
| Female | 503 (46) | 31 (43) | 45 (46) | 49 (46) | 20 (71) | 22 (39) | 40 (34) | 187 (46) | 24 (96) | 46 (42) | 39 (47) |
| Age, Mean ± SD, p = 0.067 | |||||||||||
| (In years) | 60 ± 15 | 56 ± 15 | 60 ± 16 | 63 ± 13 | 63 ± 10 | 60 ± 17 | 62 ± 16 | 60 ± 15 | 66 ± 12 | 59 ± 16 | 59 ± 16 |
| Sarcoma Subtype *, N (%), p < 0.001 | |||||||||||
| STS 6 | 829 (75) | 35 (49) | 59 (61) | 102 (96) | 28 (100) | 1 (2) 18 | 85 (73) | 304 (75) | 25 (100) | 110 (100) | 80 (96) |
| BS 7 | 270 (25) | 37 (51) | 38 (39) | 4 (4) 17 | 0 (0) | 56 (98) | 31 (27) | 101 (25) | 0 (0) | 0 (0) | 3 (4) |
| Stage, N (%), p < 0.001 | |||||||||||
| I | 486 (44) | 24 (34) | 20 (21) | 52 (49) | 4 (14) | 20 (35) | 50 (43) | 176 (43) | 4 (16) | 95 (86) | 41 (50) |
| II | 315 (29) | 26 (36) | 42 (43) | 20 (19) | 1 (4) | 18 (32) | 41 (35) | 142 (35) | 3 (12) | 4 (4) | 18 (22) |
| III | 134 (12) | 1 (1) | 19 (20) | 21 (20) | 0 (0) | 0 (0) | 17 (15) | 60 (15) | 3 (12) | 1 (1) | 12 (14) |
| IV | 58 (5) | 8 (11) | 2 (2) | 7 (6) | 2 (7) | 12 (20) | 5 (4) | 14 (4) | 2 (8) | 1 (1) | 5 (6) |
| Missing | 106 (10) | 13 (18) | 14 (14) | 6 (6) | 21 (75) | 7 (13) | 3 (3) | 13 (3) | 13 (52) | 9 (8) | 7 (8) |
| Treatment, N (%), p < 0.000 | |||||||||||
| S 8 | 448 (41) | 15 (21) | 41 (43) | 47 (44) | 21 (75) | 21 (36) | 40 (34) | 131 (33) | 11 (44) | 94 (86) | 27 (33) |
| S and R 9 | 422 (38) | 29 (40) | 32 (33) | 26 (25) | 4 (14) | 18 (32) | 54 (47) | 195 (48) | 8 (32) | 10 (9) | 46 (55) |
| S and C 10 | 79 (7) | 9 (13) | 9 (9) | 12 (11) | 0 (0) | 3 (5) | 9 (8) | 33 (8) | 2 (8) | 1 (1) | 1 (1) |
| S, R and C 11 | 86 (8) | 8 (11) | 11 (11) | 12 (11) | 2 (7) | 5 (9) | 8 (7) | 33 (8) | 1 (4) | 0 (0) | 6 (7) |
| Missing | 64 (6) | 11 (15) | 4 (4) | 9 (9) | 1 (4) | 10 (18) | 5 (4) | 13 (3) | 3 (12) | 3 (4) | 3 (4) |
| Time since Diagnosis, Mean ± SD, p = 0.223 | |||||||||||
| (in months) | 67 ± 30 | 68 ± 30 | 64 ± 31 | 61 ± 26 | 67 ± 28 | 73 ± 30 | 69 ± 34 | 69 ± 31 | 58 ± 22 | 67 ± 30 | 67 ± 30 |
| Comorbidities, N (%), p = 0.050 | |||||||||||
| 0 | 369 (34) | 30 (42) | 28 (29) | 29 (28) | 5 (18) | 18 (32) | 31 (27) | 159 (40) | 4 (16) | 38 (34) | 27 (32) |
| 1 | 355 (32) | 17 (23) | 35 (36) | 30 (28) | 8 (28) | 23 (40) | 43 (37) | 123 (30) | 11 (44) | 37 (34) | 28 (34) |
| ≥2 | 375 (34) | 25 (35) | 34 (35) | 47 (44) | 15 (54) | 16 (28) | 42 (36) | 123 (30) | 10 (40) | 35 (32) | 28 (34) |
| Marital Status, N (%), p = 0.006 | |||||||||||
| Together 12 | 857 (78) | 55 (76) | 68 (70) | 81 (76) | 25 (89) | 42 (74) | 87 (75) | 335 (83) | 21 (84) | 90 (82) | 53 (64) |
| Single 13 | 240 (22) | 17 (24) | 29 (30) | 25 (24) | 3 (11) | 15 (26) | 27 (23) | 70 (17) | 4 (16) | 20 (18) | 30 (36) |
| Missing | 2 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Education, N (%), p = 0.174 | |||||||||||
| No education 14 | 242 (22) | 8 (11) | 23 (24) | 23 (22) | 8 (29) | 17 (30) | 29 (25) | 90 (22) | 9 (36) | 20 (18) | 15 (18) |
| College 15 | 851 (77) | 63 (88) | 74 (76) | 82 (77) | 20 (71) | 40 (70) | 86 (74) | 313 (77) | 16 (64) | 90 (82) | 67 (81) |
| Missing | 6 (1) | 1 (1) | 0 (0) | 1 (1) | 0 (0) | 0 (0) | 1 (1) | 2 (1) | 0 (0) | 0 (0) | 1 (1) |
| Employment, N (%), p = 0.115 | |||||||||||
| Work 16 | 548 (50) | 40 (56) | 43 (44) | 46 (43) | 14 (50) | 28 (49) | 53 (46) | 205 (51) | 9 (36) | 62 (56) | 48 (58) |
| Other | 510 (46) | 26 (36) | 52 (54) | 56 (53) | 14 (50) | 26 (46) | 55 (47) | 191 (47) | 14 (56) | 43 (39) | 33 (40) |
| Missing | 41 (4) | 6 (8) | 2 (2) | 4 (4) | 0 (0) | 3 (5) | 8 (7) | 9 (2) | 2 (8) | 5 (5) | 2 (2) |
| EORTC QLQ-C30 Scale per Location | One-Way ANOVA with Post Hoc Bonferroni | Adjusted-Multivariate Linear Regression (Axial Skeleton as Reference Group) | |||||
|---|---|---|---|---|---|---|---|
| Column Name | MD | 95% CI | MD | 95% CI | Clinical Relevance 1 | ||
| Global health status | |||||||
| Head and Neck[u10] [i.11] | 6.9 | −3.7 | 17.5 | 5.7 | −0.6 | 12.1 | N.A. |
| Chest | 12.1 | 2.2 | 21.9 | 11.8 | 5.7 | 17.9 | Medium |
| Abd. and R.P.* | 9.2 | −0.5 | 18.9 | 9.3 | 2.9 | 15.8 | N.A. |
| Pelvis and urogenital organs | 7.3 | −6.1 | 20.7 | 5.2 | −3.5 | 14.0 | N.A. |
| Upper extremities | 12.8 | 3.2 | 22.4 | 12.3 | 6.3 | 18.4 | Medium |
| Lower extremities | 12.0 | 3.7 | 20.4 | 10.1 | 4.7 | 15.5 | Medium |
| Breast | 9.7 | −4.9 | 24.3 | 8.2 | −1.0 | 17.3 | N.A. |
| Skin | 18.1 | 8.4 | 27.7 | 14.2 | 7.6 | 20.8 | Medium |
| Other locations | 9.8 | −0.3 | 20.0 | 8.6 | 2.1 | 15.2 | N.A. |
| Physical functioning | |||||||
| Head and Neck | 18.0 | 5.9 | 30.1 | 13.6 | 6.6 | 20.5 | Small |
| Chest | 22.6 | 11.3 | 33.8 | 18.9 | 12.2 | 25.5 | Medium |
| Abd. and R.P.* | 16.0 | 5.0 | 27.0 | 10.1 | 3.0 | 17.1 | Small |
| Pelvis and urogenital organs | 21.5 | 6.2 | 36.8 | 13.8 | 4.2 | 23.3 | Small |
| Upper extremities | 20.8 | 9.9 | 31.7 | 15.7 | 9.1 | 22.3 | Medium |
| Lower extremities | 15.1 | 5.6 | 24.6 | 8.9 | 2.9 | 14.8 | Small |
| Breast | 17.1 | 0.5 | 33.7 | 10.9 | 0.9 | 21.0 | Small |
| Skin | 26.6 | 15.6 | 37.6 | 14.4 | 7.2 | 21.6 | Medium |
| Other locations | 14.0 | 2.4 | 25.5 | 5.2 | −1.9 | 12.4 | N.A. |
| Role functioning | |||||||
| Head and Neck | 13.6 | −2.2 | 29.3 | 7.9 | −1.5 | 17.4 | N.A. |
| Chest | 18.9 | 4.3 | 33.4 | 12.8 | 3.7 | 21.8 | Small |
| Abd. and R.P.* | 15.1 | 0.7 | 29.5 | 5.7 | −3.9 | 15.3 | N.A. |
| Pelvis and urogenital organs | 25.2 | 5.3 | 45.0 | 11.0 | −2.0 | 24.0 | N.A. |
| Upper extremities | 17.3 | 3.1 | 31.5 | 10.1 | 1.1 | 19.0 | Small |
| Lower extremities | 18.0 | 5.6 | 30.3 | 9.2 | 1.1 | 17.3 | Small |
| Breast | 10.4 | −11.2 | 32.0 | −1.7 | −15.3 | 12.0 | N.A. |
| Skin | 26.0 | 11.8 | 40.3 | 9.9 | 0.1 | 19.8 | Small |
| Other locations | 10.4 | −4.7 | 25.4 | −1.1 | −10.9 | 8.6 | N.A. |
| Emotional functioning | |||||||
| Head and Neck | 0.04 | −11.9 | 12.0 | 1.5 | −5.7 | 8.7 | N.A. |
| Chest | 6.5 | −4.6 | 17.6 | 8.1 | 1.2 | 15.0 | N.A. |
| Abd. and R.P.* | 4.8 | −6.1 | 15.8 | 6.8 | −0.5 | 14.1 | N.A. |
| Pelvis and urogenital organs | 2.9 | −12.2 | 18.0 | 4.1 | −5.8 | 13.9 | N.A. |
| Upper extremities | 8.5 | −2.3 | 19.3 | 9.3 | 2.4 | 16.1 | N.A. |
| Lower extremities | 6.2 | −3.2 | 15.6 | 6.5 | 0.3 | 12.6 | N.A. |
| Breast | −1.7 | −18.1 | 14.7 | −0.5 | −10.9 | 9.9 | N.A. |
| Skin | 7.3 | −3.5 | 18.2 | 6.3 | −1.2 | 13.8 | N.A. |
| Other locations | 3.5 | −7.8 | 14.9 | 4.7 | −2.7 | 12.1 | N.A. |
| Cognitive functioning | |||||||
| Head and Neck | −3.5 | −15.3 | 8.3 | −3.0 | −10.0 | 4.1 | N.A. |
| Chest | 5.4 | −5.5 | 16.3 | 4.7 | −2.1 | 11.5 | N.A. |
| Abd. and R.P.* | 4.8 | −6.0 | 15.6 | 3.4 | −3.8 | 10.6 | N.A. |
| Pelvis and urogenital organs | −2.3 | −17.2 | 12.6 | −5.1 | −14.8 | 4.6 | N.A. |
| Upper extremities | 6.6 | −4.0 | 17.3 | 5.0 | −1.7 | 11.8 | N.A. |
| Lower extremities | 7.2 | −2.1 | 16.5 | 4.7 | −1.3 | 10.8 | N.A. |
| Breast | 4.1 | −12.1 | 20.3 | 1.3 | −8.9 | 11.5 | N.A. |
| Skin | 6.1 | −4.6 | 16.8 | −0.3 | −7.6 | 7.1 | N.A. |
| Other locations | 2.3 | −9.0 | 13.5 | 0.7 | −6.6 | 8.0 | N.A. |
| Social functioning | |||||||
| Head and Neck | 5.4 | −7.4 | 18.2 | 4.4 | −3.5 | 12.3 | N.A. |
| Chest | 9.9 | −2.0 | 21.8 | 7.7 | 0.1 | 15.3 | N.A. |
| Abd. and R.P.* | 9.4 | −2.3 | 21.2 | 6.1 | −1.9 | 14.2 | N.A. |
| Pelvis and urogenital organs | 6.2 | −10.0 | 22.4 | 0.9 | −9.9 | 11.8 | N.A. |
| Upper extremities | 11.7 | 0.1 | 23.3 | 8.7 | 1.2 | 16.3 | Small |
| Lower extremities | 10.2 | 0.1 | 20.3 | 7.0 | 0.2 | 13.8 | Small |
| Breast | 6.2 | −11.4 | 23.8 | 1.9 | −9.5 | 13.3 | N.A. |
| Skin | 14.8 | 3.2 | 26.5 | 7.2 | −1.0 | 15.5 | N.A. |
| Other locations | 6.2 | −6.1 | 18.4 | 2.1 | −6.0 | 10.3 | N.A. |
| Fatigue | |||||||
| Head and Neck | −7.2 | −21.3 | 6.9 | −5.7 | −14.0 | 2.6 | N.A. |
| Chest | −14.8 | −27.8 | −1.7 | −12.0 | −19.9 | −4.0 | Small |
| Abd. and R.P.* | −7.9 | −20.8 | 5.0 | −4.6 | −13.1 | 3.8 | N.A. |
| Pelvis and urogenital organs | −9.1 | −26.9 | 8.6 | −2.1 | −13.5 | 9.3 | N.A. |
| Upper extremities | −14.0 | −26.7 | −1.2 | −10.1 | −18.0 | −2.2 | Small |
| Lower extremities | −14.5 | −25.7 | −3.4 | −9.7 | −16.8 | −2.6 | Small |
| Breast | −2.6 | −21.9 | 16.7 | 2.5 | −9.5 | 14.5 | N.A. |
| Skin | −20.4 | −33.2 | −7.7 | −10.5 | −19.1 | −1.8 | Small |
| Other locations | −5.9 | −19.3 | 7.6 | −1.1 | −9.7 | 7.5 | N.A. |
| Nausea/vomiting | |||||||
| Head and Neck | −2.7 | −8.1 | 2.6 | −3.2 | −6.5 | 0.1 | N.A. |
| Chest | −4.0 | −8.9 | 1.0 | −4.7 | −7.9 | −1.5 | N.A. |
| Abd. and R.P.* | 0.5 | −4.4 | 5.4 | −0.6 | −4.0 | 2.8 | N.A. |
| Pelvis and urogenital organs | −4.4 | −11.1 | 2.4 | −5.5 | −10.1 | −1.0 | N.A. |
| Upper extremities | −3.9 | −8.7 | 0.9 | −4.5 | −7.7 | −1.3 | N.A. |
| Lower extremities | −3.5 | −7.7 | 0.7 | −4.0 | −6.8 | −1.1 | N.A. |
| Breast | −0.3 | −7.6 | 7.1 | −1.8 | −6.6 | 3.1 | N.A. |
| Skin | −3.4 | −8.2 | 1.5 | −3.2 | −6.7 | 0.2 | N.A. |
| Other locations | −3.1 | −8.2 | 2.0 | −3.7 | −7.1 | −0.3 | N.A. |
| Pain | |||||||
| Head and Neck | −19.5 | −34.1 | −4.8 | −17.5 | −26.3 | −8.7 | Medium |
| Chest | −20.9 | −34.5 | −7.3 | −18.0 | −26.4 | −9.6 | Medium |
| Abd. and R.P.* | −21.2 | −34.6 | −7.8 | −17.0 | −25.9 | −8.1 | Medium |
| Pelvis and urogenital organs | −19.6 | −38.1 | −1.1 | −12.4 | −24.4 | −0.4 | Small |
| Upper extremities | −24.8 | −38.1 | −11.6 | −21.5 | −29.9 | −13.1 | Large |
| Lower extremities | −19.9 | −31.5 | −8.3 | −16.1 | −23.6 | −8.5 | Medium |
| Breast | −17.7 | −37.8 | 2.4 | −13.0 | −25.6 | −0.3 | N.A. |
| Skin | −27.4 | −40.7 | −14.0 | −17.5 | −26.7 | −8.4 | Medium |
| Other locations | −17.5 | −31.4 | −3.5 | −12.9 | −22.0 | −3.9 | Small |
| Dyspnea | |||||||
| Head and Neck | −6.2 | −19.2 | 6.8 | −5.7 | −13.5 | 2.1 | N.A. |
| Chest | −5.0 | −17.1 | 7.0 | −5.1 | −12.6 | 2.4 | N.A. |
| Abd. and R.P.* | −5.5 | −17.5 | 6.4 | −6.5 | −14.4 | 1.5 | N.A. |
| Pelvis and urogenital organs | −4.2 | −20.7 | 12.2 | −3.5 | −14.2 | 7.2 | N.A. |
| Upper extremities | −8.7 | −20.5 | 3.0 | −9.1 | −16.5 | −1.7 | N.A. |
| Lower extremities | −9.0 | −19.3 | 1.2 | −7.6 | −14.3 | −1.0 | N.A. |
| Breast | 2.7 | −15.2 | 20.6 | 3.6 | −7.6 | 14.9 | N.A. |
| Skin | −10.3 | −22.2 | 1.5 | −6.3 | −14.4 | 1.8 | N.A. |
| Other locations | −8.1 | −20.6 | 4.3 | −6.6 | −14.6 | 1.5 | N.A. |
| Insomnia | |||||||
| Head and Neck | −16.1 | −32.8 | 0.6 | −15.7 | −25.8 | −5.6 | N.A. |
| Chest | −14.7 | −30.2 | 0.8 | −15.2 | −24.9 | −5.5 | N.A. |
| Abd. and R.P.* | −13.7 | −28.9 | 1.6 | −14.0 | −24.3 | −3.8 | N.A. |
| Pelvis and urogenital organs | −16.7 | −37.8 | 4.4 | −17.4 | −31.3 | −3.5 | N.A. |
| Upper extremities | −16.7 | −31.8 | −1.6 | −15.5 | −25.1 | −5.8 | Medium |
| Lower extremities | −15.6 | −28.7 | −2.4 | −13.9 | −22.5 | −5.2 | Medium |
| Breast | −11.8 | −34.8 | 11.1 | −15.2 | −29.8 | −0.6 | N.A. |
| Skin | −22.9 | −38.1 | −7.8 | −17.7 | −28.2 | −7.1 | Medium |
| Other locations | −13.3 | −29.3 | 2.7 | −11.6 | −22.0 | −1.1 | N.A. |
| Appetite Loss | |||||||
| Head and Neck | −4.1 | −13.9 | 5.6 | −3.8 | −9.8 | 2.2 | N.A. |
| Chest | −6.3 | −15.4 | 2.7 | −6.7 | −12.5 | −0.9 | N.A. |
| Abd. and R.P.* | −2.9 | −11.8 | 6.0 | −3.2 | −9.3 | 3.0 | N.A. |
| Pelvis and urogenital organs | −7.6 | −19.9 | 4.7 | −9.6 | −17.9 | −1.3 | N.A. |
| Upper extremities | −8.7 | −17.5 | 0.1 | −8.2 | −13.9 | −2.5 | N.A. |
| Lower extremities | −9.4 | −17.1 | −1.7 | −8.6 | −13.7 | −3.4 | Small |
| Breast | −1.7 | −15.1 | 11.7 | −3.3 | −12.0 | 5.4 | N.A. |
| Skin | −8.6 | −17.4 | 0.3 | −6.3 | −12.5 | −0.01 | N.A. |
| Other locations | −7.3 | −16.7 | 2.0 | −7.1 | −13.3 | −0.9 | N.A. |
| Constipation | |||||||
| Head and Neck | −3.3 | −15.0 | 8.4 | −2.8 | −9.8 | 4.3 | N.A. |
| Chest | −9.1 | −19.9 | 1.8 | −8.1 | −14.9 | −1.3 | N.A. |
| Abd. and R.P. * | −1.4 | −12.0 | 9.3 | −0.2 | −7.4 | 7.0 | N.A. |
| Pelvis and urogenital organs | −0.8 | −15.5 | 13.9 | −2.0 | −11.7 | 7.7 | N.A. |
| Upper extremities | −7.4 | −18.0 | 3.2 | −5.6 | −12.4 | 1.1 | N.A. |
| Lower extremities | −8.1 | −17.3 | 1.1 | −6.1 | −12.2 | −0.1 | N.A. |
| Breast | −1.5 | −17.4 | 14.5 | −2.7 | −12.9 | 7.6 | N.A. |
| Skin | −11.9 | −22.5 | −1.3 | −7.1 | −14.5 | 0.2 | N.A. |
| Other locations | −7.3 | −18.4 | 3.9 | −5.2 | −12.5 | 2.1 | N.A. |
| Diarrhea | |||||||
| Head and Neck | 2.7 | −6.4 | 11.8 | 3.4 | −2.1 | 9.0 | N.A. |
| Chest | −2.0 | −10.4 | 6.5 | −1.8 | −7.2 | 3.5 | N.A. |
| Abd. and R.P.* | 6.0 | −2.3 | 14.3 | 5.7 | −0.0 | 11.4 | N.A. |
| Pelvis and urogenital organs | 5.0 | −6.4 | 16.5 | 5.9 | −1.7 | 13.6 | N.A. |
| Upper extremities | −0.5 | −8.7 | 7.7 | 0.008 | −5.3 | 5.4 | N.A. |
| Lower extremities | −0.5 | −7.7 | 6.7 | 0.3 | −4.5 | 5.1 | N.A. |
| Breast | 0.1 | −12.3 | 12.4 | 0.3 | −7.8 | 8.3 | N.A. |
| Skin | −1.9 | −10.2 | 6.3 | 0.1 | −5.7 | 5.9 | N.A. |
| Other locations | 2.7 | −6.0 | 11.4 | 3.6 | −2.2 | 9.4 | N.A. |
| Financial | |||||||
| Head and Neck | 0.5 | −12.6 | 13.6 | 0.5 | −7.5 | 8.6 | N.A. |
| Chest | −10.1 | −22.3 | 2.0 | −8.9 | −16.6 | −1.2 | N.A. |
| Abd. and R.P.* | −7.6 | −19.6 | 4.4 | −5.2 | −13.3 | 3.0 | N.A. |
| Pelvis and urogenital organs | −4.7 | −21.3 | 11.8 | −1.4 | −12.4 | 9.6 | N.A. |
| Upper extremities | −9.0 | −20.8 | 2.9 | −7.0 | −14.6 | 0.7 | N.A. |
| Lower extremities | −6.3 | −16.7 | 4.0 | −3.8 | −10.7 | 3.1 | N.A. |
| Breast | −0.3 | −18.3 | 17.7 | 4.3 | −7.3 | 15.9 | N.A. |
| Skin | −10.7 | −22.6 | 1.2 | −5.9 | −14.3 | 2.4 | N.A. |
| Other locations | −3.5 | −16.0 | 9.0 | −1.1 | −9.3 | 7.2 | N.A. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Eck, I.; den Hollander, D.; Desar, I.M.E.; Soomers, V.L.M.N.; van de Sande, M.A.J.; de Haan, J.J.; Verhoef, C.; Vriens, I.J.H.; Bonenkamp, J.J.; van der Graaf, W.T.A.; et al. Unraveling the Heterogeneity of Sarcoma Survivors’ Health-Related Quality of Life Regarding Primary Sarcoma Location: Results from the SURVSARC Study. Cancers 2020, 12, 3083. https://doi.org/10.3390/cancers12113083
van Eck I, den Hollander D, Desar IME, Soomers VLMN, van de Sande MAJ, de Haan JJ, Verhoef C, Vriens IJH, Bonenkamp JJ, van der Graaf WTA, et al. Unraveling the Heterogeneity of Sarcoma Survivors’ Health-Related Quality of Life Regarding Primary Sarcoma Location: Results from the SURVSARC Study. Cancers. 2020; 12(11):3083. https://doi.org/10.3390/cancers12113083
Chicago/Turabian Stylevan Eck, Ilse, Dide den Hollander, Ingrid M.E. Desar, Vicky L.M.N. Soomers, Michiel A.J. van de Sande, Jacco J. de Haan, Cornelis Verhoef, Ingeborg J.H. Vriens, Johannes J. Bonenkamp, Winette T.A. van der Graaf, and et al. 2020. "Unraveling the Heterogeneity of Sarcoma Survivors’ Health-Related Quality of Life Regarding Primary Sarcoma Location: Results from the SURVSARC Study" Cancers 12, no. 11: 3083. https://doi.org/10.3390/cancers12113083