Uncommon Site of Metastasis and Prolonged Survival in Patients with Anaplastic Thyroid Carcinoma: A Systematic Review of the Literature

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
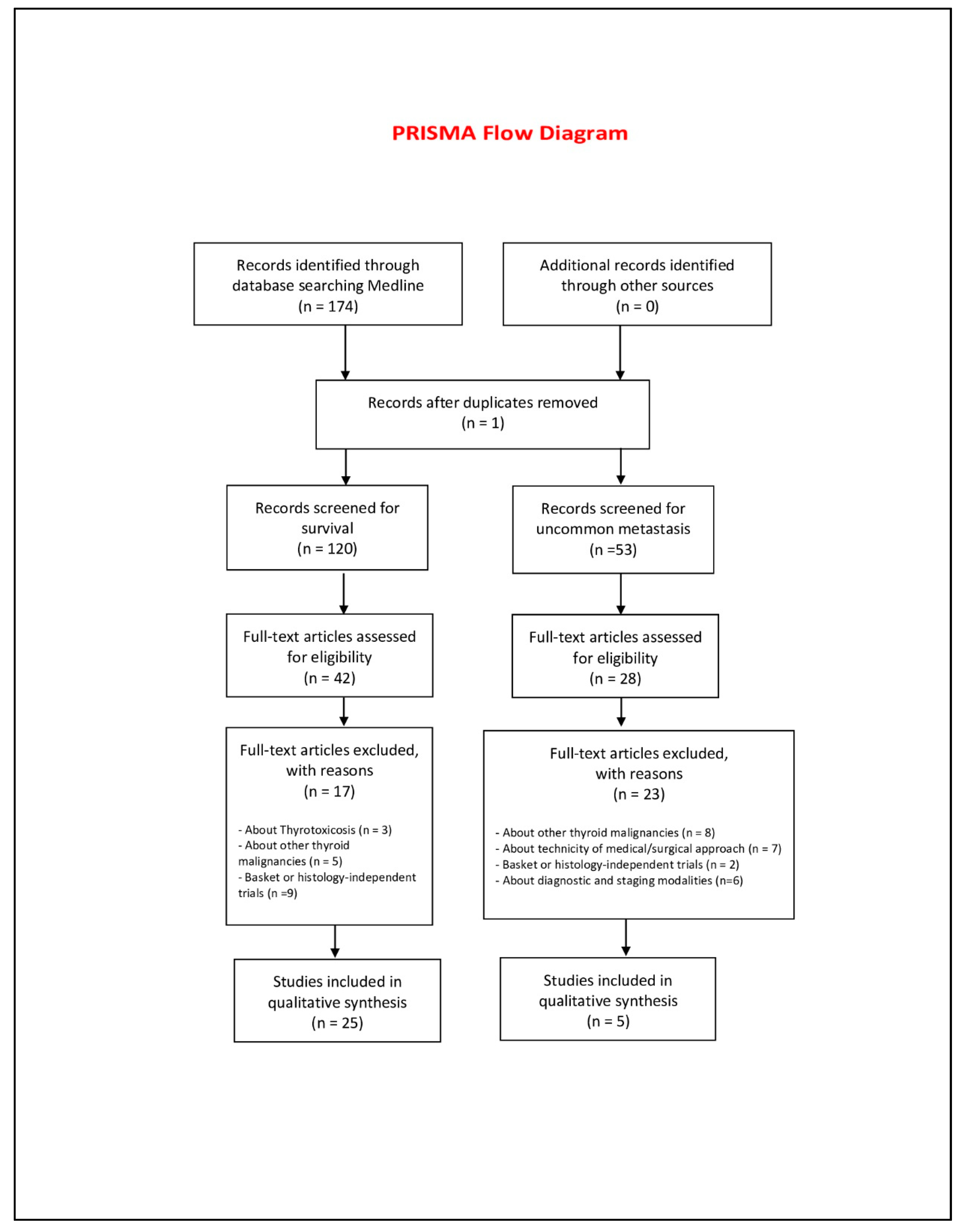
2. Methods
- Full text papers;
- Available abstracts;
- Papers written in English;
- Clinical studies, reviews and case reports related to a prolonged survival compared to the literature data;
- Clinical studies, reviews and case reports related to uncommon sites of metastasis compared to the literature data;
- Clinical studies, reviews and case reports on survival prognostic and predictive factors.
- Pediatric or pregnancy patients;
- Interim reports;
- About differentiated thyroid carcinomas;
- Non-anaplastic thyroid carcinomas;
- Molecular studies;
- Preclinical studies;
- Non-English written language;
- No full text;
- Non uncommon site of metastasis;
- Management of ATC.
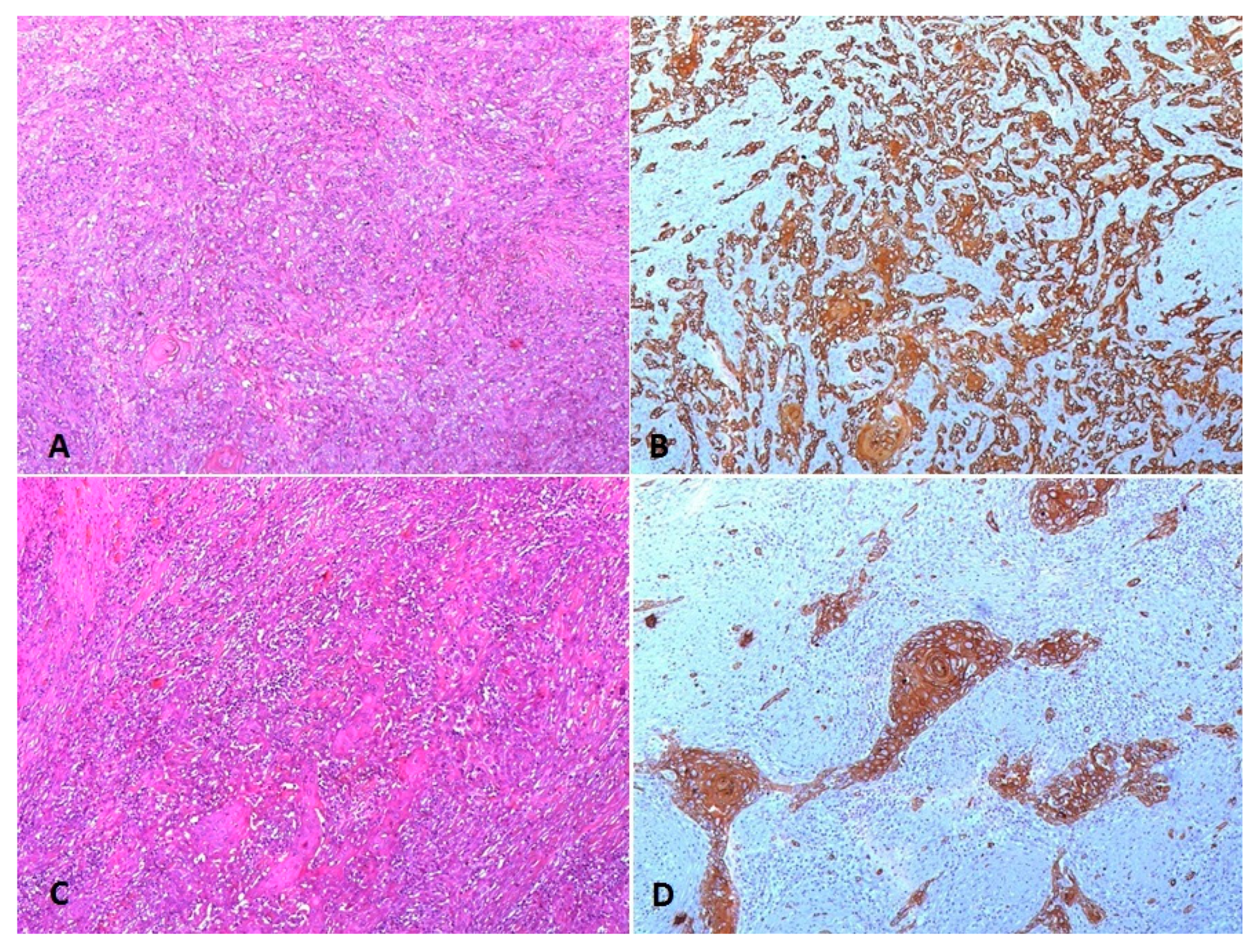
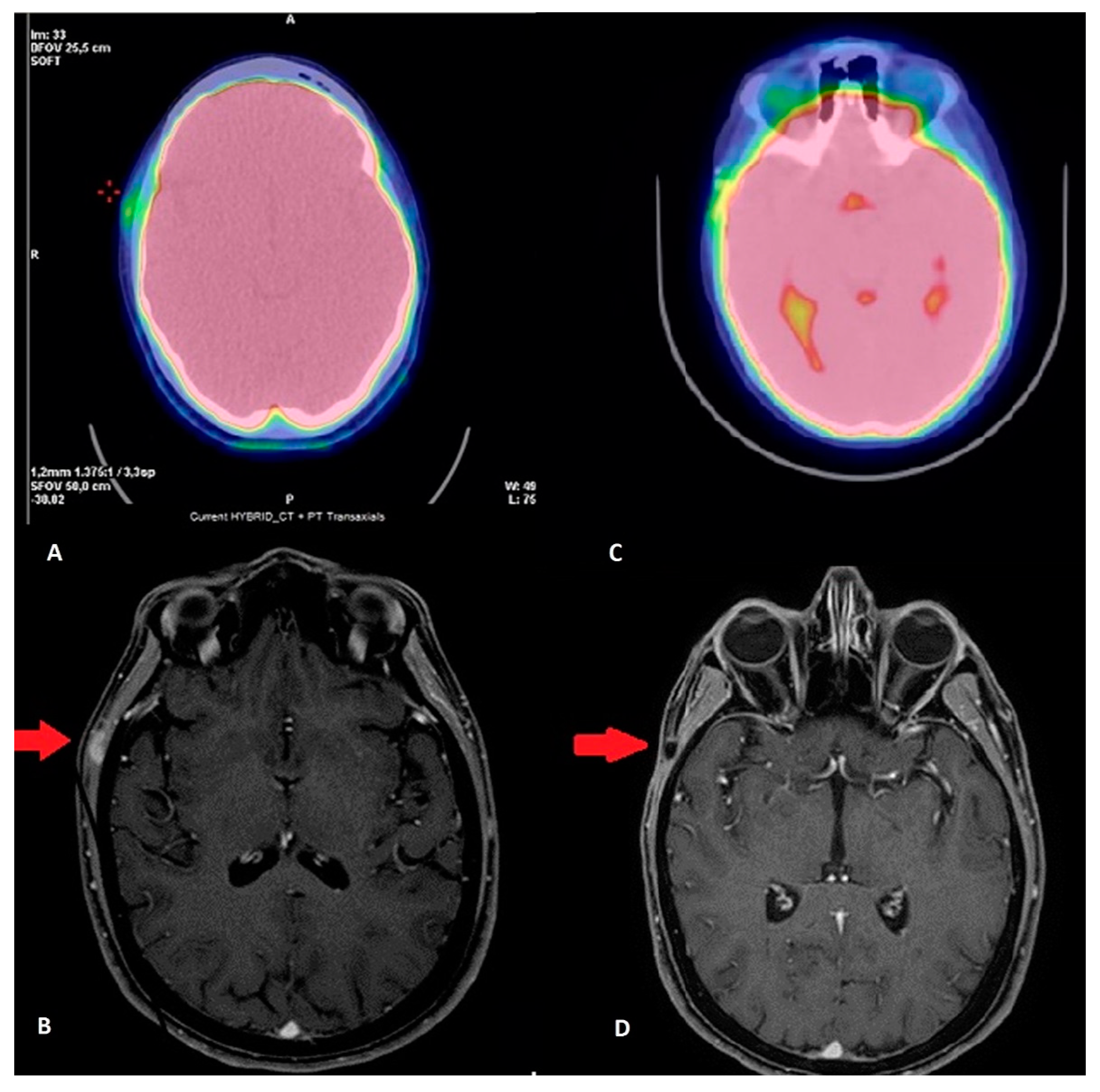
Case Description
3. Results
3.1. Prognostic Factors
3.2. Unusual Metastatic Sites
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gilliland, F.D.; Hunt, W.C.; Morris, D.M.; Key, C.R. Prognostic factors for thyroid carcinoma. A population-based study of 15698 cases from the Surveillance, epidemiology and end results (SEER) program 1973–1991. Cancer 1997, 79, 564–573. [Google Scholar] [CrossRef]
- Are, C.; Shaha, A.R. Anaplastic thyroid carcinoma: Biology, pathogenesis, prognostic factors and treatment approaches. Ann. Surg. Oncol. 2006, 13, 453–464. [Google Scholar] [CrossRef]
- Leonhardt, J.M.; Heymann, W.R. Thyroid disease and the skin. Derm. Clin. 2002, 20, 473–481. [Google Scholar] [CrossRef]
- Sun, X.S.; Sun, S.R.; Guevara, N.; Fakhry, N.; Marcy, P.Y.; Lassalle, S.; Peyrottes, I.; Bensadoun, R.J.; Lacout, A.; Santini, J.; et al. Chemoradiation in anaplastic thyroid carcinomas. Crit. Rev. Oncol. Hematol. 2013, 86, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Giuffrida, D.; Gharib, H. Anaplastic thyroid carcinoma: Current diagnosis and treatment. Ann. Oncol. 2000, 11, 1083–1090. [Google Scholar] [CrossRef]
- Besic, N.; Gazic, N. Sites of metastases of anaplastic thyroid carcinoma: Autopsy findings in 45 cases from a single institution. Thyroid 2013, 23, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Giordano, L.; Pilolli, F.; Toma, S.; Bussi, M. Parapharyngeal metastases from thyroid cancer: Surgical management of two cases with minimally-invasive video-assisted technique. Acta. Otolaryngol Ital. 2015, 35, 289–292. [Google Scholar]
- Dahl, P.R.; Brodland, D.G.; Goellner, J.R.; Hay, D. Thyroid carcinoma metastatic to the skin: A cutaneous manifestation of a widely disseminated malignancy. J. Am. Acad. Derm. 1997, 36, 1045–1050. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; the PRISMA-DTA Group. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The prisma-DTA statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Stenman, A.; Hellgren, L.S.; Jatta, K.; Hysek, M.; Zemmler, M.; Altena, R.; Nilsson, I.-L.; Bränström, R.; Zedenius, J.; Christofer Juhlin, C. Metastatic Anaplastic Thyroid Carcinoma in Complete Remission: Morphological, molecular, and clinical work-up of a rare case. Endocr. Pathol. 2020, 31, 77–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanazawa, S.; Kammori, M. Case report: 84-month disease-free survival after surgery for anaplastic thyroid carcinoma. J. Nippon. Med. Sch. 2019, 86, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Uğurlu, M.Ü.; Seven, İ.E.; Eren, F.; Yeğen, C.; Güllüoğlu, B.M. Minimally invasive thyroid anaplastic carcinoma with long survival. Turk. J. Surg. 2018, 34, 319–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Y.; Matsuzuka, F.; Yoshida, H.; Morita, S.; Nakano, K.; Kobayashi, K.; Yokozawa, T.; Hirai, K.; Kakudo, K.; Kuma, K.; et al. Encapsulated anaplastic thyroid carcinoma without invasive phenotype with favorable prognosis: Report of a case. Surg. Today 2003, 33, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Dibelius, G.; Mehra, S.; Clain, J.B.; Urken, M.L.; Wenig, B.M. Noninvasive anaplastic thyroid carcinoma: Report of a case and literature review. Thyroid 2014, 24, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Lowe, N.M.; Loughran, S.; Slevin, N.J.; Yap, B.K. Anaplastic thyroid cancer: The addition of systemic chemotherapy to radiotherapy led to an observed improvement in survival-a single centre experience and review of the literature. Sci. World J. 2014, 674583. [Google Scholar] [CrossRef]
- Siironen, P.; Hagström, J.; Mäenpää, H.O. Anaplastic and poorly differentiated thyroid carcinoma: Therapeutic strategies and treatment outcome of 52 consecutive patients. Oncology 2010, 79, 400–408. [Google Scholar] [CrossRef]
- Kurukahvecioglu, O.; Ege, B.; Poyraz, A.; Tezel, E.; Taneri, F. Anaplastic thyroid carcinoma with long term survival after combined treatment: Case report. Endocr. Regul. 2007, 41, 41–44. [Google Scholar]
- Busnardo, B.; Daniele, O.; Pelizzo, M.R.; Nacamulli, D.; DeVido, D.; Mian, C.; Girelli, M.E. A multimodality therapeutic approach in anaplastic thyroid carcinoma: Study on 39 patients. J. Endocrinol. Invest. 2000, 23, 755–761. [Google Scholar] [CrossRef]
- Derbel, O.; Limem, S.; Segura-Ferlay, C.; Lifante, J.F.; Car-Rie, C.; Peix, J.L.; Borson-Chazot, F.; Bournaud, C.; Droz, J.P.; De la Fouchardiere, C. Results of combined treatment of anaplastic thyroid carcinoma (ATC) BMC. Cancer 2011, 11, 469. [Google Scholar]
- Haddad, R.I.; Lydiatt, W.M.; Ball, D.W.; Busaidy, N.L.; Byrd, D.; Callender, G. Anaplastic thyroid carcinoma, version 2. J. Natl. Compr. Canc. Netw. 2015, 13, 1140–1150. [Google Scholar] [CrossRef] [Green Version]
- Liu, A.H.; Juan, L.Y.; Yang, A.H.; Chen, H.S.; Lin, H.D. Anaplastic thyroid cancer with uncommon long-term survival. J. Chin. Med. Assoc. 2006, 69, 489–491. [Google Scholar] [CrossRef] [Green Version]
- Dumke, A.K.; Pelz, T.; Vordermark, D. Long-term results of radiotherapy in anaplastic thyroid cancer. Radiat. Oncol. 2014, 9, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guimaraes, L.; Meneses, A.; Carrara, W.; Kefalas, A. Encapsulated anaplastic thyroid carcinoma with three-year disease-free survival. Pathol. Res. Pract. 2000, 196, 867–870. [Google Scholar] [CrossRef]
- Yau, T.; Lo, C.Y.; Epstein, R.J.; Lam, A.K.; Wan, K.Y.; Lang, B.H. Treatment outcomes in anaplastic thyroid carcino- ma: Survival improvement in young patients with localized disease treated by combination of surgery and radiotherapy. Ann. Surg. Oncol. 2008, 15, 2500–2505. [Google Scholar] [CrossRef] [PubMed]
- De Crevoiser, R.; Baudin, E.; Bachelot, A.; Leboulleux, S.; Travagli, J.P.; Caillou, B.; Schlumberger, M. Com- bined treatment of anaplastic thyroid carcinoma with surgery, chemotherapy, and hyperfractionat-ed accelerated external radiotherapy. Int. J. Radiat. Biol. Phys. 2004, 60, 1137–1143. [Google Scholar] [CrossRef]
- Swaak-Kragten, A.T.; De Wilt, J.H.; Schmitz, P.I.; Bon-Tenbal, M.; Levendag, P.C. Multimodality treatment for anaplastic thyroid carcinoma-treatment outcome in 75 patients. Radiother Oncol. 2009, 92, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Sherman, J.E.; Lim, S.H.; Ghossein, R.A.; Matthew, G.F.; Sha-ha, A.R.; Rivera, M.; Lin, O.; Wolden, S.; Lee, N.Y.; Pfister, D.G. Concurrent doxorubicin and radiotherapy for anaplastic thyroid cancer: A critical re-evaluation including uniform pathologic review radiother. Radiother. Oncol. 2011, 101, 425–430. [Google Scholar] [CrossRef]
- Liu, T.R.; Xiao, Z.-W.; Xu, H.-N.; Long, Z.; Wei, F.-Q.; Zhuang, S.-M.; Sun, X.-M.; Yang, A.-K.; Zhang, G.-P.; Fan, Y.; et al. Treatment and prognosis of anaplastic thyroid carcinoma: A clinical study of 50 cases. PLoS ONE 2016, 11, e0164840. [Google Scholar] [CrossRef]
- Brignardello, E.; Palestini, N.; Felicetti, F.; Castiglione, A.; Piovesan, A.; Gallo, M.; Freddi, M.; Ricardi, U.; Gasparri, G.; Ciccone, G.; et al. Early surgery and survival of patients with anaplastic thyroid carcinoma: Analysis of a case series referred to a single institution between 1999 and 2012. Thyroid 2014, 24, 1600–1606. [Google Scholar] [CrossRef]
- Sun, C.; Li, Q.; Hu, Z.; He, J.; Li, C.; Li, G.; Tao, X.; Yang, A. Treatment and prognosis of anaplastic thyroid carcinoma: Experience from a single institution in China. PLoS ONE 2013, 8, e80011. [Google Scholar]
- Palestini, N.; Brignardello, E.; Freddi, M. Surgical treatment of anaplastic thyroid carcinoma. Our experience. G. Chir. 2010, 31, 282–285. [Google Scholar] [PubMed]
- Roche, B.; Larroumets, G.; Dejax, C.; Kwiatkowsi, F.; Desbiez, F.; Thieblot, P.; Tauveron, I. Epidemiology, clinical presentation, treatment and prognosis of a regional series of 26 anaplastic thyroid carcinomas (ATC). Comparison with the literature. Ann. Endocrinol (Paris) 2010, 71, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.K.; Lee, M.C.; Hah, J.H.; Ahn, S.-H.; Son, Y.-I.; Rho, Y.-S.; Chung, P.-S.; Lee, Y.-S.; Koo, B.S.; Rho, Y.-S.; et al. Role of surgery in the management of anaplastic thyroid carcinoma: Korean nationwide multicenter study of 329 patients with anaplastic thyroid carcinoma, 2000 to 2012. Head Neck. 2017, 39, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Sugitani, I.; Kasai, N.; Fujimoto, Y.; Yanagisawa, A. Prognostic factors and therapeutic strategy for anaplastic carcinoma of the thyroid. World J. Surg. 2001, 25, 617–622. [Google Scholar] [CrossRef]
- Sugitani, I.; Miyauchi, A.; Sugino, K.; Okamoto, T.; Yoshida, A.; Suzuki, S. Prognostic factors and treatment outcomes for anaplastic thyroid carcinoma. ATC Research Consortium of Japan cohort study of 677 patients. World J. Surg. 2012, 36, 1247–1254. [Google Scholar] [CrossRef]
- Sugitani, I.; Onoda, N.; Ito, K.I.; Suzuki, S. Management of anaplastic thyroid carcinoma: The fruits from ATC research consortium of Japan. J. Nippon. Med. Sch. 2018, 85, 18–27. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.N.; Zafereo, M.; Dadu, R.; Busaidy, N.L.; Hess, K.; Cote, G.J.; Williams, M.D.; William, W.N.; Sandulache, V.; Gross, N.; et al. Patterns of treatment failure in anaplastic thyroid carcinoma. Thyroid 2017, 27, 672–681. [Google Scholar] [CrossRef]
- Kebebew, E.; Greenspan, F.S.; Clark, O.H.; Woeber, K.A.; McMillan, A. Anaplastic thyroid carcinoma. Treatment outcome and prognostic factors. Cancer 2005, 103, 1330–1335. [Google Scholar] [CrossRef]
- Kim, T.Y.; Kim, K.W.; Jung, T.S.; Kim, J.M.; Kim, S.W.; Chung, K.; Kim, E.Y.; Gong, G.; Oh, Y.L.; Yi, K.H.; et al. Prognostic factors for Korean patients with anaplastic thyroid carcinoma. Head Neck. 2007, 29, 765–772. [Google Scholar] [CrossRef]
- Qiu, B.; Li, H.-Q.; Chang, Q.-G.; De Yin, T. Nomograms predict survival in patients with anaplastic thyroid carcinoma. Med. Sci. Monit. 2019, 25, 8447–8556. [Google Scholar] [CrossRef]
- Smallridge, R.C.; Ain, K.B.; Asa, S.L.; Bible, K.C.; Brierley, J.D.; Burman, K.D.; Kebebew, E.; Lee, N.Y.; Nikiforov, Y.E.; Shaha, A.R.; et al. American thyroid association guidelines for management of patients with anaplastic thyroid cancer. Thyroid 2012, 22, 1104–1139. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Leeper, R.D. Treatment of locally advanced thyroid carcinoma with combination doxorubicin and radiation therapy. Cancer 1987, 60, 2372–2375. [Google Scholar] [CrossRef]
- Perri, F.; Di Lorenzo, G.; Della Vittoria Scarpati, G.; Buonerba, C. Anaplastic thyroid carcinoma: A com- prehensive review of current and future therapeutic options. World J. Clin. Oncol. 2011, 10, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Xia, Q.; Wang, W.; Xu, J.; Chen, X.; Zhong, Z.; Sun, C. Evidence from an updated meta-analysis of the prognostic impacts of postoperative radiotherapy and chemotherapy in patients with anaplastic thyroid carcinoma. Onco Targets Ther. 2018, 11, 2251–2257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salehian, B.; Liem, S.Y.; Mojazi Amiri, H.; Maghami, E. Clinical trials in management of anaplastic thyroid carcinoma; progressions and set backs: A systematic review. Int. J. Endocrinol Metab. 2019, 17, e67759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirokawa, M.; Sugitani, I.; Kakudo, K.; Sakamoto, A.; Higashiyama, T.; Sugino, K.; Toda, K.; Ogasawara, S.; Yoshimoto, S.; Hasegawaet, Y.; et al. Histopathological analysis of anaplastic thyroid carcinoma cases with long-term survival: A report from the anaplastic thyroid carcinoma research consortium of Japan. Endocr. J. 2016, 63, 441–447. [Google Scholar] [CrossRef]
- Goutas, N.; Vlachodimitropoulos, D.; Bouka, M.; Lazaris, A.C.; Nasioulas, G.; Gazouli, M. BRAF and K-RAS mutation in a Greek papillary and medullary thyroid carcinoma cohort. Anticancer Res. 2008, 28, 305–308. [Google Scholar]
- Kim, S.K.; Song, K.H.; Lim, S.D.; Lim, Y.C.; Yoo, Y.B.; Kim, J.S.; Hwang, T.S. Clinical and pathological features and the BRAF (V600E) mutation in patients with papillary thyroid carcinoma with and without concurrent Hashimoto thyroiditis. Thyroid 2009, 19, 137–141. [Google Scholar] [CrossRef]
- Landa, I.; Ibrahimpasic, T.; Boucai, L.; Sinha, R.; Knauf, J.A.; Shah, R.H.; Dogan, S.; Ricarte-Filho, J.C.; Krishnamoorthy, G.P.; Xu, B.; et al. Genomic and transcriptomic hallmarks of poorly differentiated and anaplastic thyroid cancers. J. Clin. Invest. 2016, 126, 1052–1066. [Google Scholar] [CrossRef] [Green Version]
- Ubertini, V.; Norelli, G.; D’Arcangelo, D.; Gurtner, A.; Cesareo, E.; Baldari, S.; Gentileschi, M.P.; Piaggio, G.; Nistico, P.; Soddu, S.; et al. Mutant p53 gains new function in promoting inflammatory signals by repression of the secreted interleukin-1 receptor antagonist. Oncogene. 2015, 34, 2493–2504. [Google Scholar] [CrossRef]
- Song, Y.S.; Jung, C.K.; Jung, K.C.; Park, Y.J.; Won, J.K. Rare manifestations of anaplastic thyroid Carcinoma: The role of BRAF Mutation Analysis. J. Korean Med. Sci. 2017, 32, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; Zafereo, M.; Williams, M.D.; Ferrarotto, R.; Dadu, R.; Gross, N.; Brandon Gunn, G.; Skinner, H.; Cote, G.; Grosu, H.B.; et al. Recent advances and emerging therapies in anaplastic thyroid carcinoma version 1. Rencent Adv. Emerg. Ther. Anaplastic Thyroid. Carcinoma 2018, 7. [Google Scholar] [CrossRef]
- Altinay, S.; Taş, B.; Ozen, A.; Süt, P.A. Anaplastic thyroid carcinoma with diffuse thoracic skin metastasis: A case report. Oncol Lett. 2014, 7, 1767–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danialan, R.; Tetzlaff, M.T.; Torres-Cabala, C.A.; Mays, S.R.; Prieto, V.G.; Bell, D.; Curry, J.L. Cutaneous metastasis from anaplastic thyroid carcinoma exhibiting exclusively a spindle cell morphology. A case report and review of literature. J. Cutan. Pathol. 2016, 43, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, T.; Sahin, S.B.; Sahin, O.Z.; Akdogan, R.; Gücer, R. Anaplastic thyroid carcinoma presenting with gastric metastasis: A case report. Hippokratia 2015, 19, 85–87. [Google Scholar]
- Lim, K.H.; Lee, K.W.; Kim, J.H.; Park, S.Y.; Choi, S.H.; Lee, J.S. Anaplastic thyroid carcinoma initially presented with abdominal cutaneous mass and hyperthyroidism. Korean J. Intern. Med. 2010, 25, 450–453. [Google Scholar] [CrossRef]
- Hassan, M.; Janjua, T.K.; Afridi, H.K.; Zahid, N.A. Anaplastic carcinoma of thyroid gland with widespread soft tissue metastasis: An unusual presentation. BMJ Case Rep. 2017. [Google Scholar] [CrossRef]
- Agaiah, G.; Hossain, A.; Mooney, C.J.; Parmentier, J.; Remick, S.C. Anaplastic thyroid cancer: A review of epidemiology, pathogenesis, and treatment. J. Oncol. 2011. [Google Scholar] [CrossRef]
- Forbes, S.A.; Beare, D.; Gunasekaran, P. COSMIC: Exploring the world’s knowledge of somatic mutations in human cancer. Nucleic Acids Res. 2015, 43, D805–D811. [Google Scholar] [CrossRef]
- Volante, M.; Rapa, I.; Gandhi, M.; Bussolati, G.; Giachino, D.; Papotti, M.; Nikiforov, Y.E. RAS Mutations are the predominant molecular alteration in poorly differentiated thyroid carcinomas and bear prognostic impact. Clin. Endocrinol. Metab. 2009, 94, 4735–4741. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Articles | Stage | Treatment | Evidence | Risk Factors | Median Survival |
|---|---|---|---|---|---|
| Stenman (2020) [10] | Locally advanced | CT/RT->CH | Case Report | BRAF neg, P53 pos, PDL1 80%, Ki67 30% | 12 mos |
| Kanazawa (2019) [11] | Locally advanced | CH->RT and Radioactive Iodine | Case Report | Ki 67 < 30%, PI = 0 | 84 mos |
| Uğurlu (2018) [12] | Early | CH->RT | Case Report | No (encapsulated and early stage) | 72 mos |
| Ito (2003) [13] | T4aN0 | CH | Case Report | No (encapsulated) | 57 mos |
| Dibelius (2014) [14] | Early | CH | Case Report | No (Not invasive) | 14 mos |
| Lowe (2014) [15] | Local/locoregional and M+ | Multimodality | Retrospective (20 pts) | Various | 6 mos (range 1–11 mos) |
| Siironen (2010) [16] | Local/locoregional and M+ | Multimodality | Retrospective (44 pts) | Various | 11.6 mos |
| Kurukahvecioglu (2007) [17] | Locally advanced | CH | Case Report | P53 and Ki 67 pos, soft tissue involvement | 36 mos |
| Busnardo (2000) [18] | Local/locoregional and M+ | Multimodality | Retrospective (39 pts) | Various | 5.7 mos |
| Derbel (2011) [19] | Local/locoregional and M+ | Multimodality | Retrospective (44 pts) | Various | 8 mos |
| Haddad (2005) [20] | Locally advanced | CH->CT/RT | Case Report | Extracapsular, positive margins | 24 mos |
| Liu (2006) [21] | Locally advanced | CH | Case Report | Extracapsular | 240 mos |
| Dumke (2014) [22] | Local or locoregional | Multimodality | Retrospective (40 pts) | Various | 10.5 mos |
| Guimaraes (2000) [23] | Early | CH | Case Report | Extracapsular foci of ATC | 35 mos |
| Sugitani (2001–2012–2018) [10,11,12] | Local/locoregional and M+ | Multimodality | Retrospective (47 pts) | Positive/Negative risk factors | >6 mos/<6 mos |
| Yau (2008) [24] | Locally advanced | CH-> RT | Retrospective (50 pts) | <65 y, N0, M0, papillary carcinoma | 3 mos (rage 4 days–16 years) |
| De Crevoisier (2004) [25] | Locoregional and M+ | Multimodality | Retrospective (30 pts) | Various | 10 mos |
| Swaak-Kragten (2009) [26] | Local/locoregional and M+ | Multimodality | Retrospective (75 pts) | Various | 2.9 mos (0–119 mos) |
| Sherman (2011) [27] | Local/locoregional | Multimodality | Retrospective (37 pts) | Various | 6 mos |
| Liu (2016) [28] | Local/locoregional and M+ | Multimodality | Retrospective (50 pts) | Various | 24 mos (range 24–48 mos) |
| Brignardello (2014) [29] | Local/locoregional | Multimodality | Retrospective (55 pts) | Various | 6.57 mos |
| Sun (2013) [30] | Local/locoregional and M+ | Multimodality | Retrospective (60 pts) | Various | 8 mos |
| Palestini (2010) [31] | Local/locoregional and M+ | Multimodality | Retrospective (20 pts) | Various | 8 mos (range 3–28 mos) |
| Roche (2010) [32] | Local/locoregional and M+ | Multimodality | Retrospective (26 pts) | Various | 4 mos |
| Baek (2017) [33] | Local/locoregional and M+ | Multimodality | Retrospective (329 pts) | Various | 8 mos |
| Articles | Age | Stage | M+ | Treatment | Evidence | Risk Factors | Survival |
|---|---|---|---|---|---|---|---|
| Danialan (2016) [54] | 65 y | Locally advanced | Lung skin | CH->RT/CT+ Pazopanib+ target therapy | Case Report | BRAF pos | 9 mos |
| Altinay (2014) [53] | 57 y | Advanced | Subcarinal, paratracheal, aortopulmonary, trachea-bronchial and mediastinal->skin | CT | Case Report | ND | 1 mo |
| Ayaz (2015) [55] | 72 y | Advanced | Lung skin gastric | / | Case Report | ND | 1 mo |
| Lim (2010) [56] | 63 y | Advanced | Skin | CT/RT | Case Report | ND | 2 mos |
| Hassan (2017) [57] | 62 y | Advanced | Soft tissue | / | Case Report | ND | 1 mo |
| Prognostic Factors | ||
|---|---|---|
| Favorable | Our Patient’s Prognostic Factors | References |
| Coexisting well differentiated carcinoma | X | Salehian (2019) [45] Hirokawa (2016) [46] Dumke (2014) [22] Sugitani (2012) [35] Rao (2017) [37] Kebebew (2005) [38] Kim (2007) [39] |
| Radical surgery | X | Baek (2017) [33] Yau (2008) [24] |
| Tumor size < 6 cm | X | Yau (2008) [24] |
| Age < 70aa | X | Baek (2017) [33] Sherman (2011) [27] |
| Female gender | X | Sugitani (2012–2018) [35,36] Sherman (2011) [27] |
| Leucocyte blood count < 10 × 109 | X | Sun (2013) [30] |
| Platelet count < 300 ×109 | X | Sun (2013) [30] |
| No nodal involvement | X | Sugitani (2012–2018) [35,36] |
| Squamous cell carcinoma components | Salehian (2019) [45] Hirokawa (2016) [46] Dumke (2014) [22] | |
| Concomitant chemo-radiotherapy | X | Baek (2017) [33] Kim (1987) [42] Perri (2011) [43] Derbel (2011) [19] De Crevoiser (2004) [25] Swaak-Kragten (2009) [26] Liu (2016) [28] Xia (2018) [44] Salehian (2019) [45] |
| Radiotherapy > 60 Gy | X | Sherman (2011) [27] |
| Unfavorable | ||
| Acute symptoms | Sugitani (2001) [34] | |
| Rapid tumor growth | X | Sugitani (2012) [35] Rao (2017) [37] Kebebew (2005) [38] Kim (2007) [39] |
| Distant metastasis | X | Sugitani (2001) [34] Baek (2017) [33] |
| Age > 60 y.o. | X | Baek (2017) [33] |
| Extrathyroidal invasion | X | Baek (2017) [33] |
| Giant cell and pleomorphic pattern | Baek (2017) [33] | |
| Capsular invasion | X | Uğurlu,(2018) [12] |
| Lymphocytic and neutrophilic infiltration | X | Salehian (2019) [45] Hirokawa (2016) [46] Dumke (2014) [22] |
| TP53 mutation | Rao (2017) [37] Ubertini (2015) [50] | |
| RAS mutation | X | Volante (2009) [60] Landa (2016) [37] |
| BRAF mutation | Landa (2016) [49] | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirabile, A.; Biafora, M.; Giordano, L.; Arrigoni, G.; Cangi, M.G.; Dell’Oca, I.; Lira Luce, F.; Di Santo, D.; Galli, A.; Tulli, M.; et al. Uncommon Site of Metastasis and Prolonged Survival in Patients with Anaplastic Thyroid Carcinoma: A Systematic Review of the Literature. Cancers 2020, 12, 2585. https://doi.org/10.3390/cancers12092585
Mirabile A, Biafora M, Giordano L, Arrigoni G, Cangi MG, Dell’Oca I, Lira Luce F, Di Santo D, Galli A, Tulli M, et al. Uncommon Site of Metastasis and Prolonged Survival in Patients with Anaplastic Thyroid Carcinoma: A Systematic Review of the Literature. Cancers. 2020; 12(9):2585. https://doi.org/10.3390/cancers12092585
Chicago/Turabian StyleMirabile, Aurora, Matteo Biafora, Leone Giordano, Gianluigi Arrigoni, Maria Giulia Cangi, Italo Dell’Oca, Francesca Lira Luce, Davide Di Santo, Andrea Galli, Michele Tulli, and et al. 2020. "Uncommon Site of Metastasis and Prolonged Survival in Patients with Anaplastic Thyroid Carcinoma: A Systematic Review of the Literature" Cancers 12, no. 9: 2585. https://doi.org/10.3390/cancers12092585