PKM2 Expression as Biomarker for Resistance to Oxaliplatin-Based Chemotherapy in Colorectal Cancer

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics and Clinico-Pathological Features
2.2. PKM2 mRNA Expression in Different CRC groups, Adenomas, and Normal Mucosa
2.3. PKM2 mRNA Expression in Different Groups and Correlations with Clinico-Pathological Features and Analysed Markers
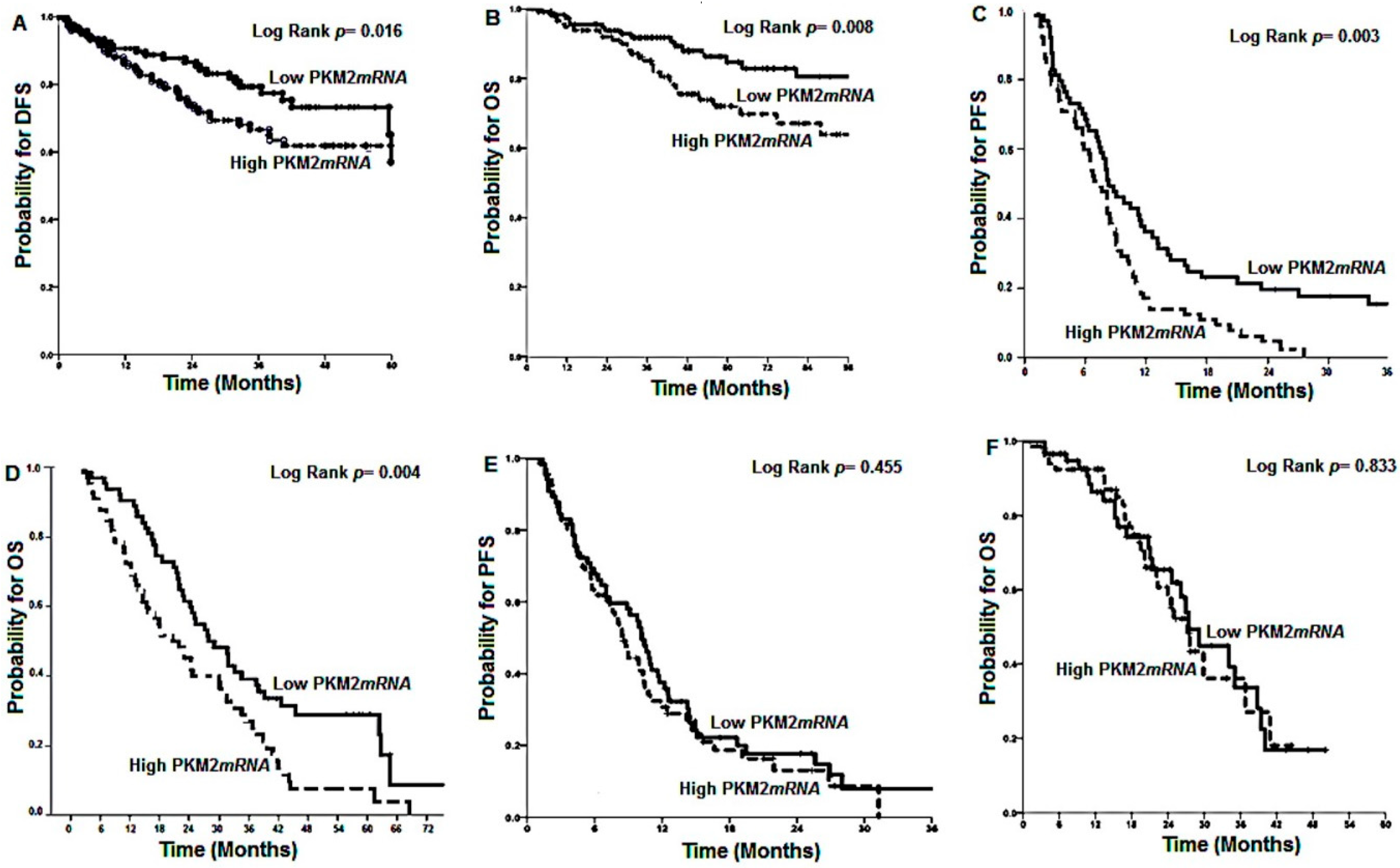
2.4. Patients’ Outcome According to PKM2 mRNA Expression
2.5. Multivariate and Univariate Analysis
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- References Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzmaurice, C.; Akinyemiju, T.F.; Al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: A systematic analysis for the global burden of disease study. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar] [PubMed]
- Labianca, R.; Nordlinger, B.; Beretta, G.D.; Mosconi, S.; Mandala, M.; Cervantes, A.; Arnold, D. Early colon cancer: Esmo clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24 (Suppl. 6), vi64–vi72. [Google Scholar] [CrossRef] [PubMed]
- Vogelstein, B.; Kinzler, K.W. Cancer genes and the pathways they control. Nat. Med. 2004, 10, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.D.; Parsons, D.W.; Jones, S.; Lin, J.; Sjoblom, T.; Leary, R.J.; Shen, D.; Boca, S.M.; Barber, T.; Ptak, J.; et al. The genomic landscapes of human breast and colorectal cancers. Science 2007, 318, 1108–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, L.A., Jr.; Le, D.T. Pd-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 373, 1979. [Google Scholar] [PubMed]
- Christofk, H.R.; Vander Heiden, M.G.; Harris, M.H.; Ramanathan, A.; Gerszten, R.E.; Wei, R.; Fleming, M.D.; Schreiber, S.L.; Cantley, L.C. The m2 splice isoform of pyruvate kinase is important for cancer metabolism and tumour growth. Nature 2008, 452, 230–233. [Google Scholar] [CrossRef]
- Dayton, T.L.; Jacks, T.; Vander Heiden, M.G. Pkm2, cancer metabolism, and the road ahead. EMBO Rep. 2016, 17, 1721–1730. [Google Scholar] [CrossRef] [Green Version]
- Liberti, M.V.; Locasale, J.W. The warburg effect: How does it benefit cancer cells? Trends Biochem. Sci. 2016, 41, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.F.; Li, X.B.; Sun, H.; Zhang, B.; Han, Y.S.; Jiang, Y.; Zhuang, Q.L.; Fang, J.; Wu, G.H. Pyruvate kinase type m2 is upregulated in colorectal cancer and promotes proliferation and migration of colon cancer cells. IUBMB Life 2012, 64, 775–782. [Google Scholar] [CrossRef]
- Zhu, H.; Wu, J.; Zhang, W.; Luo, H.; Shen, Z.; Cheng, H.; Zhu, X. Pkm2 enhances chemosensitivity to cisplatin through interaction with the mtor pathway in cervical cancer. Sci. Rep. 2016, 6, 30788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adem, S.; Comakli, V.; Uzun, N. Pyruvate kinase activators as a therapy target: A patent review 2011–2017. Expert Opin. Ther. Pat. 2018, 28, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Dong, G.; Mao, Q.; Xia, W.; Xu, Y.; Wang, J.; Xu, L.; Jiang, F. Pkm2 and cancer: The function of pkm2 beyond glycolysis. Oncol. Lett. 2016, 11, 1980–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.; Xia, Y.; Ji, H.; Zheng, Y.; Liang, J.; Huang, W.; Gao, X.; Aldape, K.; Lu, Z. Nuclear pkm2 regulates beta-catenin transactivation upon egfr activation. Nature 2011, 480, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.Q.; Hu, Y.Y.; Lin, X.P.; Fan, W. Knockdown of pkm2 and gls1 expression can significantly reverse oxaliplatin-resistance in colorectal cancer cells. Oncotarget 2017, 8, 44171–44185. [Google Scholar] [CrossRef] [Green Version]
- Karachaliou, N.; Papadaki, C.; Lagoudaki, E.; Trypaki, M.; Sfakianaki, M.; Koutsopoulos, A.; Mavroudis, D.; Stathopoulos, E.; Georgoulias, V.; Souglakos, J. Predictive value of brca1, ercc1, atp7b, pkm2, topoi, topomicron-iia, topoiib and c-myc genes in patients with small cell lung cancer (sclc) who received first line therapy with cisplatin and etoposide. PLoS ONE 2013, 8, e74611. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, C.; Sfakianaki, M.; Lagoudaki, E.; Giagkas, G.; Ioannidis, G.; Trypaki, M.; Tsakalaki, E.; Voutsina, A.; Koutsopoulos, A.; Mavroudis, D.; et al. Pkm2 as a biomarker for chemosensitivity to front-line platinum-based chemotherapy in patients with metastatic non-small-cell lung cancer. Br. J. Cancer 2014, 111, 1757–1764. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Cardus, A.; Martinez-Balibrea, E.; Bandres, E.; Malumbres, R.; Gines, A.; Manzano, J.L.; Taron, M.; Garcia-Foncillas, J.; Abad, A. Pharmacogenomic approach for the identification of novel determinants of acquired resistance to oxaliplatin in colorectal cancer. Mol. Cancer Ther. 2009, 8, 194–202. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Balibrea, E.; Plasencia, C.; Gines, A.; Martinez-Cardus, A.; Musulen, E.; Aguilera, R.; Manzano, J.L.; Neamati, N.; Abad, A. A proteomic approach links decreased pyruvate kinase m2 expression to oxaliplatin resistance in patients with colorectal cancer and in human cell lines. Mol. Cancer Ther. 2009, 8, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Stetak, A.; Veress, R.; Ovadi, J.; Csermely, P.; Keri, G.; Ullrich, A. Nuclear translocation of the tumor marker pyruvate kinase m2 induces programmed cell death. Cancer Res. 2007, 67, 1602–1608. [Google Scholar] [CrossRef] [Green Version]
- Li, S.L.; Ye, F.; Cai, W.J.; Hu, H.D.; Hu, P.; Ren, H.; Zhu, F.F.; Zhang, D.Z. Quantitative proteome analysis of multidrug resistance in human ovarian cancer cell line. J. Cell. Biochem. 2010, 109, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Yoo, B.C.; Ku, J.L.; Hong, S.H.; Shin, Y.K.; Park, S.Y.; Kim, H.K.; Park, J.G. Decreased pyruvate kinase m2 activity linked to cisplatin resistance in human gastric carcinoma cell lines. Int. J. Cancer 2004, 108, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Cao, Y.; Zhang, Y.; Li, S.; Gao, J.; Wang, X.A.; Mu, J.; Hu, Y.P.; Jiang, L.; Dong, P.; et al. Up-regulation of pkm2 promote malignancy and related to adverse prognostic risk factor in human gallbladder cancer. Sci. Rep. 2016, 6, 26351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Zhang, F.; Wu, X.R. Inhibition of pyruvate kinase m2 markedly reduces chemoresistance of advanced bladder cancer to cisplatin. Sci. Rep. 2017, 7, 45983. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.S.; Zhang, F.J.; Li, H.; Liu, Y.; Du, G.Y.; Huang, Y.H. Tanshinone a inhibits human esophageal cancer cell growth through mir-122-mediated pkm2 down-regulation. Arch. Biochem. Biophys. 2016, 598, 50–56. [Google Scholar] [CrossRef]
- Zhang, X.; He, C.; He, C.; Chen, B.; Liu, Y.; Kong, M.; Wang, C.; Lin, L.; Dong, Y.; Sheng, H. Nuclear pkm2 expression predicts poor prognosis in patients with esophageal squamous cell carcinoma. Pathol. Res. Pract. 2013, 209, 510–515. [Google Scholar] [CrossRef]
- Gines, A.; Bystrup, S.; Ruiz de Porras, V.; Guardia, C.; Musulen, E.; Martinez-Cardus, A.; Manzano, J.L.; Layos, L.; Abad, A.; Martinez-Balibrea, E. Pkm2 subcellular localization is involved in oxaliplatin resistance acquisition in ht29 human colorectal cancer cell lines. PLoS ONE 2015, 10, e0123830. [Google Scholar] [CrossRef] [Green Version]
- Koss, K.; Maxton, D.; Jankowski, J.A. Faecal dimeric m2 pyruvate kinase in colorectal cancer and polyps correlates with tumour staging and surgical intervention. Colorectal Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2008, 10, 244–248. [Google Scholar] [CrossRef]
- Cui, R.; Shi, X.Y. Expression of pyruvate kinase m2 in human colorectal cancer and its prognostic value. Int. J. Clin. Exp. Pathol. 2015, 8, 11393–11399. [Google Scholar]
- Lim, D.R.; Kuk, J.K.; Kim, T.; Shin, E.J. Comparison of oncological outcomes of right-sided colon cancer versus left-sided colon cancer after curative resection: Which side is better outcome? Medicine 2017, 96, e8241. [Google Scholar] [CrossRef]
- Icard, P.; Fournel, L.; Wu, Z.; Alifano, M.; Lincet, H. Interconnection between metabolism and cell cycle in cancer. Trends Biochem. Sci. 2019, 44, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wang, Y.; Wang, T.; Hawke, D.H.; Zheng, Y.; Li, X.; Zhou, Q.; Majumder, S.; Bi, E.; Liu, D.X.; et al. Pkm2 phosphorylates mlc2 and regulates cytokinesis of tumour cells. Nat. Commun. 2014, 5, 5566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, C.L.; Bian, Y.Y.; Xue, Y.; Liu, Z.X.; Zhou, K.Q.; Yao, C.F.; Lin, Y.; Zou, H.F.; Luo, F.X.; Qu, Y.Y.; et al. Pyruvate kinase m2 activates mtorc1 by phosphorylating akt1s1. Sci. Rep. 2016, 6, 21524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.; Du, S.; Lei, T.; Li, X.; Liu, Y.; Wang, H.; Tong, R.; Wang, Y. Pkm2 in carcinogenesis and oncotherapy. Oncotarget 2017, 8, 110656–110670. [Google Scholar] [CrossRef] [Green Version]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of adjuvant chemotherapy for stage iii colon cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef]
- Papadaki, C.; Mavroudis, D.; Trypaki, M.; Koutsopoulos, A.; Stathopoulos, E.; Hatzidaki, D.; Tsakalaki, E.; Georgoulias, V.; Souglakos, J. Tumoral expression of txr1 and tsp1 predicts overall survival of patients with lung adenocarcinoma treated with first-line docetaxel-gemcitabine regimen. Clin. Cancer Res. 2009, 15, 3827–3833. [Google Scholar] [CrossRef] [Green Version]
- Souglakos, J.; Philips, J.; Wang, R.; Marwah, S.; Silver, M.; Tzardi, M.; Silver, J.; Ogino, S.; Hooshmand, S.; Kwak, E.; et al. Prognostic and predictive value of common mutations for treatment response and survival in patients with metastatic colorectal cancer. Br. J. Cancer 2009, 101, 465–472. [Google Scholar] [CrossRef]
- Cushman-Vokoun, A.M.; Stover, D.G.; Zhao, Z.; Koehler, E.A.; Berlin, J.D.; Vnencak-Jones, C.L. Clinical utility of kras and braf mutations in a cohort of patients with colorectal neoplasms submitted for microsatellite instability testing. Clin. Colorectal Cancer 2013, 12, 168–178. [Google Scholar] [CrossRef] [Green Version]
- Sfakianaki, M.; Papadaki, C.; Tzardi, M.; Trypaki, M.; Alam, S.; Lagoudaki, E.D.; Messaritakis, I.; Zoras, O.; Mavroudis, D.; Georgoulias, V.; et al. Loss of lkb1 protein expression correlates with increased risk of recurrence and death in patients with resected, stage ii or iii colon cancer. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2019, 51, 1518. [Google Scholar] [CrossRef]


{kind=link}
| Pts | Group A (262) | Group B (118) | Group C (104) | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Median Age (Range) | 67 (33–75) | 65 (35–84) | 65 (41–79) | |||
| ≤70 years | 162 | 62 | 77 | 65 | 78 | 73 |
| >70 years | 100 | 38 | 41 | 35 | 26 | 27 |
| Gender | ||||||
| Male | 152 | 58 | 76 | 64 | 66 | 64 |
| Female | 110 | 42 | 42 | 36 | 38 | 36 |
| Performance Status (ECOG) # | ||||||
| 0 | 196 | 75 | 110 | 93 | 98 | 94 |
| 1 | 66 | 25 | 8 | 7 | 6 | 6 |
| Stage | ||||||
| IIa | 90 | 34 | ||||
| IIb | 14 | 6 | ||||
| IIIa | 19 | 7 | ||||
| IIIb | 81 | 31 | ||||
| IIIc | 58 | 22 | ||||
| IV | 118 | 100 | 104 | 100 | ||
| Tumor grade | ||||||
| low | 160 | 61 | 69 | 59 | 60 | 58 |
| high | 102 | 39 | 49 | 41 | 44 | 42 |
| Mucinous | ||||||
| Yes | 59 | 23 | ||||
| No | 203 | 77 | ||||
| Obstruction | 27 | 10 | ||||
| Perforation | 40 | 15 | ||||
| Location | ||||||
| Right-sided | 91 | 35 | 36 | 31 | 26 | 25 |
| Left-sided | 171 | 65 | 82 | 69 | 78 | 75 |
| Regimen | ||||||
| CAPOX | 171 | 65 | ||||
| FOLFOX | 91 | 35 | ||||
| FOLFOX/CAPOX | 46 | 39 | ||||
| FOLFOX/CAPOX + Bevacizumab | 45 | 38 | ||||
| FOLFOX/CAPOX + Cetuximab | 27 | 23 | ||||
| FOLFIRI | 18 | 17 | ||||
| FOLFIRI + Bevacizumab | 86 | 83 | ||||
| BRAFV600E status | ||||||
| Wild type (WT) | 230 | 87.8 | 110 | 93 | 97 | 94 |
| Mutant | 13 | 5.0 | 8 | 7 | 7 | 6 |
| Failed | 19 | 7.2 | ||||
| KRAS exon 2 mutation | ||||||
| WT | 169 | 64.5 | 76 | 64 | 69 | 66 |
| Mutant | 82 | 31.3 | 42 | 36 | 35 | 34 |
| Failed | 11 | 4.2 | ||||
| MMR Status | ||||||
| Proficient | 200 | 76.3 | Not Done | Not Done | ||
| Deficient | 35 | 13.4 | Not Done | Not Done | ||
| Failed | 27 | 10.3 | ||||
| Median No of Retrieved Lymph Nodes (min–max) | 15 (6–108) | |||||
| Median No of +ve Lymph Nodes (min–max) | 1 (0–18) | |||||
| Median Number of metastatic sites | 1 (1–4) | 1 (1–5) | ||||
| Metastatic disease | ||||||
| Synchronous | 44 | 37 | 30 | 29 | ||
| Metachronous | 74 | 63 | 74 | 71 | ||
| PKM2 mRNA Expression. | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| (n = 258) | (n = 118) | (n = 104) | |||||||
| Group A | Group B | Group C | |||||||
| Low (n = 129) | High (n = 129) | p value | Low (n = 117) | High (n = 137) | p value | Low (n = 117) | High (n = 137) | p value | |
| Patients enrolled | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |||
| Age Median (min–max) | 67 (33–75) | 67 (37–75) | 0.147 # | 65 (35–81) | 65 (39–84) | 0.564 # | 65 (44–76) | 64 (41–79) | 0.218 # |
| Age group | |||||||||
| ≤70 | 72 (45.3) | 87 (54.7) | 0.08 @ | 52 (67.5) | 25 (32.5) | 0.499 @ | 47 (60.2) | 31 (39.8) | 0.614 @ |
| >70 | 57 (57.5) | 42(42.5) | 28 (68.2) | 13 (31.8) | 15 (57.7) | 11 (42.3) | |||
| Gender | |||||||||
| Male | 75 (51.0) | 72(49.0) | 0.669 * | 49 (64.5) | 27 (35.5) | 0.411 * | 35 (53.0) | 31 (47) | 0.571 * |
| Female | 52 (47.7) | 57(52.3) | 31 (73.8) | 11 (26.2) | 21 (55.3) | 17 (34.7) | |||
| Lymph Node Status | |||||||||
| N0 | 63(61.8) | 39 (38.2) | 0.018 * | ||||||
| N1–2 | 64 (41.8) | 89 (58.2) | |||||||
| Tumor Location | |||||||||
| Right | 55 (60.4) | 36 (39.6) | 0.011 * | 24 (66.7) | 12 (33.3) | 0.003 * | 16 (61.5) | 10 (38.5) | 0.001 * |
| Left | 74 (44.3) | 93 (56.7) | 39 (47.6) | 43 (52.4) | 29 (37.2) | 49 (62.8) | |||
| Grade | |||||||||
| Low grade | 117 (74.5) | 41 (25.5) | 0.001 * | 51 (73.9) | 18 (26.1) | 0.017 * | 43 (71.7) | 17 (18.3) | 0.021 * |
| High grade | 12 (12.0) | 88 (88.0) | 8 (16.3) | 41 (83.7) | 7 (15.8) | 37 (84.2) | |||
| Mucinous | |||||||||
| Yes | 40 (68.9) | 18 (31.1) | 0.001 * | ||||||
| No | 89 (44.5) | 111 (55.5) | |||||||
| KRAS exon 2 status | |||||||||
| Wild type | 87 (51.5) | 83 (48.5) | 0.87 | 47 (61.8) | 29 (38.2) | 0.009 * | 46 (66.7) | 23 (33.3) | 0.026 * |
| Mutant | 40 (48.8) | 42 (51.2) | 6 (14.3) | 36 (85.7) | 9 (25.7) | 26 (74.3) | |||
| UKNOWN | 2 | 4 | 0 | 0 | |||||
| BRAFV600E status | |||||||||
| Wild type | 112 (48.1) | 117 (51.9) | 0.109 | 74 (67.3) | 36 (32.7) | 0.041 * | 58 (59.8) | 39 (40.2) | 0.05 * |
| Mutant | 8 (61.5) | 5 (38.5) | 1 (12.5) | 7 (87.5) | 1 (16.7) | 6 (83.3) | |||
| UKNOWN | 9 | 7 | 0 | 0 | 0 | 0 | |||
| MMR Status | |||||||||
| Proficient | 88 (44) | 108 (56) | <0.001 | ||||||
| Deficient | 29 (82.8) | 6 (17.2) | |||||||
| UKNOWN | 12 | 15 | |||||||
| Pts | Group A | Group B | Group C | |||
|---|---|---|---|---|---|---|
| Feature | HR # (95% CI ^) | p Value | HR # (95% CI ^) | p Value | HR # (95% CI ^) | p Value |
| PFS | ||||||
| Age (>70 y vs. ≤70 y) | 1.03 (0.64–1.67) | 0.887 | 1.17 (0.89–1.32) | 0.214 | 1.21 (0.94–1.41) | 0.167 |
| Gender (Men vs. Women) | 1.18 (0.92–1.80) | 0.112 | 1.07 (0.61–1.18) | 0.816 | 1.04 (0.63–1.14) | 0.883 |
| Stage (III vs. II) | 1.80(1.61–2.10) | 0.023 | ||||
| Tumor Location (Right vs. Left) | 1.13 (0.68–1.87) | 0.234 | 1.34 (1.09–2.09) | 0.037 | 1.29 (1.06–1.99) | 0.043 |
| Grade (High vs. Low) | 1.86 (1.18–3.08) | 0.722 | 1.16 (0.84–1.23) | 0.304 | 1.21 (0.79–1.94) | 0.682 |
| PKM2 mRNA expression (High vs. Low) | 1.82 (1.21–2.96) | 0.003 | 1.91 (1.34–2.99) | 0.002 | 1.06 (0.65–1.31) | 0.769 |
| KRAS exon2 mutation (Mutants. & vs. wild type @) | 1.76 (1.09–3.10) | 0.050 | 1.85 (1.16–2.85) | 0.047 | 1.80 (1.09–2.91) | 0.046 |
| BRAFV600E mutation (Mut. & vs. wt @) | 1.97 (1.79–2.50) | 0.001 | 3.02 (2.46–5.73) | 0.001 | 2.88 (1.93–50.8) | 0.001 |
| MMR status (Proficient vs. Deficient) | 1.73 (1.29–3.51) | 0.025 | ||||
| OS | ||||||
| Age (>70 y vs. ≤70 y) | 1.01 (0.98–1.04) | 0.781 | 1.22 (0.94–1.38) | 0.189 | 1.24 (0.96–1.44) | 0.118 |
| Gender (Men vs. Women) | 1.21 (0.94–1.84) | 0.106 | 1.11 (0.72–1.24) | 0.603 | 1.17 (0.77–1.32) | 0.712 |
| Stage (III vs. II) | 1.64 (1.45–2. 01) | 0.030 | ||||
| Tumor Location (Right vs. Left) | 1.02 (0.56–1.85) | 0.906 | 1.44 (1.18–2.31) | 0.018 | 1.39 (1.23–2.08) | 0.023 |
| Grade (High vs. Low) | 1.11 (0.57–2.21) | 0.781 | 1.09 (0.88–1.21) | 0.446 | 1.14 (0.8–1.91) | 0.588 |
| PKM2 mRNA expression (High vs. Low) | 1.84 (1.29–3.26) | 0.002 | 2.12 (1.51–3.17) | 0.002 | 1.04 (0.58–1.24) | 0.811 |
| KRAS exon2 mutation (Mut. & vs. wt @) | 1.20 (0.61–2.33) | 0.113 | 1.56 (0.98–1.94) | 0.077 | 1.49 (0.96–2.03) | 0.102 |
| BRAFV600E mutation (Mut. & vs. wt @) | 1.62 (1.14–2.31) | 0.007 | 3.02 (2.46–5.73) | 0.001 | 2.88 (1.93–50.8) | 0.001 |
| MMR status (Proficient vs. Deficient) | 1.38 (1.04–2.71) | 0.036 | ||||
| Feature | Group A | Group B | Group C | |||
|---|---|---|---|---|---|---|
| HR # (95% CI ^) | p Value | HR # (95% CI ^) | p Value | HR # (95% CI ^) | p Value | |
| DFS/PFS | ||||||
| Stage (III vs. II) | 1.27 (1.03–1.76) | 0.046 | ||||
| Tumor Location (Right vs. Left) | 1.17 (0.91–1.88) | 0.121 | 1.12 (0.88–1.69) | 0.198 | ||
| PKM2 mRNA expression (High vs. Low) | 1.88 (1.37–2.99) | 0.002 | 1.94 (1.38–3.32) | 0.001 | 1.08 (0.66–1.33) | 0.517 |
| KRAS exon2 mutation (Mut. & vs. wt @) | 1.35 (0.92–1.91) | 0.103 | 1.31 (0.91–2.06) | 0.197 | 1.29 (0.86–1.91) | 0.267 |
| BRAFV600E mutation (Mut. & vs. wt @) | 1.98 (1.64–2.67) | 0.001 | 3.61 (2.67–5.81) | <0.001 | 3.43 (2.58–5.79) | <0.001 |
| MMR status (Proficient vs. Deficient) | 1.76 (1.31–3.44) | 0.021 | ||||
| OS (overall survival) | ||||||
| Stage (III vs. II) | 1.33 (1.09–1.88) | 0.039 | ||||
| Tumor Location (Right vs. Left) | 1.25 (0.98–2.07) | 0.081 | 1.118 (0.93–1.88) | 0.092 | ||
| PKM2 mRNA expression (High vs. Low) | 1.91 (1.45–2.97) | 0.001 | 1.99 (1.49–3.41) | 0.001 | 1.03 (0.59–1.39) | 0.612 |
| KRAS exon2 mutation (Mut. & vs. wt @) | 1.35 (0.92–1.91) | 0.103 | 1.31 (0.91–2.06) | 0.197 | 1.29 (0.86–1.91) | 0.267 |
| BRAFV600E mutation (Mut. & vs. wt @) | 2.12 (1.69–2.91) | <0.001 | 3.78 (2.81–5.66) | <0.001 | 3.64 (2.66–5.61) | <0.001 |
| MMR (Mismatch Repair System) status (Proficient vs. Deficient) | 1.89 (1.47–3.52) | 0.002 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sfakianaki, M.; Papadaki, C.; Tzardi, M.; Trypaki, M.; Manolakou, S.; Messaritakis, I.; Saridaki, Z.; Athanasakis, E.; Mavroudis, D.; Tsiaoussis, J.; et al. PKM2 Expression as Biomarker for Resistance to Oxaliplatin-Based Chemotherapy in Colorectal Cancer. Cancers 2020, 12, 2058. https://doi.org/10.3390/cancers12082058
Sfakianaki M, Papadaki C, Tzardi M, Trypaki M, Manolakou S, Messaritakis I, Saridaki Z, Athanasakis E, Mavroudis D, Tsiaoussis J, et al. PKM2 Expression as Biomarker for Resistance to Oxaliplatin-Based Chemotherapy in Colorectal Cancer. Cancers. 2020; 12(8):2058. https://doi.org/10.3390/cancers12082058
Chicago/Turabian StyleSfakianaki, Maria, Chara Papadaki, Maria Tzardi, Maria Trypaki, Stavroula Manolakou, Ippokratis Messaritakis, Zenia Saridaki, Elias Athanasakis, Dimitrios Mavroudis, John Tsiaoussis, and et al. 2020. "PKM2 Expression as Biomarker for Resistance to Oxaliplatin-Based Chemotherapy in Colorectal Cancer" Cancers 12, no. 8: 2058. https://doi.org/10.3390/cancers12082058