Ductal Carcinoma In Situ of the Breast: An Update with Emphasis on Radiological and Morphological Features as Predictive Prognostic Factors

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Definition
2. Epidemiology
3. Clinical Features
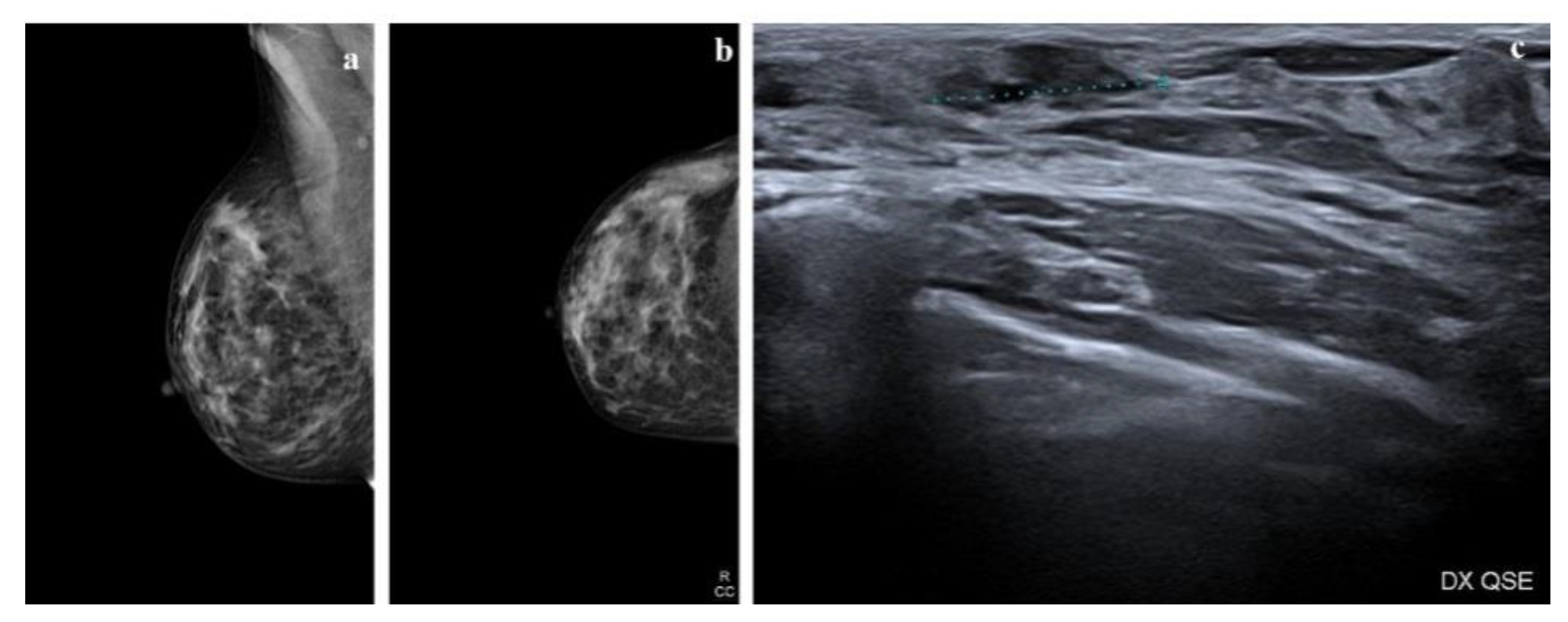
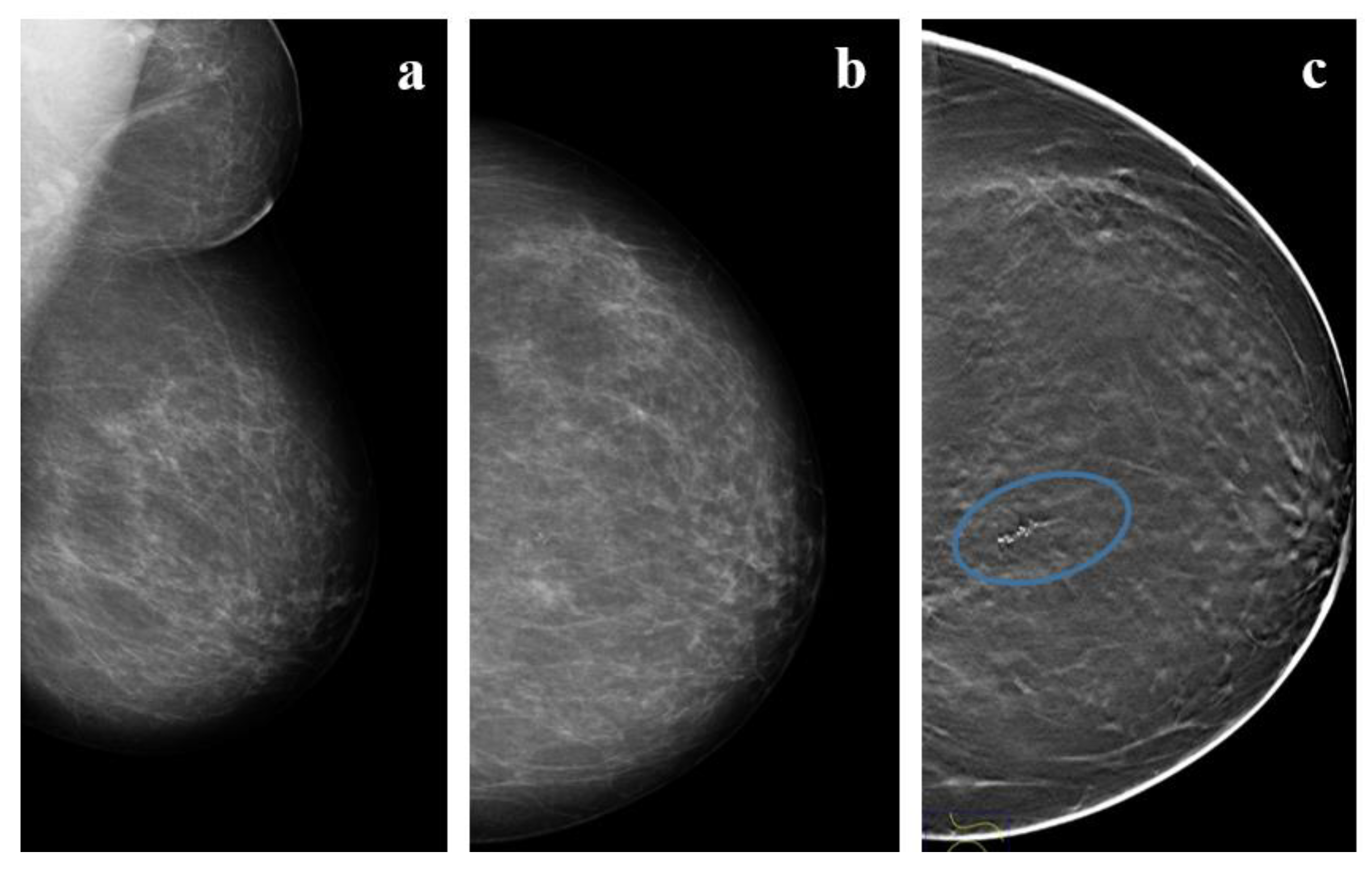
4. Radiologic Features
5. Magnetic Resonance Imaging
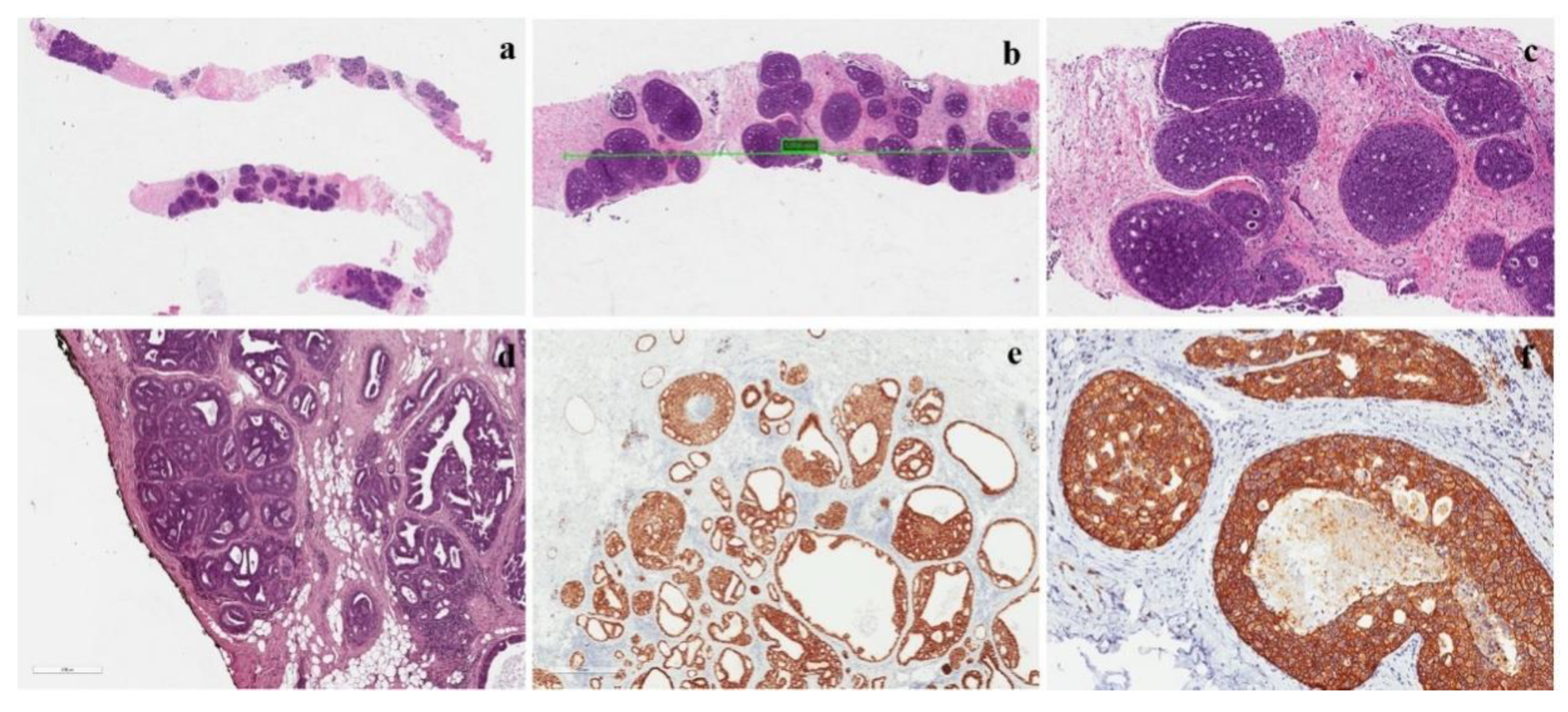
6. Morphological Features of Carcinoma In Situ
7. Immunohistochemical Profile
8. Molecular Features
9. Surgical Margins
10. Sentinel Node Sampling
11. Natural History
12. Treatment
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Classification of Breast Tumours, 5th ed.; WHO Classification of Tumours Editorial Board: Geneva, Switzerland, 2019; Volume 2. [Google Scholar]
- Weaver, D.L.; Rosenberg, R.D.; Barlow, W.E.; Ichikawa, L.; Carney, P.A.; Kerlikowske, K.; Buist, D.; Geller, B.M.; Key, C.R.; Maygarden, S.J.; et al. Pathologic findings from the Breast Cancer SurvellainceConsortium: Vpopulation-based outcomes in women undergoing biopsy after screening mammography. Cancer 2006, 106, 732–742. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Levinsohn, E.; Altman, M.; Chagpar, A.B. Controversies regarding the diagnosis and management of ductal carcinoma in situ. Am. Surg. 2018, 84, 1–6. [Google Scholar] [PubMed]
- Virnig, B.A.; Tuttle, T.M.; Shamliyan, T.; Shamliyan, T.; Kane, R.L. Ductal carcinoma in situ of the breast: A systematic review of incidence, treatment, and outcomes. J. Natl. Cancer Inst. 2010, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, S.R.; Ellis, I.O.; Schnitt, S.J. WHO/IARC Classification of Tumours of the Breast, 4th ed.; WHO/IARC: Lyon, France, 2012; Volume 4. [Google Scholar]
- Bijker, N.; Donker, M.; Wesseling, J.; Th Rutgers, E.J. Is DCIS breast cancer, and how do I treat it? Curr. Treat. Options Oncol. 2013, 14, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Ernster, V.L.; Ballard-Barbash, R.; Barlow, W.E.; Zheng, Y.; Weaver, D.L.; Cutter, G.; Yankaskas, B.C.; Rosenberg, R.; Carney, P.A.; Kerlikowske, K.; et al. Detection of ductal carcinoma in situin women undergoing screening mammography. J. Natl. Cancer Inst. 2002, 94, 1546–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stomper, P.C.; Connolly, J.L.; Meyer, J.E.; Harris, J.R. Clinically occult ductal carcinoma in situdetected with mammography: Analysis of 100 cases with radiologic-pathologic correlation. Radiology 1989, 172, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, D.; Macaskill, P.; Pellegrini, M.; Valentini, M.; Fantò, C.; Ostillio, L.; Tuttobene, P.; Luparia, A.; Houssami, N. Breast cancer screening with tomosynthesis (3D mammography) with acquired or synthetic 2D mammography compared with 2D mammography alone (STORM-2): A population-based prospective study. Lancet Oncol. 2016, 17, 1105–1113. [Google Scholar] [CrossRef]
- Mcneil, J.H.; Morris, E.A.; Dershaw, D.D.; Abramson, A.F.; Brogi, E.; Liberman, L. Determination of the presence and extent of pure ductal carcinoma in situby mammography and magnetic resonance imaging. Breast J. 2005, 11, 382–390. [Google Scholar] [CrossRef]
- Pediconi, F.; Catalano, C.; Roselli, A.; Padula, S.; Altomari, F.; Moriconi, E.; Pronio, A.M.; Kirchin, M.A.; Passariello, R. Contrast-enhanced MR mammography for evaluation of the contralateral breast in patients with diagnosed unilateral breast cancer or high-risk lesions. Radiology 2007, 243, 670–680. [Google Scholar] [CrossRef]
- Londero, V.; Zuiani, C.; Linda, A.; Girometti, R.; Bazzocchi, M.; Sardanelli, F. High-risk breast lesions at imaging- guided needle biopsy: Usefulness of MRI fur treatment decision. AJR Am. J. Roentgenol. 2012, 199, W240–W250. [Google Scholar] [CrossRef] [PubMed]
- College of American Pathologists (CAP). Protocol for the Examination of Specimens from Patients with Ductal Carcinoma in Situ(DCIS) of the Breast; Version: Breast DCIS 4.1.0.0.; CAP: Northfield, IL, USA, 2018. [Google Scholar]
- Zhang, X.; Dai, H.; Liu, B.; Song, F.; Chen, K. Predictors for local invasive recurrence of ductal carcinoma in situ of the breast: A meta-analysis. Eur. J. Cancer Prev. 2016, 25, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, W.M.; Parra-Herran, C.; Lu, F.I.; Slodkowska, E.; Rakovitch, E.; Nofech-Mozes, S. Ductal carcinoma in situ of the breast: An update for the pathologist in the era of individualized risk assessment and tailored therapies. Mod. Pathol. 2019, 32, 896–915. [Google Scholar] [CrossRef]
- Sneige, N.; McNeese, M.D.; Atkinson, E.N.; Ames, F.C.; Kemp, B.; Sahin, A.; Ayala, A.G. Ductal carcinoma in situtreated with lumpectomy and irradiation: Histopathological analysis of 49 specimens with emphasis on risk factors and long term results. Hum. Pathol. 1995, 26, 642–649. [Google Scholar] [CrossRef]
- Loi, S.; Sirtaine, N.; Piette, F.; Salgado, R.; Viale, G.; Van Eenoo, F.; Rouas, G.; Francis, P.; Crown, J.P.A.; Hitre, E.; et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J. Clin. Oncol. 2013, 31, 860–867. [Google Scholar] [CrossRef]
- Dieci, M.V.; Mathieu, M.C.; Guarneri, V.; Conte, P.; Delaloge, S.; Andre, F.; Goubar, A. Prognostic and predictive value of tumor-infiltrating lymphocytes in two phase III randomized adjuvant breast cancer trials. Ann. Oncol. 2015, 26, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Stanton, S.E.; Adams, S.; Disis, M.L. Variation in the Incidence and Magnitude of Tumor-Infiltrating Lymphocytes in Breast Cancer Subtypes: A Systematic Review. JAMA Oncol. 2016, 2, 1354–1360. [Google Scholar] [CrossRef] [PubMed]
- Pruneri, G.; Lazzeroni, M.; Bagnardi, V.; Tiburzio, V.; Rotmensz, N.; DeCensi, A.; Guerrieri-Gonzaga, A.; Vingiani, A.; Curigliano, G.; Zurrida, S.; et al. The prevalence and clinical relevance of tumor-infiltrating lymphocytes (TILs) in ductal carcinoma in situ of the breast. Ann. Oncol. 2017, 28, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Shamliyan, T.; Wang, S.Y.; Virnig, B.A.; Tuttle, T.M.; Kane, R.M. Association between patient and tumor characteristics with clinical outcomes in women with ductal carcinoma in situ. J. Natl. Cancer Inst. Monogr. 2010, 41, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Sikand, K.; Lee, A.H.; Pinder, S.E.; Elston, C.W.; Ellis, I.O. Sections of the nipple and quadrants in mastectomy specimens for carcinoma are of limited value. J. Clin. Pathol. 2005, 58, 543–545. [Google Scholar] [CrossRef] [Green Version]
- Punglia, R.S.; Jiang, W.; Lipsitz, S.R.; Hughes, M.E.; Schnitt, S.J.; Hassett, M.J.; Nekhlyudov, L.; Achacoso, N.; Edge, S.; Javid, S.H.; et al. Clinical risk score to predict likelihood of recurrence after ductal carcinoma in situtreated with breast-conserving surgery. Breast Cancer Res. Treat. 2018, 167, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.E.; Barnes, N.L.; Cramer, A.; Johnson, R.; Cheema, K.; Morris, J.; Howe, M.; Bundred, N.J. Molecular phenotypes of DCIS predict overall and invasive recurrence. Ann. Oncol. 2015, 26, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Wapnir, I.L.; Dignam, J.J.; Fisher, B.; Mamounas, E.P.; Anderson, S.J.; Julian, T.B.; Land, A.R.; Margolese, R.G.; Swain, S.M.; Costantino, J.P.; et al. Long-Term Outcomes of Invasive Ipsilateral Breast Tumor Recurrences After Lumpectomy in NSABP B-17 and B-24 Randomized Clinical Trials for DCIS. J. Natl. Cancer Inst. 2011, 103, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Morrow, M.; Van Zee, K.J.; Solin, L.J.; Houssami, N.; Chavez-MacGregor, M.; Harris, J.R.; Horton, J.; Hwang, S.; Johnson, P.L.; Marinovich, M.L.; et al. Society of Surgical Oncology-American Society for Radiation Oncology-American Society of Clinical Oncology Consensus Guideline on Margins for Breast-Conserving Surgery with Whole-Breast Irradiation in Ductal Carcinoma In Situ. Ann. Surg. Oncol. 2016, 23, 3801–3810. [Google Scholar] [CrossRef] [Green Version]
- Francis, A.; Thomas, J.; Fallowfield, L.; Wallis, M.; Bartlett, J.M.; Brookes, C.; Roberts, T.; Pirrie, S.; Gaunt, C.; Young, J.; et al. Addressing overtreatment of screen detected DCIS; the LORIS trial. Eur. J. Cancer 2015, 51, 2296–2303. [Google Scholar] [CrossRef] [Green Version]
- Senkus, E.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rutgers, E. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, V8–V30. [Google Scholar] [CrossRef]
- National Institute of Health and Clinical Excellence. Early and locally advanced breast cancer: Diagnosis and treatment. NICE clinical guideline 80. In Surgery to the Breast (1.31); National Institute of Health and Clinical Excellence: London, UK, 2009. [Google Scholar]
- New Zealand Guidelines Group (NZGG). Ductal carcinoma in situ. In Management of Early Breast Cancer; New Zealand Guidelines Group (NZGG): Wellington, New Zealand, 2009; pp. 133–141. [Google Scholar]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines; Breast Cancer Version 1; New Zealand Guidelines Group (NZGG): Wellington, New Zealand, 2017. [Google Scholar]
- American Society of Breast Surgeons. The American Society of Breast Surgeons Position Statement on Breast Cancer Lumpectomy Margins; American Society of Breast Surgeons: Colombia, MD, USA, 2015. [Google Scholar]
- Tadros, A.B.; Smith, B.D.; Shen, Y.; Lin, H.; Krishnamurthy, S.; Lucci, A. Contemporary Breast Conservation Patient Outcomes for Ductal Carcinoma in situand Margins <2 mm; American Society of Clinical Oncology: Alexandria, VA, USA, 2017. [Google Scholar]
- Van Zee, K.J.; Subhedar, P.; Olcese, C.; Patil, S.; Morrow, M. Relationship between Margin Width and Recurrence of Ductal Carcinoma In situ: Analysis of 2996 Women Treated with Breast-conserving Surgery for 30 Years. Ann. Surg. 2015, 262, 623–631. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.H.; Sweeney, K.J.; Wilson, M.E.; Goldberg, J.I.; Buchanan, C.L.; Tan, L.K.; Liberman, L.; Turner, R.R.; Lagios, M.D.; Cody, H.S., III; et al. Outcomes for women with ductal carcinoma-in-situ and a positive sentinel node: A multi-institutional audit. Ann. Surg. Oncol. 2007, 14, 2911–2917. [Google Scholar] [CrossRef]
- Stuart, K.E.; Houssami, N.; Taylor, R.; Hayen, A.; Boyages, J. Long-term outcomes of ductal carcinoma in situ of the breast: A systematic review, meta-analysis and meta-regression analysis. BMC Cancer 2015, 15, 890. [Google Scholar] [CrossRef] [Green Version]
- Collins, L.C.; Tamimi, R.; Baer, H.; Connolly, J.; Colditz, G.; Schnitt, S. Risk of invasive breast cancer in patients with ductal carcinoma in situ [DCIS] treated by diagnostic biopsy alone:Results from the Nurses’ Health Study. Breast Cancer Res. Treat. 1994, 88, 1083. [Google Scholar] [CrossRef]
- Page, D.L.; Dupont, W.D.; Rogers, L.W.; Jensen, R.A.; Schuyler, P.A. Continued local recurrence of carcinoma 15–25 years after a diagnosis of low grade ductal carcinoma in situ of the breast treated only by biopsy. Cancer 1995, 76, 197–2000. [Google Scholar] [CrossRef]
- Sanders, M.E.; Schuyler, P.A.; Dupont, W.D.; Page, D.L. The natural history of low-grade ductal carcinoma in situ of the breast in women treated by biopsy only revealed over 30 years of long-term follow-up. Cancer 2005, 103, 2481–2484. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.E.; Schuyler, P.A.; Simpson, J.F.; Page, D.L.; Dupont, W.D. Continued observation of the natural history of low-grade ductal carcinoma in situreaffirms proclivity for local recurrence even after more than 30 years of follow-up. Mod. Pathol. 2015, 28, 662–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryser, M.D.; Worni, M.; Turner, E.L.; Marks, J.R.; Durrett, R.; Hwang, E.S. Outcomes of active surveillance for ductal carcinoma in situ: A computational risk analysis. J. Natl. Cancer Inst. 2015, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solin, L.J.; Gray, R.; Hughes, L.L.; Wood, W.C.; Lowen, M.A.; Badve, S.S.; Baehner, F.L.; Ingle, J.N.; Perez, E.A.; Recht, A.; et al. Surgical excision without radiation for ductal carcinoma in situ of the breast: 12-year results from the ECOG-ACRIN E5194 Study. J. Clin. Oncol. 2015, 33, 3938–3944. [Google Scholar] [CrossRef] [Green Version]
- Holmes, P.; Lloyd, J.; Chervoneva, I.; Pequinot, E.; Cornfield, D.B.; Schwartz, G.F.; Allen, K.G.; Palazzo, J.P. Prognostic markers and long-term outcomes in ductal carcinoma in situ of the breast treated with excision alone. Cancer 2011, 117, 3650–3657. [Google Scholar] [CrossRef]
- Rakovitch, E.; Nofech-Mozes, S.; Hanna, W.; Narod, S.; Thiruchelvam, D.; Saskin, R.; Spayne, J.; Taylor, C.; Paszat, L. HER2/neu and Ki-67 expression predict non-invasive recurrence following breast-conserving therapy for ductal carcinoma in situ. Br. J. Cancer 2012, 106, 1160–1165. [Google Scholar] [CrossRef] [Green Version]
- Donker, M.; Litière, S.; Werutsky, G.; Julien, J.P.; Fentiman, I.S.; Agresti, R.; Rouanet, P.; de Lara, C.T.; Bartelink, H.; Duez, N.; et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma in situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized phase III trial. J. Clin. Oncol. 2013, 31, 4054–4059. [Google Scholar] [CrossRef]
- Wärnberg, F.; Garmo, H.; Emdin, S.; Hedberg, V.; Adwall, L.; Sandelin, K.; Ringberg, A.; Karlsson, P.; Arnesson, L.G.; Anderson, H.; et al. Effect of radiotherapy after breast-conserving surgery for ductal carcinoma in situ: 20 years follow-up in the randomized SweDCIS Trial. J. Clin. Oncol. 2014, 32, 3613–3618. [Google Scholar] [CrossRef]
- Cuzick, J.; Sestak, I.; Pinder, S.E.; Ellis, I.O.; Forsyth, S.; Bundred, N.J.; Forbes, J.F.; Bishop, H.; Fentiman, I.S.; George, W.D. Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: Long-term results from the UK/ANZ DCIS trial. Lancet Oncol. 2011, 12, 21–29. [Google Scholar] [CrossRef]
- Guerrieri-Gonzaga, A.; Sestak, I.; Lazzeroni, M.; Serrano, D.; Rotmensz, N.; Cazzaniga, M.; Varricchio, C.; Pruneri, G.; Leonardi, M.C.; Orecchia, R.; et al. Benefit of low-dose tamoxifen in a large observational cohort of high risk ER positive breast DCIS. Int. J. Cancer 2016, 139, 2127–2134. [Google Scholar] [CrossRef] [PubMed]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvatorelli, L.; Puzzo, L.; Vecchio, G.M.; Caltabiano, R.; Virzì, V.; Magro, G. Ductal Carcinoma In Situ of the Breast: An Update with Emphasis on Radiological and Morphological Features as Predictive Prognostic Factors. Cancers 2020, 12, 609. https://doi.org/10.3390/cancers12030609
Salvatorelli L, Puzzo L, Vecchio GM, Caltabiano R, Virzì V, Magro G. Ductal Carcinoma In Situ of the Breast: An Update with Emphasis on Radiological and Morphological Features as Predictive Prognostic Factors. Cancers. 2020; 12(3):609. https://doi.org/10.3390/cancers12030609
Chicago/Turabian StyleSalvatorelli, Lucia, Lidia Puzzo, Giada Maria Vecchio, Rosario Caltabiano, Valentina Virzì, and Gaetano Magro. 2020. "Ductal Carcinoma In Situ of the Breast: An Update with Emphasis on Radiological and Morphological Features as Predictive Prognostic Factors" Cancers 12, no. 3: 609. https://doi.org/10.3390/cancers12030609