Proton Beam Therapy Combined with Intra-Arterial Infusion Chemotherapy for Stage IV Adenoid Cystic Carcinoma of the Base of the Tongue

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Compliance
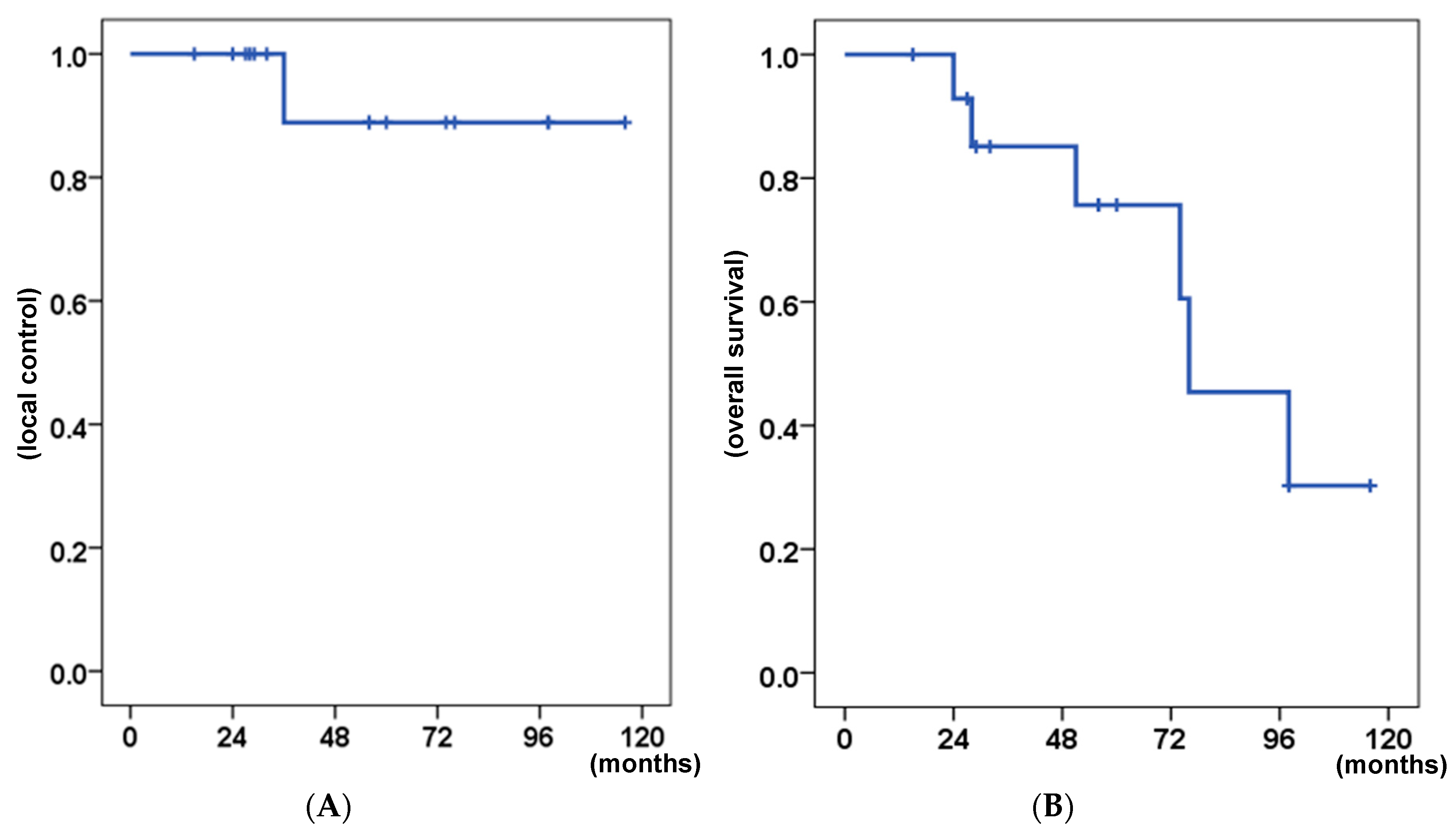
2.3. Response and Survival
2.4. Toxicities
3. Discussion
4. Materials and Methods
4.1. Ethics Statement
4.2. Patients and Study Design
4.3. PBT
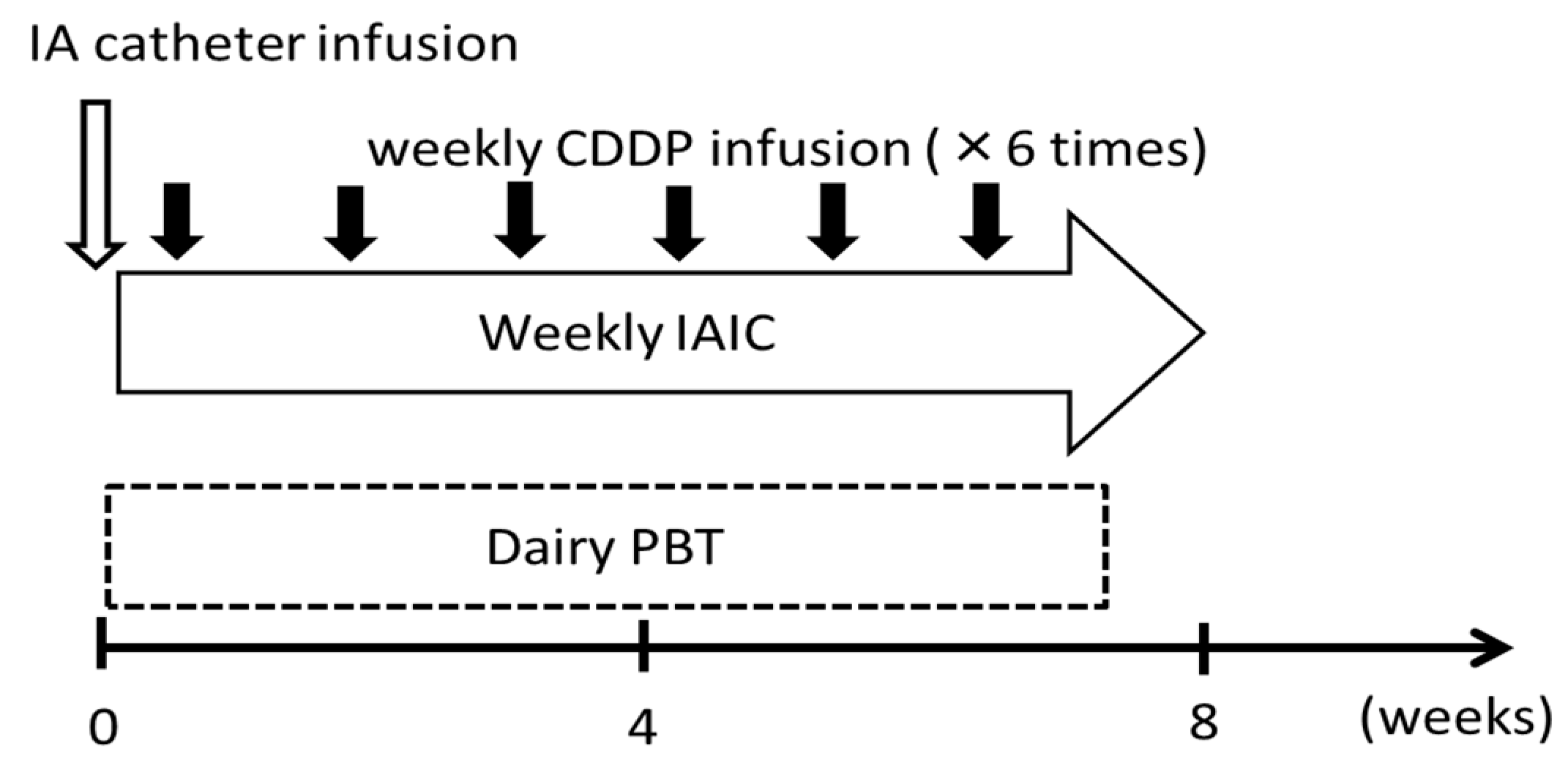
4.4. IAIC
4.5. Patient Assessments (Follow-up)
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kim, K.H.; Sung, M.W.; Chung, P.S.; Rhee, C.S.; Park, C.; Kim, W.H. Adenoid cystic carcinoma of the head and neck. Arch. Otolaryngol. Head Neck Surg. 1994, 120, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Khafif, A.; Anavi, Y.; Haviv, J.; Fienmesser, R.; Calderon, S.; Marshak, G. Adenoid cystic carcinoma of the salivary glands: A 20-year review with long-term follow-up. Ear Nose Throat J. 2005, 84, 662, 664–667. [Google Scholar] [CrossRef] [PubMed]
- Spiro, R.H.; Huvos, A.G.; Strong, E.W. Adenoid cystic carcinoma of salivary origin. A clinicopathologic study of 242 cases. Am. J. Surg. 1974, 128, 512–520. [Google Scholar] [CrossRef]
- Goepfert, H.; Giraldo, A.A.; Byers, R.M.; Luna, M.A. Salivary gland tumors of the base of the tongue. Arch. Otolaryngol. 1976, 102, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Silverman, D.A.; Carlson, T.P.; Khuntia, D.; Bergstrom, R.T.; Saxton, J.; Esclamado, R.M. Role for postoperative radiation therapy in adenoid cystic carcinoma of the head and neck. Laryngoscope 2004, 114, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Bucci, M.K.; Weinberg, V.; Garcia, J.; Quivey, J.M.; Schechter, N.R.; Phillips, T.L.; Fu, K.K.; Eisele, D.W. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: Prognostic features of recurrence. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Werning, J.W.; Hinerman, R.W.; Villaret, D.B. Radiotherapy alone or combined with surgery for adenoid cystic carcinoma of the head and neck. Head Neck 2004, 26, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Kokemueller, H.; Eckardt, A.; Brachvogel, P.; Hausamen, J.E. Adenoid cystic carcinoma of the head and neck--a 20 years experience. Int. J. Oral Maxillofac. Surg. 2004, 33, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Sur, R.K.; Donde, B.; Levin, V.; Pacella, J.; Kotzen, J.; Cooper, K.; Hale, M. Adenoid cystic carcinoma of the salivary glands: A review of 10 years. Laryngoscope 1997, 107, 1276–1280. [Google Scholar] [CrossRef]
- Fuwa, N.; Kodaira, T.; Furutani, K.; Tachibana, H.; Nakamura, T. A new method of selective intra-arterial infusion therapy via the superficial temporal artery for head and neck cancer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 783–789. [Google Scholar] [CrossRef]
- Mitsudo, K.; Hayashi, Y.; Minamiyama, S.; Ohashi, N.; Iida, M.; Iwai, T.; Oguri, S.; Koizumi, T.; Kioi, M.; Hirota, M.; et al. Chemoradiotherapy using retrograde superselective intra-arterial infusion for tongue cancer: Analysis of therapeutic results in 118 cases. Oral Oncol. 2018, 79, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Robbins, K.T.; Kumar, P.; Harris, J.; McCulloch, T.; Cmelak, A.; Sofferman, R.; Levine, P.; Weisman, R.; Wilson, W.; Weymuller, E.; et al. Supradose intra-arterial cisplatin and concurrent radiation therapy for the treatment of stage IV head and neck squamous cell carcinoma is feasible and efficacious in a multi-institutional setting: Results of Radiation Therapy Oncology Group Trial 9615. J. Clin. Oncol. 2005, 23, 1447–1454. [Google Scholar] [CrossRef] [PubMed]
- Homma, A.; Sakashita, T.; Hatakeyama, H.; Kano, S.; Mizumachi, T.; Nakamaru, Y.; Yoshida, D.; Onimaru, R.; Tsuchiya, K.; Yasuda, K.; et al. The efficacy of superselective intra-arterial infusion with concomitant radiotherapy for adenoid cystic carcinoma of the head and neck. Acta Otolaryngol. 2015, 135, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Fokas, E.; Kraft, G.; An, H.; Engenhart-Cabillic, R. Ion beam radiobiology and cancer: Time to update ourselves. Biochim. Biophys. Acta 2009, 1796, 216–229. [Google Scholar] [CrossRef] [PubMed]
- Urie, M.M.; Sisterson, J.M.; Koehler, A.M.; Goitein, M.; Zoesman, J. Proton beam penumbra: Effects of separation between patient and beam modifying devices. Med. Phys. 1986, 13, 734–741. [Google Scholar] [CrossRef]
- Takagi, M.; Demizu, Y.; Hashimoto, N.; Mima, M.; Terashima, K.; Fujii, O.; Jin, D.; Niwa, Y.; Morimoto, K.; Akagi, T.; et al. Treatment outcomes of particle radiotherapy using protons or carbon ions as a single-modality therapy for adenoid cystic carcinoma of the head and neck. Radiother. Oncol. 2014, 113, 364–370. [Google Scholar] [CrossRef]
- Koto, M.; Hasegawa, A.; Takagi, R.; Ikawa, H.; Naganawa, K.; Mizoe, J.E.; Jingu, K.; Tsujii, H.; Tsuji, H.; Kamada, T.; et al. Organizing Committee for the Working Group for Head and Neck Cancer. Evaluation of the safety and efficacy of carbon ion radiotherapy for locally advanced adenoid cystic carcinoma of the tongue base. Head Neck 2016, 38, E2122–E2126. [Google Scholar] [CrossRef]
- Namazie, A.; Alavi, S.; Abemayor, E.; Calcaterra, T.C.; Blackwell, K.E. Adenoid cystic carcinoma of the base of the tongue. Ann. Otol. Rhinol. Laryngol. 2001, 110, 248–253. [Google Scholar] [CrossRef]
- Waldron, C.A.; el-Mofty, S.K.; Gnepp, D.R. Tumors of the intraoral minor salivary glands: A demographic and histologic study of 426 cases. Oral Surg. Oral Med. Oral Pathol. 1988, 66, 323–333. [Google Scholar] [CrossRef]
- Huang, M.; Ma, D.; Sun, K.; Yu, G.; Guo, C.; Gao, F. Factors influencing survival rate in adenoid cystic carcinoma of the salivary glands. Int. J. Oral Maxillofac. Surg. 1997, 26, 435–439. [Google Scholar] [CrossRef]
- Bradley, P.J. Adenoid cystic carcinoma of the head and neck: A review. Curr. Opin. Otolaryngol. Head Neck Surg. 2004, 12, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Luna-Ortiz, K.; Carmona-Luna, T.; Cano-Valdez, A.M.; Mosqueda-Taylor, A.; Herrera-Gómez, A.; Villavicencio-Valencia, V. Adenoid cystic carcinoma of the tongue--clinicopathological study and survival analysis. Head Neck Oncol. 2009, 1, 15. [Google Scholar] [CrossRef] [PubMed]
- Vikram, B.; Strong, E.W.; Shah, J.P.; Spiro, R.H. Radiation therapy in adenoid-cystic carcinoma. Int.J. Radiat. Oncol. Biol. Phys. 1984, 10, 221–223. [Google Scholar] [CrossRef]
- Jereczek-Fossa, B.A.; Orecchia, R. Radiotherapy-induced mandibular bone complications. Cancer Treat. Rev. 2002, 28, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Caparrotti, F.; Huang, S.H.; Lu, L.; Bratman, S.V.; Ringash, J.; Bayley, A.; Cho, J.; Giuliani, M.; Kim, J.; Waldron, J.; et al. Osteoradionecrosis of the mandible in patients with oropharyngeal carcinoma treated with intensity-modulated radiotherapy. Cancer 2017, 123, 3691–3700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, C.J.; Hofstede, T.M.; Sturgis, E.M.; Garden, A.S.; Lindberg, M.E.; Wei, Q.; Tucker, S.L.; Dong, L. Osteoradionecrosis and radiation dose to the mandible in patients with oropharyngeal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 415–420. [Google Scholar] [CrossRef] [PubMed]
- MD Anderson Head and Neck Cancer Symptom Working Group; Spatial-Non-spatial Multi-Dimensional Analysis of Radiotherapy Treatment/Toxicity Team (SMART3). Chronic radiation-associated dysphagia in oropharyngeal cancer survivors: Towards age-adjusted dose constraints for deglutitive muscles. Clin. Transl. Radiat. Oncol. 2019, 18, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triantafillidou, K.; Dimitrakopoulos, J.; Iordanidis, F.; Koufogiannis, D. Management of adenoid cystic carcinoma of minor salivary glands. J. Oral Maxillofac. Surg. 2006, 64, 1114–1120. [Google Scholar] [CrossRef]
- Sagardoy, T.; Fernandez, P.; Ghafouri, A.; Digue, L.; Haaser, T.; de Clermont-Galleran, H.; Castetbon, V.; de Monès, E. Accuracy of (18) FDG PET-CT for treatment evaluation 3 months after completion of chemoradiotherapy for head and neck squamous cell carcinoma: 2-year minimum follow-up. Head Neck 2016, 38, E1271–E1276. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, 8th ed.; John Wiley & Sons, LTD: New York, NY, USA, 2017. [Google Scholar]
- Fowler, J.F. 21 years of biologically effective dose. Br. J. Radiol. 2010, 83, 554–568. [Google Scholar] [CrossRef]
- Nakamura, T.; Fuwa, N.; Takayama, K.; Tomoda, T.; Takada, A.; Makita, C.; Shiomi, M.; Yokouchi, J.; Watanabe, K. A new method MRI to delineate areas of head and neck cancer targeted by intra-arterial infusion via a superficial temporal artery. Oral Oncol. 2011, 47, 387–390. [Google Scholar] [CrossRef] [PubMed]
- NCI Common Termiology Criteria for Adverse Events (CTCAE) V4.0 Data Files. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf (accessed on 10 August 2019).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n or Median (% or Range) |
|---|---|
| Number of patients | 15 |
| Age, years | 60 (31–78) |
| Sex | |
| Male | 5 (33) |
| Female | 10 (67) |
| ECOG-PS | |
| 0 | 10 (67) |
| 1 | 5 (33) |
| T classification * | |
| T3 | 1 (7) |
| T4a | 12 (80) |
| T4b | 2 (13) |
| N classification * | |
| N0 | 9 (60) |
| N1 | 2 (13) |
| N2b | 2 (13) |
| N2c | 2 (13) |
| M classification * | |
| M0 | 10 (67) |
| M1 | 5 (33) |
| Stage | |
| IVA | 9 (60) |
| IVB | 1(7) |
| IVC | 5 (33) |
| Location | |
| Right | 9 (60) |
| Left | 6 (40) |
| FDG accumulation before treatment | 7.3 (1–12.5) |
| Reasons for not performing surgery | |
| Operabl | |
| Refusal | 6 (40) |
| Old age | 1 (7) |
| Inoperable | |
| Locally advanced | 3 (20) |
| Distant metastasis | 2 (13) |
| Locally advanced + distant metastasis | 3 (20) |
| Characteristics | n or Median (% or Range) |
|---|---|
| GTV | 50 (21–120) mL |
| PTV | 160 (75–331) mL |
| Prescribed dose | |
| 61.6 Gy (RBE)/28 fr. | 1 (7) |
| 66.0 Gy (RBE)/30 fr. | 4 (26) |
| 70.4 Gy (RBE)/32 fr. | 4 (26) |
| 72.6 Gy (RBE)/33 fr. | 1 (7) |
| others | 5 (33) |
| Total radiation dose | |
| BED10 | 84.4 (75.2–88.6) Gy (RBE) |
| BED3 | 119.1 (106.8–125.8) Gy (RBE) |
| EQD10/2 | 70.3 (62.6–73.8) Gy (RBE) |
| EQD3/2 | 71.5 (64.1–75.5) Gy (RBE) |
| Total dose of cisplatin on IAIC | 410 (200–580) mg |
| Arterial injection vessels | |
| LA + ECA | 6 (40) |
| LA | 1 (7) |
| ECA | 8 (53) |
| Nutrition | |
| PEG | 6 (40) |
| Oral intake | 5 (33) |
| Naso-gastric tube | 4 (26) |
| Factors | No. of Patients | p Value | |
|---|---|---|---|
| OS | LC | ||
| Age | 0.790 | 0.264 | |
| <60 years | 7 | ||
| ≥60 years | 8 | ||
| Sex | 0.430 | 0.724 | |
| Male | 5 | ||
| Female | 10 | ||
| Surgical indication | 0.720 | 0.264 | |
| Operable | 7 | ||
| Inoperable | 8 | ||
| Primary tumor size (GTV) | 0.744 | 0.264 | |
| <50 mL | 7 | ||
| ≥50 mL | 8 | ||
| Irradiation volume (PTV) | 0.835 | 0.264 | |
| <160 mL | 7 | ||
| ≥160 mL | 8 | ||
| Lymph node status | 0.157 | 0.264 | |
| Negative | 9 | ||
| Positive | 6 | ||
| Lung metastasis before treatment | 0.007 * | 0.061 | |
| Negative | 10 | ||
| Positive | 5 | ||
| SUVmax value on PET | 0.284 | 0.371 | |
| <7.3 | 8 | ||
| ≥7.3 | 7 | ||
| Reduction of SUVmax after treatment | 0.364 | 0.371 | |
| <5.9 | 7 | ||
| ≥5.9 | 8 | ||
| Total dose; EQD10/2 (GyE10/2) | 0.664 | 0.371 | |
| <70.3 Gy (RBE) | 8 | ||
| ≥70.3 Gy (RBE) | 7 | ||
| Total dose of cisplatin on IAIC | 0.607 | 0.264 | |
| <410 mg | 7 | ||
| ≥410 mg | 8 | ||
| Toxicity, maximum/latest | Grade, n | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Mucositis oral | 0/2 | 3/0 | 12/0 | 0 | 0 |
| Dermatitis radiation | 4/0 | 6/0 | 3/0 | 0 | 0 |
| Neutropenia | 0 | 6/0 | 2/0 | 0 | 0 |
| Anemia | 0 | 2/0 | 1/0 | 0 | 0 |
| Platelet count decreased | 0 | 1/0 | 0 | 0 | 0 |
| Nausea | 6/0 | 4/0 | 0 | - | - |
| Acute kidney injury | 0 | 0 | 0 | 0 | 0 |
| Hepatobiliary disorders | 1/0 | 0 | 0 | 0 | 0 |
| Dry mouth | 7/3 | 2/0 | 0 | - | - |
| Dysgeusia | 9/4 | 6/0 | - | - | - |
| Laryngeal edema | 3/0 | 0 | 0 | 0 | 0 |
| Dysarthria | 3/1 | 2/1 | 0 | - | - |
| Dysphagia | 4/2 | 2/1 | 2/0 | 1/1 | 0 |
| Pharyngeal mucositis or ulcer | 10/4 | 3/0 | 2/0 | 0 | 0 |
| Pharyngeal necrosis | - | - | 0 | 0 | 1/1 |
| Osteonecrosis of jaw | 0 | 1/0 | 0 | 0 | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takayama, K.; Kato, T.; Nakamura, T.; Azami, Y.; Ono, T.; Suzuki, M.; Takada, A.; Yamaguchi, H.; Seto, I.; Nakasato, T.; et al. Proton Beam Therapy Combined with Intra-Arterial Infusion Chemotherapy for Stage IV Adenoid Cystic Carcinoma of the Base of the Tongue. Cancers 2019, 11, 1413. https://doi.org/10.3390/cancers11101413
Takayama K, Kato T, Nakamura T, Azami Y, Ono T, Suzuki M, Takada A, Yamaguchi H, Seto I, Nakasato T, et al. Proton Beam Therapy Combined with Intra-Arterial Infusion Chemotherapy for Stage IV Adenoid Cystic Carcinoma of the Base of the Tongue. Cancers. 2019; 11(10):1413. https://doi.org/10.3390/cancers11101413
Chicago/Turabian StyleTakayama, Kanako, Takahiro Kato, Tatsuya Nakamura, Yusuke Azami, Takashi Ono, Motohisa Suzuki, Akinori Takada, Hisashi Yamaguchi, Ichiro Seto, Tatsuhiko Nakasato, and et al. 2019. "Proton Beam Therapy Combined with Intra-Arterial Infusion Chemotherapy for Stage IV Adenoid Cystic Carcinoma of the Base of the Tongue" Cancers 11, no. 10: 1413. https://doi.org/10.3390/cancers11101413