Morpho-Molecular Assessment Indicates New Prognostic Aspects and Personalized Therapeutic Options in Sinonasal Melanoma

 , ,
, ,
Abstract
:1. Introduction
2. Results
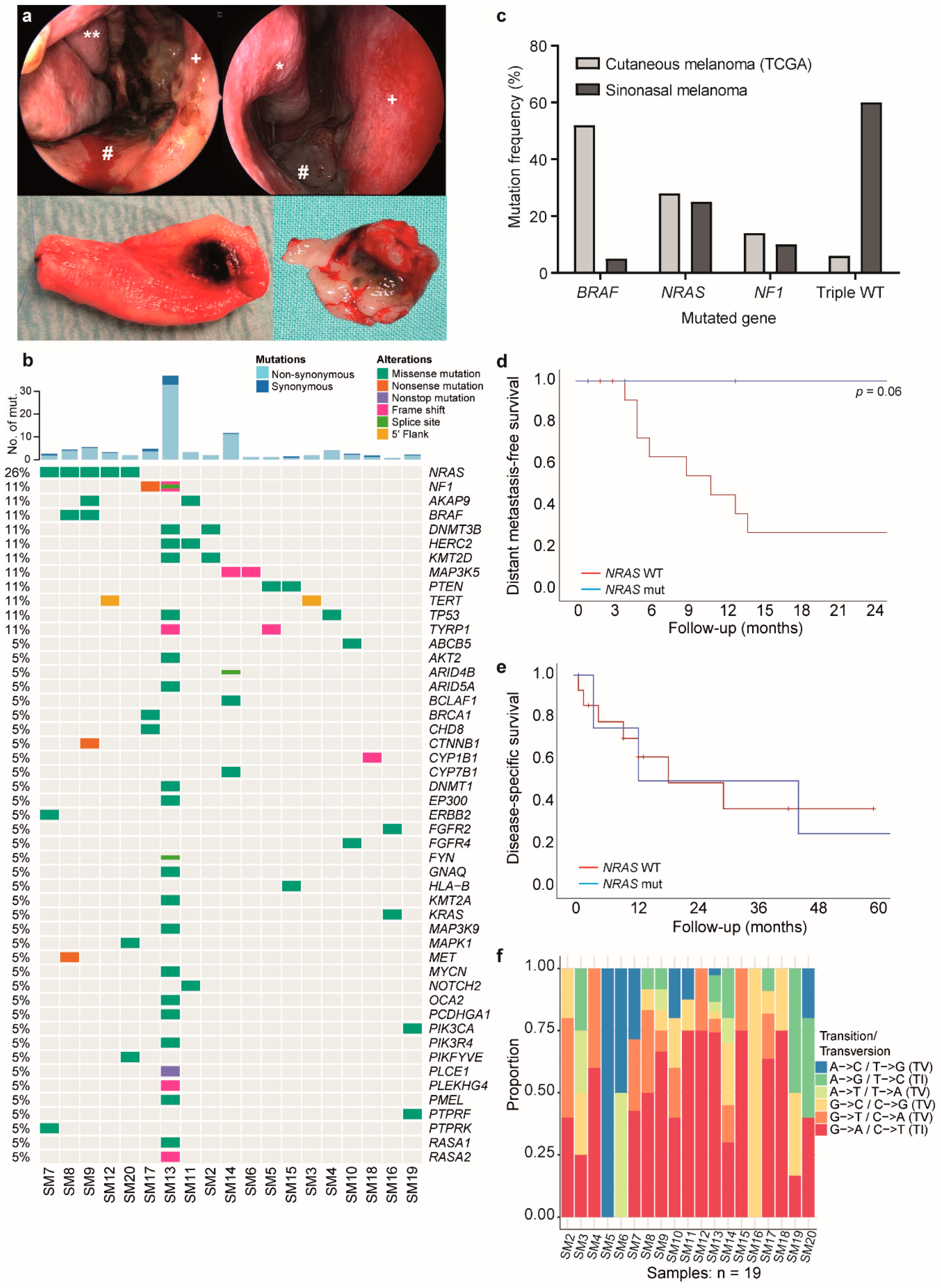
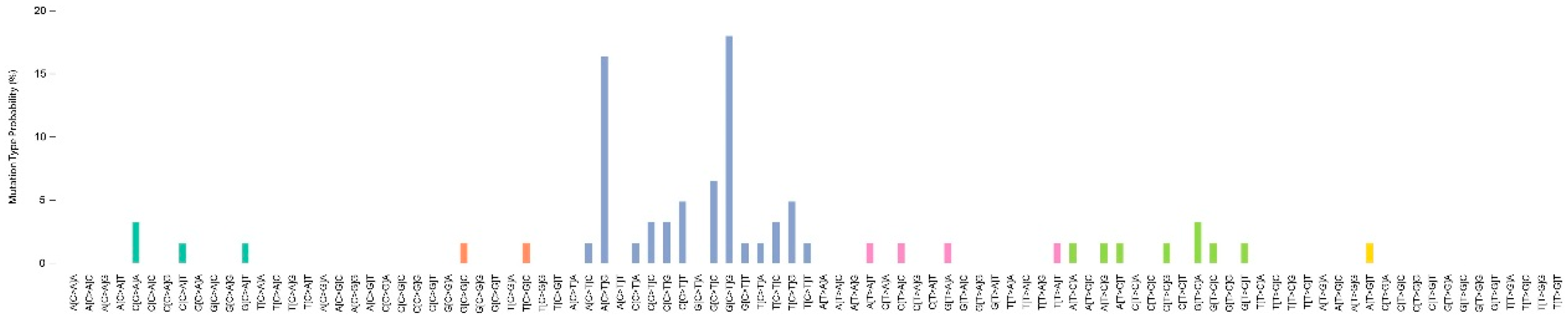
2.1. Mutation Analysis Reveals a Generally Low Mutational Burden with NRAS Mutation as the Most Frequent Driver
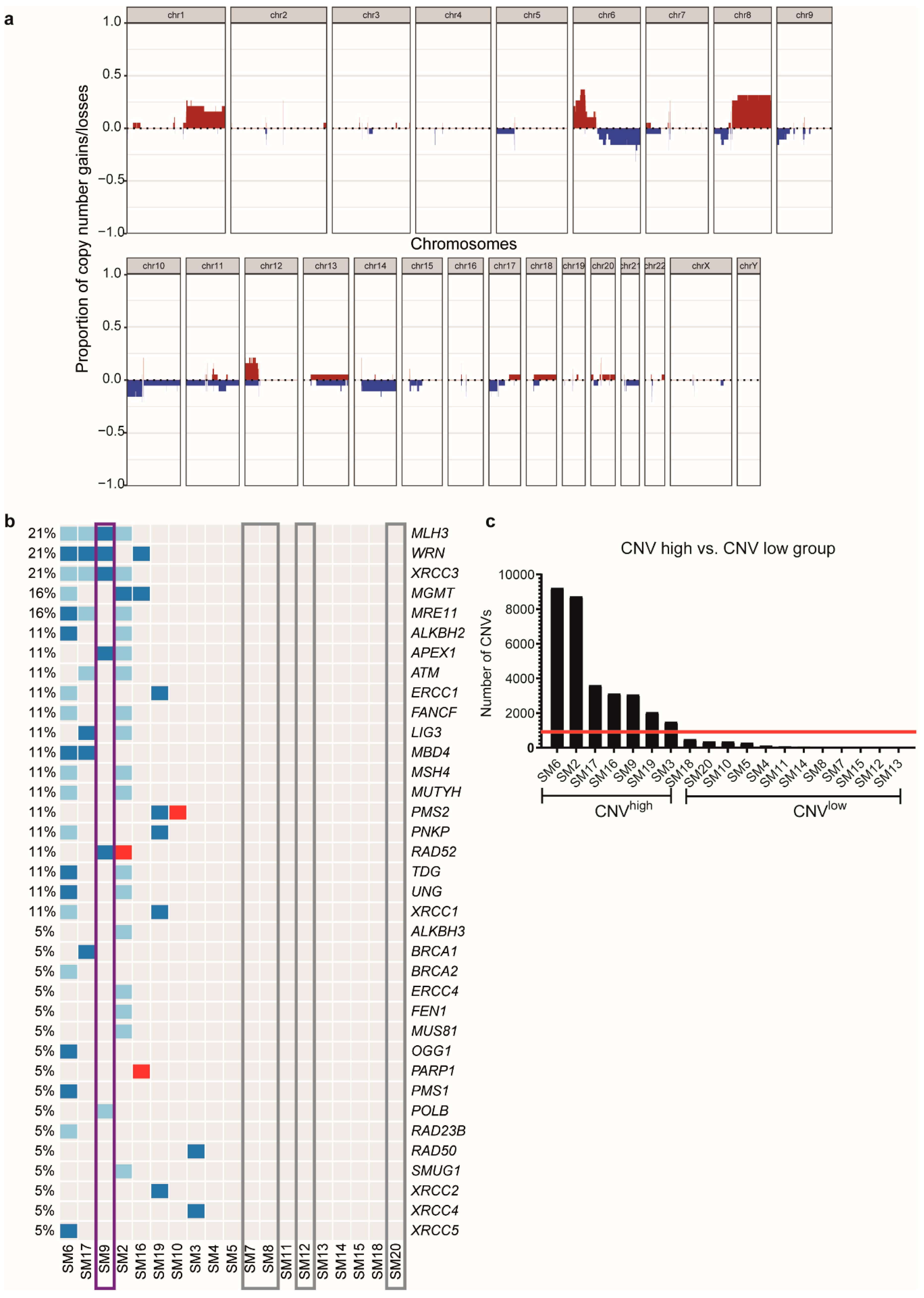
2.2. Presence or Absence of DNA Repair Gene Alterations Divide the Cohort into Different Groups
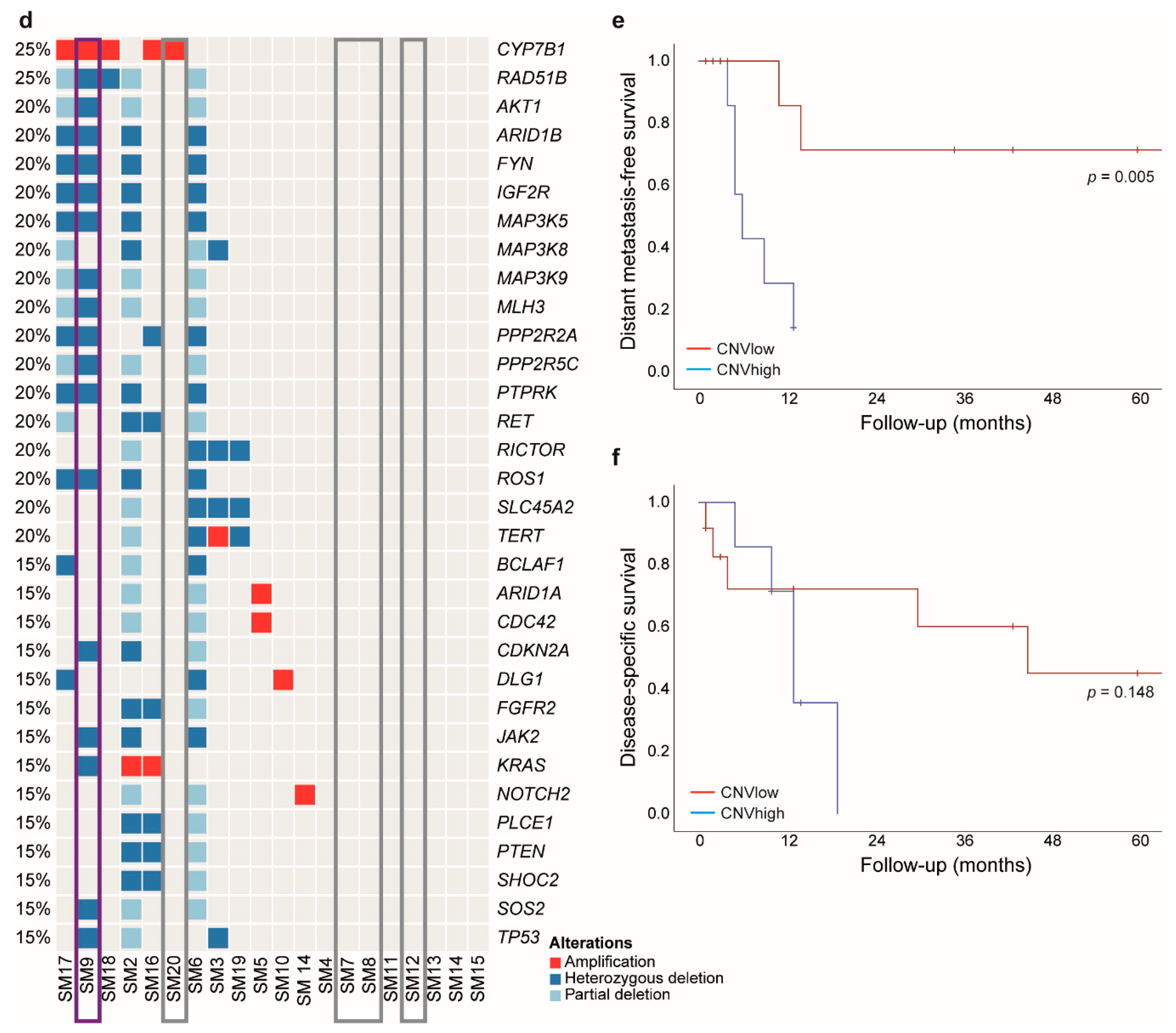
2.3. Low CNV Numbers Are Associated with NRAS Mutations and Prolonged Distant Metastasis-Free Survival
2.4. Fusions
2.5. Oncogenic Alterations Are Mostly Associated with MAPK or PI3K/mTOR Pathway
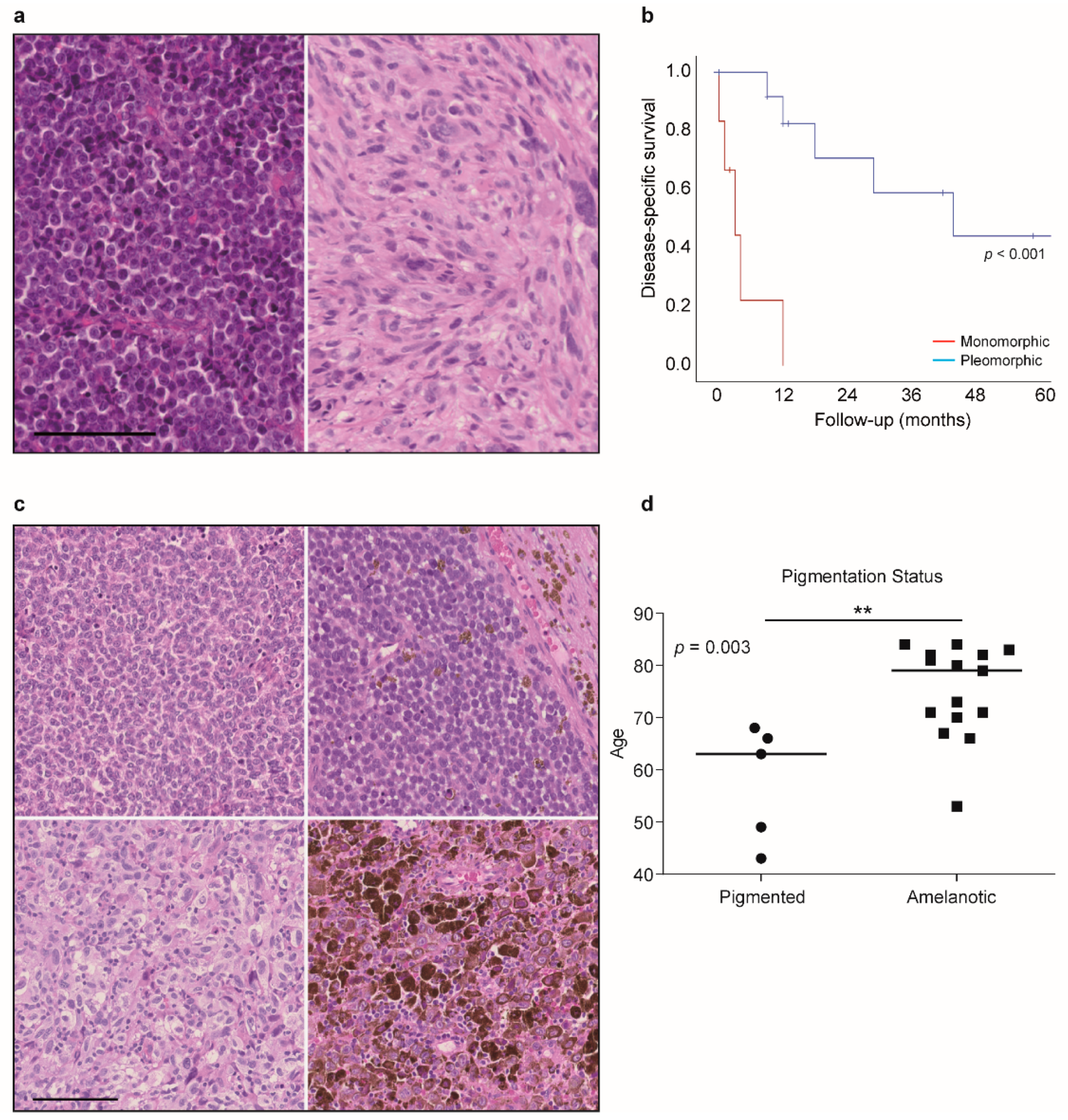
2.6. Histological Evaluation Shows an Association of Monomorphic Features with Worse Outcome
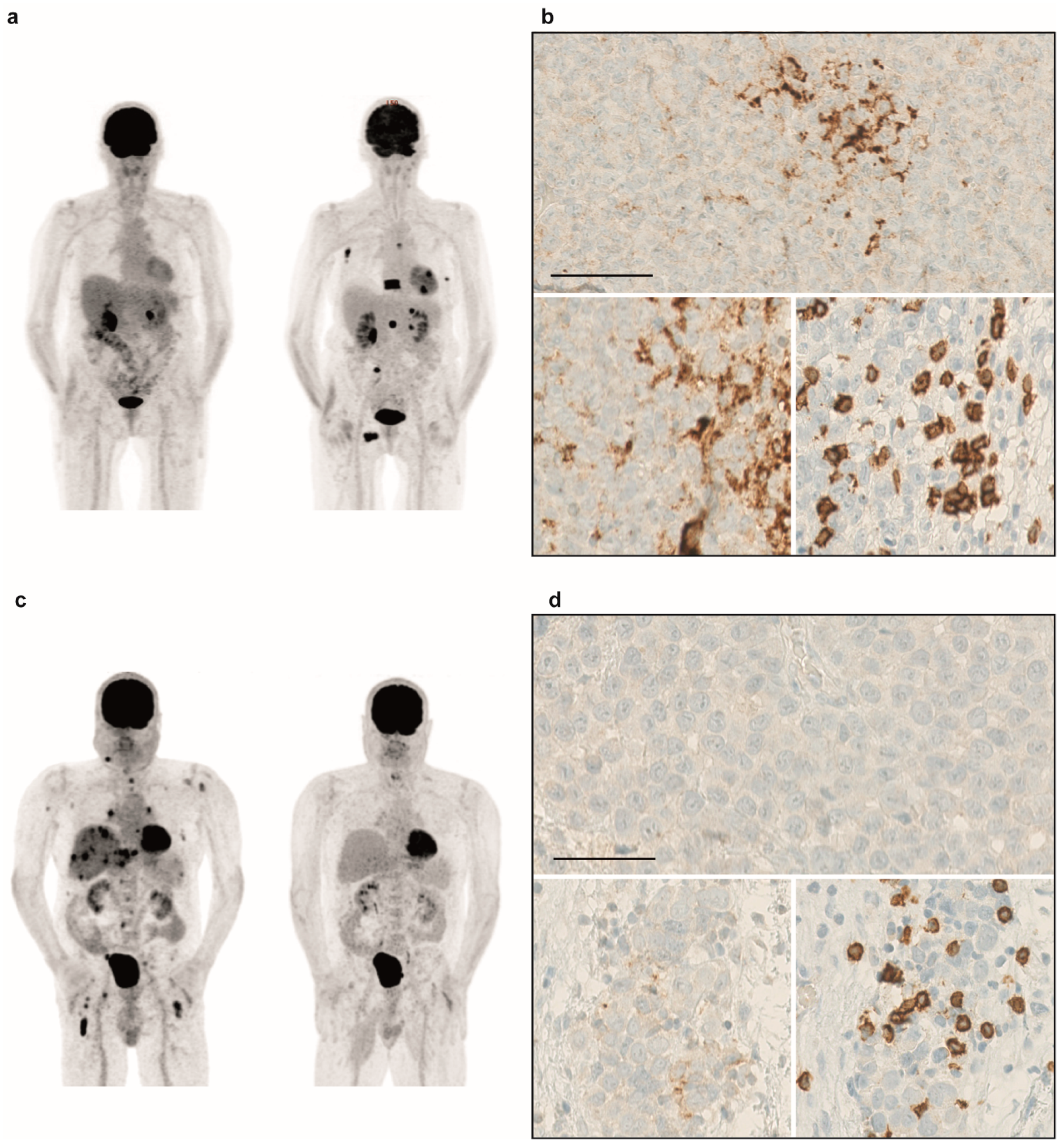
2.7. Immunohistochemistry Reveals Mostly PD-L1 Negativity and Infiltration of T-Cells
2.8. Immunotherapy is an Option for Sinonasal Melanoma Patients
2.9. Molecular Alterations Provide Opportunities to Experimental Therapy
3. Discussion
4. Materials and Methods
4.1. Patient Samples
4.2. Collection of Clinical Data
4.3. Sample Preparation
4.4. DNA Isolation
4.5. Library Preparation
4.6. Sequencing
4.7. Analysis
4.8. (Immuno-)Histological Staining and Evaluation
4.9. Statistics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Torres-Cabala, C.A.; Wang, W.-L.; Trent, J.; Yang, D.; Chen, S.; Galbincea, J.; Kim, K.B.; Woodman, S.; Davies, M.; Plaza, J.A.; et al. Correlation between KIT expression and KIT mutation in melanoma: A study of 173 cases with emphasis on the acral-lentiginous/mucosal type. Mod. Pathol. 2009, 22, 1446–1456. [Google Scholar] [CrossRef] [PubMed]
- Schoenewolf, N.L.; Bull, C.; Belloni, B.; Holzmann, D.; Tonolla, S.; Lang, R.; Mihic-Probst, D.; Andres, C.; Dummer, R. Sinonasal, genital and acrolentiginous melanomas show distinct characteristics of KIT expression and mutations. Eur. J. Cancer 2012, 48, 1842–1852. [Google Scholar] [CrossRef] [PubMed]
- Del Prete, V.; Chaloupka, K.; Holzmann, D.; Fink, D.; Levesque, M.; Dummer, R.; Goldinger, S.M. Noncutaneous Melanomas: A Single-Center Analysis. Dermatology 2016, 232, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Turri-Zanoni, M.; Medicina, D.; Lombardi, D.; Ungari, M.; Balzarini, P.; Rossini, C.; Pellegrini, W.; Battaglia, P.; Capella, C.; Castelnuovo, P.; et al. Sinonasal mucosal melanoma: Molecular profile and therapeutic implications from a series of 32 cases. Head Neck 2013, 35, 1066–1077. [Google Scholar] [CrossRef] [PubMed]
- Chraybi, M.; Alsamad, I.A.; Copie-Bergman, C.; Baia, M.; André, J.; Dumaz, N.; Ortonne, N. Oncogene abnormalities in a series of primary melanomas of the sinonasal tract: NRAS mutations and cyclin D1 amplification are more frequent than KIT or BRAF mutations. Hum. Pathol. 2013, 44, 1902–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zebary, A.; Jangard, M.; Omholt, K.; Ragnarsson-Olding, B.; Hansson, J. KIT, NRAS and BRAF mutations in sinonasal mucosal melanoma: A study of 56 cases. Br. J. Cancer 2013, 109, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Ozturk Sari, S.; Yilmaz, I.; Taskin, O.C.; Narli, G.; Sen, F.; Comoglu, S.; Firat, P.; Bİlgİç, B.; Yilmazbayhan, D.; Ozluk, Y.; et al. BRAF, NRAS, KIT, TERT, GNAQ/GNA11 mutation profile analysis of head and neck mucosal melanomas: A study of 42 cases. Pathology 2017, 49, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Jangard, M.; Zebary, A.; Ragnarsson-Olding, B.; Hansson, J. TERT promoter mutations in sinonasal malignant melanoma: A study of 49 cases. Melanoma Res. 2015, 25, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Amit, M.; Tam, S.; Abdelmeguid, A.S.; Roberts, D.B.; Takahashi, Y.; Raza, S.M.; Su, S.Y.; Kupferman, M.E.; Demonte, F.; Hanna, E.Y. Mutation status among patients with sinonasal mucosal melanoma and its impact on survival. Br. J. Cancer 2017, 116, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Cosgarea, I.; Ugurel, S.; Sucker, A.; Livingstone, E.; Zimmer, L.; Ziemer, M.; Utikal, J.; Mohr, P.; Pfeiffer, C.; Pföhler, C.; et al. Targeted next generation sequencing of mucosal melanomas identifies frequent NF1 and RAS mutations. Oncotarget 2017, 8, 40683–40692. [Google Scholar] [CrossRef] [PubMed]
- Wroblewska, J.P.; Mull, J.; Wu, C.L.; Fujimoto, M.; Ogawa, T.; Marszalek, A.; Hoang, M.P. SF3B1, NRAS, KIT, and BRAF Mutation; CD117 and cMYC Expression; and Tumoral Pigmentation in Sinonasal Melanomas: An Analysis with Newly Found Molecular Alterations and Some Population-Based Molecular Differences. Am. J. Surg. Pathol. 2019, 43, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, G.C.; Falzone, L.; Salemi, R.; Zanghi, A.; Spandidos, D.A.; McCubrey, J.A.; Candido, S.; Libra, M. Cutaneous melanoma: From pathogenesis to therapy (Review). Int. J. Oncol. 2018, 52, 1071–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amit, M.; Na’Ara, S.; Hanna, E.Y. Contemporary Treatment Approaches to Sinonasal Mucosal Melanoma. Curr. Oncol. Rep. 2018, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Dummer, R.; Keilholz, U.; Committee, E.G. Appendix 2: Cutaneous melanoma (2): EUpdate published online September 2016 (http://www.esmo.org/Guidelines/Melanoma). Ann. Oncol. 2016, 27, v136–v137. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Accorona, R.; Botti, G.; Farina, D.; Fossati, P.; Gatta, G.; Gogas, H.; Lombardi, D.; Maroldi, R.; Nicolai, P.; et al. Mucosal melanoma of the head and neck. Crit. Rev. Oncol. 2017, 112, 136–152. [Google Scholar] [CrossRef] [PubMed]
- Krauthammer, M.; Kong, Y.; Bacchiocchi, A.; Evans, P.; Pornputtapong, N.; Wu, C.; McCusker, J.P.; Ma, S.; Cheng, E.; Straub, R.; et al. Exome sequencing identifies recurrent mutations in NF1 and RASopathy genes in sun-exposed melanomas. Nat. Genet. 2015, 47, 996–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halaban, R.; Krauthammer, M. RASopathy Gene Mutations in Melanoma. J. Investig. Dermatol. 2016, 136, 1755–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayward, N.K.; Wilmott, J.S.; Waddell, N.; Johansson, P.A.; Field, M.A.; Nones, K.; Patch, A.-M.; Kakavand, H.; Alexandrov, L.B.; Burke, H.; et al. Whole-genome landscapes of major melanoma subtypes. Nature 2017, 545, 175–180. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Network. Genomic Classification of Cutaneous Melanoma. Cell 2015, 161, 1681–1696. [Google Scholar] [CrossRef]
- Hodis, E.; Watson, I.R.; Kryukov, G.V.; Arold, S.T.; Imielinski, M.; Theurillat, J.-P.; Nickerson, E.; Auclair, D.; Li, L.; Place, C.; et al. A Landscape of Driver Mutations in Melanoma. Cell 2012, 150, 251–263. [Google Scholar] [CrossRef] [Green Version]
- Beadling, C.; Jacobson-Dunlop, E.; Hodi, F.S.; Le, C.; Warrick, A.; Patterson, J.; Town, A.; Harlow, A.; Cruz, F.; Azar, S.; et al. KIT Gene Mutations and Copy Number in Melanoma Subtypes. Clin. Cancer Res. 2008, 14, 6821–6828. [Google Scholar] [CrossRef] [PubMed]
- Iida, Y.; Salomon, M.P.; Hata, K.; Tran, K.; Ohe, S.; Griffiths, C.F.; Hsu, S.C.; Nelson, N.; Hoon, D.S.B. Predominance of triple wild-type and IGF2R mutations in mucosal melanomas. BMC Cancer 2018, 18, 1054. [Google Scholar] [CrossRef] [PubMed]
- Onken, M.D.; Worley, L.A.; Long, M.D.; Duan, S.; Council, M.L.; Bowcock, A.M.; Harbour, J.W. Oncogenic mutations in GNAQ occur early in uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5230–5234. [Google Scholar] [CrossRef] [PubMed]
- Cirenajwis, H.; Lauss, M.; Ekedahl, H.; Törngren, T.; Kvist, A.; Saal, L.H.; Olsson, H.; Staaf, J.; Carneiro, A.; Ingvar, C.; et al. NF1-mutated melanoma tumors harbor distinct clinical and biological characteristics. Mol. Oncol. 2017, 11, 438–451. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Siepmann, T.; Engel, J.; Schubert-Fritschle, G.; Eckel, R.; Mirlach, L.; Kirchner, T.; Jung, A.; Gesierich, A.; Ruzicka, T.; et al. Prognostic significance of BRAF and NRAS mutations in melanoma: A German study from routine care. BMC Cancer 2017, 17, 536. [Google Scholar] [CrossRef] [PubMed]
- Devitt, B.; Liu, W.; Salemi, R.; Wolfe, R.; Kelly, J.; Tzen, C.-Y.; Dobrovic, A.; McArthur, G. Clinical outcome and pathological features associated with NRAS mutation in cutaneous melanoma. Pigment. Cell Melanoma Res. 2011, 24, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Curtin, J.A.; Fridlyand, J.; Kageshita, T.; Patel, H.N.; Busam, K.J.; Kutzner, H.; Cho, K.-H.; Aiba, S.; Bröcker, E.-B.; LeBoit, P.E.; et al. Distinct Sets of Genetic Alterations in Melanoma. N. Engl. J. Med. 2005, 353, 2135–2147. [Google Scholar] [CrossRef]
- Van Dijk, M.; Sprenger, S.; Rombout, P.; Marres, H.; Kaanders, J.; Jeuken, J.; Ruiter, D. Distinct chromosomal aberrations in sinonasal mucosal melanoma as detected by comparative genomic hybridization. Genes Chromosomes Cancer 2003, 36, 151–158. [Google Scholar] [CrossRef]
- Kulkarni, A.; Al-Hraishawi, H.; Simhadri, S.; Hirshfield, K.M.; Chen, S.; Pine, S.; Jeyamohan, C.; Sokol, L.; Ali, S.; Teo, M.L.; et al. BRAF Fusion as a Novel Mechanism of Acquired Resistance to Vemurafenib in BRAF V600E Mutant Melanoma. Clin. Cancer Res. 2017, 23, 5631–5638. [Google Scholar] [CrossRef]
- Turner, J.; Couts, K.; Sheren, J.; Saichaemchan, S.; Ariyawutyakorn, W.; Avolio, I.; Cabral, E.; Glogowska, M.; Amato, C.; Robinson, S.; et al. Kinase Gene Fusions in Defined Subsets of Melanoma. Pigment. Cell Melanoma Res. 2017, 30, 53–62. [Google Scholar] [CrossRef]
- Mateo, J.; Carreira, S.; Sandhu, S.; Miranda, S.; Mossop, H.; Perez-Lopez, R.; Rodrigues, D.N.; Robinson, D.; Omlin, A.; Tunariu, N.; et al. DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer. N. Engl. J. Med. 2015, 373, 1697–1708. [Google Scholar] [CrossRef] [PubMed]
- Nissan, M.H.; Pratilas, C.A.; Jones, A.M.; Ramirez, R.; Won, H.; Liu, C.; Tiwari, S.; Kong, L.; Hanrahan, A.J.; Yao, Z.; et al. Loss of NF1 in cutaneous melanoma is associated with RAS activation and MEK dependence. Cancer Res. 2014, 74, 2340–2350. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Zou, B.; Wang, S. Clinicopathological Features and Prognosis of Sinonasal Mucosal Malignant Melanoma: A Retrospective Study of 83 Cases in a Chinese Population. ORL 2016, 78, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.E.; Kricker, A.; Waxweiler, W.T.; Dillon, P.M.; Busam, K.J.; From, L.; Groben, P.A.; Armstrong, B.K.; Anton-Culver, H.; Gruber, S.B.; et al. Comparison of Clinicopathologic Features and Survival of Histopathologically Amelanotic and Pigmented Melanomas: A Population-Based Study. JAMA Dermatol. 2014, 150, 1306–1314. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Hodi, F.S.; Wolchok, J.D. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 1270–1271. [Google Scholar] [CrossRef] [PubMed]
- Straub, M.; Drecoll, E.; Pfarr, N.; Weichert, W.; Langer, R.; Hapfelmeier, A.; Götz, C.; Wolff, K.-D.; Kolk, A.; Specht, K. CD274/PD-L1 gene amplification and PD-L1 protein expression are common events in squamous cell carcinoma of the oral cavity. Oncotarget 2016, 7, 12024–12034. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.G.; Mary, K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2017. [Google Scholar]
- Freiberger, S.N.; Cheng, P.; Pornputtapong, N.; Turko, P.; Kong, Y.; Irmisch, A.; Khan, M.; Halaban, R.; Dummer, R.; Wild, P.J. MelArray: An integrated targeted sequencing panel to assess mutations, copy number, structural variants, and immunological features in melanoma for clinical decision support. unpublished, manuscript in preparation.
- Jiang, H.; Lei, R.; Ding, S.-W.; Zhu, S. Skewer: A fast and accurate adapter trimmer for next-generation sequencing paired-end reads. BMC Bioinform. 2014, 15, 182. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Durbin, R. Fast and accurate short read alignment with Burrows–Wheeler transform. Bioinformatics 2009, 25, 1754–1760. [Google Scholar] [CrossRef] [PubMed]
- Cibulskis, K.; Lawrence, M.S.; Carter, S.L.; Sivachenko, A.; Jaffe, D.; Sougnez, C.; Gabriel, S.; Meyerson, M.; Lander, E.S.; Getz, G. Sensitive detection of somatic point mutations in impure and heterogeneous cancer samples. Nat. Biotechnol. 2013, 31, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Favero, F.; Joshi, T.; Marquard, A.M.; Birkbak, N.J.; Krzystanek, M.; Li, Q.; Szallasi, Z.; Eklund, A.C. Sequenza: Allele-specific copy number and mutation profiles from tumor sequencing data. Ann. Oncol. 2015, 26, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Rupp, N.J.; Rechsteiner, M.; Freiberger, S.N.; Lenggenhager, D.; Urosevic, M.; Burger, I.A.; Rushing, E.J.; Mihic-Probst, D. New observations in tumor cell plasticity: Mutational profiling in a case of metastatic melanoma with biphasic sarcomatoid transdifferentiation. Virchows Arch. 2018, 473, 517–521. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Alteration | Pathway/Function |
|---|---|---|
| SM2 | KRAS amplification, NF1/PTEN/CDKN2A loss | MAPK pathway, PI3K/mTOR pathway, cell cycle |
| SM3 | TP53 loss | Tumor suppressor |
| SM4 | TP53 p.Arg273Cys (subclonal) | Tumor suppressor |
| SM5 | PTEN p.Leu108Arg | PI3K/mTOR pathway |
| SM6 | MAP3K5 p.Gly39AlafsTer142 (subclonal), MAP3K5/PTEN/CDKN2A loss | p38 pathway, PI3K/mTOR pathway, cell cycle |
| SM7 | NRAS p.Gln61His | MAPK pathway |
| SM8 | NRAS p.Gly61Lys | MAPK pathway |
| SM9 | BRAF p.Asp594Asn, NRAS p.Gly12Asp, TP53/CDKN2A loss | MAPK pathway, pathway cell cycle |
| SM10 | - | - |
| SM11 | - | - |
| SM12 | NRAS p.Gln61Lys, TERT prom. -124C>T | MAPK pathway |
| SM13 | NF1 p.Leu307Ter | MAPK pathway |
| SM14 | MAP3K5 p.Pro47ValfsTer56, MAP3K5 p.Gly39AlafsTer142 (both subclonal) | p38 pathway |
| SM15 | PTEN p.Arg74Ile (subclonal) | PI3K/mTOR pathway |
| SM16 | KRAS p.Gly12Ala, KRAS amplification, PTEN loss | MAPK pathway, PI3K/mTOR pathway |
| SM17 | NF1 p.Gln1520Ter, NF1 loss, BRCA1 loss, BRCA1 predictive damaging VUS | MAPK pathway, DNA repair |
| SM18 | - | - |
| SM19 | PIK3CA p.Glu545Gly | PI3K/mTOR pathway |
| SM20 | NRAS p.Gln61Arg | MAPK pathway |
| Sample | Pigmentation Status | S100 | HMB-45 | MelanA | SOX10 |
|---|---|---|---|---|---|
| SM2 | pigmented | + | N/D | + | N/D |
| SM3 | amelanotic | + | N/D | + | N/D |
| SM4 | amelanotic | (+) | + | + | N/D |
| SM5 | amelanotic | + | N/D | + | N/D |
| SM6 | pigmented | + | N/D | + | N/D |
| SM7 | amelanotic | + | (+) | + | N/D |
| SM8 | amelanotic | + | (+) | + | N/D |
| SM9 | amelanotic | + | (+) | + | N/D |
| SM10 | amelanotic | + | + | + | N/D |
| SM11 | amelanotic | − | + | (+) | + |
| SM12 | pigmented | + | N/D | + | N/D |
| SM13 | pigmented | + | + | + | N/D |
| SM14 | amelanotic | + | + | + | N/D |
| SM15 | amelanotic | + | + | + | N/D |
| SM16 | amelanotic | (+) | + | (+) | + |
| SM17 | amelanotic | + | + | + | N/D |
| SM18 | amelanotic | + | + | + | N/D |
| SM19 | pigmented | + | + | + | N/D |
| SM20 | pigmented | + | + | + | N/D |
| Characteristics | Distribution in the cohort |
|---|---|
| Gender | n (%) |
| Male | 8 (42%) |
| Female | 11 (58%) |
| Age at diagnosis | Median (range) |
| Male | 72 (53–84) |
| Female | 71 (49–84) |
| Total | 71 (43–84) |
| Clinical classification of the tumor | n (%) |
| T3 | 11 (58%) |
| T4 | 8 (42%) |
| Pigmentation status of primary tumor | n (%) |
| Pigmented | 6 (32%) |
| Amelanotic | 13 (68%) |
| Morphology of primary tumor | n (%) |
| Monomorphic | 6 (32%) |
| Pleomorphic | 13 (68%) |
| Distant Metastasis-Free Survival | Disease-Specific Survival | |||
|---|---|---|---|---|
| Median (SE) | p-Value | Median (SE) | p-Value | |
| NRAS Status | ||||
| WT | 13.1 | 0.049 | 19.0 (10.7) | 0.921 |
| Mutated | 60.0 | 13.0 (20.5) | ||
| CNV Status | ||||
| CNVhigh | -(-) | 0.005 | 13.0 (1.6) | 0.148 |
| CNVlow | 6.0 (1.3) | 45.0 (17.95) | ||
| Morphology | ||||
| Monomorphic | 5.0 (-) | 0.941 | 4.0 (2.0) | 0.000082 |
| Pleomorphic | 13.0 (2.6) | 45.0 (17.95) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freiberger, S.N.; Morand, G.B.; Turko, P.; Wager, U.; Dummer, R.; Hüllner, M.; Holzmann, D.; Rupp, N.J.; Levesque, M.P. Morpho-Molecular Assessment Indicates New Prognostic Aspects and Personalized Therapeutic Options in Sinonasal Melanoma. Cancers 2019, 11, 1329. https://doi.org/10.3390/cancers11091329
Freiberger SN, Morand GB, Turko P, Wager U, Dummer R, Hüllner M, Holzmann D, Rupp NJ, Levesque MP. Morpho-Molecular Assessment Indicates New Prognostic Aspects and Personalized Therapeutic Options in Sinonasal Melanoma. Cancers. 2019; 11(9):1329. https://doi.org/10.3390/cancers11091329
Chicago/Turabian StyleFreiberger, Sandra N., Grégoire B. Morand, Patrick Turko, Ulrich Wager, Reinhard Dummer, Martin Hüllner, David Holzmann, Niels J. Rupp, and Mitchell P. Levesque. 2019. "Morpho-Molecular Assessment Indicates New Prognostic Aspects and Personalized Therapeutic Options in Sinonasal Melanoma" Cancers 11, no. 9: 1329. https://doi.org/10.3390/cancers11091329