Skeletal Metastases of Unknown Primary: Biological Landscape and Clinical Overview

 , , , and
, , , and
Abstract
:1. Introduction
2. Cancer Cell Homing to the Bone Marrow: Bridging the Gap Between the Malignancy and the Neighborhood
2.1. The Biological Landscape of Cancer Cells of Unknown Primary
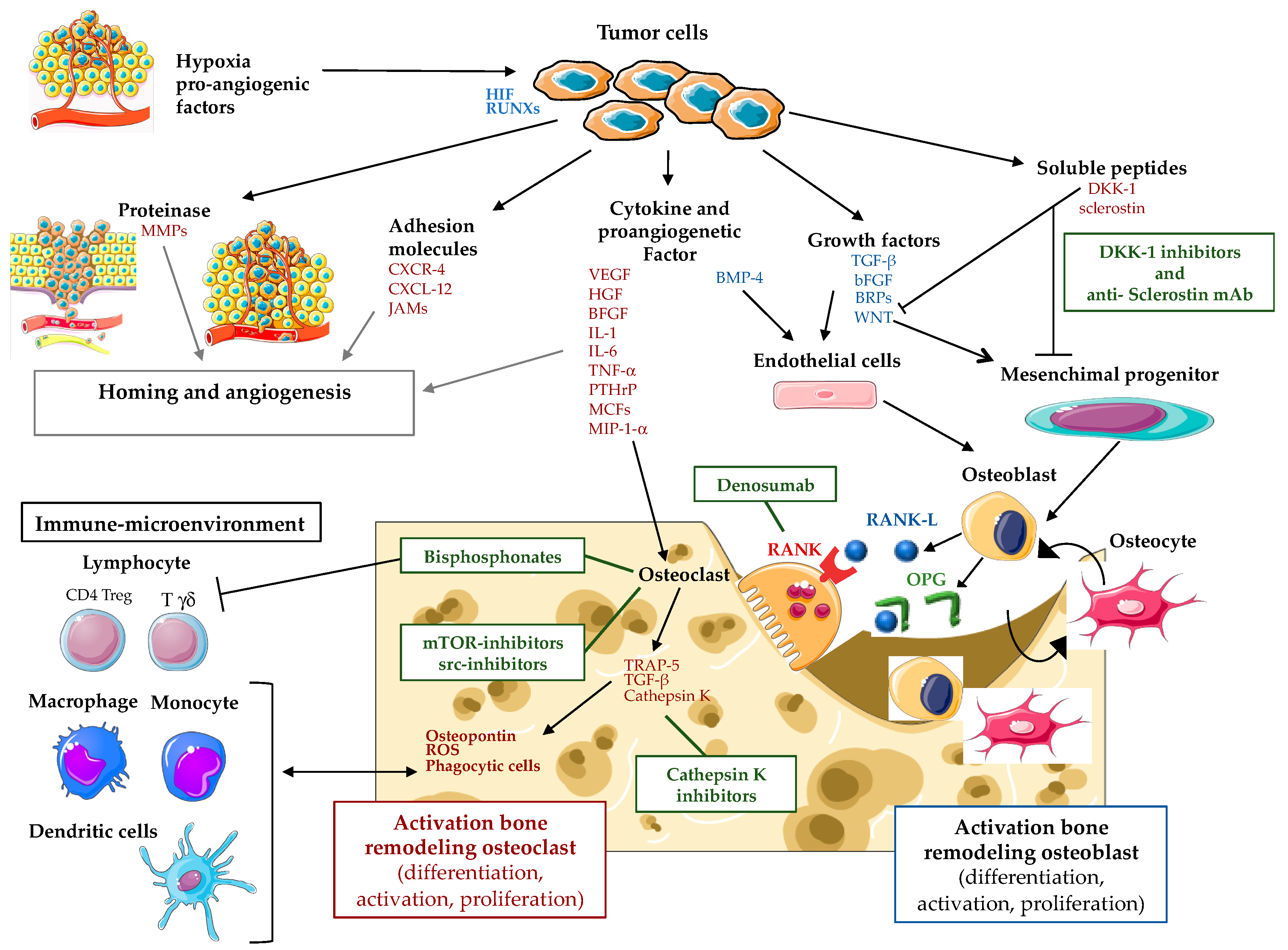
2.2. Bone Dissemination Mechanisms: From Cell Biology to Metastatic Niche Physiopathology
3. Clinical Management for Skeletal Metastasis of Unknown Primary
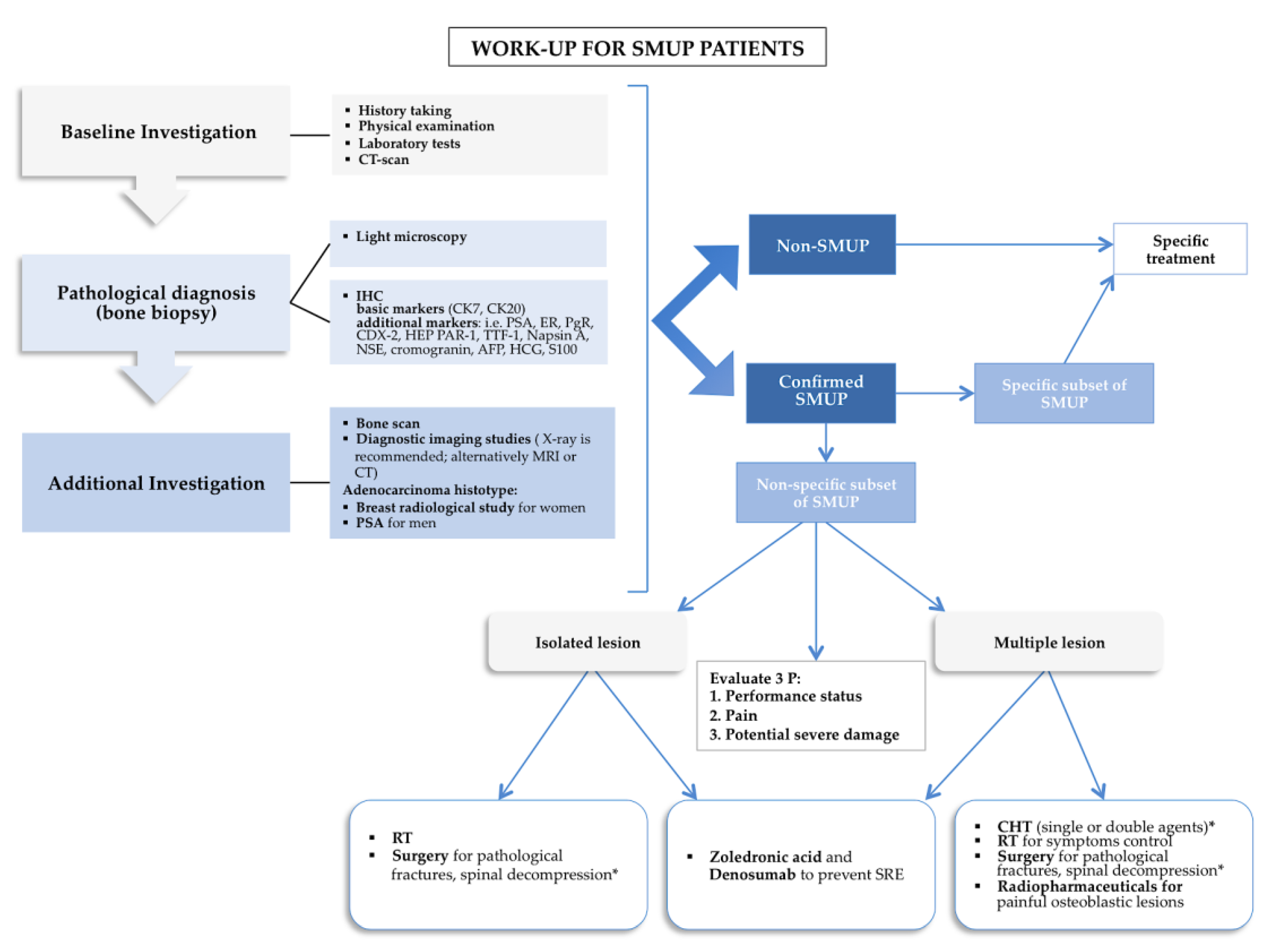
3.1. Diagnostic Work-Up of SMUP
3.2. Therapeutic Approach of SMUP
3.3. Bone Disease Modifying Agent and Bio-Marker Reciprocal Interconnections
3.3.1. Bisphosphonates and Bone Disease Modifying Agents
3.3.2. The Role of Bone Turnover Markers in Diagnosis and Therapy Response with Inhibitors of Bone Resorption Evaluation
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massard, C.; Loriot, Y.; Fizazi, K. Carcinomas of an unknown primary origin—Diagnosis and treatment. Nat. Rev. Clin. Oncol. 2011, 8, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Hess, K.R.; Abbruzzese, M.C.; Lenzi, R.; Raber, M.N.; Abbruzzese, J.L. Classification and regression tree analysis of 1000 consecutive patients with unknown primary carcinoma. Clin. Cancer Res. 1999, 5, 3403–3410. [Google Scholar] [PubMed]
- Carretero, R.G.; Brugera, M.R.; Rebollo-Aparicio, N.; Mohamed, L.E.B. Primary bone metastasis as first manifestation of an unknown primary tumour. BMJ Case Rep. 2015, 2015, 2015211302. [Google Scholar] [CrossRef] [PubMed]
- Piccioli, A.; Maccauro, G.; Spinelli, M.S.; Biagini, R.; Rossi, B. Bone metastases of unknown origin: Epidemiology and principles of management. J. Orthop. Traumatol. 2015, 16, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Destombe, C.; Botton, E.; Le Gal, G.; Roudaut, A.; Jousse-Joulin, S.; Devauchelle-Pensec, V.; Saraux, A. Investigations for bone metastasis from an unknown primary. Jt. Bone Spine 2007, 74, 85–89. [Google Scholar] [CrossRef]
- Kodaira, M.; Takahashi, S.; Yamada, S.; Ueda, K.; Mishima, Y.; Takeuchi, K.; Yamamoto, N.; Ishikawa, Y.; Yokoyama, M.; Saotome, T.; et al. Bone metastasis and poor performance status are prognostic factors for survival of carcinoma of unknown primary site in patients treated with systemic chemotherapy. Ann. Oncol. 2010, 21, 1163–1167. [Google Scholar] [CrossRef]
- Hemminki, K.; Riihimäki, M.; Sundquist, K.; Hemminki, A. Site-specific survival rates for cancer of unknown primary according to location of metastases. Int. J. Cancer 2013, 133, 182–189. [Google Scholar] [CrossRef]
- Takagi, T.; Katagiri, H.; Kim, Y.; Suehara, Y.; Kubota, D.; Akaike, K.; Ishii, M.; Mukaihara, K.; Okubo, T.; Murata, H.; et al. Skeletal Metastasis of Unknown Primary Origin at the Initial Visit: A Retrospective Analysis of 286 Cases. PLoS ONE 2015, 10, e0129428. [Google Scholar] [CrossRef]
- Simon, A.M.; Karluk, M.B. Skeletal metastases of unknown origin. Diagnostic strategy for orthopedic surgeons. Clin. Orthop. Relat. Res. 1982, 166, 96–103. [Google Scholar]
- Simon, M.A.; Bartucci, E.J. The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986, 58, 1088–1095. [Google Scholar] [CrossRef]
- Nottebaert, M.; Exner, G.U.; Von Hochstetter, A.R.; Schreiber, A.; Hochstetter, A. Metastatic bone disease from occult carcinoma: A profile. Int. Orthop. 1989, 13, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Shih, L.-Y.; Chen, T.-H.; Lo, W.-H.; Shih, L.; Chen, T.; Lo, W. Skeletal metastasis from occult carcinoma. J. Surg. Oncol. 1992, 51, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Kneisl, J.S.; Rougraff, B.T.; Simon, M.A. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J. Bone Jt. Surg. Am. 1993, 75, 1276–1281. [Google Scholar]
- Jacobsen, S.; Stephensen, S.L.; Paaske, B.P.; Lie, P.G.; Lausten, G.S. Skeletal metastases of unknown origin: A retrospective analysis of 29 cases. Acta Orthop. Belg. 1997, 63, 15–22. [Google Scholar] [PubMed]
- Katagiri, H.; Takahashi, M.; Inagaki, J.; Sugiura, H.; Ito, S.; Iwata, H. Determining the site of the primary cancer in patients with skeletal metastasis of unknown origin: A retrospective study. Cancer 1999, 86, 533–537. [Google Scholar] [CrossRef]
- Vandecandelaere, M.; Flipo, R.-M.; Cortet, B.; Catanzariti, L.; Duquesnoy, B.; Delcambre, B. Bone metastases revealing primary tumors. Comparison of two series separated by 30 years. Jt. Bone Spine 2004, 71, 224–229. [Google Scholar] [CrossRef]
- Iizuka, Y.; Iizuka, H.; Tsutsumi, S.; Nakagawa, Y.; Nakajima, T.; Sorimachi, Y.; Ara, T.; Nishinome, M.; Seki, T.; Takagishi, K. Diagnosis of a previously unidentified primary site in patients with spinal metastasis: Diagnostic usefulness of laboratory analysis, CT scanning and CT-guided biopsy. Eur. Spine J. 2009, 18, 1431–1435. [Google Scholar] [CrossRef]
- Van De Wouw, A.J.; Jansen, R.L.H.; Speel, E.J.M.; Hillen, H.F.P. The unknown biology of the unknown primary tumour: A literature review. Ann. Oncol. 2003, 14, 191–196. [Google Scholar] [CrossRef]
- Conway, A.M.; Mitchell, C.; Kilgour, E.; Brady, G.; Dive, C.; Cook, N. Molecular characterization and liquid biomarkers in Carcinoma of Unknown Primary (CUP): Taking the ‘U’out of ‘CUP’. Br. J. Cancer 2018, 120, 141–153. [Google Scholar] [CrossRef]
- Korbling, M.; Katz, R.L.; Khanna, A.; Ruifrok, A.C.; Champlin, R.E.; Estrov, Z.; Rondón, G.; Albitar, M. Hepatocytes and Epithelial Cells of Donor Origin in Recipients of Peripheral-Blood Stem Cells. N. Engl. J. Med. 2002, 346, 738–746. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, E.A. Stem cells and diversity. Leukemia 2003, 17, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Young, H.E.; Duplaà, C.; Romero-Ramos, M.; Chesselet, M.-F.; Vourc’H, P.; Yost, M.J.; Ericson, K.; Terracio, L.; Asahara, T.; Masuda, H.; et al. Adult Reserve Stem Cells and Their Potential for Tissue Engineering. Cell Biochem. Biophys. 2004, 40, 1–80. [Google Scholar] [CrossRef]
- Dieterlen-Lièvre, F. Lineage-switching by pluripotent cells derived from adults. J. de la Société de Biol. 2001, 195, 39–46. [Google Scholar] [CrossRef]
- Wood, L.A.; Venner, P.M.; Pabst, H.F.; Wood, P.M.V.L.A. Monozygotic Twin Brothers with Primary Immunodeficiency Presenting with Metastatic Adenocarcinoma of Unknown Primary. Acta Oncol. 1998, 37, 771–772. [Google Scholar] [CrossRef] [PubMed]
- Tomuleasa, C.; Zaharie, F.; Muresan, M.S.; Pop, L.; Fekete, Z.; Dima, D.; Frinc, I.; Trifa, A.; Berce, C.; Jurj, A.; et al. How to Diagnose and Treat a Cancer of Unknown Primary Site. J. Gastrointestin. Liver Dis. 2017, 26, 69–79. [Google Scholar] [PubMed]
- Hemminki, K.; Ji, J.; Sundquist, J.; Shu, X. Familial Risks in Cancer of Unknown Primary: Tracking the Primary Sites. J. Clin. Oncol. 2011, 29, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Economopoulou, P.; Mountzios, G.; Pavlidis, N.; Pentheroudakis, G. Cancer of Unknown Primary origin in the genomic era: Elucidating the dark box of cancer. Cancer Treat. Rev. 2015, 41, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, N.; Fizazi, K. Cancer of unknown primary (CUP). Crit. Rev. Oncol. Hematol. 2005, 54, 243–250. [Google Scholar] [CrossRef]
- Kamposioras, K.; Pentheroudakis, G.; Pavlidis, N. Exploring the biology of cancer of unknown primary: Breakthroughs and drawbacks. Eur. J. Clin. Investig. 2013, 43, 491–500. [Google Scholar] [CrossRef]
- Briasoulis, E.; Tsokos, M.; Fountzilas, G.; Bafaloukos, D.; Kosmidis, P.; Samantas, E.; Skarlos, D.; Nicolaides, C.; Pavlidis, N. Bcl2 and p53 protein expression in metastatic carcinoma of unknown primary origin: Biological and clinical implications. A Hellenic Co-operative Oncology Group study. Anticancer Res. 1998, 18, 1907–1914. [Google Scholar] [PubMed]
- Hainsworth, J.D.; Lennington, W.J.; Greco, F.A. Overexpression of Her-2 in Patients With Poorly Differentiated Carcinoma or Poorly Differentiated Adenocarcinoma of Unknown Primary Site. J. Clin. Oncol. 2000, 18, 632. [Google Scholar] [CrossRef] [PubMed]
- Byrne, N.M.; Summers, A.M.; McDonald, M.M. Tumor Cell Dormancy and Reactivation in Bone: Skeletal Biology and Therapeutic Opportunities. JBMR Plus 2019, 3, e10125. [Google Scholar] [CrossRef] [PubMed]
- Leone, P.; Di Lernia, G.; Solimando, A.G.; Cicco, S.; Saltarella, I.; Lamanuzzi, A.; Ria, R.; Frassanito, M.A.; Ponzoni, M.; Ditonno, P.; et al. Bone marrow endothelial cells sustain a tumor-specific CD8+ T cell subset with suppressive function in myeloma patients. OncoImmunology 2019, 8, e1486949. [Google Scholar] [CrossRef] [PubMed]
- Croucher, P.I.; McDonald, M.M.; Martin, T.J. Bone metastasis: The importance of the neighbourhood. Nat. Rev. Cancer 2016, 16, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Frassanito, M.A.; DeSantis, V.; Di Marzo, L.; Craparotta, I.; Beltrame, L.; Marchini, S.; Annese, T.; Visino, F.; Arciuli, M.; Saltarella, I.; et al. Bone marrow fibroblasts overexpress miR-27b and miR-214 in step with multiple myeloma progression, dependent on tumour cell-derived exosomes. J. Pathol. 2019, 247, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Holohan, C.; Van Schaeybroeck, S.; Longley, D.B.; Johnston, P.G. Cancer drug resistance: An evolving paradigm. Nat. Rev. Cancer 2013, 13, 714–726. [Google Scholar] [CrossRef]
- Porcelli, L.; Iacobazzi, R.M.; Di Fonte, R.; Serratì, S.; Intini, A.; Solimando, A.G.; Brunetti, O.; Calabrese, A.; Leonetti, F.; Azzariti, A.; et al. CAFs and TGF-β Signaling Activation by Mast Cells Contribute to Resistance to Gemcitabine/Nabpaclitaxel in Pancreatic Cancer. Cancers 2019, 11, 330. [Google Scholar] [CrossRef]
- French, C.A.; Kutok, J.L.; Faquin, W.C.; Toretsky, J.A.; Antonescu, C.R.; Griffin, C.A.; Nosé, V.; Vargas, S.O.; Moschovi, M.; Tzortzatou-Stathopoulou, F.; et al. Midline Carcinoma of Children and Young Adults with NUT Rearrangement. J. Clin. Oncol. 2004, 22, 4135–4139. [Google Scholar] [CrossRef]
- Wu, K.; Zhang, X.; Li, F.; Xiao, D.; Hou, Y.; Zhu, S.; Liu, D.; Ye, X.; Ye, M.; Yang, J.; et al. Frequent alterations in cytoskeleton remodelling genes in primary and metastatic lung adenocarcinomas. Nat. Commun. 2015, 6, 10131. [Google Scholar] [CrossRef]
- Fonseca, A.-V.; Freund, D.; Bornhäuser, M.; Corbeil, D. Polarization and Migration of Hematopoietic Stem and Progenitor Cells Rely on the RhoA/ROCK I Pathway and an Active Reorganization of the Microtubule Network. J. Boil. Chem. 2010, 285, 31661–31671. [Google Scholar] [CrossRef] [Green Version]
- Darash-Yahana, M.; Pikarsky, E.; Abramovitch, R.; Zeira, E.; Pal, B.; Karplus, R.; Beider, K.; Avniel, S.; Kasem, S.; Galun, E.; et al. Role of high expression levels of CXCR4 in tumor growth, vascularization, and metastasis. FASEB J. 2004, 18, 1240–1242. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.H.; Serie, D.J.; Parasramka, M.; Cheville, J.C.; Bot, B.M.; Tan, W.; Wang, L.; Joseph, R.W.; Hilton, T.; Leibovich, B.C.; et al. Differential gene expression profiling of matched primary renal cell carcinoma and metastases reveals upregulation of extracellular matrix genes. Ann. Oncol. 2016, 28, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Mondal, N.; Greco, T.M.; Wei, Y.; Spadazzi, C.; Lin, S.-C.; Zheng, H.; Cheung, C.; Magnani, J.L.; Lin, S.-H.; et al. Bone vascular niche E-selectin induces mesenchymal-epithelial transition and Wnt activation in cancer cells to promote bone metastasis. Nat. Cell Biol. 2019, 21, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Solimando, A.G.; Brandl, A.; Mattenheimer, K.; Graf, C.; Ritz, M.; Ruckdeschel, A.; Stühmer, T.; Mokhtari, Z.; Rudelius, M.; Dotterweich, J.; et al. JAM-A as a prognostic factor and new therapeutic target in multiple myeloma. Leukemia 2018, 32, 736. [Google Scholar] [CrossRef]
- van Roosmalen, W.; Le Dévédec, S.E.; Golani, O.; Smid, M.; Pulyakhina, I.; Timmermans, A.M.; Look, M.P.; Zi, D.; Pont, C.; de Graauw, M.; et al. Tumor cell migration screen identifies SRPK1 as breast cancer metastasis determinant. J. Clin. Investig. 2015, 125, 1648–1664. [Google Scholar] [CrossRef] [PubMed]
- Caino, M.C.; Chae, Y.C.; Vaira, V.; Ferrero, S.; Nosotti, M.; Martin, N.M.; Weeraratna, A.; O’Connell, M.; Jernigan, D.; Fatatis, A.; et al. Metabolic stress regulates cytoskeletal dynamics and metastasis of cancer cells. J. Clin. Investig. 2013, 123, 2907–2920. [Google Scholar] [CrossRef]
- Rudelius, M.; Rosenfeldt, M.T.; Leich, E.; Rauert-Wunderlich, H.; Solimando, A.G.; Beilhack, A.; Ott, G.; Rosenwald, A. Inhibition of focal adhesion kinase overcomes resistance of mantle cell lymphoma to ibrutinib in the bone marrow microenvironment. Haematologica 2018, 103, 116–125. [Google Scholar] [CrossRef]
- Mohme, M.; Riethdorf, S.; Pantel, K. Circulating and disseminated tumour cells—mechanisms of immune surveillance and escape. Nat. Rev. Clin. Oncol. 2017, 14, 155. [Google Scholar] [CrossRef]
- Rao, L.; De Veirman, K.; Giannico, D.; Saltarella, I.; DeSantis, V.; Frassanito, M.A.; Solimando, A.G.; Ribatti, D.; Prete, M.; Harstrick, A.; et al. Targeting angiogenesis in multiple myeloma by the VEGF and HGF blocking DARPin® protein MP0250: A preclinical study. Oncotarget 2018, 9, 13366–13381. [Google Scholar] [CrossRef]
- Lopez-Soto, A.; Gonzalez, S.; Smyth, M.J.; Galluzzi, L. Control of metastasis by NK cells. Cancer Cell 2017, 32, 135–154. [Google Scholar] [CrossRef] [PubMed]
- Moschetta, M.; Sacco, A.; Belotti, A.; Ribolla, R.; Chiarini, M.; Giustini, V.; Bertoli, D.; Sottini, A.; Valotti, M.; Ghidini, C.; et al. Bone Marrow Stroma and Vascular Contributions to Myeloma Bone Homing. Curr. Osteoporos. Rep. 2017, 15, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Rossnagl, S.; Ghura, H.; Groth, C.; Altrock, E.; Jakob, F.; Schott, S.; Wimberger, P.; Link, T.; Kuhlmann, J.D.; Stenzl, A.; et al. A subpopulation of stromal cells controls cancer cell homing to the bone marrow. Cancer Res. 2018, 78, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Rossnagl, S.; Von Au, A.; Vasel, M.; Cecchini, A.G.; Nakchbandi, I.A. Blood Clot Formation Does Not Affect Metastasis Formation or Tumor Growth in a Murine Model of Breast Cancer. PLoS ONE 2014, 9, e94922. [Google Scholar] [CrossRef] [PubMed]
- Augustin, H.G.; Koh, G.Y. Organotypic vasculature: From descriptive heterogeneity to functional pathophysiology. Science 2017, 357, 2379. [Google Scholar] [CrossRef]
- Hiraga, T. Hypoxic Microenvironment and Metastatic Bone Disease. Int. J. Mol. Sci. 2018, 19, 3523. [Google Scholar] [CrossRef]
- Malfettone, A.; Silvestris, N.; Paradiso, A.; Mattioli, E.; Simone, G.; Mangia, A. Overexpression of nuclear NHERF1 in advanced colorectal cancer: Association with hypoxic microenvironment and tumor invasive phenotype. Exp. Mol. Pathol. 2012, 92, 296–303. [Google Scholar] [CrossRef]
- Mazzone, M.; Dettori, D.; De Oliveira, R.L.; Loges, S.; Schmidt, T.; Jonckx, B.; Tian, Y.-M.; Lanahan, A.A.; Pollard, P.; De Almodovar, C.R.; et al. Heterozygous Deficiency of PHD2 Restores Tumor Oxygenation and Inhibits Metastasis via Endothelial Normalization. Cell 2009, 136, 839–851. [Google Scholar] [CrossRef] [Green Version]
- D’Oronzo, S.; Coleman, R.; Brown, J.; Silvestris, F. Metastatic bone disease: Pathogenesis and therapeutic options. J. Bone Oncol. 2018, 15, 004. [Google Scholar] [CrossRef]
- Fizazi, K.; Greco, F.A.; Pavlidis, N.; Daugaard, G.; Oien, K.; Pentheroudakis, G. Cancers of unknown primary site: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v133–v138. [Google Scholar] [CrossRef]
- Hainsworth, J.D.; Greco, F.A. Cancer of Unknown Primary Site: New Treatment Paradigms in the Era of Precision Medicine. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Bochtler, T.; Löffler, H.; Krämer, A. Diagnosis and management of metastatic neoplasms with unknown primary. Semin. Diagn. Pathol. 2018, 35, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Bender, R.A.; Erlander, M.G. Molecular Classification of Unknown Primary Cancer. Semin. Oncol. 2009, 36, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Monzon, A.F.; Koen, T.J. Diagnosis of metastatic neoplasms: Molecular approaches for identification of tissue of origin. Arch. Pathol. Lab. Med. 2010, 134, 216–224. [Google Scholar] [PubMed]
- Varadhachary, G.R.; Raber, M.N. Cancer of unknown primary site. N. Engl. J. Med. 2014, 371, 757–765. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Occult primary (cancer of unknown primary [CUP]). In NCCN Clinical Practice Guidelines in Oncology; Version 1; National Comprehensive Cancer Network: Fort Washington, PA, USA, 2018; Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on 15 August 2019).
- Losa, F.; Soler, G.; Casado, A.; Estival, A.; Fernández, I.; Giménez, S.; Longo, F.; Pazo-Cid, R.; Salgado, J.; Seguí, M.Á. SEOM clinical guideline on unknown primary cancer (2017). Clin. Transl. Oncol. 2017, 20, 89–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, R.; Body, J.J.; Aapro, M.; Hadji, P.; Herrstedt, J. On behalf of the ESMO Guidelines Working Group Bone health in cancer patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2014, 25, iii124–iii137. [Google Scholar] [CrossRef] [PubMed]
- Macedo, F.; Ladeira, K.; Pinho, F.; Saraiva, N.; Bonito, N.; Pinto, L.; Gonçalves, F. Bone metastases: An overview. Oncol. Rev. 2017, 11, 321. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-L.; Liu, T.; Wang, X.-M.; Xu, Y.; Deng, S.-M. Diagnosis of bone metastases: A meta-analysis comparing 18FDG PET, CT, MRI and bone scintigraphy. Eur. Radiol. 2011, 21, 2604–2617. [Google Scholar] [CrossRef]
- Heindel, W.; Gübitz, R.; Vieth, V.; Weckesser, M.; Schober, O.; Schäfers, M. The Diagnostic Imaging of Bone Metastases. Dtsch. Arztebl. Int. 2014, 111, 741–747. [Google Scholar] [CrossRef]
- Kwee, R.M. Combined FDG-PET/CT for the detection of unknown primary tumors: Systematic review and meta-analysis. Eur. Radiol. 2009, 19, 731–744. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Chen, J.; Ni, S.; Tan, C.; Xu, M.; Dong, L.; Yuan, L.; Wang, Q.; Du, X. Pan-cancer transcriptome analysis reveals a gene expression signature for the identification of tumor tissue origin. Mod. Pathol. 2016, 29, 546–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hainsworth, J.D.; Rubin, M.S.; Spigel, D.R.; Boccia, R.V.; Raby, S.; Quinn, R.; Greco, F.A. Molecular gene expression profiling to predict the tissue of origin and direct site-specific therapy in patients with carcinoma of unknown primary site: A prospective trial of the Sarah Cannon research institute. J. Clin. Oncol. 2012, 31, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, N.; Briasoulis, E.; Hainsworth, J.; Greco, F. Diagnostic and therapeutic management of cancer of an unknown primary. Eur. J. Cancer 2003, 39, 1990–2005. [Google Scholar] [CrossRef]
- Greco, F.A.; Pavlidis, N. Treatment for Patients with Unknown Primary Carcinoma and Unfavorable Prognostic Factors. Semin. Oncol. 2009, 36, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Varadhachary, G.R.; Greco, F.A. Overview of Patient Management and Future Directions in Unknown Primary Carcinoma. Semin. Oncol. 2009, 36, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Culine, S. Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients with Carcinomas of an Unknown Primary Site. J. Clin. Oncol. 2002, 20, 4679–4683. [Google Scholar] [CrossRef] [PubMed]
- Seve, P.; Sawyer, M.; Hanson, J.; Broussolle, C.; Négrier, S.; Dumontet, C.; Mackey, J.R.; Trillet-Lenoir, V.; Ray-Coquard, I.; Trillet-Lenoir, V.; et al. Low serum albumin levels and liver metastasis are powerful prognostic markers for survival in patients with carcinomas of unknown primary site. Cancer 2006, 107, 2698–2705. [Google Scholar] [CrossRef] [PubMed]
- Trivanovic, D.; Petković, M.; Stimac, D. New Prognostic Index to Predict Survival in Patients with Cancer of Unknown Primary Site with Unfavourable Prognosis. Clin. Oncol. 2009, 21, 43–48. [Google Scholar] [CrossRef]
- Chen, K.-W.; Liu, C.-J.; Lu, H.-J.; Tzeng, C.-H.; Liu, J.-H.; Chiou, T.-J.; Yen, C.-C.; Wang, W.-S.; Chao, T.-C.; Teng, H.-W.; et al. Evaluation of prognostic factors and the role of chemotherapy in unfavorable carcinoma of unknown primary site: A 10-year cohort study. BMC Res. Notes 2012, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Santoni, M.; Conti, A.; Procopio, G.; Porta, C.; Ibrahim, T.; Barni, S.; Guida, F.M.; Fontana, A.; Berruti, A.; Berardi, R.; et al. Bone metastases in patients with metastatic renal cell carcinoma: Are they always associated with poor prognosis? J. Exp. Clin. Cancer Res. 2015, 34, 10. [Google Scholar] [CrossRef] [PubMed]
- Sierko, E.; Hempel, D.; Zuzda, K.; Wojtukiewicz, M.Z. Personalized Radiation Therapy in Cancer Pain Management. Cancers 2019, 11, 390. [Google Scholar] [CrossRef] [PubMed]
- Spratt, E.D. Combination therapies in prostate cancer: Proceed with caution. Lancet Oncol. 2019, 20, 321–323. [Google Scholar] [CrossRef]
- Golfinopoulos, V.; Pentheroudakis, G.; Salanti, G.; Nearchou, A.D.; Ioannidis, J.P.; Pavlidis, N. Comparative survival with diverse chemotherapy regimens for cancer of unknown primary site: Multiple-treatments meta-analysis. Cancer Treat. Rev. 2009, 35, 570–573. [Google Scholar] [CrossRef] [PubMed]
- Hainsworth, J.D.; Spigel, D.R.; Clark, B.L.; Shipley, D.; Thompson, D.S.; Farley, C.; West-Osterfield, K.; Lane, C.M.; Cescon, T.; Bury, M.J.; et al. Paclitaxel/carboplatin/etoposide versus gemcitabine/irinotecan in the first-line treatment of patients with carcinoma of unknown primary site: A randomized, phase III Sarah Cannon Oncology Research Consortium Trial. Cancer J. 2010, 16, 70–75. [Google Scholar] [CrossRef]
- Culine, S.; Lortholary, A.; Voigt, J.-J.; Bugat, R.; Théodore, C.; Priou, F.; Kaminsky, M.-C.; Lesimple, T.; Pivot, X.; Coudert, B.; et al. Cisplatin in combination with either gemcitabine or irinotecan in carcinomas of unknown primary site: Results of a randomized phase II study—Trial for the French Study Group on Carcinomas of Unknown Primary (GEFCAPI 01). J. Clin. Oncol. 2003, 21, 3479–3482. [Google Scholar] [CrossRef] [PubMed]
- Santini, D.; Pantano, F.; Riccardi, F.; Di Costanzo, G.G.; Addeo, R.; Guida, F.M.; Ceruso, M.S.; Barni, S.; Bertocchi, P.; Marinelli, S.; et al. Natural History of Malignant Bone Disease in Hepatocellular Carcinoma: Final Results of a Multicenter Bone Metastasis Survey. PLoS ONE 2014, 9, e105268. [Google Scholar] [CrossRef]
- Santini, D.; Procopio, G.; Porta, C.; Ibrahim, T.; Barni, S.; Mazzara, C.; Fontana, A.; Berruti, A.; Berardi, R.; Vincenzi, B.; et al. Natural History of Malignant Bone Disease in Renal Cancer: Final Results of an Italian Bone Metastasis Survey. PLoS ONE 2013, 8, e83026. [Google Scholar] [CrossRef]
- Silvestris, N.; Pantano, F.; Ibrahim, T.; Gamucci, T.; De Vita, F.; Di Palma, T.; Pedrazzoli, P.; Barni, S.; Bernardo, A.; Febbraro, A.; et al. Natural History of Malignant Bone Disease in Gastric Cancer: Final Results of a Multicenter Bone Metastasis Survey. PLoS ONE 2013, 8, e74402. [Google Scholar] [CrossRef]
- Santini, D.; Brandi, G.; Aprile, G.; Russano, M.; Cereda, S.; Leone, F.; Lonardi, S.; Fornaro, L.; Scartozzi, M.; Silvestris, N.; et al. Bone metastases in biliary cancers: A multicenter retrospective survey. J. Bone Oncol. 2018, 12, 33–37. [Google Scholar] [CrossRef]
- Santini, D.; Tampellini, M.; Vincenzi, B.; Ibrahim, T.; Ortega, C.; Virzi, V.; Silvestris, N.; Berardi, R.; Masini, C.; Calipari, N.; et al. Natural history of bone metastasis in colorectal cancer: Final results of a large Italian bone metastases study. Ann. Oncol. 2012, 23, 2072–2077. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.H.F.; Stockler, M.R. Bisphosphonates and other bone agents for breast cancer. Cochrane Database Syst. Rev. 2012, 2, CD003474. [Google Scholar]
- Stopeck, A.T.; Lipton, A.; Body, J.-J.; Steger, G.G.; Tonkin, K.; De Boer, R.H.; Lichinitser, M.; Fujiwara, Y.; Yardley, D.A.; Viniegra, M.; et al. Denosumab Compared with Zoledronic Acid for the Treatment of Bone Metastases in Patients With Advanced Breast Cancer: A Randomized, Double-Blind Study. J. Clin. Oncol. 2010, 28, 5132–5139. [Google Scholar] [CrossRef] [PubMed]
- Santini, D.; Galluzzo, S.; Zoccoli, A.; Pantano, F.; Fratto, M.; Vincenzi, B.; Lombardi, L.; Gucciardino, C.; Silvestris, N.; Riva, E.; et al. New molecular targets in bone metastases. Cancer Treat. Rev. 2010, 36, S6–S10. [Google Scholar] [CrossRef] [Green Version]
- Lipton, A.; Fizazi, K.; Stopeck, A.; Henry, D.; Smith, M.; Shore, N.; Martin, M.; Vadhan-Raj, S.; Brown, J.; Richardson, G.; et al. Effect of denosumab versus zoledronic acid in preventing skeletal-related events in patients with bone metastases by baseline characteristics. Eur. J. Cancer 2016, 53, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.B.; Wynne, C.; Ramirez, G.; He, W.; Song, Y.; Berd, Y.; Wang, H.; Mehta, A.; Lombardi, A. The Cathepsin K Inhibitor Odanacatib Suppresses Bone Resorption in Women with Breast Cancer and Established Bone Metastases: Results of a 4-Week, Double-Blind, Randomized, Controlled Trial. Clin. Breast Cancer 2010, 10, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Argentiero, A.; De Summa, S.; Di Fonte, R.; Iacobazzi, R.M.; Porcelli, L.; Da Vià, M.; Brunetti, O.; Azzariti, A.; Silvestris, N.; Solimando, A.G. Gene Expression Comparison between the Lymph Node-Positive and -Negative Reveals a Peculiar Immune Microenvironment Signature and a Theranostic Role for WNT Targeting in Pancreatic Ductal Adenocarcinoma: A Pilot Study. Cancers 2019, 11, 942. [Google Scholar] [CrossRef] [PubMed]
- Campone, M.; Bondarenko, I.; Brincat, S.; Hotko, Y.; Munster, P.N.; Chmielowska, E. Phase II study of single-agent bosutinib, a Src/Abl tyrosine kinase inhibitor, in patients with locally advanced or metastatic breast cancer pretreated with chemotherapy. Ann. Oncol. 2012, 23, 610–617. [Google Scholar] [CrossRef]
- Rosen, L.S.; Gordon, D.; Kaminski, M.; Howell, A.; Belch, A.; Mackey, J.; Apffelstaedt, J.; Hussein, M.A.; Coleman, R.E.; Reitsma, D.J.; et al. Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: A randomized, double-blind, multicenter, comparative trial. Cancer 2003, 98, 1735–1744. [Google Scholar] [CrossRef]
- Saad, F.; Gleason, D.M.; Murray, R.; Tchekmedyian, S.; Venner, P.; Lacombe, L.; Chin, J.L.; Vinholes, J.J.; Goas, J.A.; Zheng, M. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J. Natl. Cancer Inst. 2004, 96, 879–882. [Google Scholar] [CrossRef]
- Rosen, L.S.; Gordon, D.; Tchekmedyian, S.; Yanagihara, R.; Hirsh, V.; Krzakowski, M.; Pawlicki, M.; de Souza, P.; Zheng, M.; Urbanowitz, G.; et al. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: A phase III, double-blind, randomized trial. The Zoledronic Acid Lung Cancer and other Solid Tumors Study Group. J. Clin. Oncol. 2003, 21, 3150–3157. [Google Scholar] [CrossRef] [PubMed]
- Body, J.J.; Mancini, I. Bisphosphonates for cancer patients: Why, how and when? Support. Cancer Care 2002, 10, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Hirsh, V.; Tchekmedyian, N.S.; Rosen, L.S.; Zheng, M.; Hei, Y.-J. Clinical Benefit of Zoledronic Acid in Patients with Lung Cancer and OtherSolid Tumors: Analysis Based on History of Skeletal Complications. Clin. Lung Cancer 2004, 6, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Wyngaert, T.V.D.; Delforge, M.; Doyen, C.; Duck, L.; Wouters, K.; Delabaye, I.; Wouters, C.; Wildiers, H. Prospective observational study of treatment pattern, effectiveness and safety of zoledronic acid therapy beyond 24 months in patients with multiple myeloma or bone metastases from solid tumors. Support. Care Cancer 2013, 21, 3483–3490. [Google Scholar] [CrossRef] [PubMed]
- Winters, J.P.; Fekrazad, M.H.; Gilliam, E.H.; Lee, S.; Choi, K.; Royce, M. Efficacy and safety of intravenous bisphosphonates beyond two years of use. J. Clin. Oncol. 2010, 28, e19619. [Google Scholar] [CrossRef]
- Body, J.J.; Facon, T.; Coleman, R.E.; Lipton, A.; Geurs, F.; Fan, M.; Holloway, D.; Peterson, M.C.; Bekker, P.J. A study of the biological receptor activator of nuclear FactorkappaB ligand inhibitor, denosumab, in patients with multiple myeloma or bone metastases from breast cancer. Clin. Cancer Res. 2006, 12, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Body, J.J.; Diel, I.J.; Lichinitzer, M.; Lazarev, A.; Pecherstorfer, M.; Bell, R.; Tripathy, D.; Bergstrom, B. Oral ibandronate reduces the risk of skeletal complications in breast cancer patients with metastatic bone disease: Results from two randomized, placebo-controlled phase III studies. Br. J. Cancer 2004, 90, 1133–1137. [Google Scholar] [CrossRef]
- Heras, P.; Kritikos, K.; Hatzopoulos, A.; Georgopoulou, A.-P. Efficacy of ibandronate for the treatment of skeletal events in patients with metastatic breast cancer. Eur. J. Cancer Care 2009, 18, 653–656. [Google Scholar] [CrossRef]
- Body, J.-J.; Diel, I.J.; Lichinitser, M.R.; Kreuser, E.D.; Dornoff, W.; Gorbunova, V.A.; Budde, M.; Bergström, B. Intravenous ibandronate reduces the incidence of skeletal complications in patients with breast cancer and bone metastases. Ann. Oncol. 2003, 14, 1399–1405. [Google Scholar] [CrossRef]
- Von Moos, R.; Costa, L.; Gonzalez-Suarez, E.; Terpos, E.; Niepel, D.; Body, J. Management of bone health in solid tumours: From bisphosphonates to a monoclonal antibody. Cancer Treat. Rev. 2019, 76, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Carducci, M.; Smith, M.; Damião, R.; Brown, J.; Karsh, L.; Milecki, P.; Shore, N.; Rader, M.; Wang, H.; et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: A randomised, double-blind study. Lancet 2011, 377, 813–822. [Google Scholar] [CrossRef]
- Stopeck, A.T.; Fizazi, K.; Body, J.J.; Brown, J.E.; Carducci, M.; Diel, I.; Fujiwara, Y.; Martín, M.; Paterson, A.; Tonkin, K.; et al. Safety of long-term denosumab therapy: Results from the open label extension phase of two phase 3 studies in patients with metastatic breast and prostate cancer. Support. Care Cancer 2016, 24, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Aapro, M.; Abrahamsson, P.A.; Body, J.J.; Coleman, R.E.; Colomer, R.; Costa, L.; Crino, L.; Dirix, L.; Gnant, M.; Gralow, J.; et al. Guidance on the use of bisphosphonate in solid tumors: Recommendations of an international expert panel. Ann. Oncol. 2008, 19, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.; Solomon, D.H.; Tsacogianis, T.N.; Landon, J.E.; Song, H.J.; Kim, S.C. Comparative safety and effectiveness of denosumab versus zoledronic acid in patients with osteoporosis: A cohort study. J. Bone Miner. Res. 2017, 32, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Van Poznak, C.H.; Von Roenn, J.H.; Temin, S. American Society of Clinical Oncology Clinical Practice Guideline Update: Recommendations on the Role of Bone-Modifying Agents in Metastatic Breast Cancer. J. Oncol. Pract. 2011, 7, 117–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchette, P.S.; Pritchard, K.I. The Role of Bisphosphonates in Early- and Advanced-Stage Breast Cancer: Have We Finally Optimized Care? Oncology (Williston Park) 2015, 29, 23–30. [Google Scholar]
- Vasikaran, S.; Cooper, C.; Eastell, R.; Griesmacher, A.; Morris, H.A.; Trenti, T.; Kanis, J.A. International Osteoporosis Foundation and International Federation of Clinical Chemistry and Laboratory Medicine Position on bone marker standards in osteoporosis. Clin. Chem. Lab. Med. 2011, 49, 1271–1274. [Google Scholar] [CrossRef]
- Vasikaran, S.D.; Chubb, S.A.P. The use of biochemical markers of bone turnover in the clinical management of primary and secondary osteoporosis. Endocrine 2016, 52, 222–225. [Google Scholar] [CrossRef]
- D’Oronzo, S.; Brown, J.; Coleman, R. The role of biomarkers in the management of bone-homing malignancies. J. Bone Oncol. 2017, 9, 1–9. [Google Scholar] [CrossRef]
- Jung, K.; Lein, M. Bone turnover markers in serum and urine as diagnostic, prognostic and monitoring biomarkers of bone metastasis. Biochim. Biophys. Acta 2014, 1846, 425–438. [Google Scholar] [CrossRef]
- Coleman, R.; Costa, L.; Saad, F.; Cook, R.; Hadji, P.; Terpos, E.; Garnero, P.; Brown, J.; Body, J.-J.; Smith, M.; et al. Consensus on the utility of bone markers in the malignant bone disease setting. Crit. Rev. Oncol. 2011, 80, 411–432. [Google Scholar] [CrossRef] [PubMed]
- Som, A.; Tu, S.-M.; Liu, J.; Wang, X.; Qiao, W.; Logothetis, C.; Corn, P.G. Response in bone turnover markers during therapy predicts overall survival in patients with metastatic prostate cancer: Analysis of three clinical trials. Br. J. Cancer 2012, 107, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Massard, C.; Smith, M.; Rader, M.; Brown, J.; Milecki, P.; Shore, N.; Oudard, S.; Karsh, L.; Carducci, M.; et al. Bone-related Parameters are the Main Prognostic Factors for Overall Survival in Men with Bone Metastases from Castration-resistant Prostate Cancer. Eur. Urol. 2015, 68, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.M.; Demers, L.M.; Leitzel, K.; Harvey, H.A.; Clemens, D.; Mallinak, N.; Engle, L.; Chinchilli, V.; Costa, L.; Brady, C.; et al. Baseline serum NTx levels are prognostic in metastatic breast cancer patients with bone-only metastasis. Ann. Oncol. 2004, 15, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Abildgaard, N.; Brixen, K.; Eriksen, E.F.; Kristensen, J.E.; Nielsen, J.L.; Heickendorff, L. Sequential analysis of biochemical markers of bone resorption and bone densitometry in multiple myeloma. Haematologica 2004, 89, 567–577. [Google Scholar] [PubMed]
- Fizazi, K.; Lipton, A.; Mariette, X.; Body, J.-J.; Rahim, Y.; Gralow, J.R.; Gao, G.; Wu, L.; Sohn, W.; Jun, S. Randomized Phase II Trial of Denosumab in Patients with Bone Metastases from Prostate Cancer, Breast Cancer, or Other Neoplasms After Intravenous Bisphosphonates. J. Clin. Oncol. 2009, 27, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, H.; Carrasquinha, E.; Alho, I.; Ferreira, A.R.; Costa, L.; Carvalho, A.M.; Vinga, S. Modelling cancer outcomes of bone metastatic patients: Combining survival data with N-Telopeptide of type I collagen (NTX) dynamics through joint models. BMC Med. Inform. Decis. Mak. 2019, 19, 13. [Google Scholar] [CrossRef]
- Schiano, C.; Soricelli, A.; De Nigris, F.; Napoli, C. New challenges in integrated diagnosis by imaging and osteo-immunology in bone lesions. Expert Rev. Clin. Immunol. 2019, 15, 289–301. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | SMUP at Diagnosis | Identified Primary Cancer | Number and Site of Primary Cancer Identified | Confirmed SMUP | mOS Confirmed SMUP (Months) |
|---|---|---|---|---|---|
| Simon and Karluk [10] | n = 12 | n = 6 (50%) | Kidney (3), lung (2), others (1) | n = 6 (50%) | NA |
| Simon and Bartucci [11] | n = 46 | n = 20 (44%) | Lung (7), kidney (6), breast = prostate (2), ovarian/thyroid/liver (1) | n = 26 (56%) | NA |
| Nottebaert et al. [12] | n = 51 | n = 33 (65%) | Lung (17), others (16) | n = 18 (35%) | 11.1 |
| Shih et al. [13] | n = 52 | n = 28 (54%) | Lung (9), liver (8), kidney (5), prostate (3), thyroid (2), rectum (1) | n = 24 (46%) | 11 |
| Rougraff et al. [14] | n = 40 | n = 34 (85%) | Lung (23), kidney (4), breast/colon/liver/ bladder (1), others (3) | n = 6 (15%) | NA |
| Jacobsen et al. [15] | n = 29 | n = 24 (83%) (2 patients postmortem) | Lung (11), prostate (3), breast/lymphomas (2), kidney/ovary/pancreas/stomach/small intestine carcinoid/retroperitoneal rhabdomyosarcoma (1) | n = 5 (17%) | 12 |
| Katagiri et al. [16] | n = 64 | n = 59 (92%) | Lung (23), prostate (11), breast/liver (5), others (15) | n = 5 (8%) | 5 |
| Vandecandelaere et al. [17] | n = 129 | n = 84 (65%) | Lung (36), prostate (17), kidney (15), breast (9), stomach (2), bladder/colon/testis/pancreas/liver (1) | n = 45 (35%) | 6 |
| Destombe et al. [6] | n = 152 | n = 94 (88%) | Lung (37), prostate (26), breast (20), urinary system (11) | n = 13 (12%) | NA |
| Iizuka et al. [18] | n = 27 | n = 26 (96%) | Myeloma (7), lymphoma (3), lung (6), prostate (4), kidney/thyroid/liver/pancreas/stomach/esophagus (1) | n = 1 (4%) | NA |
| Hemminki et al. [8] | n = 501 | n = 256 (60%) | Lung (128), urinary (29), prostate (16), breast (14), colon (12), pancreas/gastrointestinal (10), liver (9), biliary system (4), stomach (3), mediastinum (2), others (19) | n = 203 (40%) | 3 |
| Takagi et al. [9] | n = 286 | n = 254 (89%) | Lung (72), myeloma (41), prostate (26), lymphoma (23), kidney (18), liver (12), breast (12), gastric (10), pancreatic (10), thyroid (9), bile duct/colon (6), esophageal (3), others (6) | n = 32 (11%) | 11 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argentiero, A.; Solimando, A.G.; Brunetti, O.; Calabrese, A.; Pantano, F.; Iuliani, M.; Santini, D.; Silvestris, N.; Vacca, A. Skeletal Metastases of Unknown Primary: Biological Landscape and Clinical Overview. Cancers 2019, 11, 1270. https://doi.org/10.3390/cancers11091270
Argentiero A, Solimando AG, Brunetti O, Calabrese A, Pantano F, Iuliani M, Santini D, Silvestris N, Vacca A. Skeletal Metastases of Unknown Primary: Biological Landscape and Clinical Overview. Cancers. 2019; 11(9):1270. https://doi.org/10.3390/cancers11091270
Chicago/Turabian StyleArgentiero, Antonella, Antonio Giovanni Solimando, Oronzo Brunetti, Angela Calabrese, Francesco Pantano, Michele Iuliani, Daniele Santini, Nicola Silvestris, and Angelo Vacca. 2019. "Skeletal Metastases of Unknown Primary: Biological Landscape and Clinical Overview" Cancers 11, no. 9: 1270. https://doi.org/10.3390/cancers11091270