The Clinical Outcomes of Locally Advanced Cervical Esophageal Squamous Cell Carcinoma Patients Receiving Curative Concurrent Chemoradiotherapy: A Population-Based Propensity Score-Matched Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Clinical Outcomes of Cervical ESCC Patients
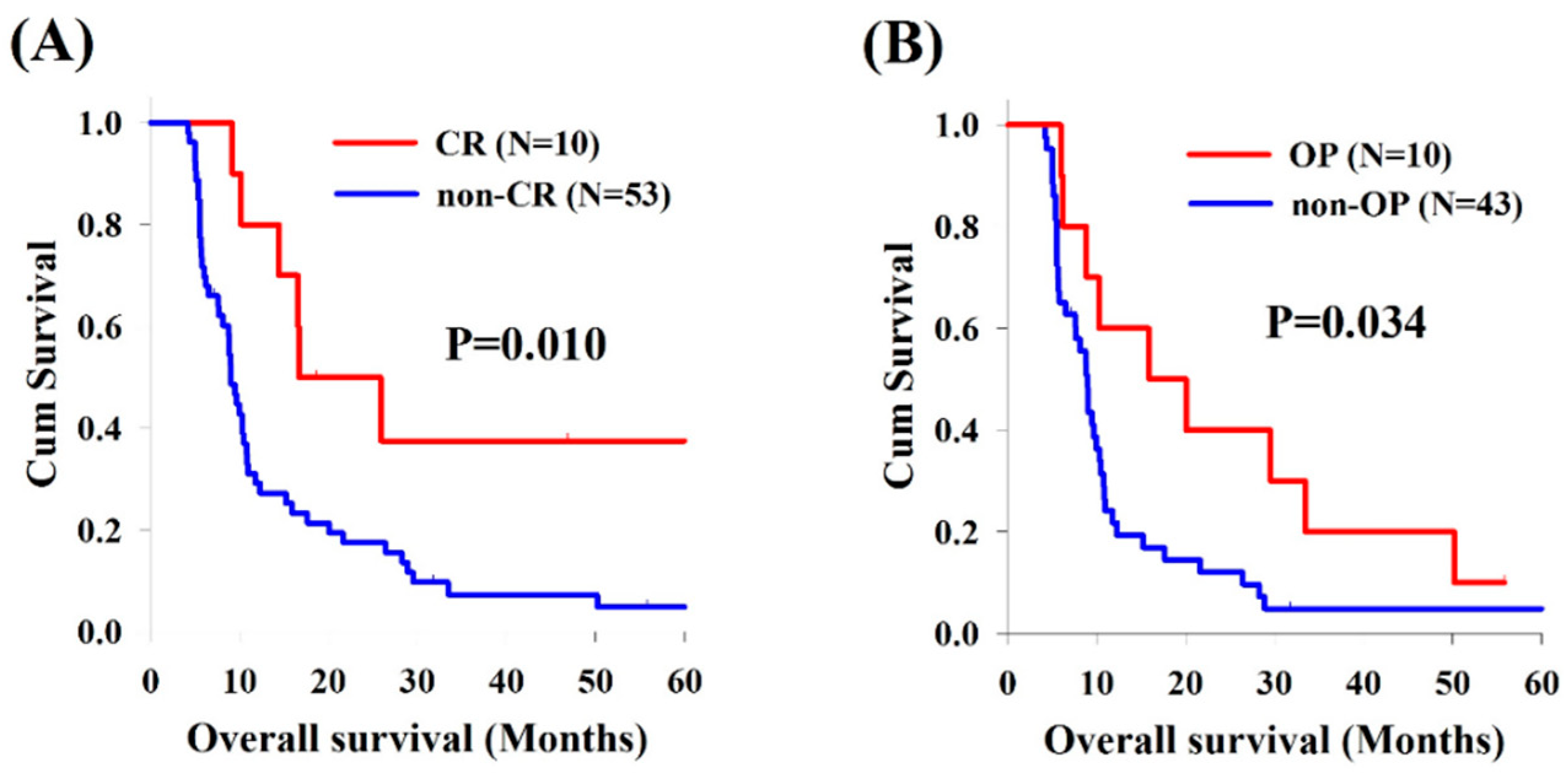
2.3. Comparisons between Cervical and Thoracic ESCC Patients
2.4. The Effect of Surgical Intervention
3. Discussion
4. Material and Methods
4.1. Patient Eligibility and Study Design
4.2. CCRT Setting and Surgery
4.3. Definition of Clinical Complete Response
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Department of Health, Republic of China. Cancer Registry Annual Report 2015; National Department of Health, Republic of China: Beijing, China, 2015.
- Yin, W.B.; Zhang, L.; Miao, Y.; Yu, Z.; Zhang, Z.; Zhueng, C.; Wang, M.; Li, G.; Liu, Y.; Jia, Y.; et al. The results of high-energy electron therapy in carcinoma of the oesophagus compared with telecobalt therapy. Clin. Radiol. 1983, 34, 113–116. [Google Scholar] [CrossRef]
- Grass, G.D.; Cooper, S.L.; Armeson, K.; Garrett-Mayer, E.; Sharma, A. Cervical esophageal cancer: A population-based study. Head Neck 2015, 37, 808–814. [Google Scholar] [CrossRef]
- al-Sarraf, M.; Martz, K.; Herskovic, A.; Leichman, L.; Brindle, J.S.; Vaitkevicius, V.K.; Cooper, J.; Byhardt, R.; Davis, L.; Emami, B. Progress report of combined chemoradiotherapy versus radiotherapy alone in patients with esophageal cancer: An intergroup study. J. Clin. Oncol. 1997, 15, 277–284. [Google Scholar] [CrossRef]
- Bedenne, L.; Michel, P.; Bouche, O.; Milan, C.; Mariette, C.; Conroy, T.; Pezet, D.; Roullet, B.; Seitz, J.F.; Herr, J.P.; et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J. Clin. Oncol. 2007, 25, 1160–1168. [Google Scholar] [CrossRef]
- Cooper, J.S.; Guo, M.D.; Herskovic, A.; Macdonald, J.S.; Martenson, J.A., Jr.; Al-Sarraf, M.; Byhardt, R.; Russell, A.H.; Beitler, J.J.; Spencer, S.; et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA 1999, 281, 1623–1627. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, Y.; Hieda, Y.; Nakajima, M.; Kitajima, K.; Yoshida, R.; Yoshizako, T.; Ue, A.; Tokudo, M.; Hirahara, N.; Moriyama, I.; et al. Concurrent Chemoradiotherapy with Docetaxel, Cisplatin, and 5-fluorouracil Improves Survival of Patients with Advanced Esophageal Cancer Compared with Conventional Concurrent Chemoradiotherapy with Cisplatin and 5-fluorouracil. J. Cancer 2018, 9, 2765–2772. [Google Scholar] [CrossRef] [PubMed]
- Zenda, S.; Kojima, T.; Kato, K.; Izumi, S.; Ozawa, T.; Kiyota, N.; Katada, C.; Tsushima, T.; Ito, Y.; Akimoto, T.; et al. Multicenter Phase 2 Study of Cisplatin and 5-Fluorouracil with Concurrent Radiation Therapy as an Organ Preservation Approach in Patients with Squamous Cell Carcinoma of the Cervical Esophagus. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 976–984. [Google Scholar] [CrossRef]
- Haefner, M.F.; Lang, K.; Verma, V.; Koerber, S.A.; Uhlmann, L.; Debus, J.; Sterzing, F. Neoadjuvant versus definitive chemoradiotherapy for locally advanced esophageal cancer: Outcomes and patterns of failure. Strahlenther. Onkol. 2018, 194, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Vellayappan, B.A.; Soon, Y.Y.; Ku, G.Y.; Leong, C.N.; Lu, J.J.; Tey, J.C. Chemoradiotherapy versus chemoradiotherapy plus surgery for esophageal cancer. Cochrane Database Syst. Rev. 2017, 8, CD010511. [Google Scholar] [CrossRef]
- Lee, D.J.; Harris, A.; Gillette, A.; Munoz, L.; Kashima, H. Carcinoma of the cervical esophagus: Diagnosis, management, and results. South Med. J. 1984, 77, 1365–1367. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, K.; Tsubosa, Y.; Matsuda, S.; Kawamorita, K.; Niihara, M.; Tsushima, T.; Yokota, T.; Sato, H.; Onozawa, Y.; Ogawa, H.; et al. Comparison of curative surgery and definitive chemoradiotherapy as initial treatment for patients with cervical esophageal cancer. Dis. Esophagus 2017, 30, 1–5. [Google Scholar] [CrossRef]
- Valmasoni, M.; Pierobon, E.S.; Zanchettin, G.; Briscolini, D.; Moletta, L.; Ruol, A.; Salvador, R.; Merigliano, S. Cervical Esophageal Cancer Treatment Strategies: A Cohort Study Appraising the Debated Role of Surgery. Ann. Surg. Oncol. 2018, 25, 2747–2755. [Google Scholar] [CrossRef]
- Pignon, J.P.; le Maitre, A.; Maillard, E.; Bourhis, J.; Group, M.-N.C. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef]
- Shimada, H.; Kitabayashi, H.; Nabeya, Y.; Okazumi, S.; Matsubara, H.; Funami, Y.; Miyazawa, Y.; Shiratori, T.; Uno, T.; Itoh, H.; et al. Treatment response and prognosis of patients after recurrence of esophageal cancer. Surgery 2003, 133, 24–31. [Google Scholar] [CrossRef]
- Shimada, H.; Okazumi, S.; Matsubara, H.; Nabeya, Y.; Shiratori, T.; Shimizu, T.; Shuto, K.; Hayashi, H.; Ochiai, T. Impact of the number and extent of positive lymph nodes in 200 patients with thoracic esophageal squamous cell carcinoma after three-field lymph node dissection. World J. Surg. 2006, 30, 1441–1449. [Google Scholar] [CrossRef]
- Tachibana, M.; Dhar, D.K.; Kinugasa, S.; Yoshimura, H.; Shibakita, M.; Ohno, S.; Ueda, S.; Fujii, T.; Kohno, H.; Nagasue, N. Surgical treatment for locally advanced (T4) squamous cell carcinoma of the thoracic esophagus. Dysphagia 2002, 17, 255–261. [Google Scholar] [CrossRef]
- Ishikawa, K.; Nakamatsu, K.; Shiraishi, O.; Yasuda, T.; Nishimura, Y. Clinical results of definitive-dose (50 Gy/25 fractions) preoperative chemoradiotherapy for unresectable esophageal cancer. Int. J. Clin. Oncol. 2015, 20, 531–537. [Google Scholar] [CrossRef]
- Okamoto, H.; Taniyama, Y.; Sakurai, T.; Heishi, T.; Teshima, J.; Sato, C.; Maruyama, S.; Ito, K.; Onodera, Y.; Konno-Kumagai, T.; et al. Definitive chemoradiotherapy with docetaxel, cisplatin, and 5-fluorouracil (DCF-R) for advanced cervical esophageal cancer. Esophagus 2018, 15, 281–285. [Google Scholar] [CrossRef]
- Edge, S.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.; Trotti, A. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Chen, Y.H.; Lu, H.I.; Chien, C.Y.; Lo, C.M.; Wang, Y.M.; Chou, S.Y.; Su, Y.Y.; Shih, L.H.; Li, S.H. Treatment Outcomes of Patients with Locally Advanced Synchronous Esophageal and Head/Neck Squamous Cell Carcinoma Receiving Curative Concurrent Chemoradiotherapy. Sci. Rep. 2017, 7, 41785. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.H.; Lu, H.I.; Lo, C.M.; Wang, Y.M.; Chou, S.Y.; Hsiao, C.C.; Shih, L.H.; Chen, S.W.; Li, S.H. Neck Lymph Node Metastasis as A Poor Prognostic Factor in Thoracic Esophageal Squamous Cell Carcinoma Patients Receiving Concurrent Chemoradiotherapy: A Propensity Score-Matched Analysis. Sci. Rep. 2018, 8, 15073. [Google Scholar] [CrossRef]
- Chen, Y.H.; Lu, H.I.; Lo, C.M.; Wang, Y.M.; Chou, S.Y.; Huang, C.H.; Shih, L.H.; Chen, S.W.; Li, S.H. The clinical impact of supraclavicular lymph node metastasis in patients with locally advanced esophageal squamous cell carcinoma receiving curative concurrent chemoradiotherapy. PLoS ONE 2018, 13, e0198800. [Google Scholar] [CrossRef]
- Chen, Y.H.; Lu, H.I.; Wang, Y.M.; Lo, C.M.; Chou, S.Y.; Huang, C.H.; Shih, L.H.; Chen, S.W.; Li, S.H. The prognostic significance of celiac lymph node metastasis in patients with locally advanced esophageal squamous cell carcinoma receiving curative concurrent chemoradiotherapy. Oncotarget 2017, 8, 96190–96202. [Google Scholar] [PubMed] [Green Version]
- Wu, C.C.; Li, S.H.; Lu, H.I.; Lo, C.M.; Wang, Y.M.; Chou, S.Y.; Chen, Y.H. Inflammation-based prognostic scores predict the prognosis of locally advanced cervical esophageal squamous cell carcinoma patients receiving curative concurrent chemoradiotherapy: A propensity score-matched analysis. PeerJ 2018, 6, e5655. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Japan Esophageal, S. Japanese Classification of Esophageal Cancer, 11th Edition: Part II and III. Esophagus 2017, 14, 37–65. [Google Scholar] [CrossRef]
- Ohkura, Y.; Shindoh, J.; Ueno, M.; Iizuka, T.; Udagawa, H. Comparison of Outcome of Esophagectomy Versus Nonsurgical Treatment for Resectable Esophageal Cancer with Clinical Complete Response to Neoadjuvant Therapy. Ann. Surg. Oncol. 2018, 25, 2428–2433. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef]
- Ela Bella, A.J.; Zhang, Y.R.; Fan, W.; Luo, K.J.; Rong, T.H.; Lin, P.; Yang, H.; Fu, J.H. Maximum standardized uptake value on PET/CT in preoperative assessment of lymph node metastasis from thoracic esophageal squamous cell carcinoma. Chin. J. Cancer 2014, 33, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Lu, H.I.; Huang, S.C.; Hsu, C.C.; Chiu, N.T.; Wang, Y.M.; Chiu, Y.C.; Li, S.H. FDG PET using SUVmax for preoperative T-staging of esophageal squamous cell carcinoma with and without neoadjuvant chemoradiotherapy. BMC Med. Imaging 2017, 17, 1. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Cervical ESCC Group (N = 63) | Thoracic ESCC Group (N = 348) | p Value |
|---|---|---|---|
| Age (years) | |||
| <60 years | 37 (59%) | 242 (70%) | 0.09 |
| ≥60 years | 26 (41%) | 106 (30%) | |
| Sex | |||
| Male | 61 (97%) | 340 (98%) | 0.68 |
| Female | 2 (3%) | 8 (2%) | |
| T status | |||
| 1 | 0 (0%) | 13 (4%) | 0.001 * |
| 2 | 1 (1%) | 13 (4%) | |
| 3 | 13 (21%) | 144 (41%) | |
| 4a | 5 (8%) | 38 (11%) | |
| 4b | 44 (70%) | 140 (40%) | |
| N status | |||
| 0 | 5 (8%) | 5 (2%) | 0.023 * |
| 1 | 24 (38%) | 137 (39%) | |
| 2 | 23 (37%) | 136 (39%) | |
| 3 | 11 (17%) | 70 (20%) | |
| Tumor stage | |||
| IIIA | 7 (11%) | 80 (23%) | 0.012 * |
| IIIB | 5 (8%) | 54 (16%) | |
| IIIC | 51 (81%) | 214 (61%) | |
| Grade | |||
| 1 | 6 (12%) | 61 (18%) | 0.63 |
| 2 | 18 (35%) | 203 (58%) | |
| 3 | 27 (53%) | 84 (24%) | |
| Characteristics | Cervical ESCC Group (N = 63) | Thoracic ESCC Group # (N = 63) | p-Value |
| Age (years) | |||
| <60 years | 37 (59%) | 37 (59%) | 1.0 |
| ≥60 years | 26 (41%) | 26 (41%) | |
| Sex | |||
| Male | 61 (97%) | 61 (97%) | 1.0 |
| Female | 2 (3%) | 2 (3%) | |
| T status | |||
| 1 | 0 (0%) | 0 (0%) | 1.0 |
| 2 | 1 (1%) | 1 (1%) | |
| 3 | 13 (21%) | 13 (21%) | |
| 4a | 5 (8%) | 5 (8%) | |
| 4b | 44 (70%) | 44 (70%) | |
| N status | |||
| 0 | 5 (8%) | 5 (8%) | 1.0 |
| 1 | 24 (38%) | 24 (38%) | |
| 2 | 23 (37%) | 23 (37%) | |
| 3 | 11 (17%) | 11 (17%) | |
| Tumor stage | |||
| IIIA | 7 (11%) | 7 (11%) | 1.0 |
| IIIB | 5 (8%) | 5 (8%) | |
| IIIC | 51 (81%) | 51 (81%) | |
| Grade | |||
| 1 | 6 (12%) | 6 (12%) | 1.0 |
| 2 | 18 (35%) | 18 (35%) | |
| 3 | 27 (53%) | 27 (53%) |
| Characteristics | No. of Patients | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| Median OS (Months) | p-Value | HR (95% CI) | p-Value | ||
| Age (years) | |||||
| <60 years | 37 (59%) | 21.6 | 0.44 | ||
| ≥60 years | 26 (41%) | 12.0 | |||
| T status | |||||
| 2 + 3 + 4a | 19 (30%) | 26.1 | 0.035 * | 0.47 (0.23–0.98) | 0.044 * |
| 4b | 44 (70%) | 17.3 | |||
| N status | |||||
| 0 + 1 | 29 (46%) | 21.6 | 0.54 | ||
| 2 + 3 | 34 (54%) | 19.1 | |||
| Tumor stage | |||||
| IIIA + IIIB | 12 (19%) | 25.3 | 0.56 | ||
| IIIC | 51 (81%) | 21.0 | |||
| Grade | |||||
| 1 + 2 | 50 (79%) | 22.2 | 0.015 * | 0.42 (0.20–0.89) | 0.023 * |
| 3 | 13 (21%) | 11.3 | |||
| Response | Cervical ESCC Group (N = 63) | Thoracic ESCC Group # (N = 63) | p-Value |
|---|---|---|---|
| Complete response (CR) | 21 (33%) | 10 (16%) | |
| Partial response (PR) | 27 (43%) | 30 (48%) | |
| Stable disease (SD) | 6 (10%) | 15 (23%) | |
| Progressive disease (PD) | 9 (14%) | 8 (13%) | |
| CR rate | 21 (33%) | 10 (16%) | 0.038 * |
| Response rate | |||
| CR + PR | 76% | 64% | 0.12 |
| Disease control rate | |||
| CR + PR + SD | 83% | 87% | 0.62 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-H.; Lu, H.-I.; Lo, C.-M.; Wang, Y.-M.; Chou, S.-Y.; Hsiao, C.-C.; Li, S.-H. The Clinical Outcomes of Locally Advanced Cervical Esophageal Squamous Cell Carcinoma Patients Receiving Curative Concurrent Chemoradiotherapy: A Population-Based Propensity Score-Matched Analysis. Cancers 2019, 11, 451. https://doi.org/10.3390/cancers11040451
Chen Y-H, Lu H-I, Lo C-M, Wang Y-M, Chou S-Y, Hsiao C-C, Li S-H. The Clinical Outcomes of Locally Advanced Cervical Esophageal Squamous Cell Carcinoma Patients Receiving Curative Concurrent Chemoradiotherapy: A Population-Based Propensity Score-Matched Analysis. Cancers. 2019; 11(4):451. https://doi.org/10.3390/cancers11040451
Chicago/Turabian StyleChen, Yen-Hao, Hung-I Lu, Chien-Ming Lo, Yu-Ming Wang, Shang-Yu Chou, Chang-Chun Hsiao, and Shau-Hsuan Li. 2019. "The Clinical Outcomes of Locally Advanced Cervical Esophageal Squamous Cell Carcinoma Patients Receiving Curative Concurrent Chemoradiotherapy: A Population-Based Propensity Score-Matched Analysis" Cancers 11, no. 4: 451. https://doi.org/10.3390/cancers11040451