
Measuring Experiential Avoidance: Evidence toward Multidimensional Predictors of Trauma Sequelae

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Analytic Strategy
3. Results
3.1. Bivariate Correlations
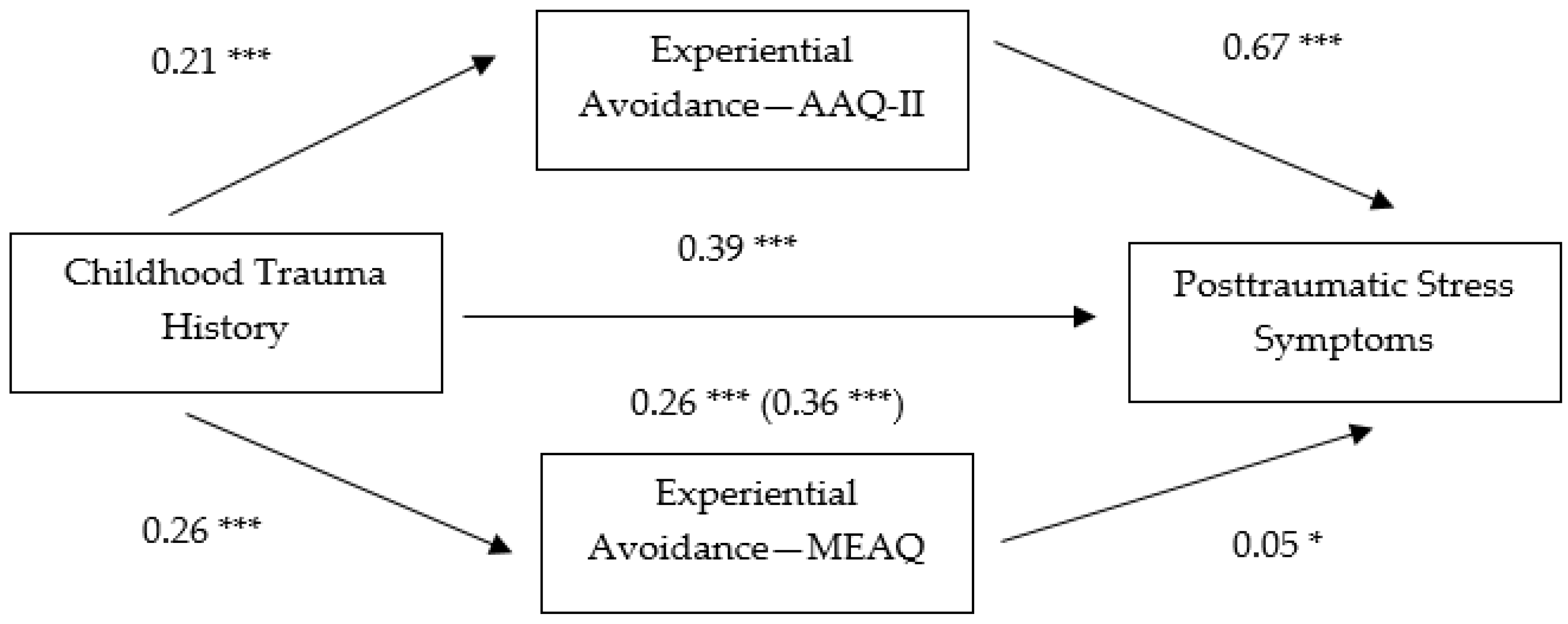
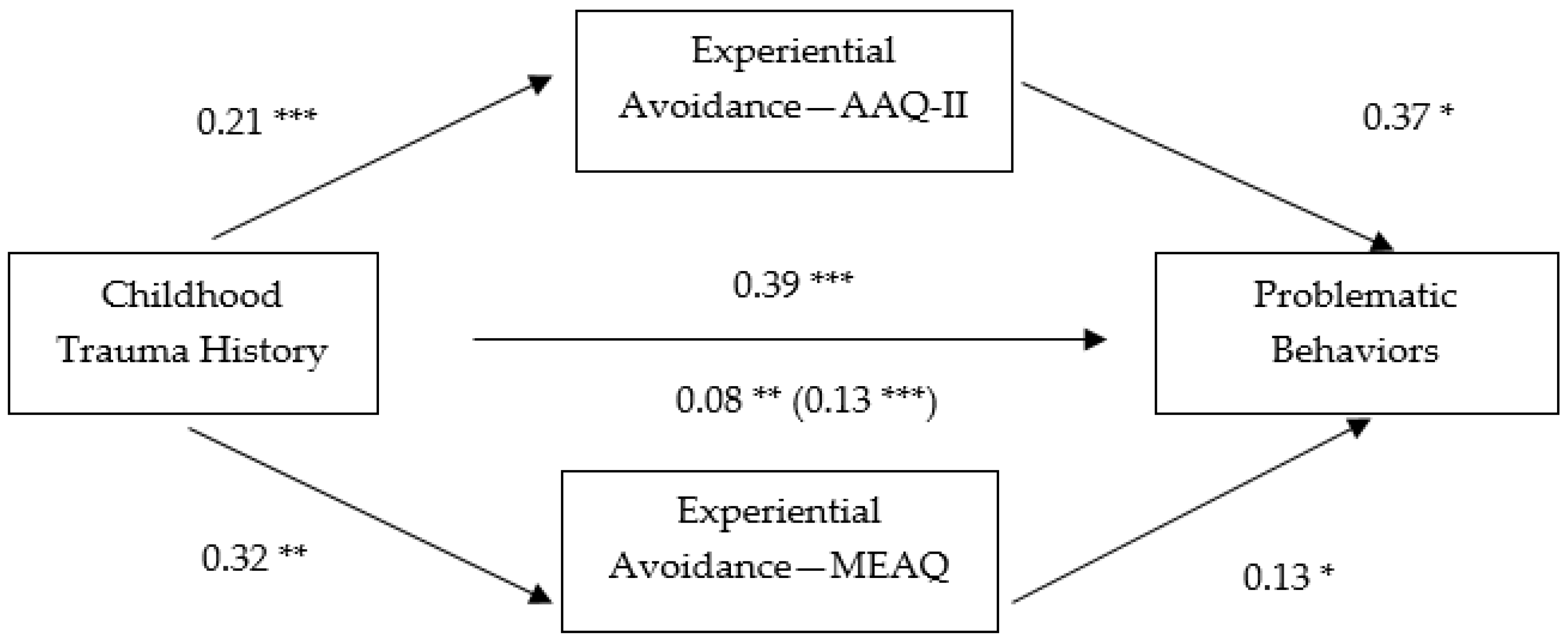
3.2. Non-Parametric Bootstrapping Analyses
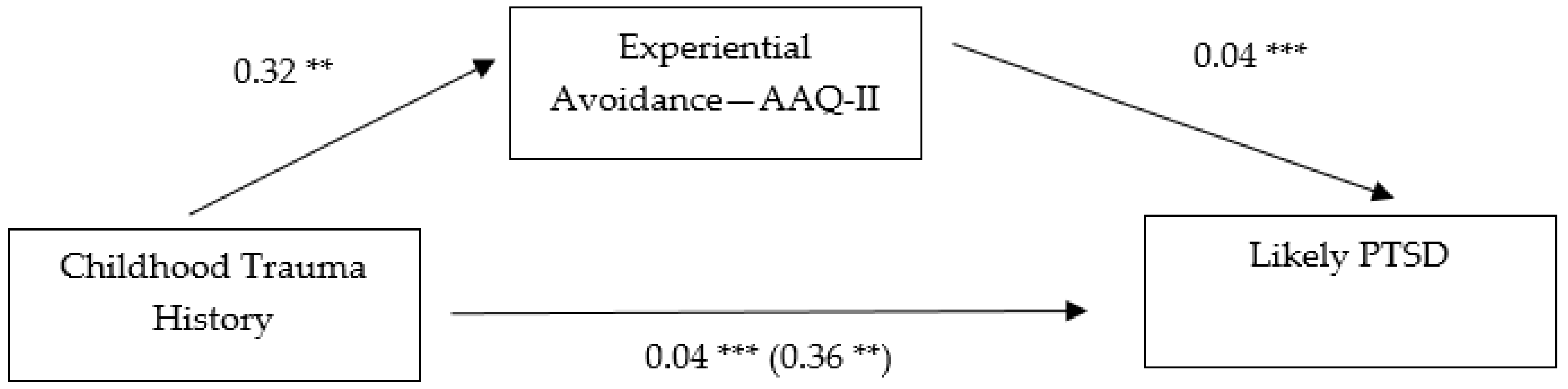
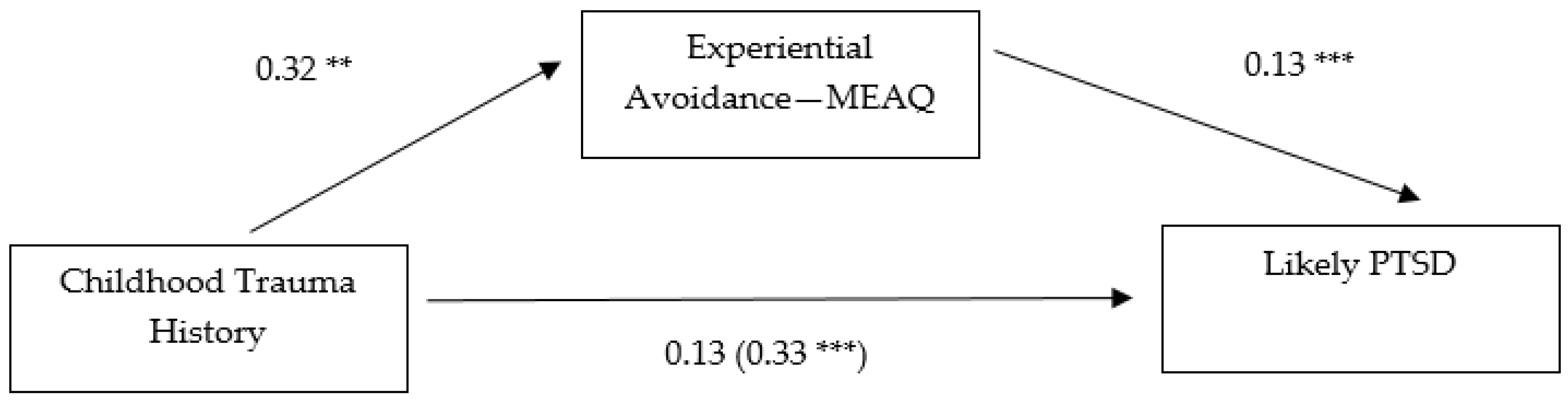
3.3. Likely PTSD Diagnosis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gámez, W.; Chmielewski, M.; Kotov, R.; Ruggero, C.; Watson, D. Development of a measure of experiential avoidance: the multidimensional experiential avoidance questionnaire. Psychol. Assess. 2011, 23, 692–713. [Google Scholar] [CrossRef] [PubMed]
- Mansell, W.; Harvey, A.; Watkins, E.; Shafran, R. Conceptual foundations of the transdiagnostic approach to CBT. J. Cogn. Psychother. 2009, 23, 6–19. [Google Scholar] [CrossRef]
- Chawla, N.; Ostafin, B. Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. J. Clin. Psychol. 2007, 63, 871–890. [Google Scholar] [CrossRef] [PubMed]
- Kashdan, T.B.; Barrios, V.; Forsyth, J.P.; Steger, M.F. Experiential avoidance as a generalized psychological vulnerability: Comparisons with coping and emotion regulation strategies. Behav. Res. Ther. 2006, 44, 1301–1320. [Google Scholar] [CrossRef] [PubMed]
- Wenzlaff, R.M.; Wegner, D.M. Paradoxical effects of thought suppression. J. Pers. Soc. Psychol. 1987, 53, 5–13. [Google Scholar]
- Giorgio, J.M.; Sanflippo, J.; Kleiman, E.; Reilly, D.; Bender, R.E.; Wagner, C.A.; Liu, R.T.; Alloy, L.B. An experiential avoidance conceptualization of depressive rumination: Three tests of the model. Behav. Res. Ther. 2010, 48, 1021–1031. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Orsillo, S.M.; Roemer, L.; Allen, B. Distress and avoidance in generalized anxiety disorder: exploring the relationships with intolerance of uncertainty and worry. Cog. Behav. Ther. 2010, 39, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.L.; Waltz, J. Mindfulness and experiential avoidance as predictors of posttraumatic stress disorder avoidance symptom severity. J. Anxiety Disord. 2010, 24, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, R.D.; Arens, A.M.; Kuvaas, N.J.; Williams, T.J.; Kilwein, T.M. Problematic alcohol use, trauma history, and PTSD symptom level: A path analysis. J. Dual Diag. 2013, 9, 281–291. [Google Scholar] [CrossRef]
- Zettle, R.D.; Barner, S.L.; Gird, S.R.; Boone, L.T.; Renollet, D.L.; Burdsal, C.A. A psychological biathlon: The relationship between level of experiential avoidance and perseverance on two challenging tasks. Psychol. Rec. 2012, 62, 433–445. [Google Scholar]
- Amstadter, A.B.; Vernon, L.L. A preliminary examination of thought suppression, emotion regulation, and coping in a trauma exposed sample. J. Aggress. Maltreat. Trauma 2008, 17, 279–295. [Google Scholar] [CrossRef] [PubMed]
- Barrett, R. Experiential avoidance: Associations with childhood trauma, internalised shame, psychopathology and maladaptive behaviours. Ph.D. Thesis, University of Southampton, Southampton, UK, May 2010. [Google Scholar]
- Kashdan, T.B.; Kane, J.Q. Posttraumatic distress and the presence of posttraumatic growth and meaning in life: Experiential avoidance as a moderator. Pers. Indiv. Differen. 2010, 50, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Kumpula, M.J.; Orcutt, H.K.; Bardeen, J.R.; Varkovitzky, R.L. Peritraumatic dissociation and experiential avoidance as prospective predictors of posttraumatic stress symptoms. J. Abnorm. Psychol. 2011, 120, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.K.; Pickett, S.M.; Orcutt, H.K. Experiential avoidance as a mediator in the relationship between childhood psychological abuse and current mental health symptoms in college students. J. Emot. Abuse 2006, 6, 67–85. [Google Scholar] [CrossRef]
- Batten, S.V.; Follette, V.M.; Aban, I.B. Experiential avoidance and high-risk sexual behavior in survivors of child sexual abuse. J. Child Sex. Abuse 2001, 10, 101–120. [Google Scholar] [CrossRef]
- Levin, M.E.; Lillis, J.; Seeley, J.; Hayes, S.C.; Pistorello, J.; Biglan, A. Exploring the relationship between experiential avoidance, alcohol use disorders, and alcohol-related problems among first-year college students. J. Am. Coll. Health 2012, 60, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, M.Z.; Polusny, M.A.; Follette, V.M. Avoidance mediates the relationship between perceived criticism in the family of origin and psychological distress in adulthood. J. Emot. Abuse 2006, 6, 87–102. [Google Scholar] [CrossRef]
- Marx, B.P.; Sloan, D.M. The role of emotion in the psychological functioning of adult survivors of childhood sexual abuse. Behav. Ther. 2002, 33, 563–577. [Google Scholar] [CrossRef]
- Polusny, M.A.; Rosenthal, M.Z.; Aban, I.; Follette, V.M. Experiential avoidance as a mediator of the effects of adolescent sexual victimization on negative adult outcomes. Viol. Vict. 2004, 19, 109–120. [Google Scholar] [CrossRef]
- Rosenthal, Z.M.; Rasmussen Hall, M.L.; Palm, K.M.; Batten, S.V.; Follette, V.M. Chronic avoidance helps explain the relationship between severity of childhood sexual abuse and psychological distress in adulthood. J. Child Sex. Abuse 2005, 14, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Kingston, J.; Clarke, S.; Remington, B. Experiential avoidance and problem behavior: A mediational analysis. Behav. Mod. 2010, 34, 145–163. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, A.; Lejoyeux, M. Internet addiction or excessive internet use. Am. J. Drug Alcohol Abuse 2010, 36, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: A revised measure of psychological flexibility and experiential avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.M.; Loverich, T.M. An examination of experiential avoidance as a vulnerability factor for posttraumatic stress symptoms and excessive behaviors in parent and adult child dyads. Unpublished manuscript. 2014. [Google Scholar]
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Domino, J.L. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD, 2014. Available online: http://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp (accessed on 3 June 2015). [Google Scholar]
- Kingston, J.L.; Clarke, S.; Ritchie, T.D.; Remington, R.E. Developing and validating the “Composite Measure of Problem Behaviors”. J. Clin. Psychol. 2011, 67, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Mertler, C.A.; Vannatta, R.A. Advanced and Multivariate Statistical Methods: Practical Application and Interpretation, 3rd ed.; Pyrczak: Los Angeles, CA, USA, 2005. [Google Scholar]
- Schafer, J.L.; Graham, J.W. Missing data: Our view of the state of the art. Psychol. Meth. 2002, 7, 147–177. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Comm. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Gámez, W.; Chmielewski, M.; Kotov, R.; Ruggero, C.; Suzuki, N.; Watson, D. The Brief Experiential Avoidance Questionnaire: Development and initial validation. Psychol. Assess. 2014, 26, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C. Acceptance and Commitment Therapy and the new behavior therapies: Mindfulness, acceptance and relationship. In Mindfulness and Acceptance: Expanding the Cognitive Behavioral Tradition; Hayes, S.C., Follette, V.M., Linehan, M., Eds.; Guilford: New York, NY, USA, 2004; pp. 1–29. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | 1 | 2 | 3 | 4 | M(SD) | Range |
|---|---|---|---|---|---|---|
| (1) MEAQ | - | 226 (28.86) | 114–332 | |||
| (2) AAQ-II | 0.61 ** | - | 22 (9.16) | 7–47 | ||
| (3) CTQ-SF | 0.24 * | 0.37 ** | - | 51 (15.39) | 34–122 | |
| (4) PCL | 0.39 ** | 0.62 ** | 0.40 ** | - | 39 (14.76) | 16–76 |
| (5) CMPB | 0.29 ** | 0.32 ** | 0.28 ** | 0.37 ** | 115 (24.24) | 72–201 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewis, M.; Naugle, A. Measuring Experiential Avoidance: Evidence toward Multidimensional Predictors of Trauma Sequelae. Behav. Sci. 2017, 7, 9. https://doi.org/10.3390/bs7010009
Lewis M, Naugle A. Measuring Experiential Avoidance: Evidence toward Multidimensional Predictors of Trauma Sequelae. Behavioral Sciences. 2017; 7(1):9. https://doi.org/10.3390/bs7010009
Chicago/Turabian StyleLewis, Meaghan, and Amy Naugle. 2017. "Measuring Experiential Avoidance: Evidence toward Multidimensional Predictors of Trauma Sequelae" Behavioral Sciences 7, no. 1: 9. https://doi.org/10.3390/bs7010009