
The Challenge of Diffusion Magnetic Resonance Imaging in Cerebral Palsy: A Proposed Method to Identify White Matter Pathways
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Acquisition
2.3. Data Preprocessing
2.3.1. Data Correction
2.3.2. Diffusion Metrics
2.3.3. Whole Brain Tractography
2.3.4. Tractogram Extraction
Automatic Extraction
Atlas-Based Customized Extraction
- Atlas registration
- 2.
- ROI and Bundle Extraction
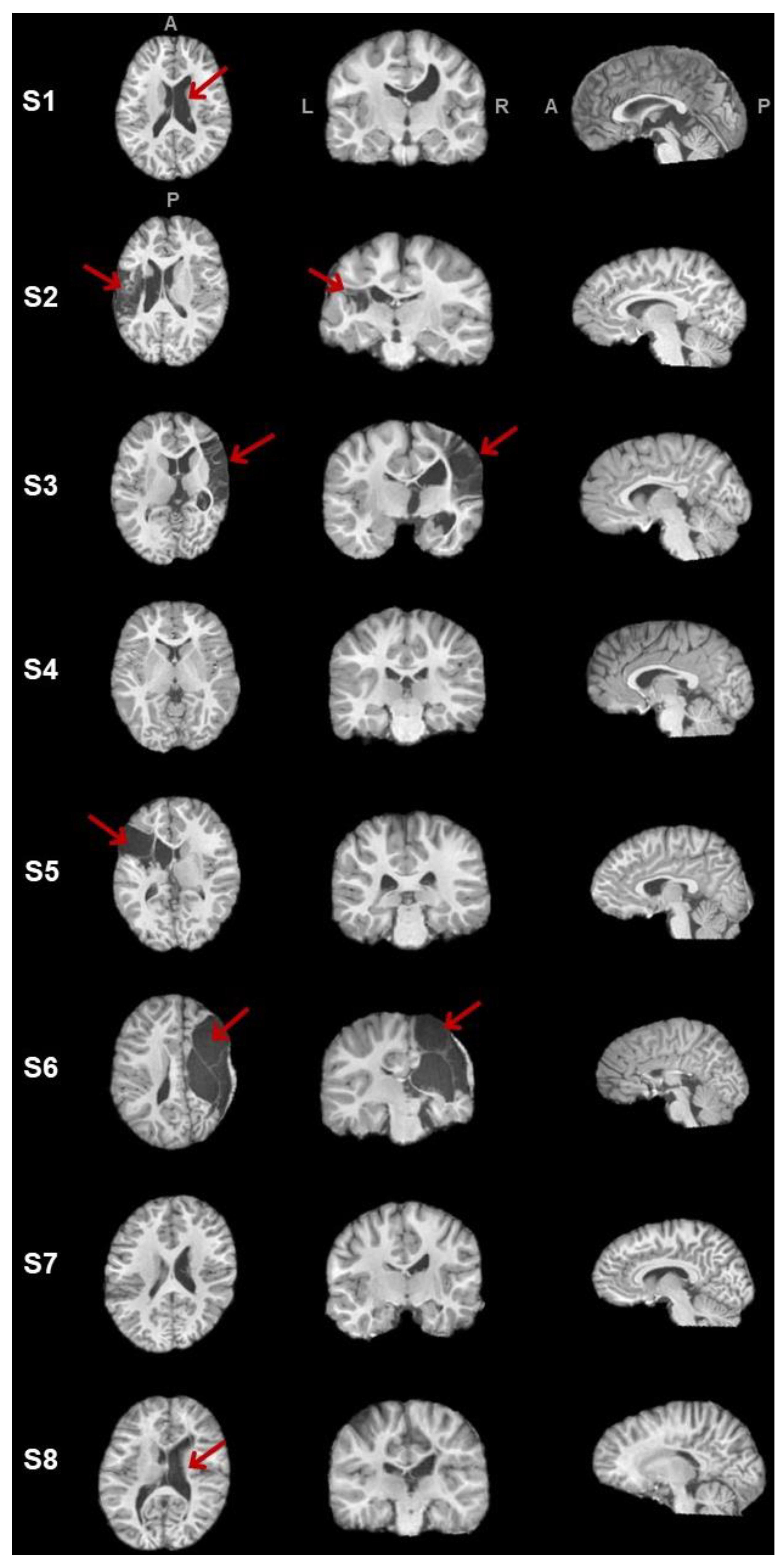
2.4. Lesion Characterization
2.5. Tracometry
3. Results
3.1. Clinical Data
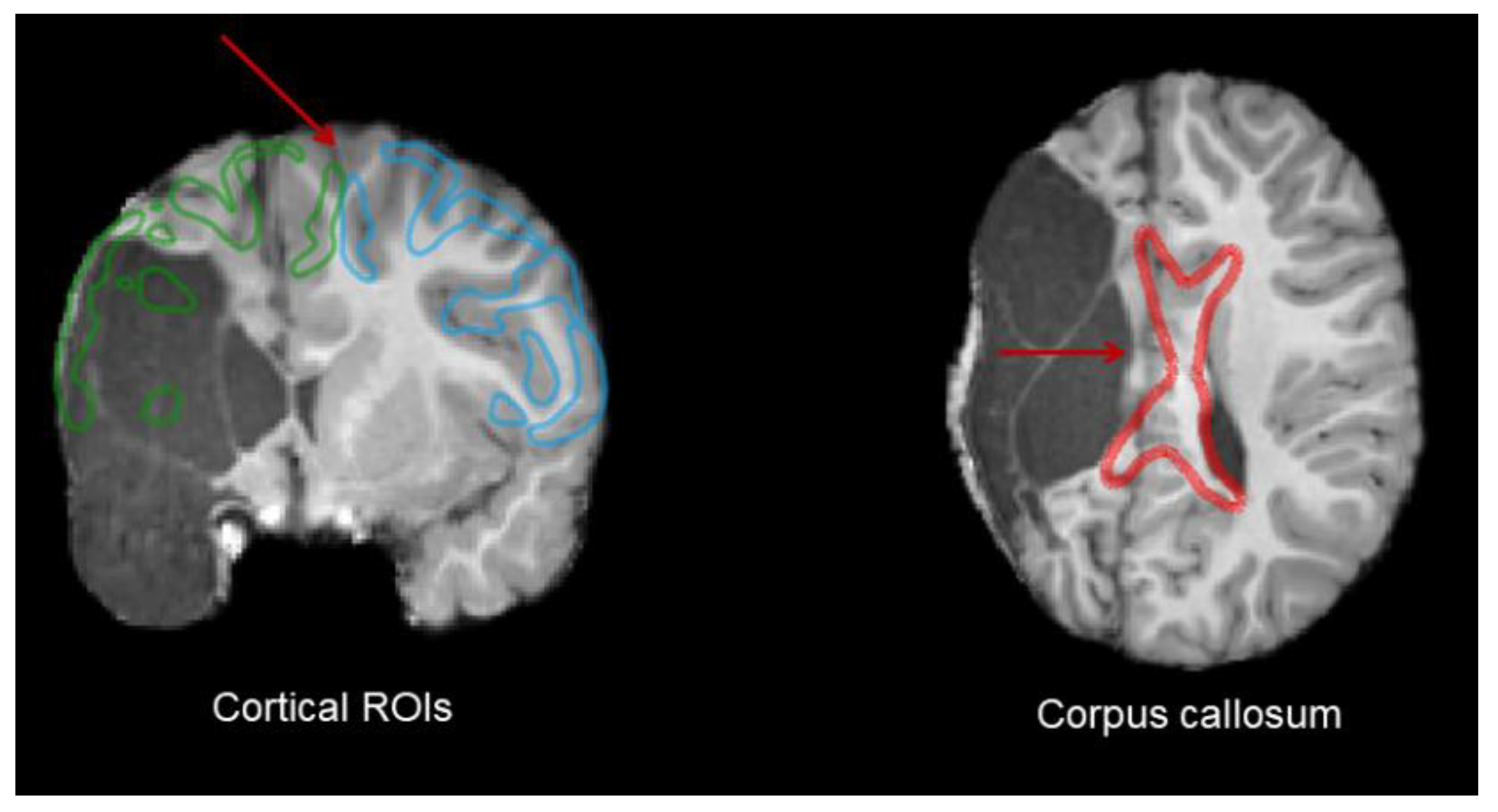
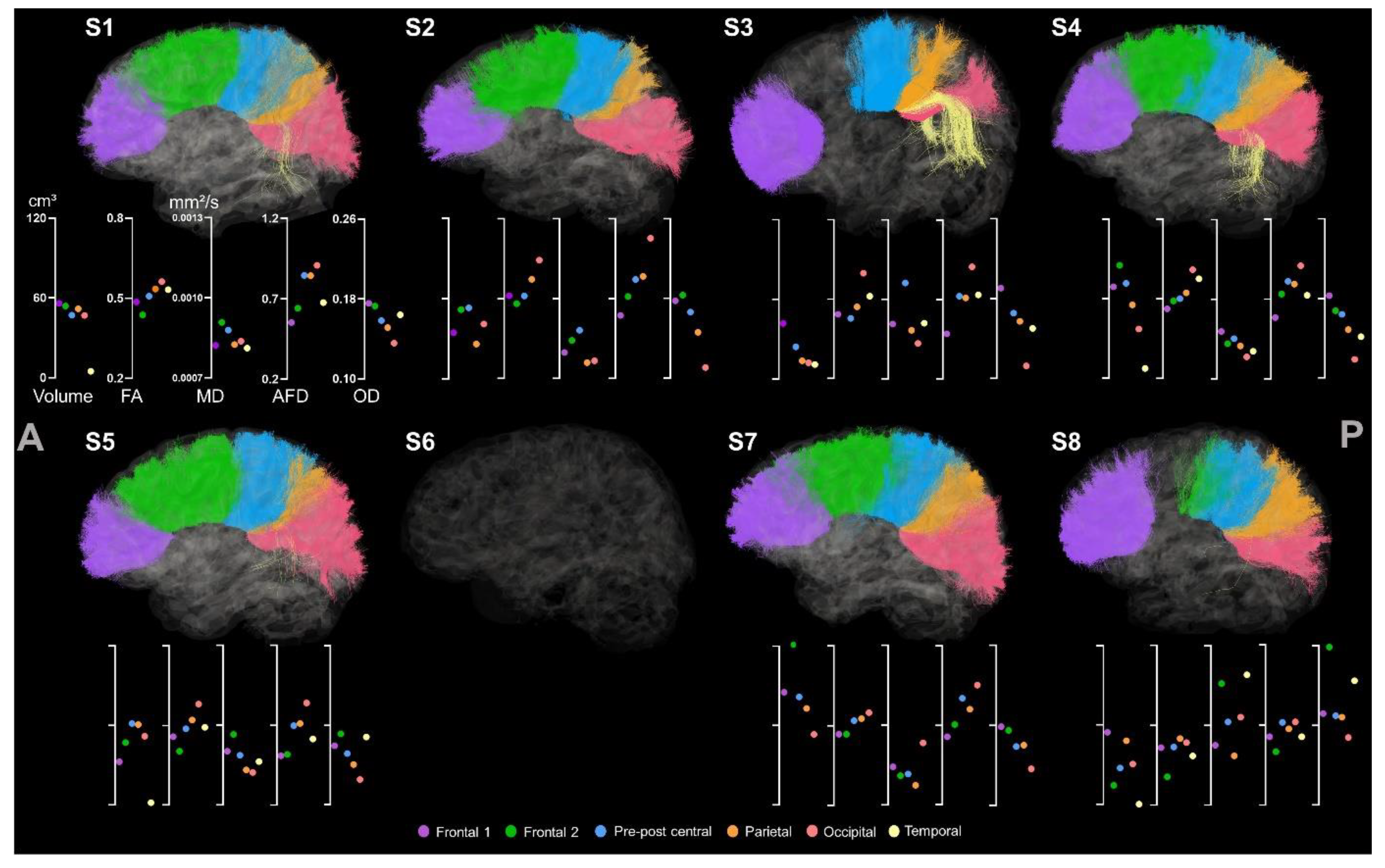
3.2. Automatic Tract Extraction
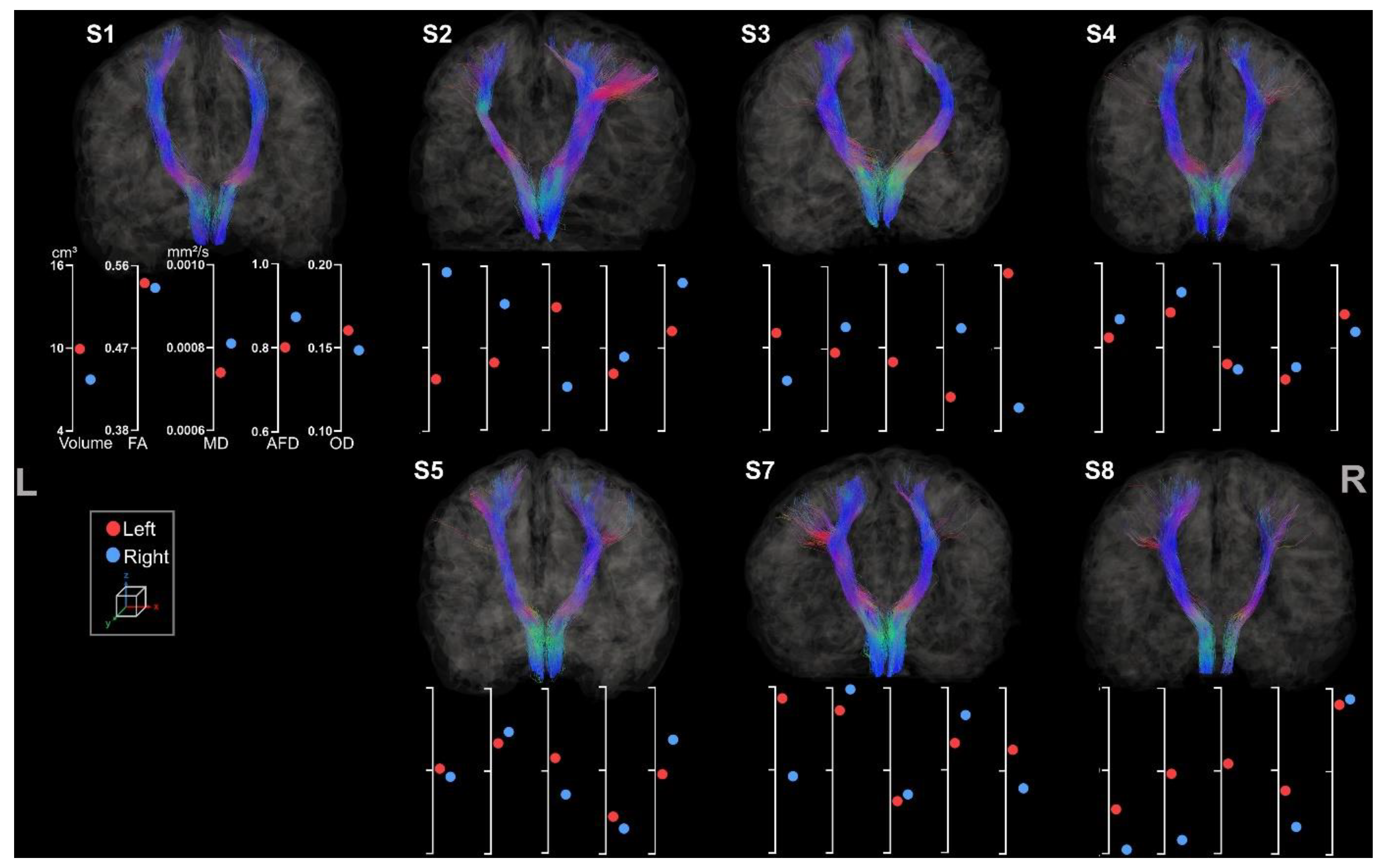
3.2.1. Corticospinal Tracts
3.2.2. Corpus Callosum
3.3. Atlas-Based Tracts Extraction
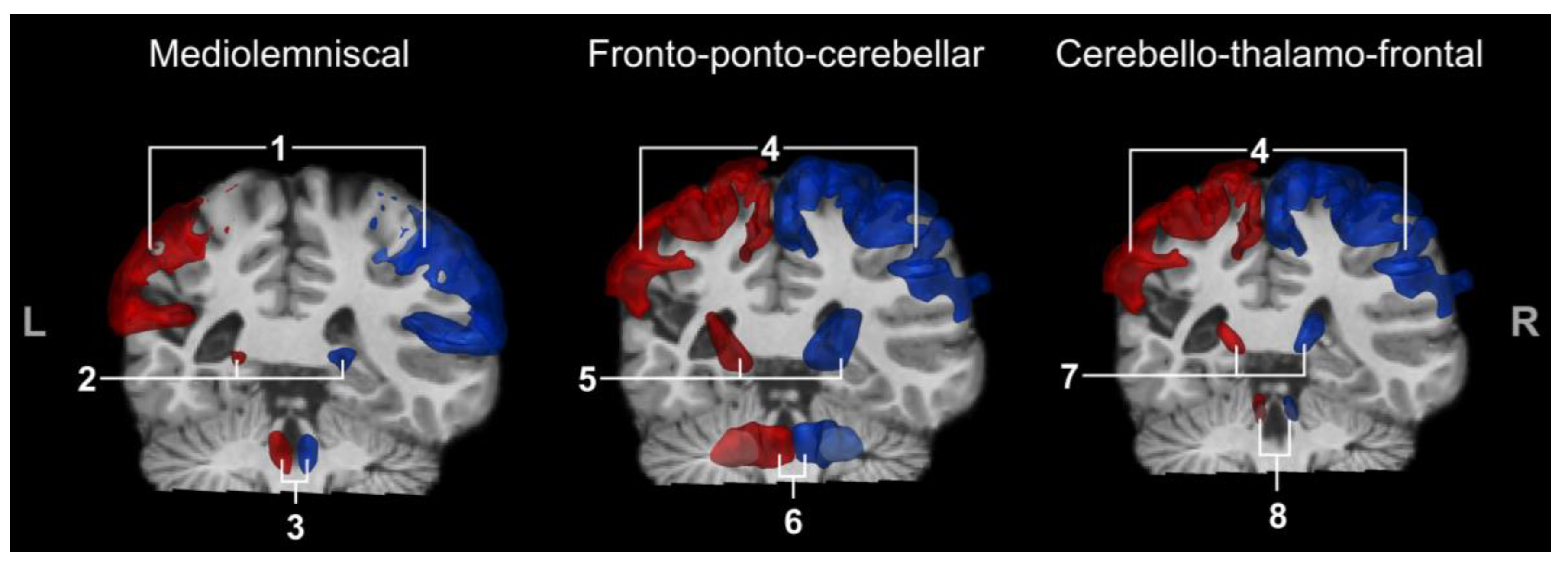
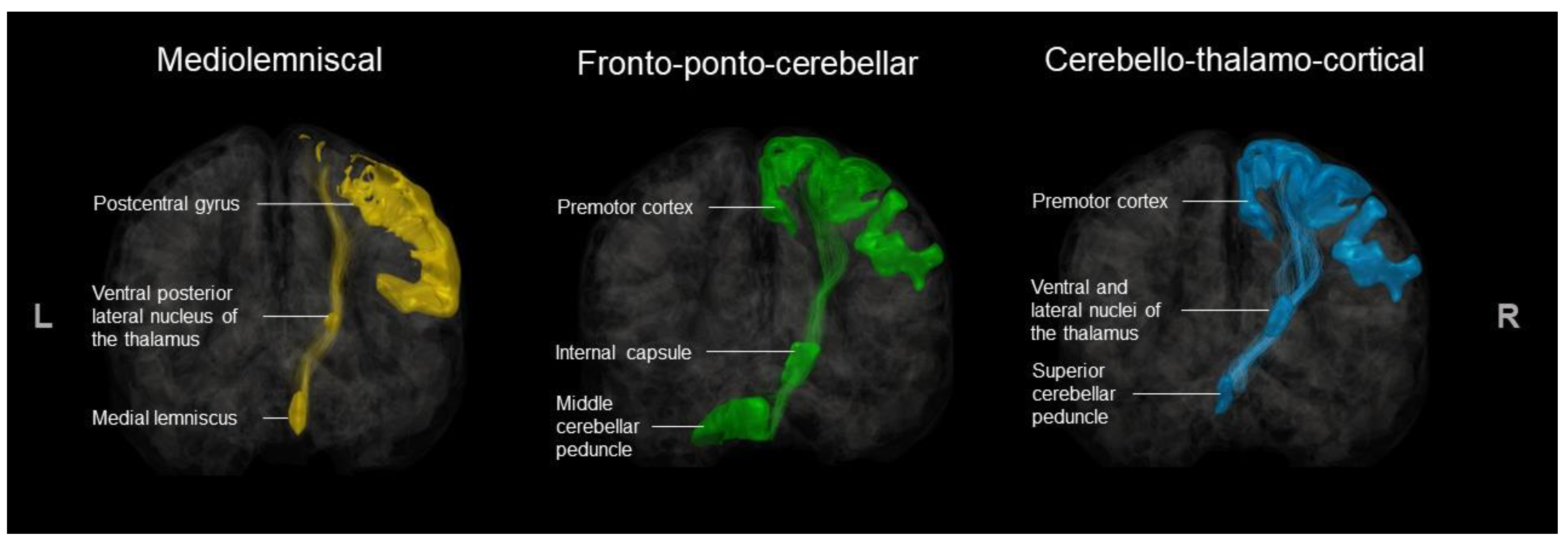
3.3.1. Medio-Lemniscal Tracts Extraction
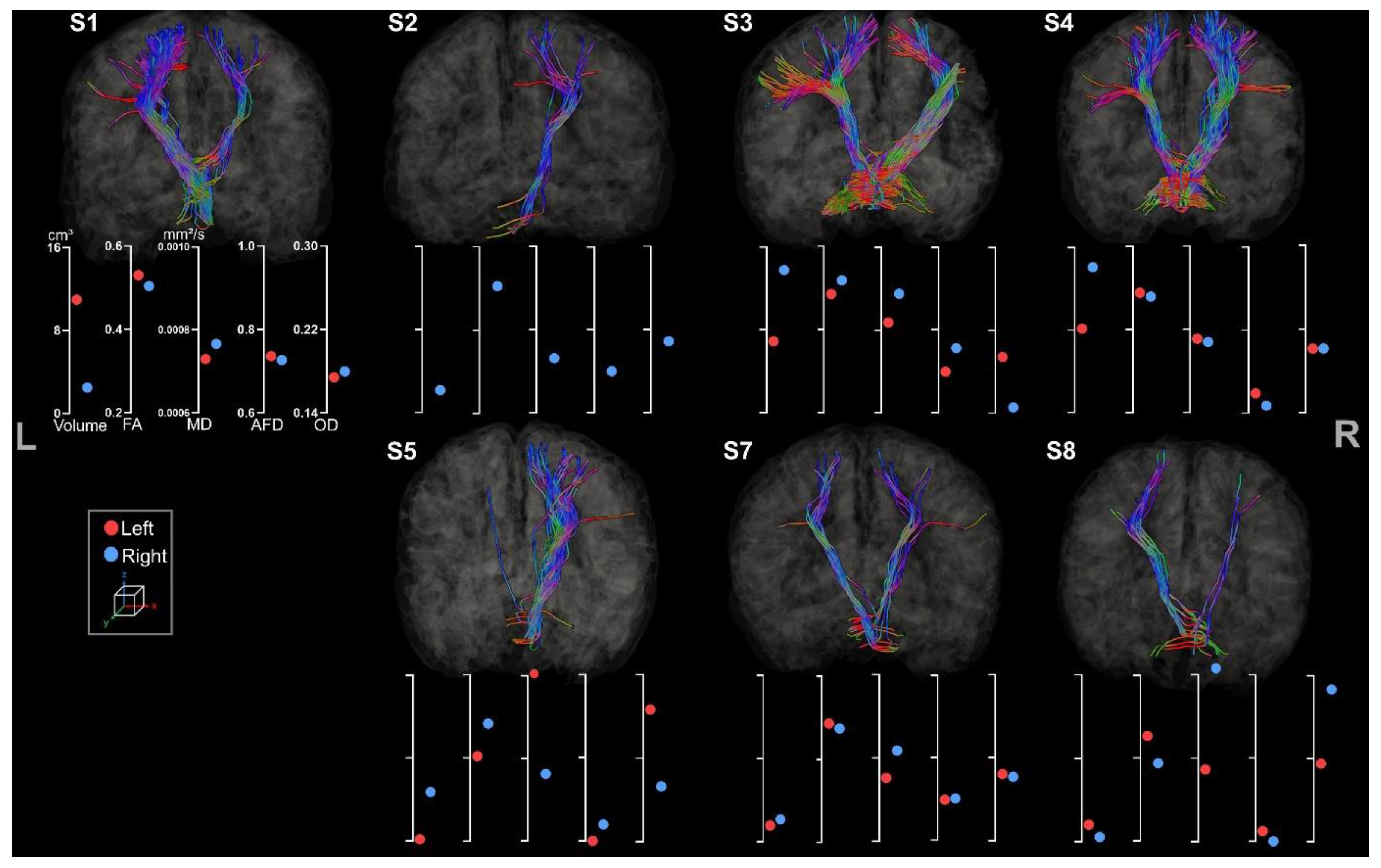
3.3.2. Fronto-Ponto-Cerebellar Tracts
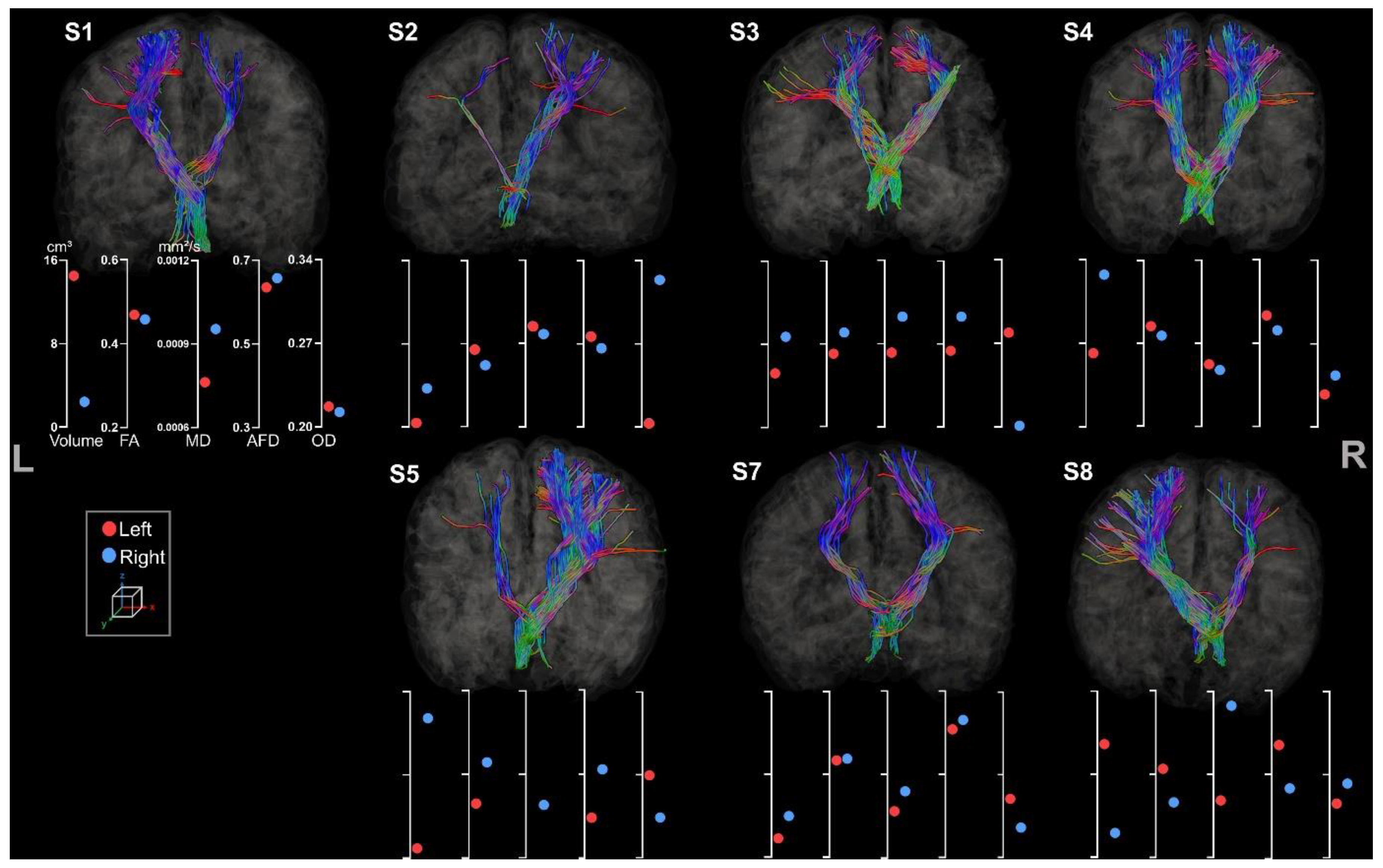
3.3.3. Cerebello-Thalamo-Frontal Tracts
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Shevell, M.; Dagenais, L.; Oskoui, M. The epidemiology of cerebral palsy: New perspectives from a Canadian registry. Semin. Pediatr. Neurol. 2013, 20, 60–64. [Google Scholar] [CrossRef]
- Oskoui, M.; Coutinho, F.; Dykeman, J.; Jetté, N.; Pringsheim, T. An update on the prevalence of cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2013, 55, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy. Dev. Med. Child Neurol. Suppl. 2006, 109 (Suppl. S109), 8–14. [Google Scholar]
- Mailleux, L.; Franki, I.; Emsell, L.; Peedima, M.L.; Fehrenbach, A.; Feys, H.; Ortibus, E. The relationship between neuroimaging and motor outcome in children with cerebral palsy: A systematic review—Part B diffusion imaging and tractography. Res. Dev. Disabil. 2020, 97, 103569. [Google Scholar] [CrossRef] [PubMed]
- Mailleux, L.; Simon-martinez, C.; Klingels, K.; Jaspers, E. Structural Brain Damage and Upper Limb Kinematics in Children with Unilateral Cerebral Palsy. Front. Hum. Neurosci. 2017, 11, 607. [Google Scholar] [CrossRef]
- Robert, M.T.; Gutterman, J.; Ferre, C.L.; Chin, K.; Brandao, M.; Gordon, A.M.; Friel, K. Corpus Callosum Integrity Relates to Improvement of Upper-Extremity Function Following Intensive Rehabilitation in Children With Unilateral Spastic Cerebral Palsy. Neurorehabilit. Neural Repair 2021, 35, 534–544. [Google Scholar] [CrossRef]
- Hung, Y.; Robert, M.T.; Friel, K.M.; Gordon, A.M.; Rose, J. Relationship Between Integrity of the Corpus Callosum and Bimanual Coordination in Children With Unilateral Spastic Cerebral Palsy. Front. Hum. Neurosci. 2019, 13, 334. [Google Scholar] [CrossRef]
- NINDS. Cerebral Palsy: Hope Through Research. 2013. Available online: https://www.ninds.nih.gov/health-information/patient-caregiver-education/hope-through-research/cerebral-palsy-hope-through-research (accessed on 18 September 2023).
- Ashwal, R.S.; Russman, B.S.; Blasco, P.A.; Miller, G.; Sandler, A.; Shevell, M.; Stevenson, R.D. Practice parameter, diagnostic assessment of the child with cerebral palsy, report. Neurology 2004, 62, 851–863. [Google Scholar] [CrossRef]
- Le Bihan, D.; Breton, E. In vivo magnetic resonance imaging of diffusion. Comptes Rendus Seances L’academie Sci. 1985, 301, 1109–1112. [Google Scholar]
- Beaulieu, C. The basis of anisotropic water diffusion in the nervous system ± a technical review. NMR Biomed. 2002, 15, 435–455. [Google Scholar] [CrossRef]
- Mori, S.; Zhang, J. Principles of Diffusion Tensor Imaging and Its Applications to Basic Neuroscience Research. Neuron 2006, 51, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Basser, P.J.; Mattiello, J.; Lebihan, D. MR Diffusion Tensor Spectroscopy and Imaging. Biophys. J. 1994, 66, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Arrigoni, F.; Peruzzo, C.; Gagliardi, C.; Maghini, P.; Colombo, P.; Servodio Iammarrone, F.; Pierpaoli, C.; Triulzi, F.; Turconi, A.C. Whole-Brain DTI Assessment of White Matter Damage in Children with Bilateral Cerebral Palsy: Evidence of Involvement beyond the Primary Target of the Anoxic Insult. Am. J. Neuroradiol. 2016, 37, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kwon, Y.M.; Son, S.M. Motor function outcomes of pediatric patients with hemiplegic cerebral palsy after rehabilitation treatment: A diffusion tensor imaging study. Neural Regen. Res. 2015, 10, 624. [Google Scholar] [CrossRef] [PubMed]
- Kuczynski, A.M.; Dukelow, S.P.; Hodge, J.A.; Carlson, H.L.; Lebel, C.; Semrau, J.A.; Kirton, A. Corticospinal tract diffusion properties and robotic visually guided reaching in children with hemiparetic cerebral palsy. Hum. Brain Mapp. 2018, 39, 1130–1144. [Google Scholar] [CrossRef]
- Mahanna, A.M.; El-toukhy, N.A.E.; Mousa, A.E.; Megahed, K.F. Does motor deficit in children with cerebral palsy correlate with diffusion tensor metrics abnormalities in thalamocortical pathways? Egypt. J. Radiol. Nucl. Med. 2021, 52, 82. [Google Scholar] [CrossRef]
- Bleyenheuft, Y.; Dricot, L.; Gilis, N.; Kuo, H.-C.; Grandin, C.; Bleyenheuft, C.; Gordon, A.M.; Friel, K.M. Capturing neuroplastic changes after bimanual intensive rehabilitation in children with unilateral spastic cerebral palsy: A combined DTI, TMS and fMRI pilot study. Res. Dev. Disabil. 2015, 43, 136–149. [Google Scholar] [CrossRef]
- Rickards, T.; Sterling, C.; Taub, E.; Perkins-Hu, C.; Gauthier, L.; Graham, M.; Griffin, A.; Davis, D.; Mark, V.W.; Uswatte, G. Diffusion tensor imaging study of the response to constraint-induced movement therapy of children with hemiparetic cerebral palsy and adults with chronic stroke. Arch. Phys. Med. Rehabil. 2013, 95, 506–514. [Google Scholar] [CrossRef]
- Friel, K.M.; Ching, H.; Carmel, J.B.; Rowny, S.B.; Gordon, A.M. Improvements in hand function after intensive bimanual training are not associated with corticospinal tract dysgenesis in children with unilateral cerebral palsy. Exp. Brain Res. 2014, 232, 2001–2009. [Google Scholar] [CrossRef]
- Papadelis, C.; Kaye, H.; Shore, B.; Snyder, B.; Grant, P.E.; Rotenberg, A. Maturation of Corticospinal Tracts in Children With Hemiplegic Cerebral Palsy Assessed by Diffusion Tensor Imaging and Transcranial Magnetic Stimulation. Front. Hum. Neurosci. 2019, 13, 254. [Google Scholar] [CrossRef]
- Curran, K.M.; Emsell, L.; Leemans, A. Quantitative DTI measures. In Diffusion Tensor Imaging: A Practical Handbook; Springer: Berlin/Heidelberg, Germany, 2016; pp. 65–87. [Google Scholar] [CrossRef]
- Hui, E.S.; Cheung, M.M.; Chan, K.C.; Wu, E.X. B-value dependence of DTI quantitation and sensitivity in detecting neural tissue changes. NeuroImage 2010, 49, 2366–2374. [Google Scholar] [CrossRef]
- Jones, M.; Cercignani, D.K. Twenty-five pitfalls in the analysis of diffusion MRI data. NMR Biomed. 2010, 23, 803–820. [Google Scholar] [CrossRef]
- Raffelt, D.; Tournier, J.D.; Rose, S.; Ridgway, G.R.; Henderson, R.; Crozier, S.; Salvado, O.; Conelly, A. Apparent Fibre Density: A novel measure for the analysis of diffusion-weighted magnetic resonance images. NeuroImage 2012, 59, 3976–3994. [Google Scholar] [CrossRef]
- Descoteaux, M. High Angular Resolution Diffusion MRI: From Local Estimation to Segmentation and Tractography. Ph.D. Thesis, Université Nice Sophia Antipolis, Nice, France, 2008. [Google Scholar]
- Tournier, D.J.; Calamante, F.; Gadian, D.G.; Connelly, A. Direct estimation of the fiber orientation density function from diffusion-weighted MRI data using spherical deconvolution. NeuroImage 2004, 23, 1176–1185. [Google Scholar] [CrossRef]
- Descoteaux, M.; Deriche, R.; Knösche, T.R.; Anwander, A. Deterministic and Probabilistic Tractography Based on Complex Fibre Orientation Distributions. IEEE Trans. Med. Imaging 2009, 28, 269–286. [Google Scholar] [CrossRef]
- Fiori, S.; Pannek, K.; Pasquariello, R.; Ware, R.S.; Cioni, G.; Rose, S.E.; Boyd, R.N.; Guzzetta, A. Corticopontocerebellar Connectivity Disruption in Congenital Hemiplegia. Neurorehabilit. Neural Repair 2015, 29, 858–866. [Google Scholar] [CrossRef]
- Tsao, H.; Pannek, K.; Boyd, R.N.; Rose, S.E. Changes in the integrity of thalamocortical connections are associated with sensorimotor deficits in children with congenital hemiplegia. Brain Struct. Funct. 2015, 220, 307–318. [Google Scholar] [CrossRef]
- Palesi, F.; De Rinaldis, A.; Castellazzi, G.; Calamante, F.; Muhlert, N.; Chard, D.; Tournier, J.D.; Magenes, G.; D’Angelo, E.; Gandini Wheeler-Kingshott, C.A. Contralateral cortico-ponto-cerebellar pathways reconstruction in humans in vivo: Implications for reciprocal cerebro-cerebellar structural connectivity in motor and non-motor areas. Sci. Rep. 2017, 7, 12481. [Google Scholar] [CrossRef]
- Palesi, F.; De Rinaldis, A.; Castellazzi, G.; Calamante, F.; Muhlert, N.; Chard, D.; Tournier, J.D.; Magenes, G.; D’Angelo, E.; Wheeler-Kingshott, C. Contralateral cerebello-thalamo-cortical pathways with prominent involvement of associative areas in humans in vivo. Brain Struct. Funct. 2015, 220, 3369–3384. [Google Scholar] [CrossRef]
- Zhang, H.; Schneider, T.; Wheeler-Kingshott, C.A.; Alexander, D.C. NODDI: Practical in vivo neurite orientation dispersion and density imaging of the human brain. NeuroImage 2012, 61, 1000–1016. [Google Scholar] [CrossRef]
- Pagnozzi, A.M.; Gal, Y.; Boyd, R.N.; Fiori, S.; Fripp, J.; Rose, S.; Dowson, N. The need for improved brain lesion segmentation techniques for children with cerebral palsy: A review. Int. Soc. Dev. Neurosci. 2015, 47, 229–246. [Google Scholar] [CrossRef] [PubMed]
- Northam, G.B.; Chong, W.K.; Wyatt, J.S.; Baldeweg, T. Total Brain White Matter Is a Major Determinant of IQ in Adolescents Born Preterm. Ann. Neurol. 2011, 69, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Craig, B.T.; Lang, E.K.; Hilderley, A.J.; Carlson, H.L. Structural connectivity of the sensorimotor network within the non-lesioned hemisphere of children with perinatal stroke. Sci. Rep. 2022, 12, 3866. [Google Scholar] [CrossRef] [PubMed]
- Krägeloh-Mann, I.; Horber, V. The role of magnetic resonance imaging in elucidating the pathogenesis of cerebral palsy. Dev. Med. Child. Neurol. 2007, 49, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Franki, I.; Mailleux, L.; Emsell, L.; Peedima, M.L.; Fehrenbach, A.; Feys, H.; Ortibus, E. The relationship between neuroimaging and motor outcome in children with cerebral palsy: A systematic review—Part A. Structural imaging. Res. Dev. Disabil. 2020, 100, 103606. [Google Scholar] [CrossRef]
- Tax, C.M.W.; Bastiani, M.; Veraart, J.; Garyfallidis, E.; Irfanoglu, M.O. What’s new and what’s next in diffusion MRI preprocessing. NeuroImage 2022, 249, 118830. [Google Scholar] [CrossRef]
- Theaud, G.; Houde, J.; Bor, A.; Morency, F.; Descoteaux, M. TractoFlow: A robust, efficient, and reproducible diffusion MRI pipeline leveraging Nextflow & Singularity. NeuroImage 2020, 218, 116889. [Google Scholar] [CrossRef]
- Soares, J.M.; Marques, P.; Alves, V.; Sousa, N. A hitchhiker’s guide to diffusion tensor imaging. Front. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef]
- Edde, M.; Theaud, G.; Dumont, M.; Theberge, A.; Valcourt-Caron, A.; Gilbert, G.; Houde, J.-C.; Maltais, L.; Rheault, F.; Spagnolo, F. High-frequency longitudinal white matter diffusion- and myelin-based MRI database Reliability and variability. Hum. Brain Mapp. 2023, 44, 3758–3780. [Google Scholar] [CrossRef]
- Garyfallidis, E.; Brett, M.; Amirbekian, B.; Rokem, A.; Van Der Walt, S. Dipy, a library for the analysis of diffusion MRI data. Front. Neuroinform. 2014, 8, 8. [Google Scholar] [CrossRef]
- Jenkinson, M.; Beckmann, C.F.; Behrens, T.E.J.; Woolrich, M.W.; Smith, S.M. FSL. NeuroImage 2011, 62, 2296–2311. [Google Scholar] [CrossRef] [PubMed]
- Tournier, J.D.; Smith, R.; Raffelt, D.; Tabbara, R.; Dhollander, T.; Pietsch, M.; Christiaens, D.; Jeurissen, B.; Yeh, C.-H.; Connelly, A. MRtrix3: A fast, flexible and open software framework for medical image processing and visualization. NeuroImage 2019, 202, 116137. [Google Scholar] [CrossRef] [PubMed]
- Avants, B.B.; Tustison, N.; Johnson, H. Advanced Normalization Tools (ANTS). Insight J. 2009, 2, 1–35. [Google Scholar]
- Kurtzer, G.M.; Sochat, V.; Bauer, M.W. Singularity: Scientific containers for mobility of compute. PLoS ONE 2017, 12, e0177459. [Google Scholar] [CrossRef] [PubMed]
- Di Tommaso, C.P.; Chatzou, M.; Floden, E.W.; Barja, P.P.; Palumbo, E.; Notredame, C. Nextflow enables reproducible computational workflows. Nat. Biotechnol. 2017, 35, 316–319. [Google Scholar] [CrossRef]
- Pines, A.R.; Cieslak, M.; Larsen, B.; Baum, G.L.; Cook, P.A.; Adebimpe, A.; Davila, D.G.; Alliott, M.A.; Jirsaraie, R.; Murtha, K.; et al. Leveraging multi-shell diffusion for studies of brain development in youth and young adulthood. Dev. Cogn. Neurosci. 2020, 43, 100788. [Google Scholar] [CrossRef]
- Raffelt, D.A.; Smith, R.E.; Ridgway, G.R.; Tournier, J.D.; Vaughan, D.N.; Rose, S.; Henderson, R.; Connelly, A. Connectivity-based fixel enhancement: Whole-brain statistical analysis of diffusion MRI measures in the presence of crossing fibres. NeuroImage 2015, 117, 40–55. [Google Scholar] [CrossRef]
- Dell’Acqua, F.; Simmons, A.; Williams, S.C.; Catani, M. Can Spherical Deconvolution Provide More Information Than Fiber Orientations? Hindrance Modulated Orientational Anisotropy, a True-Tract Specific Index to Characterize White Matter Diffusion. Hum. Brain Mapp. 2013, 34, 2464–2483. [Google Scholar] [CrossRef]
- Daducci, A.; Canales-Rodríguez, E.J.; Zhang, H.; Dyrby, T.B.; Alexander, D.C.; Thiran, J. Accelerated Microstructure Imaging via Convex Optimization (AMICO) from diffusion MRI data. NeuroImage 2015, 105, 32–44. [Google Scholar] [CrossRef]
- Takemura, H.; Caiafa, C.F.; Wandell, B.A.; Pestilli, F. Ensemble Tractography. PLoS Comput. Biol. 2016, 12, 1004692. [Google Scholar] [CrossRef]
- Theaud, G.; Houde, J.; Boré, A.; Rheault, F.; Morency, F.; Descoteaux, M. TractoFlow-ABS (Atlas-Based Segmentation). bioRxiv 2020. [Google Scholar] [CrossRef]
- Bach Cuadra, M.; Duay, V.; Thiran, J.P. Atlas-based segmentation. In Handbook of Biomedical Imaging: Methodologies and Clinical Research; Springer: Berlin/Heidelberg, Germany, 2015; pp. 221–244. [Google Scholar]
- Rheault, F. Analyse et Reconstruction de Faisceaux de la Matière Blanche. Ph.D. Thesis, Computer Science. Université de Sherbrooke, Sherbrooke, QC, Canada, 2020. [Google Scholar]
- Garyfallidis, E.; Cote, M.-A.; Rheault, F.; Sidhu, J.; Hau, J.; Petit, L.; Fortin, D.; Cunanne, S.; Descoteaux, M. Recognition of white matter bundles using local and global streamline-based registration and clustering. NeuroImage 2018, 170, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Mori, L.M.; Wakana, S.; Van Zijl, P.C.; Nagae-Poetscher, L.M. MRI atlas of human white matter. Am. J. Neuroradiol. 2006, 27, 1384. [Google Scholar]
- Rheault, M.; Houde, J.C.; Goyette, N.; Morency, F.; Descoteaux, M. MI-Brain, a software to handle tractograms and perform interactive virtual dissection. In Proceedings of the ISMRM Diffusion Study Group Workshop, Lisbon, Portugal, 11–16 September 2016. [Google Scholar]
- Lancaster, J.L.; Woldorff, M.G.; PArsons, L.M.; Liotti, M.; Freitas, C.S.; Rainey, L.; Kochunov, P.V.; Nickerson, D.; Mikiten, S.A.; Fox, P.T. Automated Talairach Atlas Labels For Functional Brain Mapping. Hum. Brain Mapp. 2000, 10, 120–131. [Google Scholar] [CrossRef]
- Lancaster, J.L.; Rainey, L.H.; Summerlin, J.L.; Freitas, C.S.; Fox, P.T.; Evans, A.C.; Toga, A.W.; Mazziotta, J.C. Automated Labeling of the Human Brain: A Preliminary Report on the Development and Evaluation of a Forward-Transform Method. Hum. Brain Mapp. 1997, 5, 238–242. [Google Scholar] [CrossRef]
- Al-Sharif, N.B.E.A.C.; St-Onge, E.; Vogel, J.W.; Theaud, G. Surface Integration for Connectome Analysis in Age Prediction; OHBM: New York, NY, USA, 2019. [Google Scholar]
- Garyfallidis, E.; Brett, M.; Correia, M.M.; Williams, G.B.; Nimmo-Smith, I. QuickBundles, a method for tractography simplification. Front. Neurosci. 2012, 6, 175. [Google Scholar] [CrossRef]
- Lidzba, K.; Staudt, M.; Wilke, M.; Krageloh-Mann, I. Visuospatial deficits in patients with early left-hemispheric lesions and functional reorganization of language: Consequence of lesion or reorganization? Neuropsychologia 2006, 44, 1088–1094. [Google Scholar] [CrossRef]
- Fischl, B. FreeSurfer. NeuroImage 2012, 62, 774–781. [Google Scholar] [CrossRef]
- Ingram, T.T.S. The Neurology of Cerebral Palsy. Arch. Dis. Child. 1966, 41, 337. [Google Scholar] [CrossRef]
- Rose, S.; Guzzetta, A.; Pannek, K.; Boyd, R. MRI Structural Connectivity, Disruption of Primary Sensorimotor Pathways, and Hand Function in Cerebral Palsy. Brain Connect. 2011, 1, 309–316. [Google Scholar] [CrossRef]
- Cousineau, M. Analyse de Populations Neurodégénératives et Assurance Qualité. Master’s Thesis, Université de Sherbrooke, Sherbrooke, QC, Canada, 2017. [Google Scholar]
- Riffert, T.W.; Schreiber, J.; Anwander, A.; Knösche, T.R. Beyond fractional anisotropy: Extraction of bundle-specific structural metrics from crossing fiber models. NeuroImage 2014, 100, 176–191. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Hori, M.; Aoki, S. NODDI in clinical research. J. Neurosci. Methods 2020, 346, 108908. [Google Scholar] [CrossRef] [PubMed]
- Yeatman, J.D.; Dougherty, R.F.; Myall, N.J.; Wandell, B.A.; Feldman, H.M. Tract Profiles of White Matter Properties: Automating Fiber-Tract Quantification. PLoS ONE 2012, 7, e49790. [Google Scholar] [CrossRef] [PubMed]
- Cousineau, M.; Jodoin, P.-M.; Garyfallidis, E.; Cote, M.-A.; Morency, F.C.; Rozanski, V.; Grand’Maison, M.; Bedell, B.J.; Descoteaux, M. A test-retest study on Parkinson’s PPMI dataset yields statistically significant white matter fascicles. NeuroImage Clin 2017, 16, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Pichet Binette, A.; Theaud, G.; Rheault, F.; Roy, M.; Collins, L.D.; Levin, J.; Mori, H.; Hong Lee, J.; Rhys Farlow, M.; Schofield, P.; et al. Bundle specific associations between white matter microstructure and Aβ and tau pathology in preclinical Alzheimer’s disease. eLife 2021, 10, e62929. [Google Scholar] [CrossRef] [PubMed]
- Reid, L.B.; Rose, S.E.; Boyd, R.N. Rehabilitation and neuroplasticity in children with unilateral cerebral palsy. Nat. Publ. Gr. 2015, 11, 390–400. [Google Scholar] [CrossRef]
- Korzeniewski, S.J.; Slaughter, J.; Lenski, M.; Haak, P. The complex aetiology of cerebral palsy. Nat. Rev. Neurol 2018, 14, 528–543. [Google Scholar] [CrossRef]
- Walker, L.; Chang, L.-C.; Nayak, A.; Irfanoglu, M.O.; Botteron, K.N.; McCracken, J.; McKristry, R.C.; Rivkin, M.J.; Wang, D.J.; Rumsey, J.; et al. The diffusion tensor imaging (DTI) component of the NIH MRI study of normal brain development (PedsDTI). NeuroImage 2016, 124, 1125–1130. [Google Scholar] [CrossRef]
- Pannek, K.; Boyd, R.N.; Fiori, S.; Guzzetta, A.; Rose, S.E. Assessment of the structural brain network reveals altered connectivity in children with unilateral cerebral palsy due to periventricular white matter lesions. NeuroImage Clin. 2014, 5, 84–92. [Google Scholar] [CrossRef]
- Timmers, I.; Roebroeck, A.; Bastiani, M.; Jansma, B.; Rubio-Gozalbo, E.; Zhang, H. Assessing Microstructural Substrates of White Matter Abnormalities: A Comparative Study Using DTI and NODDI. PLoS ONE 2016, 11, e0167884. [Google Scholar] [CrossRef]
- Johnson, D.; Ricciardi, A.; Brownlee, W.; Kanber, B.; Prados, F.; Collorone, S.; Kaden, E.; Toosy, A.; Alexander, D.C.; Gandini Wheeler-Kingshott, C.A.M.; et al. Comparison of Neurite Orientation Dispersion and Density Imaging and Two-Compartment Spherical Mean Technique Parameter Maps in Multiple Sclerosis. Front. Neurol. 2021, 12, 662855. [Google Scholar] [CrossRef] [PubMed]
- Tamnes, C.K.; Roalf, D.R.; Goddings, A.; Lebel, C. Diffusion MRI of white matter microstructure development in childhood and adolescence: Methods, challenges and progress. Dev. Cogn. Neurosci. 2018, 33, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; Deoni, S. The development of brain white matter microstructure. NeuroImage 2018, 182, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Schilling, K.G.; Rheault, F.; Petit, L.; Hansen, C.B.; Nath, V.; Yeh, F.-C.; Girard, G.; Barakovic, M.; Rafael-Patino, J.; Yu, T.; et al. Tractography dissection variability: What happens when 42 groups dissect 14 white matter bundles on the same dataset? NeuroImage 2021, 243, 118502. [Google Scholar] [CrossRef] [PubMed]
- Avants, B.B.; Tustison, N.J.; Song, G.; Cook, P.A.; Klein, A.; Gee, J.C. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage 2011, 54, 2033–2044. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Song, G.; Das, S.; van Strien, N.; Stone, J.R.; Gee, J.C. The ANTs cortical thickness processing pipeline. Med. Imaging 2013, 8672, 126–129. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age | Lesion Side | Etiology | MACS | |
|---|---|---|---|---|---|
| S1 | M | 13 y, 10 m | Right | Pre- or perinatal stroke (undefined) | I |
| S2 | M | 12 y, 5 m | Left | Perinatal stroke | III |
| S3 | F | 8 y, 9 m | Right | Prenatal stroke | II |
| S4 | M | 9 y, 3 m | Right | Unknown | I |
| S5 | F | 11 y, 6 m | Left | Periventricular leukomalacia | II |
| S6 | F | 11 y, 4 m | Right | Prenatal stroke | III |
| S7 | M | 13 y, 3 m | Right | Prenatal stroke | I |
| S8 | F | 11 y, 3 m | Right | Prenatal stroke | II |
| Left Hemisphere Volume | Right Hemisphere Volume | ||||||
|---|---|---|---|---|---|---|---|
| WM | GM | WM | GM | Brain Volume | Tissues Ratio | AI | |
| S1 | 214.6 | 297 | 199.8 | 280.8 | 1166.1 | 1.06 | 0.03 |
| S2 | 145.1 | 204.7 | 232.1 | 293.8 | 1075 | 0.67 | 0.2 |
| S3 | No segmentation | ||||||
| S4 | 202.1 | 274.2 | 202.4 | 275.5 | 1131.5 | 1 | 0 |
| S5 | 152.7 | 249.7 | 215.1 | 304.8 | 1088 | 0.77 | 0.13 |
| S6 | No segmentation | ||||||
| S7 | 237.5 | 307.2 | 219.8 | 282.3 | 1217 | 1.08 | 0.04 |
| S8 | 183.9 | 239 | 165 | 225.8 | 950.9 | 1.08 | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinie, O.; Karan, P.; Traverse, E.; Mercier, C.; Descoteaux, M.; Robert, M.T. The Challenge of Diffusion Magnetic Resonance Imaging in Cerebral Palsy: A Proposed Method to Identify White Matter Pathways. Brain Sci. 2023, 13, 1386. https://doi.org/10.3390/brainsci13101386
Martinie O, Karan P, Traverse E, Mercier C, Descoteaux M, Robert MT. The Challenge of Diffusion Magnetic Resonance Imaging in Cerebral Palsy: A Proposed Method to Identify White Matter Pathways. Brain Sciences. 2023; 13(10):1386. https://doi.org/10.3390/brainsci13101386
Chicago/Turabian StyleMartinie, Ophélie, Philippe Karan, Elodie Traverse, Catherine Mercier, Maxime Descoteaux, and Maxime T. Robert. 2023. "The Challenge of Diffusion Magnetic Resonance Imaging in Cerebral Palsy: A Proposed Method to Identify White Matter Pathways" Brain Sciences 13, no. 10: 1386. https://doi.org/10.3390/brainsci13101386