
The Efficacy of Pain Neuroscience Education on Active Rehabilitation Following Arthroscopic Rotator Cuff Repair: A CONSORT-Compliant Prospective Randomized Single-Blind Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
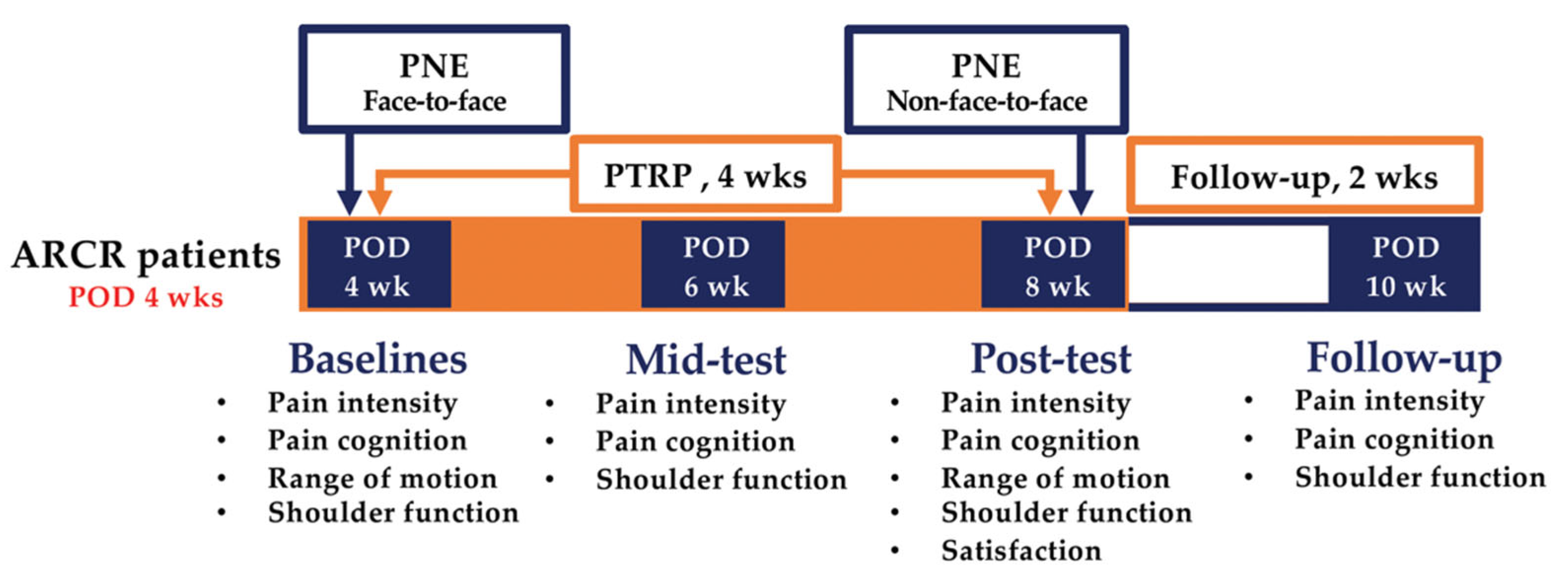
2.1. Study Design
2.2. Participants and Ethics
2.2.1. Inclusion Criteria
- Adults aged >18 years;
- Four weeks after ARCR;
- Willing to participate in the study.
2.2.2. Exclusion Criteria
- Older adults (age > 65 years);
- Unable to receive education remotely;
- Additional tendon augmentation in ARCR;
- History of surgery on the same shoulder before ARCR;
- Osteoarthritis findings in the shoulder joint;
- Mental health and cognitive problems to the extent that they cannot understand the guidelines for assessment and/or intervention.
2.2.3. Ethics
2.3. Sample Size
2.4. Randomization and Blinding
2.5. Intervention
2.5.1. Pain Neuroscience Education
- Definition and types of pain;
- Neurophysiology of pain;
- No reference to anatomical or pathoanatomical models;
- No discussion of emotional or behavioral aspects of pain;
- Nociception and nociceptive pathways;
- Mechanism of pain control;
- Peripheral sensitization;
- Pain alarm system;
- Central sensitization;
- Plasticity of the nervous system;
- Treatment cases in pain neuroscience education;
- Shoulder biomechanics;
- Arthroscopy rotator cuff repair details and procedure.
2.5.2. Physical Therapy Rehabilitation Protocol
2.6. Outcomes
2.6.1. Pain Intensity
2.6.2. Pain Cognition
2.6.3. Range of Motion
2.6.4. Shoulder Function
2.6.5. Treatment Satisfaction
2.7. Data Analysis
3. Results
3.1. General Characteristics of the Participants
3.2. Pain Intensity
3.3. Pain Cognition
3.4. Range of Motion
3.5. Shoulder Function
3.6. Treatment Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Littlewood, C.; May, S.; Walters, S. Epidemiology of Rotator Cuff Tendinopathy: A Systematic Review. Shoulder Elb. 2013, 5, 256–265. [Google Scholar] [CrossRef]
- Millett, P.J.; Wilcox, R.B.; O’holleran, J.D.; Warner, J.J.P. Rehabilitation of the Rotator Cuff: An Evaluation-Based Approach. JAAOS 2006, 14, 599–609. [Google Scholar] [CrossRef]
- Brislin, K.J.; Field, L.D.; Savoie, F.H., III. Complications after Arthroscopic Rotator Cuff Repair. Arthroscopy 2007, 23, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Tauro, J.C. Stiffness and Rotator Cuff Tears: Incidence, Arthroscopic Findings, and Treatment Results. Arthroscopy 2006, 22, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.S.; Parsley, B.; Burkhart, S.S.; Schoolfield, J.D. Reduction of Postoperative Stiffness after Arthroscopic Rotator Cuff Repair: Results of a Customized Physical Therapy Regimen Based on Risk Factors for Stiffness. Arthroscopy 2011, 27, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Houck, D.A.; Kraeutler, M.J.; Schuette, H.B.; Mccarty, E.C.; Bravman, J.T. Early Versus Delayed Motion after Rotator Cuff Repair: A Systematic Review of Overlapping Meta-Analyses. Am. J. Sports Med. 2017, 45, 2911–2915. [Google Scholar] [CrossRef]
- Huberty, D.P.; Schoolfield, J.D.; Brady, P.C.; Vadala, A.P.; Arrigoni, P.; Burkhart, S.S. Incidence and Treatment of Postoperative Stiffness Following Arthroscopic Rotator Cuff Repair. Arthroscopy 2009, 25, 880–890. [Google Scholar] [CrossRef]
- Parsons, B.O.; Gruson, K.I.; Chen, D.D.; Harrison, A.K.; Gladstone, J.; Flatow, E.L. Does Slower Rehabilitation after Arthroscopic Rotator Cuff Repair Lead to Long-Term Stiffness? J. Shoulder Elb. Surg. 2010, 19, 1034–1039. [Google Scholar] [CrossRef]
- Rubin, B.D.; Kibler, W.B. Fundamental Principles of Shoulder Rehabilitation: Conservative to Postoperative Management. Arthroscopy 2002, 18, 29–39. [Google Scholar] [CrossRef]
- Ellenbecker, T.S.; Cools, A. Rehabilitation of Shoulder Impingement Syndrome and Rotator Cuff Injuries: An Evidence-Based Review. Br. J. Sports Med. 2010, 44, 319–327. [Google Scholar] [CrossRef]
- Kim, H.; Lee, S. Effects of Pain Neuroscience Education on Kinesiophobia in Patients with Chronic Pain: A Systematic Review and Meta-Analysis. Phys. Ther. Rehabil. Sci. 2020, 9, 309–317. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Seco, J.; Royuela, A.; Peña, A.; Muriel, A. Spanish Back Pain Research Network. The Correlation between Pain, Catastrophizing, and Disability in Subacute and Chronic Low Back Pain: A Study in the Routine Clinical Practice of the Spanish National Health Service. Spine 2011, 36, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-Avoidance and Its Consequences in Chronic Musculoskeletal Pain: A State of the Art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef]
- Louw, A.; Diener, I.; Landers, M.R.; Puentedura, E.J. Preoperative Pain Neuroscience Education for Lumbar Radiculopathy: A Multicenter Randomized Controlled Trial with 1-Year Follow-Up. Spine 2014, 39, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Diener, I.; Landers, M.R.; Zimney, K.; Puentedura, E.J. Three-Year Follow-up of a Randomized Controlled Trial Comparing Preoperative Neuroscience Education for Patients Undergoing Surgery for Lumbar Radiculopathy. J. Spine Surg. 2016, 2, 289. [Google Scholar] [CrossRef]
- Louw, A.; Zimney, K.; Reed, J.; Landers, M.; Puentedura, E.J. Immediate Preoperative Outcomes of Pain Neuroscience Education for Patients Undergoing Total Knee Arthroplasty: A Case Series. Physiother. Theory Pract. 2019, 35, 543–553. [Google Scholar] [CrossRef]
- Kane, L.T.; Thakar, O.; Jamgochian, G.; Lazarus, M.D.; Abboud, J.A.; Namdari, S.; Horneff, J.G. The Role of Telehealth as a Platform for Postoperative Visits Following Rotator Cuff Repair: A Prospective, Randomized Controlled Trial. J. Shoulder Elb. Surg. 2020, 29, 775–783. [Google Scholar] [CrossRef]
- Sheps, D.M.; Silveira, A.; Beaupre, L.; Styles-Tripp, F.; Balyk, R.; Lalani, A.; Glasgow, R.; Bergman, J.; Bouliane, M. Early Active Motion Versus Sling Immobilization after Arthroscopic Rotator Cuff Repair: A Randomized Controlled Trial. Arthroscopy 2019, 35, 749–760.e2. [Google Scholar] [CrossRef]
- Mazzocca, A.D.; Arciero, R.A.; Shea, K.P.; Apostolakos, J.M.; Solovyova, O.; Gomlinski, G.; Wojcik, K.E.; Tafuto, V.; Stock, H.; Cote, M.P. The Effect of Early Range of Motion on Quality of Life, Clinical Outcome, and Repair Integrity after Arthroscopic Rotator Cuff Repair. Arthroscopy 2017, 33, 1138–1148. [Google Scholar] [CrossRef]
- Louw, A.; Puentedura, E.; Schmidt, S.; Zimney, K. Pain Neuroscience Education: Teaching People about Pain; Orthopedic Physical Therapy Products: Minneapolis, MN, USA, 2018. [Google Scholar]
- Butler, D.S.; Moseley, G.L. Explain Pain 2nd Edn; Noigroup Publications: Adelaide, Australia, 2013. [Google Scholar]
- Rondon-Ramos, A.; Martinez-Calderon, J.; Diaz-Cerrillo, J.; Rivas-Ruiz, F.; Ariza-Hurtado, G.; Clavero-Cano, S.; Luque-Suarez, A. Pain Neuroscience Education Plus Usual Care Is More Effective Than Usual Care Alone to Improve Self-Efficacy Beliefs in People with Chronic Musculoskeletal Pain: A Non-Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2195. [Google Scholar] [CrossRef]
- Kim, H.-J.; Lee, S. Physical Therapy Following Arthroscopic Rotator Cuff Repair with Graft Augmentation: A Case Report with Magnetic Resonance Imaging. Phys. Ther. Rehabil. Sci. 2021, 10, 463–469. [Google Scholar] [CrossRef]
- Kim, H.-J.; Choi, W.; Jung, J.-H.; Park, S.-G.; Joo, Y.-L.; Lee, S. Effect of Extracorporeal Shock Wave Therapy after Arthroscopic Rotator Cuff Repair. 2021. Available online: https://ClinicalTrials.gov/show/NCT04848103 (accessed on 13 April 2022).
- Kim, H.; Lee, S. Postoperative Rehabilitation Protocol Following Arthroscopic Rotator Cuff Repair: A Prospective Single-Arm Pragmatic Interventional Study. Medicina 2022, 58, 729. [Google Scholar] [CrossRef]
- Michener, L.A.; Snyder, A.R.; Leggin, B.G. Responsiveness of the Numeric Pain Rating Scale in Patients with Shoulder Pain and the Effect of Surgical Status. J. Sport Rehabil. 2011, 20, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Mintken, P.E.; Glynn, P.; Cleland, J.A. Psychometric Properties of the Shortened Disabilities of the Arm, Shoulder, and Hand Questionnaire (Quickdash) and Numeric Pain Rating Scale in Patients with Shoulder Pain. J. Shoulder Elb. Surg. 2009, 18, 920–926. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524. [Google Scholar] [CrossRef]
- Cho, S.; Kim, H.-Y.; Lee, J.-H. Validation of the Korean Version of the Pain Catastrophizing Scale in Patients with Chronic Non-Cancer Pain. Qual. Life Res. 2013, 22, 1767–1772. [Google Scholar] [CrossRef]
- García-Campayo, J.; Rodero, B.; Del Hoyo, Y.L.; Luciano, J.V.; Alda, M.; Gili, M. Validation of a Spanish Language Version of the Pain Self-Perception Scale in Patients with Fibromyalgia. BMC Musculoskelet. Disord. 2010, 11, 255. [Google Scholar] [CrossRef]
- George, S.Z.; Valencia, C.; Beneciuk, J.M. A Psychometric Investigation of Fear-Avoidance Model Measures in Patients with Chronic Low Back Pain. J. Orthop. Sports 2010, 40, 197–205. [Google Scholar] [CrossRef]
- Goubert, L.; Crombez, G.; Van Damme, S.; Vlaeyen, J.W.; Bijttebier, P.; Roelofs, J. Confirmatory Factor Analysis of the Tampa Scale for Kinesiophobia: Invariant Two-Factor Model across Low Back Pain Patients and Fibromyalgia Patients. Clin. J. Pain 2004, 20, 103–110. [Google Scholar] [CrossRef]
- Roelofs, J.; Peters, M.L.; McCracken, L.; Vlaeyen, J. The Pain Vigilance and Awareness Questionnaire (Pvaq): Further Psychometric Evaluation in Fibromyalgia and Other Chronic Pain Syndromes. Pain 2003, 101, 299–306. [Google Scholar] [CrossRef]
- Gómez-Pérez, L.; López-Martínez, A.E.; Ruiz-Párraga, G.T. Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia (Tsk). J. Pain 2011, 12, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, N.; Matsudaira, K.; Sawada, T.; Oka, H. Psychometric Properties of the Japanese Version of the Tampa Scale for Kinesiophobia (Tsk-J) in Patients with Whiplash Neck Injury Pain and/or Low Back Pain. J. Orthop. Sci. 2015, 20, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Norkin, C.C.; White, D.J. Measurement of Joint Motion: A Guide to Goniometry; FA Davis: Philadelphia, PA, USA, 2016. [Google Scholar]
- Mullaney, M.J.; McHugh, M.P.; Johnson, C.P.; Tyler, T.F. Reliability of Shoulder Range of Motion Comparing a Goniometer to a Digital Level. Physiother. Theory Pract. 2010, 26, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Homsi, C.; Bordalo-Rodrigues, M.; Da Silva, J.J.; Stump, X.M. Ultrasound in Adhesive Capsulitis of the Shoulder: Is Assessment of the Coracohumeral Ligament a Valuable Diagnostic Tool? Skelet. Radiol. 2006, 35, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Katz, J.N.; Fossel, A.H.; Wright, J.G.; Tarasuk, V.; Bombardier, C. Measuring the Whole or the Parts? Validity, Reliability, and Responsiveness of the Disabilities of the Arm, Shoulder and Hand Outcome Measure in Different Regions of the Upper Extremity. J. Hand Ther. 2001, 14, 128–142. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Lim, J.-Y.; Oh, J.H.; Ko, Y.-M. Cross-Cultural Adaptation and Clinical Evaluation of a Korean Version of the Disabilities of Arm, Shoulder, and Hand Outcome Questionnaire (K-Dash). J. Shoulder Elb. Surg. 2008, 17, 570–574. [Google Scholar] [CrossRef]
- Schmitt, J.S.; Di Fabio, R.P. Reliable Change and Minimum Important Difference (Mid) Proportions Facilitated Group Responsiveness Comparisons Using Individual Threshold Criteria. J. Clin. Epidemiol. 2004, 57, 1008–1018. [Google Scholar] [CrossRef]
- Paul, A.; Lewis, M.; Shadforth, M.F.; Croft, P.R.; Van Der Windt, D.A.W.M.; Hay, E.M. A Comparison of Four Shoulder-Specific Questionnaires in Primary Care. Ann. Rheum. Dis. 2004, 63, 1293–1299. [Google Scholar] [CrossRef]
- Roach, K.E.; Budiman-Mak, E.; Songsiridej, N.; Lertratanakul, Y. Development of a Shoulder Pain and Disability Index. Arthritis Rheumatol. 1991, 4, 143–149. [Google Scholar] [CrossRef]
- Choi, Y.; Park, J.W.; Noh, S.; Kim, M.S.; Park, Y.H.; Sung, D.H. Reliability, Validity, and Responsiveness of the Korean Version of the Shoulder Disability Questionnaire and Shoulder Rating Questionnaire. Ann. Rehabil. Med. 2015, 39, 705. [Google Scholar] [CrossRef]
- Tveitå, E.K.; Sandvik, L.; Ekeberg, O.M.; Juel, N.G.; Bautz-Holter, E. Factor Structure of the Shoulder Pain and Disability Index in Patients with Adhesive Capsulitis. BMC Musculoskelet. Disord. 2008, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.W., Jr.; Holleman, D.R., Jr.; Simel, D. Measuring Shoulder Function with the Shoulder Pain and Disability Index. J. Rheumatol. 1995, 22, 727–732. [Google Scholar] [PubMed]
- Hsu, J.E.; Russ, S.M.; Somerson, J.S.; Tang, A.; Warme, W.J.; Matsen, F.A., III. Is the Simple Shoulder Test a Valid Outcome Instrument for Shoulder Arthroplasty? J. Shoulder Elbow Surg. 2017, 26, 1693–1700. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Deloach, J.; Green, A.; Porucznik, C.A.; Powell, A.P. Minimal Clinically Important Differences in Ases and Simple Shoulder Test Scores after Nonoperative Treatment of Rotator Cuff Disease. JBJS 2010, 92, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Bradley, M.P.; Tocci, S.; Rey, J.; Henn, R.F.; Green, A. Factors Influencing Patient Satisfaction after Rotator Cuff Repair. J. Shoulder Elb. Surg. 2007, 16, 752–758. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- Correia, F.D.; Molinos, M.; Luís, S.; Carvalho, D.; Carvalho, C.; Costa, P.; Seabra, R.; Francisco, G.; Bento, V.; Lains, J. Digitally Assisted Versus Conventional Home-Based Rehabilitation after Arthroscopic Rotator Cuff Repair: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2021, 101, 237. [Google Scholar] [CrossRef]
- Ha, J.-W.; Kim, H.; Kim, S.H. Effects of Steroid Injection During Rehabilitation after Arthroscopic Rotator Cuff Repair. Clin. Shoulder Elb. 2021, 24, 166. [Google Scholar] [CrossRef]
- Conti, M.; Garofalo, R.; Rose, G.D.; Massazza, G.; Vinci, E.; Randelli, M.; Castagna, A. Post-Operative Rehabilitation after Surgical Repair of the Rotator Cuff. Musculoskelet. Surg. 2009, 93, 55–63. [Google Scholar] [CrossRef]
- Fletcher, C.; Bradnam, L.; Barr, C. The Relationship between Knowledge of Pain Neurophysiology and Fear Avoidance in People with Chronic Pain: A Point in Time, Observational Study. Physiother. Theory Pract. 2016, 32, 271–276. [Google Scholar] [CrossRef]
- Smith, P.J.A.; Russo, P.L.; Santayana, P.N. Fear Avoidance Predicts Persistent Pain in Young Adults with Low Back Pain: A Prospective Study. J. Orthop. Sports Phys. Ther. 2021, 51, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Rakhshaee, Z. Effect of Three Yoga Poses (Cobra, Cat and Fish Poses) in Women with Primary Dysmenorrhea: A Randomized Clinical Trial. J. Pediatr. Adolesc. Gynecol. 2011, 24, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Ben-Menachem, M. Treatment of Dysmenorrhea: A Relaxation Therapy Program. Int. J. Gynaecol. Obstet. 1980, 17, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Norton, P.J.; Asmundson, G.J. Amending the Fear-Avoidance Model of Chronci Pain: What Is the Role of Physiological Arousal? Behav. Ther. 2003, 34, 17–30. [Google Scholar] [CrossRef]
- Ihara, N.; Wakaizumi, K.; Nishimura, D.; Kato, J.; Yamada, T.; Suzuki, T.; Hashiguchi, S.; Terasawa, Y.; Kosugi, S.; Morisaki, H. Aberrant Resting-State Functional Connectivity of the Dorsolateral Prefrontal Cortex to the Anterior Insula and Its Association with Fear Avoidance Belief in Chronic Neck Pain Patients. PLoS ONE 2019, 14, e0221023. [Google Scholar] [CrossRef]
- Apkarian, A.V.; Bushnell, M.C.; Treede, R.-D.; Zubieta, J.-K. Human Brain Mechanisms of Pain Perception and Regulation in Health and Disease. Eur. J. Pain 2005, 9, 463–484. [Google Scholar] [CrossRef]
- Gogolla, N. The Insular Cortex. Curr. Biol. 2017, 27, R580–R586. [Google Scholar] [CrossRef]
- Schreckenberger, M.; Siessmeier, T.; Viertmann, A.; Landvogt, C.; Buchholz, H.-G.; Rolke, R.; Treede, R.-D.; Bartenstein, P.; Birklein, F. The Unpleasantness of Tonic Pain Is Encoded by the Insular Cortex. Neurology 2005, 64, 1175–1183. [Google Scholar] [CrossRef]
- Starr, C.J.; Sawaki, L.; Wittenberg, G.; Burdette, J.H.; Oshiro, Y.; Quevedo, A.S.; Coghill, R.C. Roles of the Insular Cortex in the Modulation of Pain: Insights from Brain Lesions. J. Neurosci. 2009, 29, 2684–2694. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types | Component | Dosage |
|---|---|---|
| Physical agents | Superficial heat therapy | 15 min per session, 5 sessions per week |
| Microwave therapy | 5 min per session, 5 sessions per week | |
| TENS | 15 min per session, 5 sessions per week | |
| Manual therapy | Soft tissue mobilization | 20 min per session, 5 sessions per week |
| Joint mobilization | 10 min per session, 5 sessions per week | |
| Exercises | ROM exercise | 30 min per session, 5 sessions per week |
| Therapeutic exercise | 20 min per session, 5 sessions per week |
| Variables | PNE (n = 17) | PTRP (n = 17) | X2/t |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| General characteristics | |||
| Sex (male, %) | 7 (41.18) | 6 (35.29) | 0.125 |
| Affected side (Left, %) | 6 (35.29) | 7 (41.18) | 0.125 |
| Age (years) | 51.12 ± 5.64 | 51.82 ± 4.85 | −0.391 |
| Height (cm) | 163.59 ± 7.53 | 162.18 ± 6.07 | 0.601 |
| Weight (kg) | 63.88 ± 8.87 | 64.82 ± 9.38 | −0.301 |
| BMI (kg/m2) | 23.79 ± 2.10 | 24.55 ± 2.42 | −0.971 |
| Arthroscopic rotator cuff repair | |||
| Supraspinatus (n) | 7 | 9 | 0.472 |
| Subscapularis (n) | 12 | 10 | 0.515 |
| Capsular release (n) | 7 | 13 | 4.371 * |
| Biceps tenodesis (n) | 16 | 11 | 4.497 * |
| SAD (n) | 17 | 17 | - |
| Variables | Baselines | Mid-Test | Post-Test | Follow-Up | Time (a) F (p) | Time × Group (a) | ||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | F (p) | Effect Size (b) | |||
| Pain intensity | ||||||||
| Usual pain | PNE | 4.12 ± 1.76 | 3.41 ± 2.00 | 3.82 ± 2.07 | 3.06 ± 1.85 | 3.182 (0.027) | 2.455 (0.068) | 0.071 |
| PTRP | 3.41 ± 1.46 | 3.88 ± 1.80 | 4.12 ± 1.69 | 3.41 ± 1.80 | ||||
| Worst pain | PNE | 5.65 ± 2.64 | 4.76 ± 2.46 | 5.41 ± 2.37 | 4.65 ± 2.09 | 2.399 (0.073) | 1.672 (0.178) | 0.050 |
| PTRP | 4.82 ± 2.24 | 5.29 ± 1.45 | 5.35 ± 2.12 | 4.59 ± 1.77 | ||||
| Pain cognition | ||||||||
| K-PCS | PNE | 19.24 ± 13.37 | 18.76 ± 13.11 | 20.71 ± 13.78 | 17.71 ± 12.28 | 1.611 (0.211) | 1.267 (0.286) | 0.038 |
| PTRP | 17.06 ± 11.36 | 21.06 ± 10.19 | 22.06 ± 10.35 | 21.00 ± 10.34 | ||||
| TSK-avoidance | PNE | 13.59 ± 3.24 | 12.24 ± 2.73 | 10.41 ± 3.26 ** | 10.65 ± 3.00 * | 4.469 (0.006) | 5.650 (0.001) | 0.150 |
| PTRP | 13.29 ± 3.53 | 13.24 ± 3.60 | 13.82 ± 2.74 | 13.00 ± 3.34 | ||||
| TSK-harm | PNE | 9.94 ± 2.14 | 9.71 ± 2.37 | 10.18 ± 2.40 | 10.06 ± 1.89 | 0.931 (0.417) | 0.097 (0.942) | 0.003 |
| PTRP | 9.94 ± 3.07 | 9.59 ± 2.81 | 10.35 ± 2.18 | 10.35 ± 2.96 | ||||
| TSK-total | PNE | 23.53 ± 5.16 | 21.94 ± 4.90 | 20.59 ± 5.53 | 20.71 ± 4.65 | 0.982 (0.405) | 2.191 (0.121) | 0.064 |
| PTRP | 23.24 ± 6.34 | 22.82 ± 6.06 | 24.18 ± 4.65 | 23.35 ± 6.13 | ||||
| Shoulder function | ||||||||
| K-DASH | PNE | 73.92 ± 14.75 | 59.02 ± 14.40 | 58.14 ± 16.63 | 52.35 ± 15.29 | 22.342 (0.000) | 2.190 (0.118) | 0.064 |
| PTRP | 71.18 ± 20.36 | 64.17 ± 16.30 | 64.41 ± 17.57 | 58.97 ± 16.00 | ||||
| K-SPADI -pain | PNE | 61.18 ± 26.95 | 51.06 ± 24.65 | 50.82 ± 24.21 | 40.24 ± 22.54 | 15.245 (0.000) | 1.370 (0.257) | 0.041 |
| PTRP | 56.94 ± 26.26 | 53.29 ± 21.77 | 50.47 ± 23.92 | 45.41 ± 24.42 | ||||
| K-SPADI -disability | PNE | 54.41 ± 28.11 | 41.40 ± 22.52 | 39.71 ± 24.03 | 31.91 ± 21.31 | 16.431 (0.000) | 0.080 (0.971) | 0.002 |
| PTRP | 54.49 ± 27.68 | 43.97 ± 23.35 | 40.88 ± 24.89 | 34.56 ± 23.41 | ||||
| K-SPADI -total | PNE | 57.01 ± 27.41 | 45.11 ± 22.79 | 43.98 ± 23.58 | 35.11 ± 21.42 | 17.917 (0.000) | 0.366 (0.778) | 0.011 |
| PTRP | 55.43 ± 26.83 | 47.56 ± 20.80 | 44.57 ± 23.58 | 38.73 ± 23.40 | ||||
| SST | PNE | 8.59 ± 2.92 | 6.06 ± 1.82 | 6.71 ± 3.46 | 4.82 ± 2.43 | 16.056 (0.000) | 1.469 (0.236) | 0.044 |
| PTRP | 8.18 ± 1.70 | 7.12 ± 1.69 | 6.82 ± 3.34 | 5.94 ± 3.03 | ||||
| Variables | Baselines | Post-Test | t (95% CI) (a) | Effect Size (b) | |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ||||
| Range of motion | |||||
| Flexion | PNE | 147.94 ± 29.00 | 177.94 ± 7.30 | −4.604 *** (−43.814–−16.186) | 1.419 |
| PTRP | 147.76 ± 32.94 | 172.06 ± 17.77 | −2.953 ** (−41.737–−6.851) | 0.918 | |
| t (95% CI) (c) | −0.017 (−21.856–21.503) | −1.262 (−15.566–3.609) | |||
| Scaption flexion | PNE | 145.29 ± 30.69 | 177.65 ± 7.31 | −4.715 *** (−46.899–−17.807) | 1.451 |
| PTRP | 135.18 ± 34.78 | 169.41 ± 20.53 | −3.800 ** (−53.335–−15.136) | 1.199 | |
| t (95% CI) | −0.899 (−33.035–12.800) | −1.558 (−19.262–2.791) | |||
| Abduction | PNE | 132.35 ± 35.58 | 169.41 ± 25.85 | −4.039 ** (−56.511–−17.606) | 1.192 |
| PTRP | 125.88 ± 40.44 | 154.71 ± 37.27 | −2.397 * (−54.314–−3.333) | 0.741 | |
| t (95% CI) | −0.495 (−33.080–20.139) | −1.337 (−37.222–7.811) | |||
| Horizontal adduction | PNE | 107.94 ± 25.38 | 121.18 ± 13.17 | −2.228 * (−25.827–−0.643) | 0.655 |
| PTRP | 93.82 ± 34.26 | 117.65 ± 20.47 | −2.496 * (−44.056–−3.591) | 0.844 | |
| t (95% CI) | −1.365 (−35.179–6.944) | −0.598 (−15.556–8.497) | |||
| External rotation | PNE | 64.12 ± 14.50 | 80.88 ± 9.05 | −5.647 *** (−23.058–−10.471) | 1.387 |
| PTRP | 66.76 ± 16.10 | 77.35 ± 12.64 | −3.139 ** (−17.738–−3.438) | 0.732 | |
| t (95% CI) | 0.504 (−8.055–13.349) | −0.936 (−11.210–4.152) | |||
| Internal rotation | PNE | 45.29 ± 16.53 | 53.82 ± 18.50 | −2.792 * (−15.005–−2.054) | 0.486 |
| PTRP | 41.18 ± 13.52 | 50.00 ± 16.30 | −2.839 * (−15.411–−2.236) | 0.589 | |
| t (95% CI) | −0.795 (−14.670–6.435) | −0.639 (−16.004–8.357) | |||
| Treatment satisfaction | |||||
| VAS-satisfaction | PNE | - | 8.34 ± 1.33 | - | - |
| PTRP | - | 7.87 ± 1.63 | - | - | |
| t (95% CI) | - | −0.922 (−1.511–0.569) | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Lee, S. The Efficacy of Pain Neuroscience Education on Active Rehabilitation Following Arthroscopic Rotator Cuff Repair: A CONSORT-Compliant Prospective Randomized Single-Blind Controlled Trial. Brain Sci. 2022, 12, 764. https://doi.org/10.3390/brainsci12060764
Kim H, Lee S. The Efficacy of Pain Neuroscience Education on Active Rehabilitation Following Arthroscopic Rotator Cuff Repair: A CONSORT-Compliant Prospective Randomized Single-Blind Controlled Trial. Brain Sciences. 2022; 12(6):764. https://doi.org/10.3390/brainsci12060764
Chicago/Turabian StyleKim, Hyunjoong, and Seungwon Lee. 2022. "The Efficacy of Pain Neuroscience Education on Active Rehabilitation Following Arthroscopic Rotator Cuff Repair: A CONSORT-Compliant Prospective Randomized Single-Blind Controlled Trial" Brain Sciences 12, no. 6: 764. https://doi.org/10.3390/brainsci12060764