
Extradural Motor Cortex Stimulation in Parkinson’s Disease: Long-Term Clinical Outcome

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
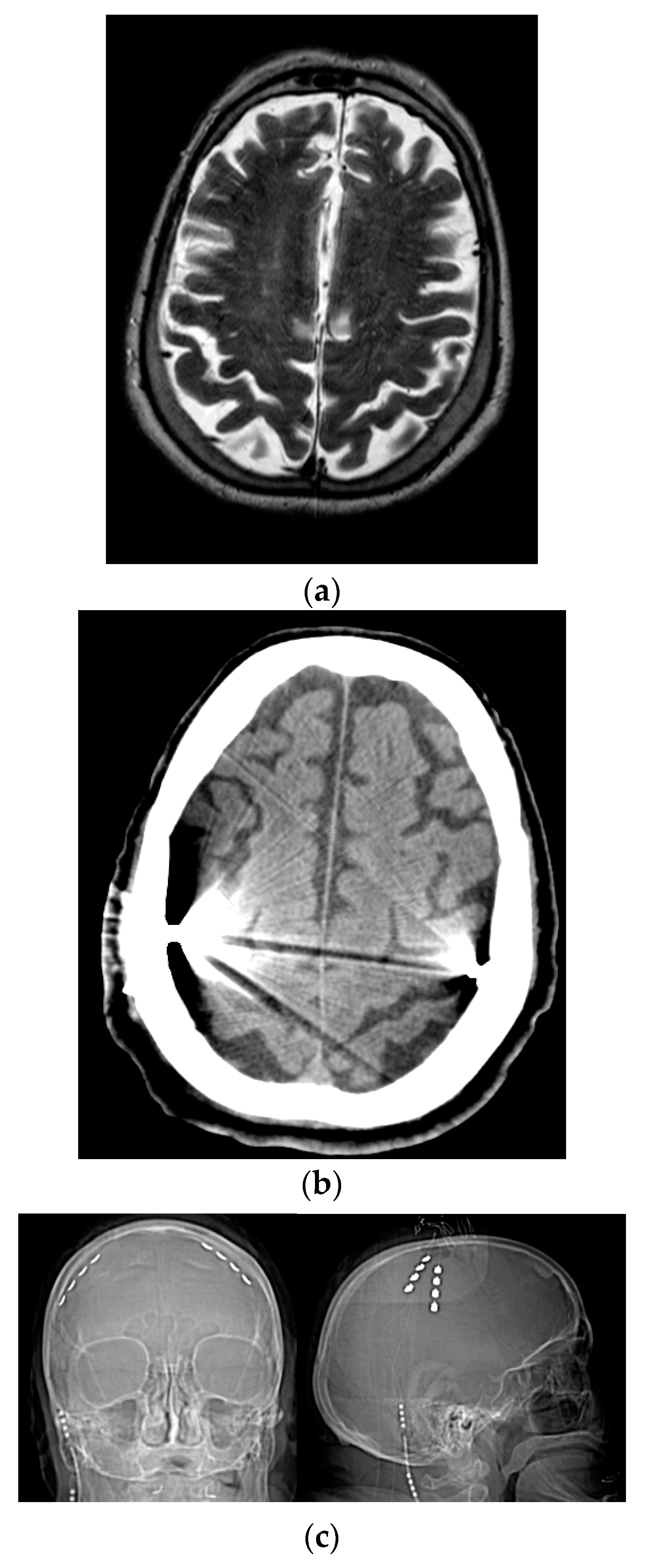
2.1. Surgical Technique
2.2. Parameter and Medication Adjustments
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
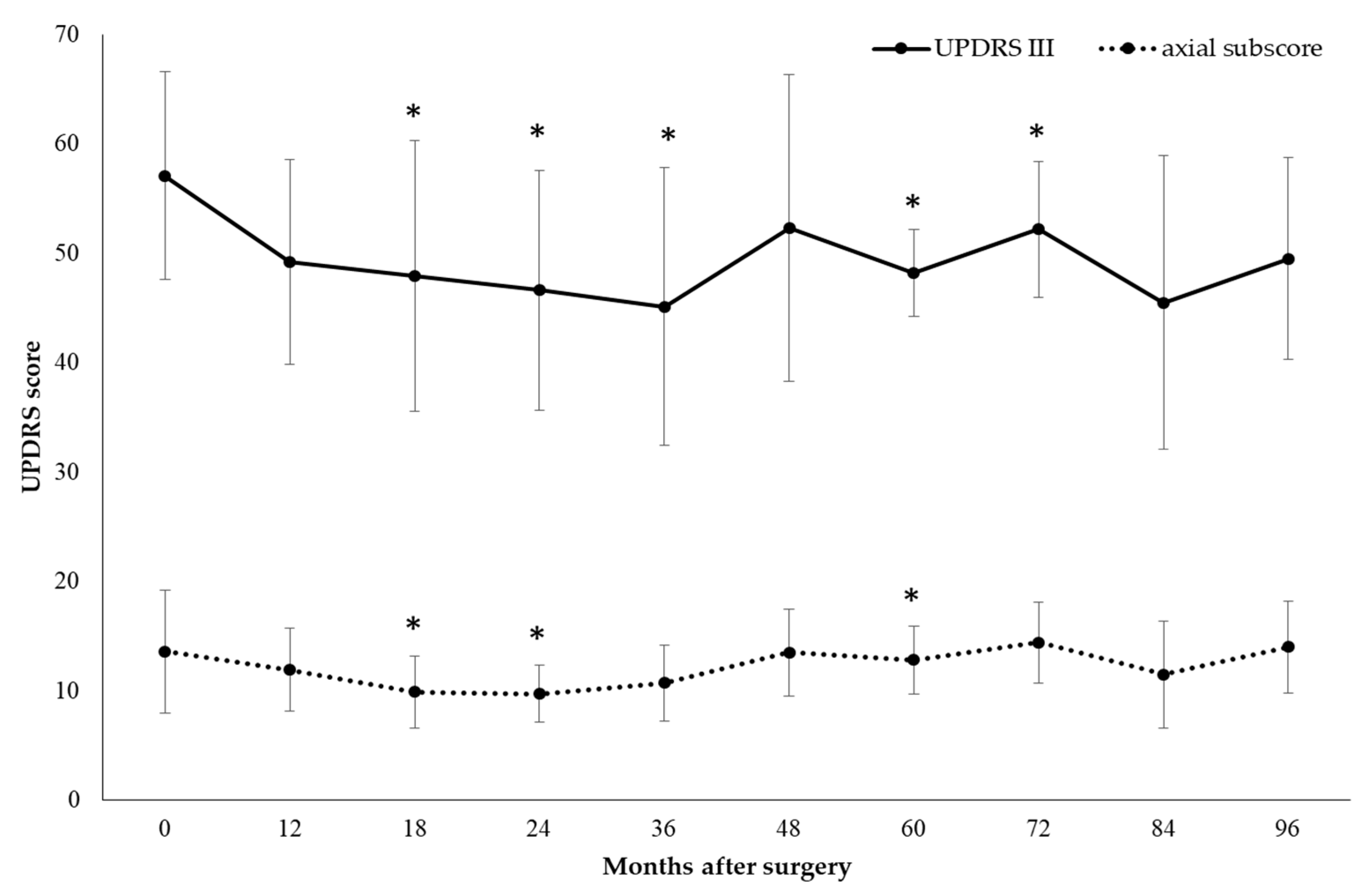
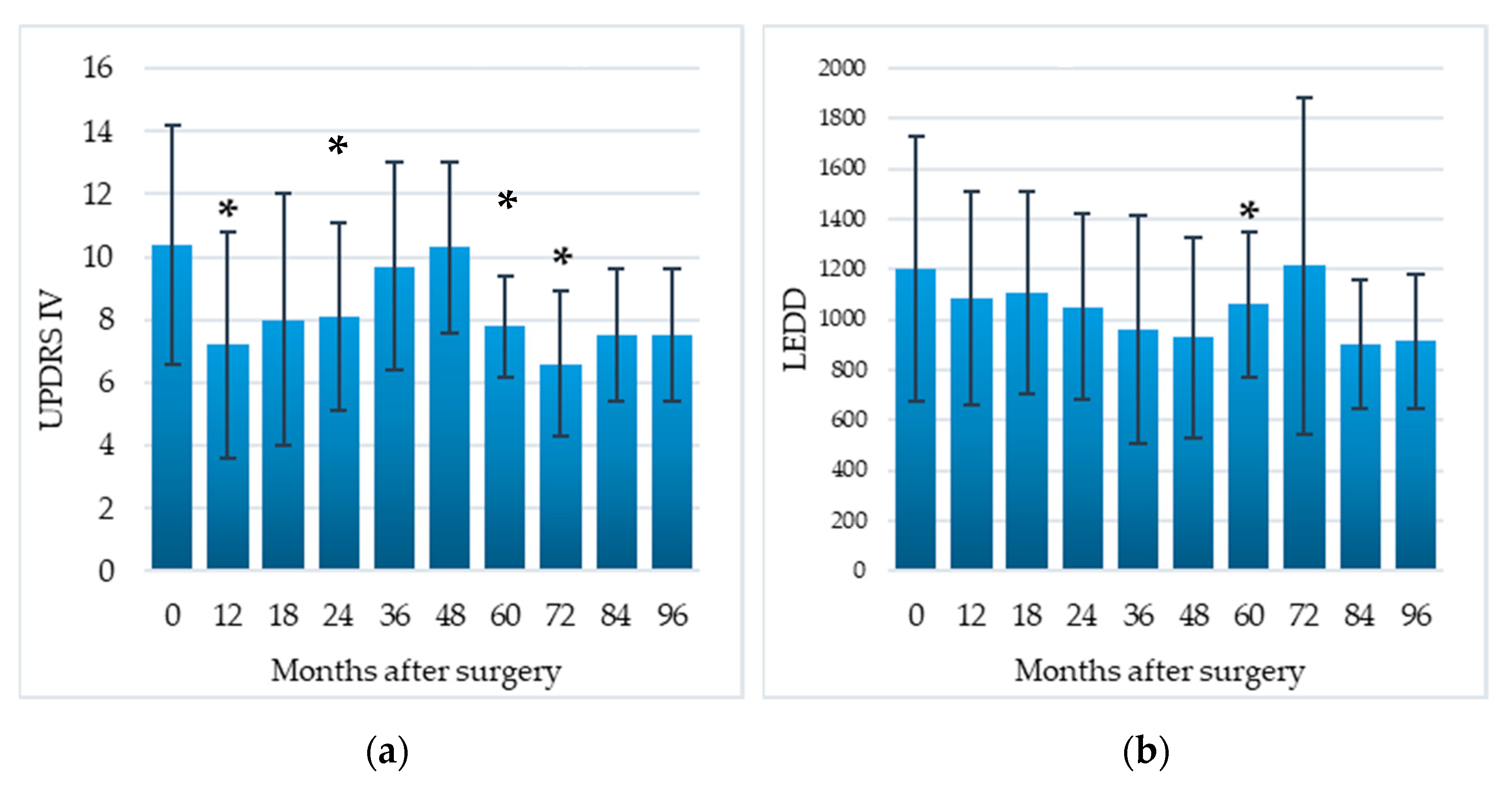
3.1. Motor Efficacy
3.2. Disease Severity
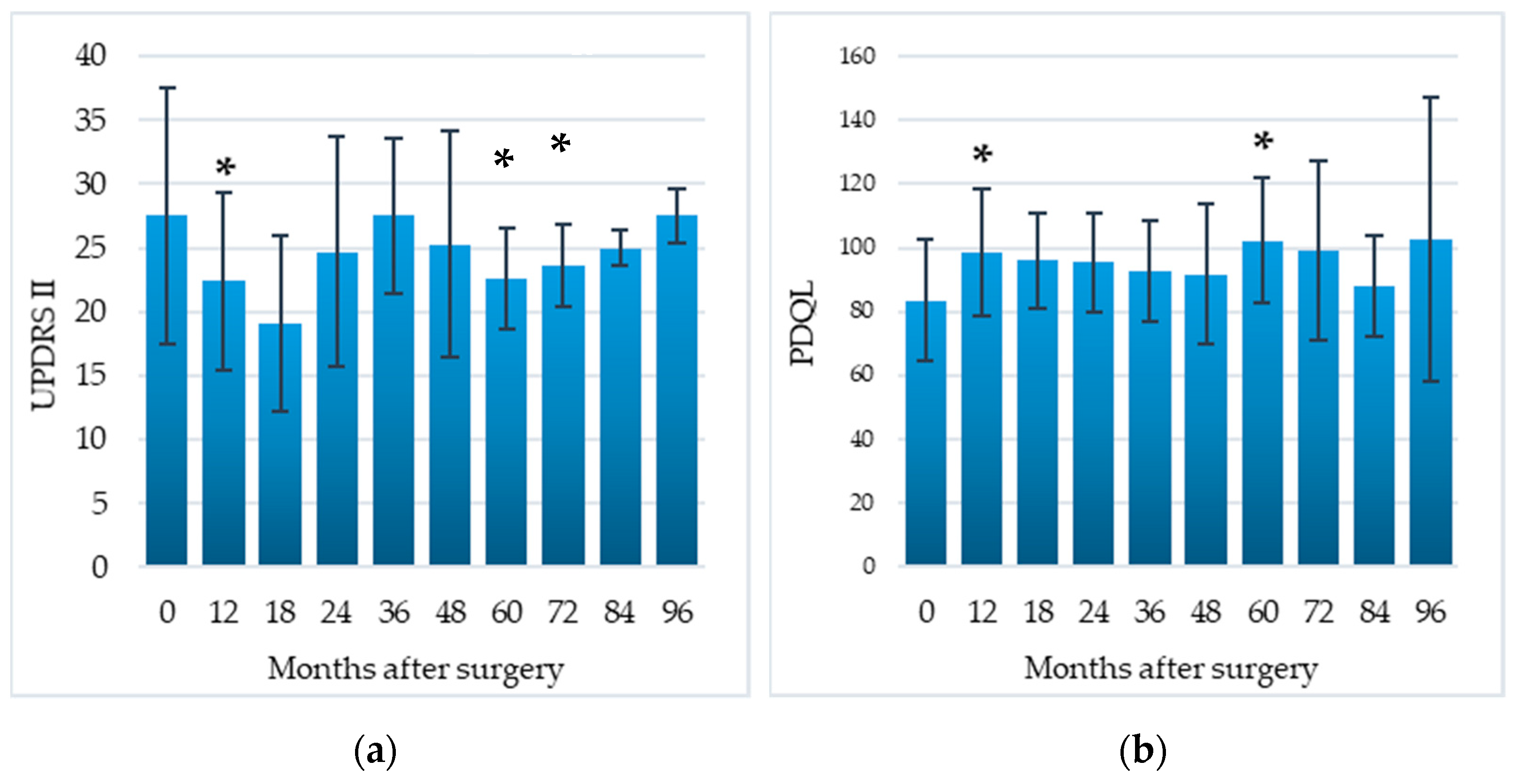
3.3. DLA and QoL
3.4. Cognitive and Behvioral Outcome
3.5. Safety
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canavero, S. Invasive Cortical Stimulation for Parkinson’s Disease (PD): Why, where and how. In Textbook of Therapeutic Cortical Stimulation; Nova Science: New York, NY, USA, 2009; pp. 217–227. [Google Scholar]
- Pagni, C.A.; Altibrandi, M.G.; Bentivoglio, A.; Caruso, G.; Cioni, B.; Fiorella, C.; Insola, A.; Lavano, A.; Maina, R.; Mazzone, P.; et al. Extradural Motor Cortex Stimulation (EMCS) for Parkinson’s disease. History and first results by the study group of the Italian neurosurgical society. Funct. Rehabil. Neurosurg. Neurotraumatol. 2005, 93, 113–119. [Google Scholar] [CrossRef]
- Priori, A.; Lefaucheur, J.-P. Chronic epidural motor cortical stimulation for movement disorders. Lancet Neurol. 2007, 6, 279–286. [Google Scholar] [CrossRef]
- Cioni, B. Motor cortex stimulation for Parkinson’s disease. Oper. Neuromodul. 2007, 97, 233–238. [Google Scholar] [CrossRef]
- Drouot, X.; Oshino, S.; Jarraya, B.; Besret, L.; Kishima, H.; Remy, P.; Dauguet, J.; Lefaucheur, J.P.; Dollé, F.; Condé, F.; et al. Functional Recovery in a Primate Model of Parkinson’s Disease following Motor Cortex Stimulation. Neuron 2004, 44, 769–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasano, A.; Piano, C.; De Simone, C.; Cioni, B.; Di Giuda, D.; Zinno, M.; Daniele, A.; Meglio, M.; Giordano, A.; Bentivoglio, A.R. High frequency extradural motor cortex stimulation transiently improves axial symptoms in a patient with Parkinson’s disease. Mov. Disord. 2008, 23, 1916–1919. [Google Scholar] [CrossRef] [PubMed]
- Canavero, S.; Paolotti, R. Extradural motor cortex stimulation for advanced Parkinson’s disease: Case report. Mov. Disord. 2000, 15, 169–171. [Google Scholar] [CrossRef]
- Canavero, S.; Paolotti, R.; Bonicalzi, V.; Castellano, G.; Greco-Crasto, S.; Rizzo, L.; Davini, O.; Zenga, F.; Ragazzi, P. Extradural motor cortex stimulation for advanced Parkinson disease. J. Neurosurg. 2002, 97, 1208–1211. [Google Scholar] [CrossRef] [PubMed]
- Cilia, R.; Landi, A.; Vergani, F.; Sganzerla, E.; Pezzoli, G.; Antonini, A. Extradural motor cortex stimulation in Parkinson’s disease. Mov. Disord. 2007, 22, 111–114. [Google Scholar] [CrossRef]
- Arle, J.E.; Apetauerova, D.; Zani, J.; Deletis, D.V.; Penney, D.L.; Hoit, D.; Gould, C.; Shils, J.L. Motor cortex stimulation in patients with Parkinson disease: 12-month follow-up in 4 patients. J. Neurosurg. 2008, 109, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez, J.C.; Seijo, F.J.; Vega, M.A.Á.; Gonzalez, F.F.; Aragoneses, B.L.; Blázquez, M. Therapeutic extradural cortical stimulation for Parkinson’s Disease: Report of six cases and review of the literature. Clin. Neurol. Neurosurg. 2009, 111, 703–707. [Google Scholar] [CrossRef]
- Moro, E.; Schwalb, J.M.; Piboolnurak, P.; Poon, Y.-Y.W.; Hamani, C.; Hung, S.W.; Arenovich, T.; Lang, A.E.; Chen, R.; Lozano, A.M. Unilateral subdural motor cortex stimulation improves essential tremor but not Parkinson’s disease. Brain 2011, 134, 2096–2105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentivoglio, A.R.; Fasano, A.; Piano, C.; Soleti, F.; Daniele, A.; Zinno, M.; Piccininni, C.; De Simone, C.; Policicchio, D.; Tufo, T.; et al. Unilateral Extradural Motor Cortex Stimulation Is Safe and Improves Parkinson Disease at 1 Year. Neurosurgery 2012, 71, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Cioni, B.; Tufo, T.; Bentivoglio, A.; Trevisi, G.; Piano, C. Motor cortex stimulation for movement disorders. J. Neurosurg. Sci. 2016, 60, 230–241. [Google Scholar]
- Lavano, A.; Guzzi, G.; De Rose, M.; Romano, M.; Della Torre, A.; Vescio, G.; Deodato, F.; Lavano, F.; Volpentesta, G. Minimally invasive motor cortex stimulation for Parkinson’s disease. J. Neurosurg. Sci. 2017, 61, 77–87. [Google Scholar]
- Samotus, O.; Parrent, A.; Jog, M. Spinal Cord Stimulation Therapy for Gait Dysfunction in Advanced Parkinson’s Disease Patients. Mov. Disord. 2018, 33, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clini-co-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahn, S.; Elton, R.; Members of the UPDRS Development Committee. The Unified Parkinson’s Disease Rating Scale. In Recent Developments in Parkinson’s Disease; Macmillan Healthcare Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–163. [Google Scholar]
- Defer, G.L.; Widner, H.; Marie, R.M.; Remy, P.; Levivier, M. Core assessment program for surgical interventional therapies in Parkinson’s disease (CAPSIT-PD). Mov. Disord. 1999, 14, 572–584. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; p. 5. [Google Scholar]
- Cioni, B.; Meglio, M.; Perotti, V.; De Bonis, P.; Montano, N. Neurophysiological aspects of chronic motor cortex stimulation. Neurophysiol. Clin. Neurophysiol. 2007, 37, 441–447. [Google Scholar] [CrossRef]
- De Boer, A.G.; Wijker, W.; Speelman, J.D.; De Haes, J.C. Quality of life in patients with Parkinson’s disease: Development of a questionnaire. J. Neurol. Neurosurg. Psychiatry 1996, 61, 70–74. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency report-ing in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Daniele, A.; Albanese, A.; Contarino, M.F.; Zinzi, P.; Barbier, A.; Gasparini, F.; Romito, L.M.A.; Bentivoglio, A.R.; Scerrati, M. Cognitive and behavioural effects of chronic stimulation of the subthalamic nucleus in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2003, 74, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Zung, W.W.K. A Self-Rating Depression Scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef]
- Zung, W.W. A Rating Instrument for Anxiety Disorders. J. Psychosom. Res. 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Fasano, A.; Aquino, C.C.; Krauss, J.K.; Honey, C.R.; Bloem, B.R. Axial disability and deep brain stimulation in patients with Parkinson disease. Nat. Rev. Neurol. 2015, 11, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Manola, L.; Holsheimer, J.; Veltink, P.; Buitenweg, J.R. Anodal vs cathodal stimulation of motor cortex: A modeling study. Clin. Neurophysiol. 2007, 118, 464–474. [Google Scholar] [CrossRef]
- Shirota, Y.; Ohtsu, H.; Hamada, M.; Enomoto, H.; Ugawa, Y.; For the Research Committee on rTMS Treatment of Parkinson’s Disease. Supplementary motor area stimulation for Parkinson disease: A randomized controlled study. Neurology 2013, 80, 1400–1405. [Google Scholar] [CrossRef]
- Piano, C.; Fasano, A.; Daniele, A.; Di Giuda, D.; Ciavarro, M.; Tufo, T.; Zinno, M.; Bentivoglio, A.R.; Cioni, B. Extradural motor cortex stimulation improves gait, speech, and language in a patient with pure akinesia. Brain Stimul. 2018, 11, 1192–1194. [Google Scholar] [CrossRef] [PubMed]
- Schrag, A.; Dodel, R.; Spottke, A.; Bornschein, B.; Siebert, U.; Quinn, N.P. Rate of clinical progression in Parkinson’s disease. A prospective study. Mov. Disord. 2007, 22, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Koch, G. rTMS effects on levodopa induced dyskinesias in Parkinson’s disease patients: Searching for effective cortical targets. Restor. Neurol. Neurosci. 2010, 28, 561–568. [Google Scholar] [CrossRef]
- Calabresi, P.; Ghiglieri, V.; Mazzocchetti, P.; Corbelli, I.; Picconi, B. Levodopa-induced plasticity: A double-edged sword in Parkinson’s disease? Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swann, N.C.; De Hemptinne, C.; Thompson, M.C.; Miocinovic, S.; Miller, A.M.; Gilron, R.; Ostrem, J.L.; Chizeck, H.J.; Starr, P.A. Adaptive deep brain stimulation for Parkinson’s disease using motor cortex sensing. J. Neural Eng. 2018, 15, 046006. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Romito, L.M.; Daniele, A.; Piano, C.; Zinno, M.; Bentivoglio, A.R.; Albanese, A. Motor and cognitive outcome in patients with Parkinson’s disease 8 years after subthalamic implants. Brain 2010, 133, 2664–2676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piano, C.; Ciavarro, M.; Bove, F.; Di Giuda, D.; Cocciolillo, F.; Bentivoglio, A.R.; Cioni, B.; Tufo, T.; Calabresi, P.; Daniele, A. Extradural Motor Cortex Stimulation might improve episodic and working memory in patients with Parkinson’s disease. NPJ Park. Dis. 2020, 6, 26. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Gender | Age at Surgery | UPDRS III Off-Med | UPDRS III On-Med | Hoehn and Yahr Stage | UPDRS IV | LEDD (mg) | Reason DBS Not Performed |
|---|---|---|---|---|---|---|---|---|
| 1 | F | 57 | 8 | 55 | 24 | 5 | 13 | Patient refusal |
| 2 | M | 55 | 16 | 68 | 19 | 5 | 13 | Brain atrophy |
| 3 | M | 62 | 9 | 62 | 18 | 4 | 11 | Patient refusal |
| 4 | F | 57 | 14 | 64 | 24 | 5 | 15 | Brain atrophy |
| 5 | F | 66 | 28 | 61 | 35 | 5 | 12 | Patient refusal |
| 6 | F | 69 | 17 | 59 | 15 | 5 | 12 | Age and comorbidities |
| 7 | F | 70 | 14 | 62 | 17 | 5 | 9 | Age and comorbidities |
| 8 | M | 72 | 11 | 43 | 16 | 3 | 6 | Age and comorbidities |
| 9 | M | 68 | 14 | 40 | 18 | 3 | 3 | Patient refusal |
| Total | 4 M/5 F | 64.0 ± 6.4 | 14.6 ± 5.9 | 57.1 ± 9.5 | 20.7 ± 6.2 | 4.4 ± 0.9 | 10.4 ± 3.8 |
| Baseline (n = 9) | 12 m (n = 9) | 18 m (n = 9) | 24 m (n = 9) | 36 m (n = 7) | 48 m (n = 6) | 60 m (n = 5) | 72 m (n = 5) | 84 m (n = 2) | 96 m (n = 2) | |
|---|---|---|---|---|---|---|---|---|---|---|
| UPDRS III med-off | 57.1 ± 9.5 | 49.2 ± 9.4 * | 47.9 ± 12.4 * | 46.6 ± 11.0 * | 45.1 ± 12.7 * | 52.3 ± 14.0 | 48.2 ± 4.0 * | 52.2 ± 6.2 * | 45.5 ± 13.4 | 49.5 ± 9.2 |
| UPDRS III axial score med-off | 13.6 ± 5.6 | 11.9 ± 3.8 | 9.9 ± 3.3 * | 9.7 ± 2.6 * | 10.7 ± 3.5 | 13.5 ± 4.0 | 12.8 ± 3.1 * | 14.4 ± 3.7 | 11.5 ± 4.9 | 14.0 ± 4.2 |
| UPDRS III med-on | 20.7 ± 6.2 | 27.1 ± 8.7 | 26.0 ± 6.5 | 26.7 ± 6.2 | 30.0 ± 7.1 * | 34.8 ± 9.9 * | 33.2 ± 5.1 * | 39.2 ± 9.0 * | 37.5 ± 13.4 | 45.0 ± 9.9 |
| UPDRS IV | 10.4 ± 3.8 | 7.2 ± 3.6 * | 8.0 ± 4.0 | 8.1 ± 3.0 * | 9.7 ± 3.3 | 10.3 ± 2.7 | 7.8 ± 1.6 * | 6.6 ± 2.3 * | 7.5 ± 2.1 | 7.5 ± 2.1 |
| LEDD | 1203.0 ± 528.1 | 1085.8 ± 424.5 | 1108.0 ± 402.3 | 1050.8 ± 369.3 | 962.4 ± 455.6 | 929.9 ± 401.0 | 1061.3 ± 286.5 * | 1214.2 ± 670.8 | 905.0 ± 254.6 | 915.0 ± 268.7 |
| UPDRS II | 27.5 ± 10.0 | 22.4 ± 6.9 * | 19.1 ± 6.9 | 24.7 ± 9.0 | 27.5 ± 6.1 | 25.3 ± 8.8 | 22.6 ± 4.0 * | 23.6 ± 3.2 * | 25.0 ± 1.4 | 27.5 ± 2.1 |
| PDQL | 83.5 ± 19.1 | 98.5 ± 20.0 * | 96.0 ± 15.0 | 95.4 ± 15.5 | 92.7 ± 15.7 | 91.8 ± 22.1 | 102.2 ± 19.6 * | 99.2 ± 28.3 | 88.0 ± 15.6 | 102.5 ± 44.5 |
| UPDRS tot | 98.8 ± 24.5 | 82.3 ± 16.9 * | 79.1 ± 21.5 * | 83.7 ± 22.1 * | 89.3 ± 17.5 | 92.3 ± 23.8 | 82.8 ± 5.5 | 88.0 ± 8.5 | 83.5 ± 10.6 | 90.0 ± 8.5 |
| Baseline (n = 9) | 12 m (n = 9) | 18 m (n = 9) | 36 m (n = 7) | 60 m (n = 5) | 96 m (n = 2) | |
|---|---|---|---|---|---|---|
| MMSE | 25.3 ± 2.6 | 25.9 ± 3.0 | 26.7 ± 3.2 * | 26.5 ± 3.9 | 25.0 ± 4.6 | 25.0 ± 2.8 |
| Digit Span forward | 4.6 ± 0.7 | 4.7 ± 1.0 | 4.4 ± 0.5 | 4.0 ± 0.6 | 5.0 ± 0 | 4.5 ± 0.7 |
| Digit Span backward | 3.2 ± 0.7 | 3.0 ± 0.7 | 3.0 ± 0.8 | 3.3 ± 0.8 | 3.0 ± 0 | 3.5 ± 0.7 |
| Corsi’s Span forward | 4.8 ± 1.3 | 4.6 ± 1.2 | 4.4 ± 1.5 | 4.2 ± 1.2 | 4.0 ± 0 | 3.5 ± 0.7 |
| Corsi’s Span backward | 3.8 ± 1.0 | 3.4 ± 1.2 | 3.1 ± 0.9 | 4.2 ± 1.5 | 3.7 ± 0.6 | 3.0 ± 0 |
| RAVLT immediate recall | 35.3 ± 6.8 | 42.2 ± 12.2 | 45.9 ± 10.9 * | 32.7 ± 5.7 | 43.7 ± 7.0 | 23.5 ± 2.1 |
| RAVLT delayed recall | 7.0 ± 2.2 | 8.5 ± 3.7 | 9.7 ± 3.0 * | 6.2 ± 1.2 | 10.0 ± 4.4 | 4.0 ± 0 |
| RPM ’47 | 20.0 ± 7.3 | 21.5 ± 2.7 | 21.4 ± 6.9 | 22.7 ± 8.6 | 24.0 ± 9.2 | 19.5 ± 4.9 |
| Phonological verbal fluency | 17.3 ± 8.3 | 19.5 ± 11.9 | 23.0 ± 13.6 | 19.2 ± 11.0 | 20.7 ± 9.3 | 21.0 ± 15.6 |
| Semantic verbal fluency | 14.1 ± 4.0 | 12.7 ± 4.1 | 13.9 ± 3.4 | 14.0 ± 5.1 | 16.3 ± 6.8 | 15.0 ± 8.5 |
| mWCST criteria | 2.4 ± 1.6 | 2.6 ± 1.7 | 3.7 ± 2.1 | 2.8 ± 1.6 | 2.3 ± 2.3 | 1.5 ± 0.7 |
| mWCST total errors | 23.4 ± 10.4 | 20.5 ± 8.7 | 17.1 ± 11.6 | 19.8 ± 8.3 | 24.0 ± 17.6 | 21.0 ± 1.4 |
| mWCST perseverative errors | 8.1 ± 4.9 | 8.5 ± 5.6 | 7.0 ± 5.4 | 6.5 ± 3.3 | 6.6 ± 7.0 | 6.5 ± 3.5 |
| Stroop interference time | 33.7 ± 32.2 | 35.2 ± 17.8 | 35.0 ± 25.1 | 25.7 ± 14.0 | 48.3 ±55.2 | 37.5 ±10.6 |
| Stroop interference errors | 1.5 ± 3.9 | 2.2 ± 3.6 | 3.1 ± 4.8 | 2.3 ± 2.1 | 3.0 ± 3.3 | 6.0 ± 8.5 |
| Zung Depression Scale | 45.6 ± 13.6 | 46.4 ± 12.5 | 44.6 ± 8.1 | 47.3 ± 8.8 | 47.6 ± 9.3 | 55.0 ± 1.4 |
| Zung Anxiety Scale | 44.9 ± 12.9 | 47.5 ± 10.0 | 44.4 ± 8.0 | 46.8 ± 8.5 | 43.0 ± 11.5 | 44.0 ± 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piano, C.; Bove, F.; Mulas, D.; Di Stasio, E.; Fasano, A.; Bentivoglio, A.R.; Daniele, A.; Cioni, B.; Calabresi, P.; Tufo, T. Extradural Motor Cortex Stimulation in Parkinson’s Disease: Long-Term Clinical Outcome. Brain Sci. 2021, 11, 416. https://doi.org/10.3390/brainsci11040416
Piano C, Bove F, Mulas D, Di Stasio E, Fasano A, Bentivoglio AR, Daniele A, Cioni B, Calabresi P, Tufo T. Extradural Motor Cortex Stimulation in Parkinson’s Disease: Long-Term Clinical Outcome. Brain Sciences. 2021; 11(4):416. https://doi.org/10.3390/brainsci11040416
Chicago/Turabian StylePiano, Carla, Francesco Bove, Delia Mulas, Enrico Di Stasio, Alfonso Fasano, Anna Rita Bentivoglio, Antonio Daniele, Beatrice Cioni, Paolo Calabresi, and Tommaso Tufo. 2021. "Extradural Motor Cortex Stimulation in Parkinson’s Disease: Long-Term Clinical Outcome" Brain Sciences 11, no. 4: 416. https://doi.org/10.3390/brainsci11040416