Distribution of Helicobacter pylori and Periodontopathic Bacterial Species in the Oral Cavity

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Subjects
2.3. Oral Cavity Specimens
2.4. H. pylori Strains and Growth Condition
2.5. Bacterial DNA Extraction
2.6. PCR Detection of H. pylori
2.7. PCR Detection of Periodontopathic Bacterial Species
2.8. PCR Detection of fimA Genotypes
2.9. Statistical Analysis
3. Results
3.1. Clinical Characteristics of H. pylori-Positive and H. pylori-Negative Subjects
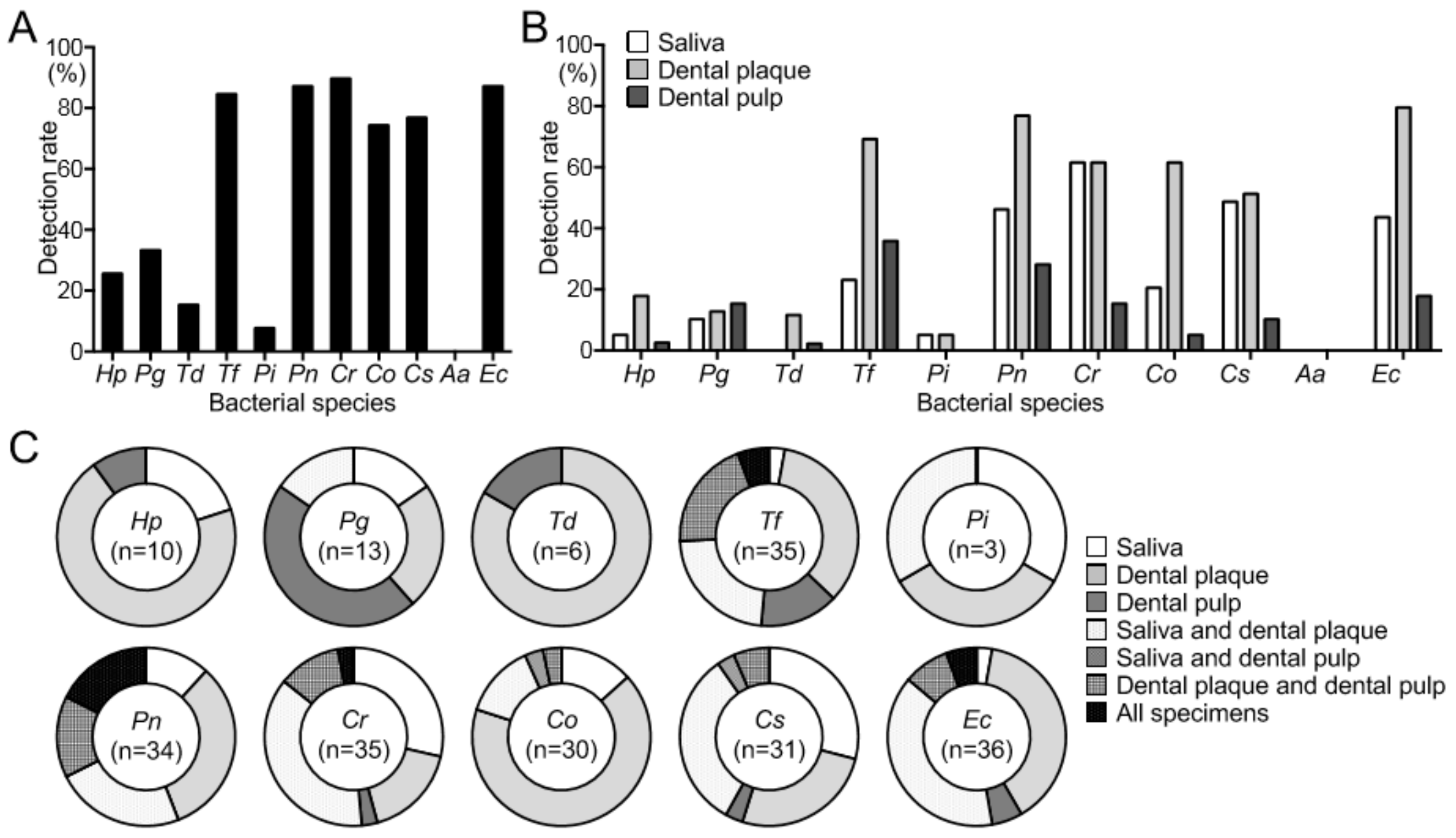
3.2. Detection of H. pylori and Periodontopathic Bacterial Species
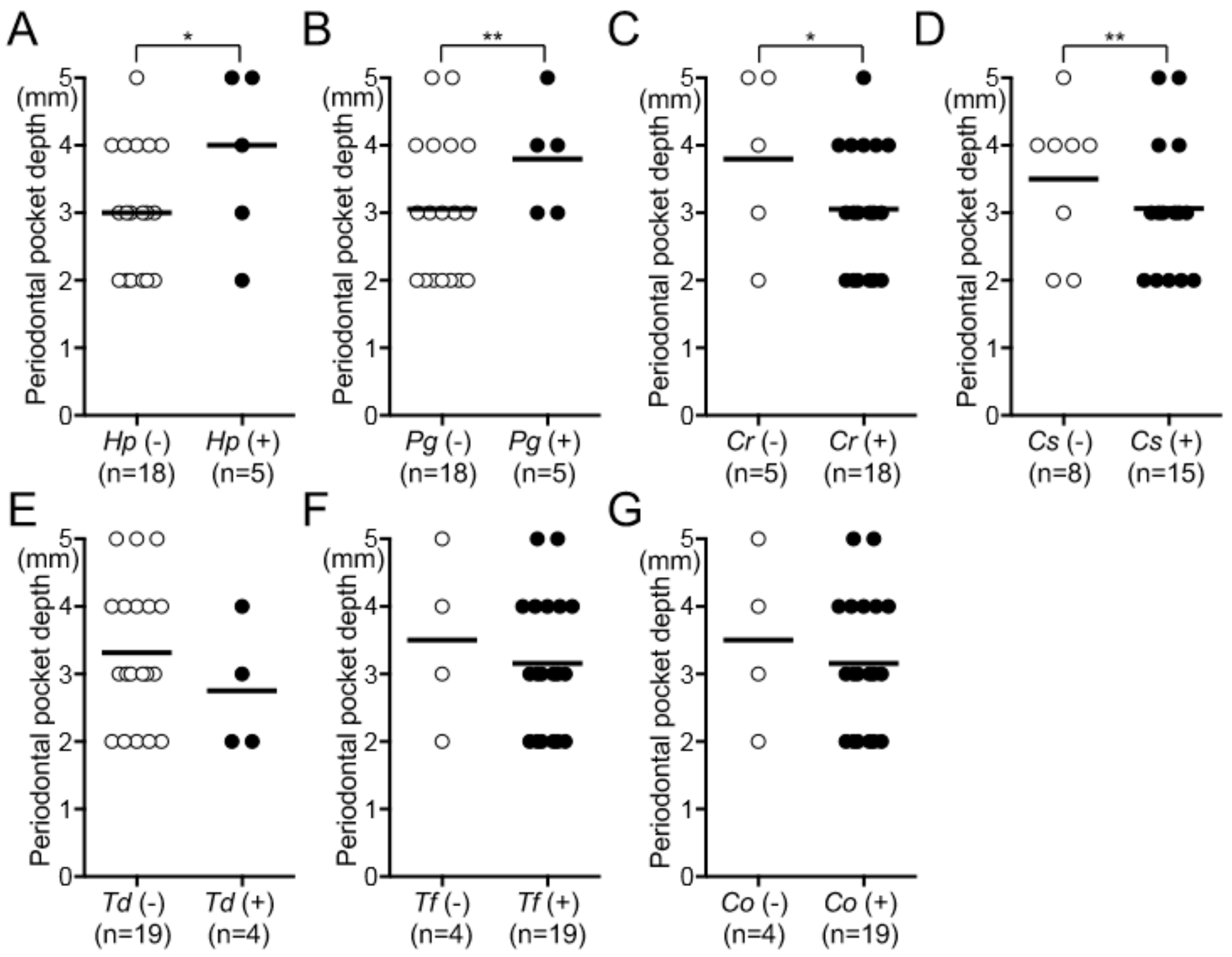
3.3. Relationship between H. pylori and Oral Disease
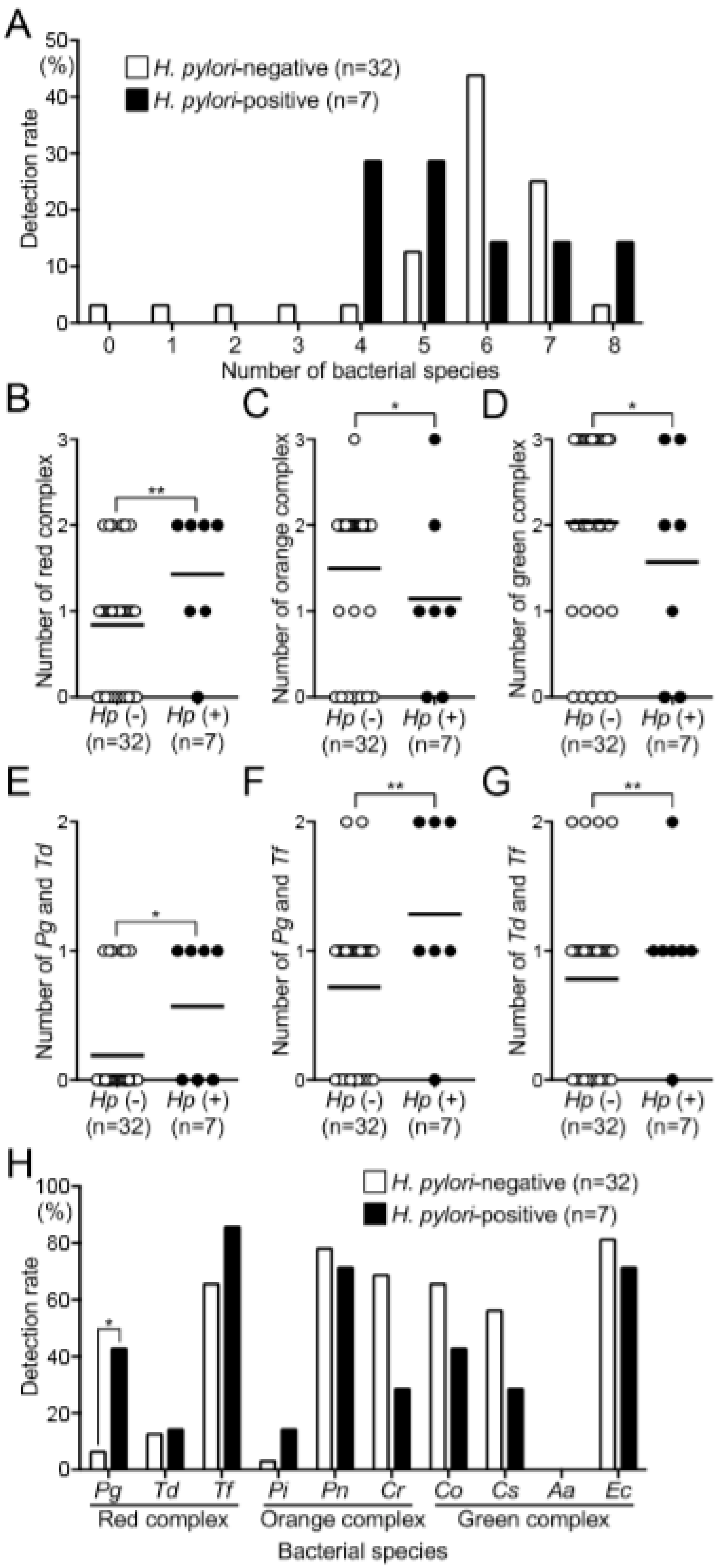
3.4. Relationship between H. pylori and Periodontopathic Bacterial Species
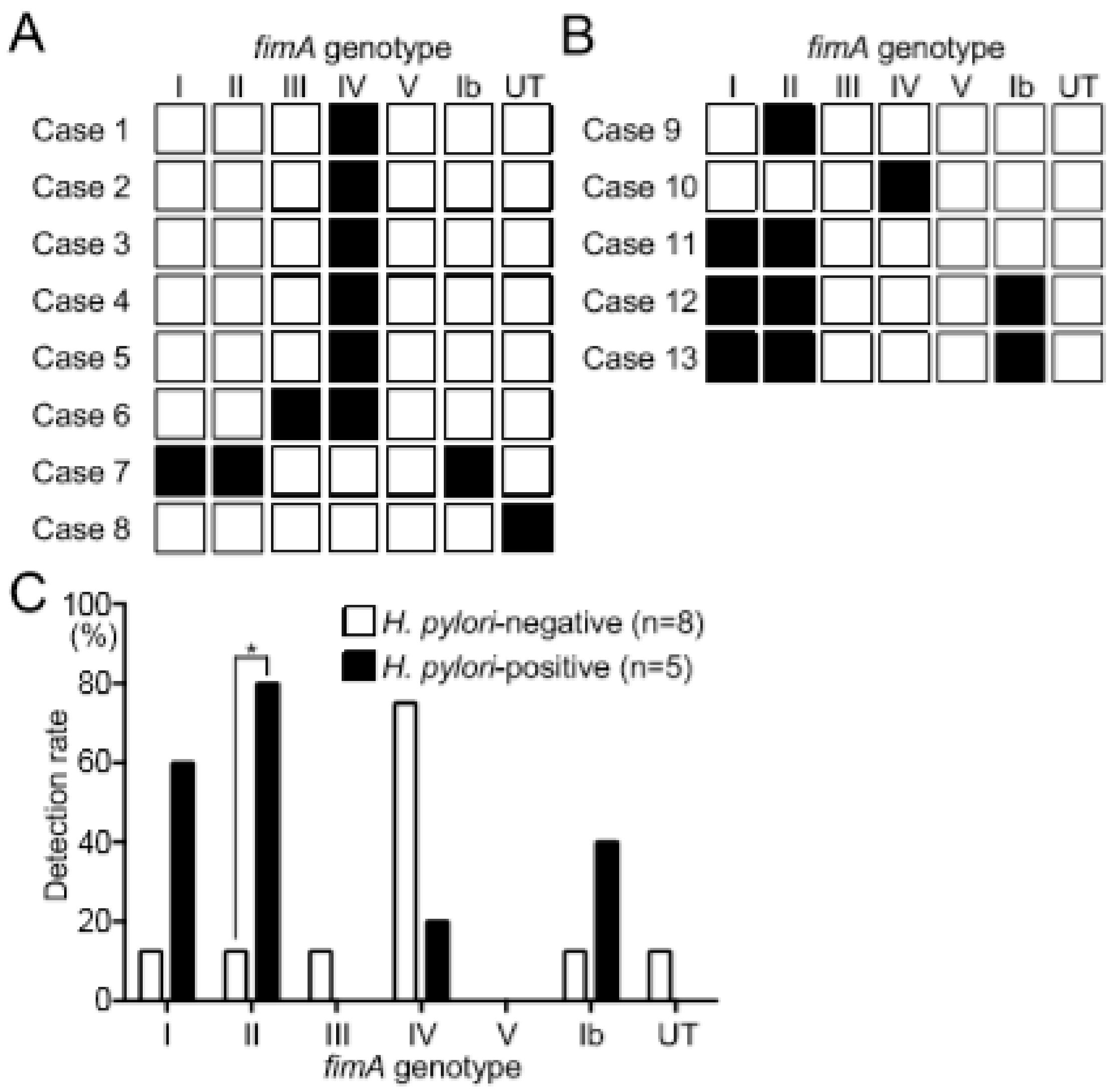
3.5. Distribution of fimA Genotypes in Subjects with or without H. pylori
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dunn, B.E.; Cohen, H.; Blaser, M.J. Helicobacter pylori. Clin. Microbiol. Rev. 1997, 10, 720–741. [Google Scholar] [CrossRef]
- Desai, H.; Gill, H.; Shankaran, K.; Mehta, P.; Prabhu, S.R. Dental plaque: A permanent reservoir of Helicobacter pylori? Scand. J. Gastroenterol. 1991, 26, 1205–1208. [Google Scholar] [CrossRef]
- Jia, C.L.; Jiang, G.S.; Li, C.H.; Li, C.R. Effect of dental plaque control on infection of Helicobacter pylori in gastric mucosa. Tex. Dent. J. 2012, 129, 1069–1073. [Google Scholar] [PubMed]
- Robert, J.; Palmer, J.R. Composition and development of oral bacterial communities. Periodontology 2000 2013, 64, 20–39. [Google Scholar]
- Socransky, S.S.; Haffajee, A.D. Dental biofilms: Difficult therapeutic targets. Periodontology 2000 2002, 28, 12–55. [Google Scholar] [CrossRef] [PubMed]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Mascitti, M.; Togni, L.; Troiano, G.; Caponio, V.C.A.; Gissi, D.B.; Montebugnoli, L.; Procaccini, M.; Lo Muzio, L.; Santarelli, A. Beyond head and neck cancer: The relationship between oral microbiota and tumour development in distant organs. Front. Cell Infect. Microbiol. 2019, 9, 232. [Google Scholar] [CrossRef]
- Hu, Z.; Zhang, Y.; Li, Z.; Yu, Y.; Kang, W.; Han, Y.; Geng, X.; Ge, S.; Sun, Y. Effect of Helicobacter pylori infection on chronic periodontitis by the change of microecology and inflammation. Oncotarget 2016, 7, 66700–66712. [Google Scholar] [CrossRef] [Green Version]
- Duran-Pinedo, A.E.; Baker, V.D.; Frias-Lopez, J. The periodontal pathogen Porphyromonas gingivalis induces expression of transposases and cell death of Streptococcus mitis in a biofilm model. Infect. Immun. 2014, 82, 3374–3382. [Google Scholar] [CrossRef] [Green Version]
- Kuboniwa, M.; Inaba, H.; Amano, A. Genotyping to distinguish microbial pathogenicity in periodontitis. Periodontology 2000 2010, 54, 136–159. [Google Scholar] [CrossRef]
- Silva, D.G.; Tinoco, E.M.; Rocha, G.A.; Rocha, A.M.; Guerra, J.B.; Saraiva, I.E.; Queiroz, D.M. Helicobacter pylori transiently in the mouth may participate in the transmission of infection. Mem. Inst. Oswaldo. Cruz. 2010, 105, 657–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogaya, Y.; Nomura, R.; Watanabe, Y.; Nakano, K. Detection of Helicobacter pylori DNA in inflamed dental pulp specimens from Japanese children and adolescents. J. Med. Microbiol. 2015, 64, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nomura, R.; Ogaya, Y.; Matayoshi, S.; Morita, Y.; Nakano, K. Molecular and clinical analyses of Helicobacter pylori colonization in inflamed dental pulp. BMC Oral Health 2018, 18, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamada, M.; Nomura, R.; Ogaya, Y.; Matayoshi, S.; Kadota, T.; Morita, Y.; Uzawa, N.; Nakano, K. Potential involvement of Helicobacter pylori from oral specimens in overweight body-mass index. Sci. Rep. 2019, 9, 4845. [Google Scholar] [CrossRef]
- Kadota, T.; Ogaya, Y.; Hatakeyama, R.; Nomura, R.; Nakano, K. Comparison of oral flora before and after triple therapy for Helicobacter pylori eradication in patient with gastric disease. Odontology 2019, 107, 261–267. [Google Scholar] [CrossRef]
- Iwai, K.; Watanabe, I.; Yamamoto, T.; Kuriyama, N.; Matsui, D.; Nomura, R.; Ogaya, Y.; Oseko, F.; Adachi, K.; Takizawa, S.; et al. Association between Helicobacter pylori infection and dental pulp reservoirs in Japanese adults. BMC Oral Health 2019, 19, 267. [Google Scholar] [CrossRef] [Green Version]
- Lauritano, D.; Cura, F.; Candotto, V.; Gaudio, R.M.; Mucchi, D.; Carinci, F. Periodontal pockets as a reservoir of Helicobacter pylori causing relapse of gastric ulcer: A review of the literature. J. Biol. Regul. Homeost. Agent. 2015, 29, 123–126. [Google Scholar]
- Tongtawee, T.; Wattanawongdon, W.; Simawaranon, T. Effects of periodontal therapy on eradication and recurrence of Helicobacter pylori infection after successful treatment. J. Int. Med. Res. 2019, 47, 875–883. [Google Scholar] [CrossRef] [Green Version]
- Marques da Silva, R.; Caugant, D.A.; Eribe, E.R.; Aas, J.A.; Lingaas, P.S.; Geiran, O.; Tronstad, L.; Olsen, I. Bacterial diversity in aortic aneurysms determined by 16S ribosomal RNA gene analysis. J. Vasc. Surg. 2006, 44, 1055–1060. [Google Scholar] [CrossRef] [Green Version]
- Kato, Y.; Shirai, M.; Murakami, M.; Mizusawa, T.; Hagimoto, A.; Wada, K.; Nomura, R.; Nakano, K.; Ooshima, T.; Asai, F. Molecular detection of human periodontal pathogens in oral swab specimens from dogs in Japan. J. Vet. Dent. 2011, 28, 84–89. [Google Scholar] [CrossRef]
- Watanabe, K.; Frommel, T.O. Porphyromonas gingivalis, Actinobacillus actinomycetemcomitans and Treponema denticola detection in oral plaque samples using the polymerase chain reaction. J. Clin. Periodontol. 1996, 23, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Ashimoto, A.; Chen, C.; Bakker, I.; Slots, J. Polymerase chain reaction detection of 8 putative periodontal pathogens in subgingival plaque of gingivitis and advanced periodontitis lesions. Oral Microbiol. Immunol. 1996, 11, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Conrads, G.; Mutters, R.; Fischer, J.; Brauner, A.; Lütticken, R.; Lampert, F. PCR reaction and dot-blot hybridization to monitor the distribution of oral pathogens within plaque samples of periodontally healthy individuals. J. Periodontol. 1996, 67, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Kuboniwa, M.; Amano, A.; Kimura, K.R.; Sekine, S.; Kato, S.; Yamamoto, Y.; Okahashi, N.; Iida, T.; Shizukuishi, S. Quantitative detection of periodontal pathogens using real-time polymerase chain reaction with TaqMan probes. Oral Microbiol. Immunol. 2004, 19, 168–176. [Google Scholar] [CrossRef]
- Amano, A.; Nakagawa, I.; Kataoka, K.; Morisaki, I.; Hamada, S. Distribution of Porphyromonas gingivalis strains with fimA genotypes in periodontitis patients. J. Clin. Microbiol. 1999, 37, 1426–1430. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, I.; Amano, A.; Kimura, R.K.; Nakamura, T.; Kawabata, S.; Hamada, S. Distribution and molecular characterization of Porphyromonas gingivalis carrying a new type of fimA gene. J. Clin. Microbiol. 2000, 38, 1909–1914. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, I.; Amano, A.; Ohara-Nemoto, Y.; Endoh, N.; Morisaki, I.; Kimura, S.; Kawabata, S.; Hamada, S. Identification of a new variant of fimA gene of Porphyromonas gingivalis and its distribution in adults and disabled populations with periodontitis. J. Periodontal Res. 2002, 37, 425–432. [Google Scholar] [CrossRef]
- Hart, R.; Doherty, D.A.; Pennell, C.E.; Newnham, I.A.; Newnham, J.P. Periodontal disease: A potential modifiable risk factor limiting conception. Hum. Reprod. 2012, 27, 1332–1342. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal pathogens as risk factors of cardiovascular diseases, diabetes, rheumatoid arthritis, cancer, and chronic obstructive pulmonary disease—Is there cause for consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Ahn, J.; Chen, C.Y.; Hayes, R.B. Oral microbiome and oral and gastrointestinal cancer risk. Cancer Causes Control 2012, 23, 399–404. [Google Scholar] [CrossRef]
- Tamura, K.; Nakano, K.; Nomura, R.; Miyake, S.; Nakagawa, I.; Amano, A.; Ooshima, T. Distribution of Porphyromonas gingivalis fimA genotypes in Japanese children and adolescents. J. Periodontol. 2005, 76, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Inaba, H.; Nomura, R.; Nemoto, H.; Takeuchi, H.; Yoshioka, H.; Toda, K.; Taniguchi, K.; Amano, A.; Ooshima, T. Distribution of Porphyromonas gingivalis fimA genotypes in cardiovascular specimens from Japanese patients. Oral Microbiol. Immunol. 2008, 23, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Wada, K.; Nomura, R.; Nemoto, H.; Inaba, H.; Kojima, A.; Naka, S.; Hokamura, K.; Mukai, T.; Hata, H.; et al. Characterization of aortic aneurysm in cardiovascular disease patients harboring Porphyromonas gingivalis. Oral Dis. 2011, 17, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Ogunbodede, E.O.; Lawal, O.O.; Lamikanra, A.; Okeke, I.N.; Rotimi, O.; Rasheed, A.A. Helicobacter pylori in the dental plaque and gastric mucosa of dyspeptic Nigerian patients. Trop. Gastroenterol. 2002, 23, 127–133. [Google Scholar]
- Sudhakar, U.; Anusuya, C.N.; Ramakrishnan, T.; Vijayalakshmi, R. Isolation of Helicobacter pylori from dental plaque: A microbiological study. J. Indian. Soc. Periodontol. 2008, 12, 67–72. [Google Scholar] [CrossRef]
- Hirsch, C.; Tegtmeyer, N.; Rohde, M.; Rowland, M.; Oyarzabal, O.A.; Backert, S. Live Helicobacter pylori in the root canal of endodontic-infected deciduous teeth. J. Gastroenterol. 2012, 47, 936–940. [Google Scholar] [CrossRef]
- How, K.Y.; Song, K.P.; Chan, K.G. Porphyromonas gingivalis: An overview of periodontopathic pathogen below the gum line. Front. Microbiol. 2016, 7, 53. [Google Scholar] [CrossRef]
- Tanaka, M.; Hanioka, T.; Tkaya, K.; Shizukuishi, S. Association of oxygen tension in human periodontal pockets with gingival inflammation. J. Periodontol. 1998, 69, 1127–1130. [Google Scholar] [CrossRef]
- Moran, A.P. The role of endotoxin in infection: Helicobacter pylori and Campylobacter jejuni. Subcell. Biochem. 2010, 53, 209–240. [Google Scholar]
- Dhonge, R.P.; Zade, R.M.; Gopinath, V.; Amirisetty, R. An insight into pericoronitis. Int. J. Dent. Med. Res. 2015, 6, 172–175. [Google Scholar]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global prevalence of Helicobacter pylori infection: Systematic review and meta-analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, R.; Ishihara, K.; Shoji, M.; Nakayama, K.; Okuda, K. Hemagglutinin/Adhesin domains of Porphyromonas gingivalis play key roles in coaggregation with Treponema denticola. FEMS Immunol. Med. Micobiol. 2010, 60, 251–260. [Google Scholar] [CrossRef] [Green Version]
- Tan, K.H.; Seers, C.A.; Dashper, S.G.; Mitchell, H.L.; Pyke, J.S.; Meuric, V.; Slakeski, N.; Cleal, S.M.; Chamber, J.L.; McConville, M.J.; et al. Porphyromonas gingivalis and Treponema denticola exhibit metabolic symbioses. PLoS Pathog. 2014, 10, e1003955. [Google Scholar] [CrossRef] [PubMed]
- Sano, Y.; Okamoto-Shibayama, K.; Tanaka, K.; Ito, R.; Shintani, S.; Yakushiji, M.; Ishihara, K. Dentilisin involvement in coaggregation between Treponema denticola and Tannerella forsythia. Anaerobe 2014, 30, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Kigure, T.; Saito, A.; Seida, K.; Yamada, S.; Ishihara, K.; Okuda, K. Distribution of Porphyromonas gingivalis and Treponema denticola in human subgingival plaque at different periodontal pocket depths examined by immunohistochemical methods. J. Periodontal Res. 1995, 30, 332–341. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Purpose | Sequence (5′-3′) | Size (bp) | References |
|---|---|---|---|
| Universal primer | |||
| (positive control) | 315 | [19] | |
| PA (forward) | F: AGA GTT TGA TCC TGG CTC AG | ||
| PD (reverse) | R: GTA TTA CCG CGG CTG CTG | ||
| Detection of H. pylori | |||
| First step PCR | 488 | [13] | |
| ureA-aF | F: ATG AAA CTC ACC CCA AAA GA | ||
| ureA-bR | R: CCG AAA GTT TTT TCT CTG TCA AAG TCT A | ||
| Second step PCR | 383 | [13] | |
| ureA-bF | F: AAA CGC AAA GAA AAA GGC ATT AA | ||
| ureA-aR | R: TTC ACT TCA AAG AAA TGG AAG TGT GA | ||
| Detection of periodontitis-related species | 267 | [20] | |
| Porphyromonas gingivalis | F: CCG CAT ACA CTT GTA TTA TTG CAT GAT A | ||
| R: AAG AAG TTT ACA ATC CTT AGG ACT GTC T | |||
| Treponema denticola | F: AAG GCG GTA GAG CCG CTC A | 311 | [21] |
| R: AGC CGC TGT CGA AAA GCC CA | |||
| Tannerella forsythia | F: GCG TAT GTA ACC TGC CCG CA | 641 | [22] |
| R: TGC TTC AGT GTC AGT TAT ACC T | |||
| Capnocytophaga ochracea | F: AGA GTT TGA TCC TGG CTC AG | 185 | [23] |
| R: GAT GCC GTC CCT ATA TAC TAT GGG G | |||
| Capnocytophaga sputigena | F: AGA GTT TGA TCC TGG CTC AG | 185 | [23] |
| R: GAT GCC GCT CCT ATA TAC CAT TAG G | |||
| Prevotella intermedia | F: TTT GTT GGG GAG TAA AGC GGG | 575 | [22] |
| R: TCA ACA TCT CTG TAT CCT GCG T | |||
| Prevotella nigrescens | F: ATG AAA CAA AGG TTT TCC GGT AAG | 804 | [22] |
| R: CCC ACG TCT CTG TGG GCT GCG A | |||
| Campylobacter rectus | F: TTT CGG AGC GTA AAC TCC TTT TC | 598 | [22] |
| R: TTT CTG CAA GCA GAC ACT CTT | |||
| Aggregatibacter actinomycetemcomitans | F: CTA CTA AGC AAT CAA GTT GCC C | 262 | [24] |
| R: CCT GAA ATT AAG CTG GTA ATC | |||
| Eikenella corrodens | F: CTA ATA CCG CAT ACG TCC TAA G | 688 | [22] |
| R: CTA CTA AGC AAT CAA GTT GCC C | |||
| Specification of fimA genotype | 392 | [25] | |
| Type I fimA | F: CTG TGT GTT TAT GGC AAA CTT C | ||
| R: AAC CCC GCT CCC TGT ATT CCG A | |||
| Type II fimA | F: ACA ACT ATA CTT ATG ACA ATG G | 257 | [25] |
| R: AAC CCC GCT CCC TGT ATT CCG A | |||
| Type III fimA | F: ATT ACA CCT ACA CAG GTG AGG C | 247 | [25] |
| R: AAC CCC GCT CCC TGT ATT CCG A | |||
| Type IV fimA | F: CTA TTC AGG TGC TAT TAC CCA A | 251 | [25] |
| R: AAC CCC GCT CCC TGT ATT CCG A | |||
| Type V fimA | F: AAC AAC AGT CTC CTT GAC AGT G | 462 | [26] |
| R: TAT TGG GGG TCG AAC GTT ACT GTC | |||
| Type Ib fimA | F: CAG CAG AGC CAA AAA CAA TCG | 271 | [27] |
| R: TGT CAG ATA ATT AGC GTC TGC |
| Clinical Characteristics | H. pylori-Negative (n = 29) | H. pylori-Positive (n = 10) |
|---|---|---|
| Age (years; mean ± SD) | 32.1 ± 12.9 | 44.4 ± 17.9 |
| Sex (Male (%)) | 10 (34.5%) | 3 (30.0%) |
| History of systemic disease (%) | 8 (27.6%) | 5 (50.0%) |
| History of gastrointestinal disease (%) | 2 (6.9%) | 1 (10.0%) |
| History of H. pylori infection in gastric tissue (%) | 2 (6.9%) | 2 (20.0%) |
| Eradication of H. pylori in gastric tissue (%) | 2 (6.9%) | 2 (20.0%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadota, T.; Hamada, M.; Nomura, R.; Ogaya, Y.; Okawa, R.; Uzawa, N.; Nakano, K. Distribution of Helicobacter pylori and Periodontopathic Bacterial Species in the Oral Cavity. Biomedicines 2020, 8, 161. https://doi.org/10.3390/biomedicines8060161
Kadota T, Hamada M, Nomura R, Ogaya Y, Okawa R, Uzawa N, Nakano K. Distribution of Helicobacter pylori and Periodontopathic Bacterial Species in the Oral Cavity. Biomedicines. 2020; 8(6):161. https://doi.org/10.3390/biomedicines8060161
Chicago/Turabian StyleKadota, Tamami, Masakazu Hamada, Ryota Nomura, Yuko Ogaya, Rena Okawa, Narikazu Uzawa, and Kazuhiko Nakano. 2020. "Distribution of Helicobacter pylori and Periodontopathic Bacterial Species in the Oral Cavity" Biomedicines 8, no. 6: 161. https://doi.org/10.3390/biomedicines8060161