
Enalapril Is Superior to Lisinopril in Improving Endothelial Function without a Difference in Blood–Pressure–Lowering Effects in Newly Diagnosed Hypertensives
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABPM | Ambulatory blood pressure monitoring |
| ACE | Angiotensin-converting enzyme |
| ACEi | Angiotensin-converting enzyme inhibitors |
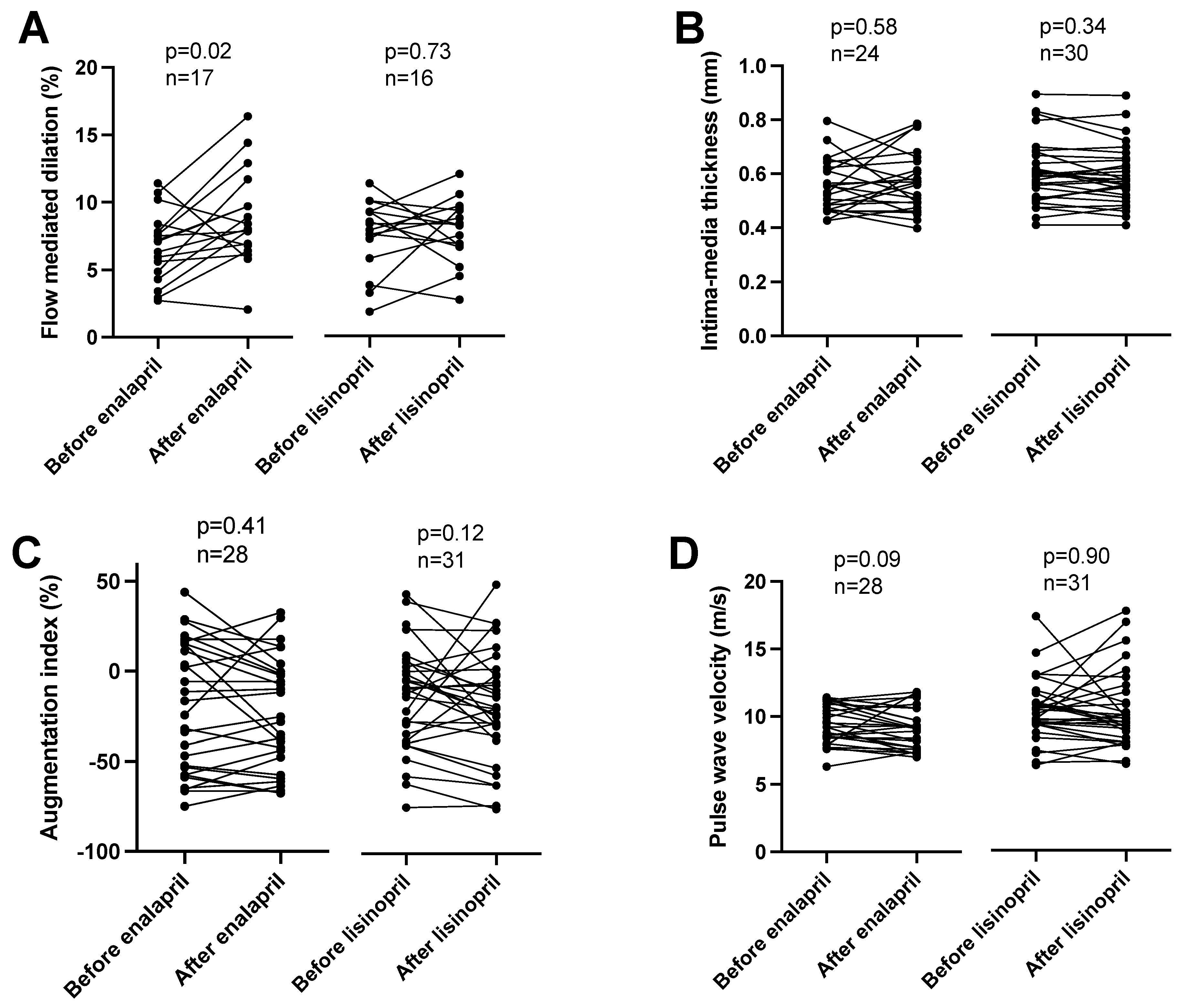
| AIx | Augmentation Index |
| FMD | Flow-mediated dilation |
| PWV | Pulse Wave Velocity |
References
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure. J. Card. Fail. 2017, 23, 628–651. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.J.; Vaughan, D.E. Angiotensin-Converting Enzyme Inhibitors. Circulation 1998, 97, 1411–1420. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, H.; Henning, F.; Täger, T.; Schellberg, D.; Grundtvig, M.; Goode, K.; Corletto, A.; Kazmi, S.; Hole, T.; Katus, H.A.; et al. Comparative effectiveness of enalapril, lisinopril, and ramipril in the treatment of patients with chronic heart failure: A propensity score-matched cohort study. Eur. Heart J. Cardiovasc. Pharmacother. 2018, 4, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Chitnis, A.S.; Aparasu, R.R.; Chen, H.; Johnson, M.L. Comparative effectiveness of different angiotensin-converting enzyme inhibitors on the risk of hospitalization in patients with heart failure. J. Comp. Eff. Res. 2012, 1, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Tu, K.; Gunraj, N.; Mamdani, M. Is Ramipril Really Better Than Other Angiotensin-Converting Enzyme Inhibitors After Acute Myocardial Infarction? Am. J. Cardiol. 2006, 98, 6–9. [Google Scholar] [CrossRef]
- Tu, K.; Mamdani, M.; Kopp, A.; Lee, D. Comparison of angiotensin-converting enzyme inhibitors in the treatment of congestive heart failure. Am. J. Cardiol. 2005, 95, 283–286. [Google Scholar] [CrossRef]
- Coca, A.; Sobrino, J.; Módol, J.; Soler, J.; Mínguez, A.; Plana, J.; De la Sierra, A. A multicenter, parallel comparative study of the antihypertensive efficacy of once-daily lisinopril vs enalapril with 24-h ambulatory blood pressure monitoring in essential hypertension. J. Hum. Hypertens. 1996, 10, 837–841. [Google Scholar] [CrossRef]
- Fagyas, M.; Úri, K.; Siket, I.M.; Daragó, A.; Boczán, J.; Bányai, E.; Édes, I.; Papp, Z.; Tóth, A. New Perspectives in the Renin-Angiotensin-Aldosterone System (RAAS) I: Endogenous Angiotensin Converting Enzyme (ACE) Inhibition. PLoS ONE 2014, 9, e87843. [Google Scholar] [CrossRef] [PubMed]
- Fagyas, M.; Úri, K.; Siket, I.M.; Daragó, A.; Boczán, J.; Bányai, E.; Édes, I.; Papp, Z.; Tóth, A. New Perspectives in the Renin-Angiotensin-Aldosterone System (RAAS) III: Endogenous Inhibition of Angiotensin Converting Enzyme (ACE) Provides Protection against Cardiovascular Diseases. PLoS ONE 2014, 9, e93719. [Google Scholar] [CrossRef] [PubMed]
- Fagyas, M.; Úri, K.; Siket, I.M.; Fülöp, G.Á.; Csató, V.; Daragó, A.; Boczán, J.; Bányai, E.; Szentkirályi, I.E.; Maros, T.M.; et al. New Perspectives in the Renin-Angiotensin-Aldosterone System (RAAS) II: Albumin Suppresses Angiotensin Converting Enzyme (ACE) Activity in Human. PLoS ONE 2014, 9, e87844. [Google Scholar] [CrossRef] [PubMed]
- Trbojevic-Stankovic, J.; Aleksic, M.; Odovic, J. Estimation of angiotensin-converting enzyme inhibitors protein binding degree using chromatographic hydrophobicity data. Srp. Arh. Za Celok. Lek. 2015, 143, 50–55. [Google Scholar] [CrossRef] [PubMed]
- White, C.M. Pharmacologic, pharmacokinetic, and therapeutic differences among ACE inhibitors. Pharmacotherapy 1998, 18, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Brunner, D.; Desponds, G.; Biollaz, J.; Keller, I.; Ferber, F.; Gavras, H.; Brunner, H.; Schelling, J. Effect of a new angiotensin converting enzyme inhibitor MK 421 and its lysine analogue on the components of the renin system in healthy subjects. Br. J. Clin. Pharmacol. 1981, 11, 461–467. [Google Scholar] [CrossRef]
- Bolzano, K.; Arriaga, J.; Bernal, R.; Bernardes, H.; Calderon, J.L.; Debruyn, J.; Dienstl, F.; Drayer, J.; Goodfriend, T.L.; Gross, W. The antihypertensive effect of lisinopril compared to atenolol in patients with mild to moderate hypertension. J. Cardiovasc. Pharmacol. 1987, 9 (Suppl. S3), S43–S47. [Google Scholar] [CrossRef] [PubMed]
- Gavras, H.; Biollaz, J.; Waeber, B.; Brunner, H.R.; Gavras, I.; Sackel, H.; Charocopos, F.; Davies, R.O. Effects of the oral angiotensin-converting enzyme inhibitor MK-421 in human hypertension. Clin. Sci. 1981, 61 (Suppl. S7), 281s–283s. [Google Scholar] [CrossRef]
- Pool, J.L.; Gennari, J.; Goldstein, R.; Kochar, M.S.; Lewin, A.J.; Maxwell, M.H.; McChesney, J.A.; Mehta, J.; Nash, D.T.; Nelson, E.B. Controlled multicenter study of the antihypertensive effects of lisinopril, hydrochlorothiazide, and lisinopril plus hydrochlorothiazide in the treatment of 394 patients with mild to moderate essential hypertension. J. Cardiovasc. Pharmacol. 1987, 9 (Suppl. S3), S36–S42. [Google Scholar] [CrossRef]
- Olvera Lopez, E.; Parmar, M.; Pendela, V.S.; Terrell, J.M. Lisinopril; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Faruqi, A.; Jain, A. Enalapril. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Baulmann, J.; Schillings, U.; Rickert, S.; Uen, S.; Düsing, R.; Illyes, M.; Cziraki, A.; Nickenig, G.; Mengden, T. A new oscillometric method for assessment of arterial stiffness: Comparison with tonometric and piezo-electronic methods. J. Hypertens. 2008, 26, 523–528. [Google Scholar] [CrossRef]
- Thijssen, D.H.J.; Black, M.A.; Pyke, K.E.; Padilla, J.; Atkinson, G.; Harris, R.A.; Parker, B.; Widlansky, M.E.; Tschakovsky, M.E.; Green, D.J. Assessment of flow-mediated dilation in humans: A methodological and physiological guideline. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H2–H12. [Google Scholar] [CrossRef]
- Hales, C.M.; Servais, J.; Martin, C.B.; Kohen, D. Prescription Drug Use Among Adults Aged 40–79 in the United States and Canada. NCHS Data Brief 2019, 347, 1–8. [Google Scholar]
- Danilov, S.M.; Tikhomirova, V.E.; Kryukova, O.V.; Balatsky, A.V.; Bulaeva, N.I.; Golukhova, E.Z.; Bokeria, L.A.; Samokhodskaya, L.M.; Kost, O.A. Conformational fingerprint of blood and tissue ACEs: Personalized approach. PLoS ONE 2018, 13, e0209861. [Google Scholar] [CrossRef] [PubMed]
- Nádasy, G.L.; Balla, A.; Szekeres, M. From Living in Saltwater to a Scarcity of Salt and Water, and Then an Overabundance of Salt—The Biological Roller Coaster to Which the Renin–Angiotensin System Has Had to Adapt: An Editorial. Biomedicines 2023, 11, 3004. [Google Scholar] [CrossRef] [PubMed]
- Bánhegyi, V.; Enyedi, A.; Fülöp, G.Á.; Oláh, A.; Siket, I.M.; Váradi, C.; Bottyán, K.; Lódi, M.; Csongrádi, A.; Umar, A.J.; et al. Human Tissue Angiotensin Converting Enzyme (ACE) Activity Is Regulated by Genetic Polymorphisms, Posttranslational Modifications, Endogenous Inhibitors and Secretion in the Serum, Lungs and Heart. Cells 2021, 10, 1708. [Google Scholar] [CrossRef]
- Weissgerber, T.L. Flow-Mediated Dilation: Can New Approaches Provide Greater Mechanistic Insight into Vascular Dysfunction in Preeclampsia and Other Diseases? Curr. Hypertens. Rep. 2014, 16, 487. [Google Scholar] [CrossRef]
- Townsend, R.R. Arterial Stiffness: Recommendations and Standardization. Pulse 2016, 4 (Suppl. S1), 3–7. [Google Scholar] [CrossRef] [PubMed]
- Martynowicz, H.; Gać, P.; Kornafel-Flak, O.; Filipów, S.; Łaczmański, Ł.; Sobieszczańska, M.; Mazur, G.; Porȩba, R. The Relationship Between the Effectiveness of Blood Pressure Control and Telomerase Reverse Transcriptase Concentration, Adipose Tissue Hormone Concentration and Endothelium Function in Hypertensives. Heart Lung Circ. 2020, 29, e200–e209. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Liu, S.; Zhao, K.-X.; Pu, J.; Xie, Y.-F.; Zhang, X.-W. Comparative Efficacy of Antihypertensive Agents in Flow-Mediated Vasodilation of Patients with Hypertension: Network Meta-Analysis of Randomized Controlled Trial. Int. J. Hypertens. 2022, 2022, 2432567. [Google Scholar] [CrossRef]
- Srivastava, P.; Badhwar, S.; Chandran, D.S.; Jaryal, A.K.; Jyotsna, V.P.; Deepak, K.K. Improvement in Angiotensin 1-7 precedes and correlates with improvement in Arterial stiffness and endothelial function following Renin-Angiotensin system inhibition in type 2 diabetes with newly diagnosed hypertension. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1253–1263. [Google Scholar] [CrossRef]
- Lv, Y.; Zhao, W.; Yu, L.; Yu, J.-G.; Zhao, L. Angiotensin-Converting Enzyme Gene D/I Polymorphism in Relation to Endothelial Function and Endothelial-Released Factors in Chinese Women. Front. Physiol. 2020, 11, 951. [Google Scholar] [CrossRef] [PubMed]
- Shahin, Y.; Khan, J.A.; Samuel, N.; Chetter, I. Angiotensin converting enzyme inhibitors effect on endothelial dysfunction: A meta-analysis of randomised controlled trials. Atherosclerosis 2011, 216, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Javanmard, S.H.; Sonbolestan, S.A.; Heshmat-Ghahdarijani, K.; Saadatnia, M.; Sonbolestan, S.A. Enalapril improves endothelial function in patients with migraine: A randomized, double-blind, placebo-controlled trial. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2011, 16, 26–32. [Google Scholar]
- Kovacs, I.; Toth, J.; Tarjan, J.; Koller, A. Correlation of flow mediated dilation with inflammatory markers in patients with impaired cardiac function. Beneficial effects of inhibition of ACE. Eur. J. Heart Fail. 2006, 8, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Eržen, B.; Gradišek, P.; Poredoš, P.; Šabovič, M. Treatment of Essential Arterial Hypertension with Enalapril Does Not Result in Normalization of Endothelial Dysfunction of the Conduit Arteries. Angiology 2006, 57, 187–192. [Google Scholar] [CrossRef]
- Diamant, M.; Vincent, H. Lisinopril versus enalapril: Evaluation of trough: Peak ratio by ambulatory blood pressure monitoring. J. Hum. Hypertens. 1999, 13, 405–412. [Google Scholar] [CrossRef]
- Arendse, L.B.; Danser, A.H.J.; Poglitsch, M.; Touyz, R.M.; Burnett, J.C.; Llorens-Cortes, C.; Ehlers, M.R.; Sturrock, E.D. Novel Therapeutic Approaches Targeting the Renin-Angiotensin System and Associated Peptides in Hypertension and Heart Failure. Pharmacol. Rev. 2019, 71, 539–570. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medical Drug | Enalapril | Lisinopril | ||
|---|---|---|---|---|
| Visit | First Visit | Follow Up | First Visit | Follow Up |
| Involved patients (n) | 43 | 28 | 44 | 30 |
| Age (years) | 45.7 ± 11.1 | N/A | 45.1 ± 11.3 | N/A |
| BMI (kg/m2) | 28.9 ± 5.6 | N/A | 28.3 ± 3.8 | N/A |
| Dose (mg/day) | 0 | 5.5 ± 2.3 | 0 | 8.3 ± 3.0 |
| Na+ (mM) | 140.6 ± 2.0 | 140.0 ± 2.5 | 140.3 ± 2.1 | 139.7 ± 2.5 |
| K+ (mM) | 4.3 ± 0.3 | 4.3 ± 0.3 | 4.2 ± 0.3 | 4.4 ± 0.4 |
| Glucose (mM) | 5.5 ± 1.0 | 5.2 ± 0.6 | 5.2 ± 1.3 | 5.2 ± 1.3 |
| HbA1C (%) | 5.3 ± 0.5 | 5.2 ± 0.3 | 5.4 ± 0.8 | 5.4 ± 0.8 |
| Urea (mmol/L) | 5.2 ± 1.4 | 5.4 ± 1.4 | 4.8 ± 1.2 | 5.0 ± 1.4 |
| Creatinine (mg/dL) | 75 ± 15 | 74 ± 15 | 78 ± 17 | 79 ± 16 |
| Trigliceride (mmol/L) | 1.5 ± 0.9 | 1.6 ± 1.5 | 2.1 ± 3.0 | 1.5 ± 0.8 |
| Cholesterol (mmol/L) | 5.1 ± 0.9 | 5.1 ± 0.9 | 5.2 ± 1.1 | 5.3 ± 1.1 |
| GOT (IU/L) | 25.2 ± 11.8 | 26.4 ± 9.6 | 22.8 ± 7.5 | 23.1 ± 7.2 |
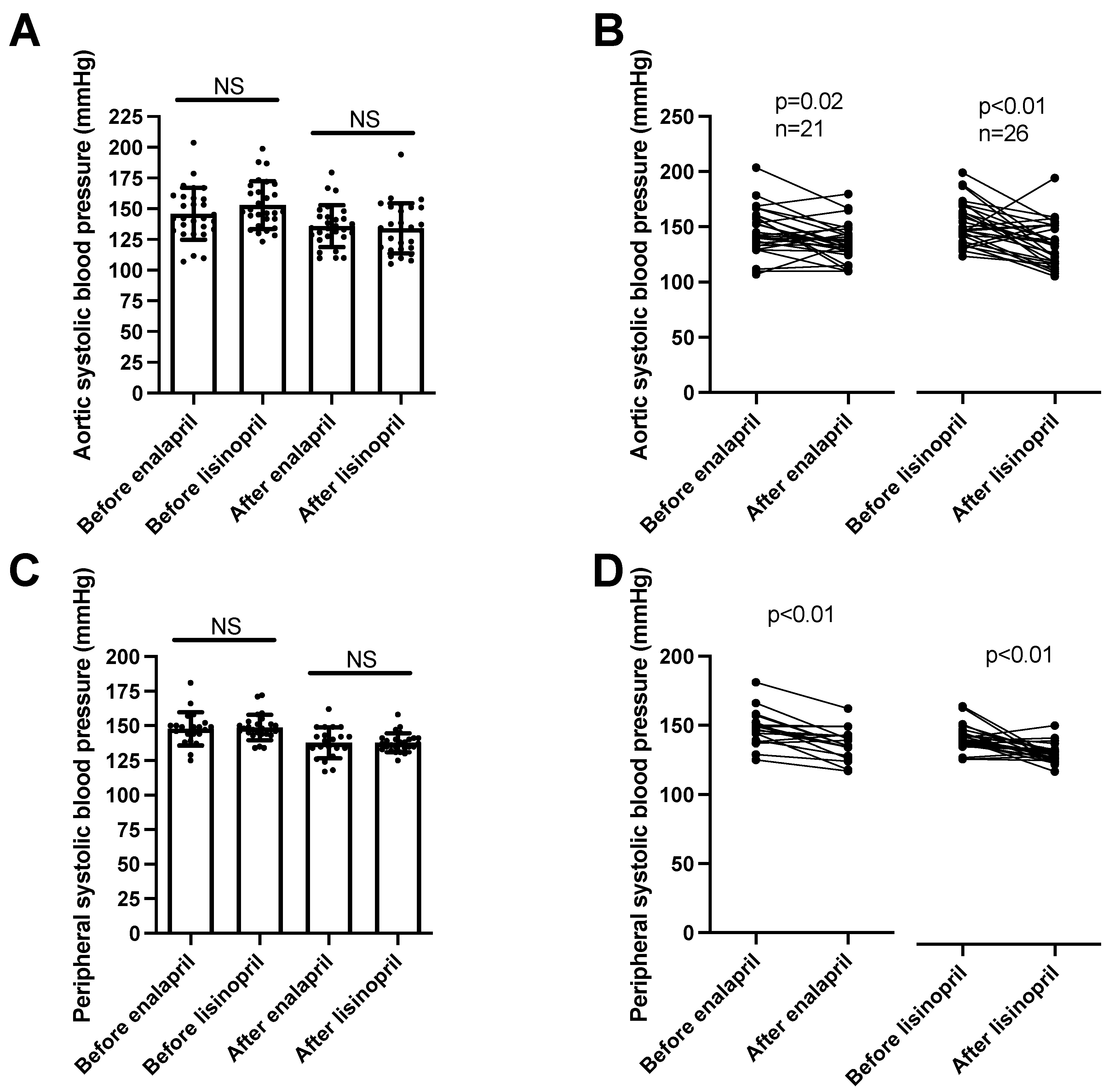
| Systolic blood pressure (active period, mmHg, SD) | 147 ± 11 | 138 ± 11 | 148 ± 11 | 139 ± 8 |
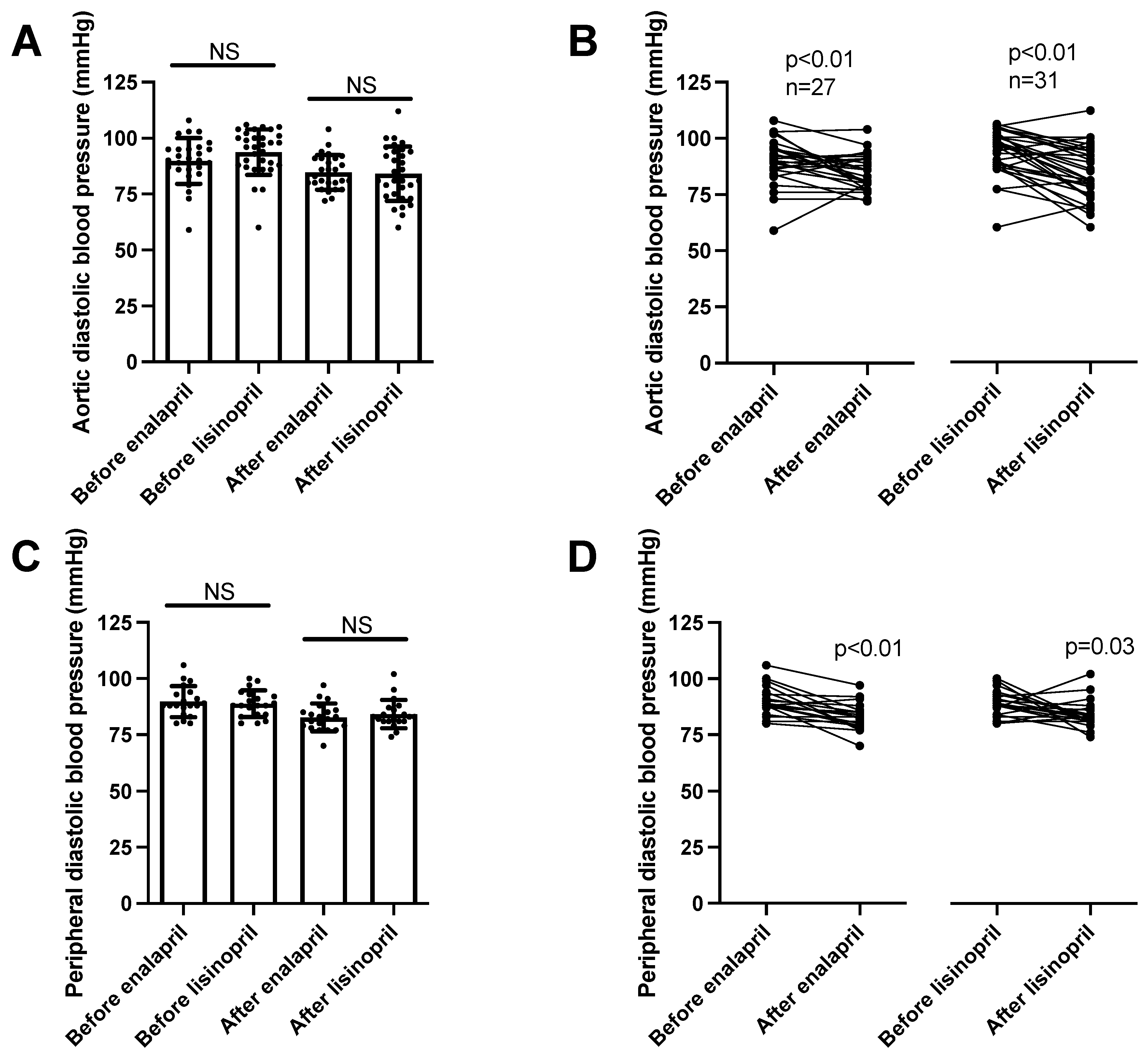
| Diastolic blood pressure (active period, mmHg, SD) | 90 ± 7 | 83 ± 7 | 90 ± 9 | 84 ± 6 |
| Systolic blood pressure (night period, mmHg, SD) | 128 ± 13 | 125 ± 14 | 132 ± 23 | 118 ± 27 |
| Diastolic blood pressure (night period, mmHg, SD) | 76 ± 8 | 75 ± 8 | 80 ± 10 | 70 ± 17 |
| FMD (%, SD) | 7.4 ± 3.1 | 8.8 ± 3.4 | 8.7 ± 4.2 | 7.8 ± 2.4 |
| IMT (mm, SD) | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.6 ± 0.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy, A.; Májer, R.; Boczán, J.; Sipka, S., Jr.; Szabó, A.; Enyedi, E.E.; Tatai, O.; Fagyas, M.; Papp, Z.; Csiba, L.; et al. Enalapril Is Superior to Lisinopril in Improving Endothelial Function without a Difference in Blood–Pressure–Lowering Effects in Newly Diagnosed Hypertensives. Biomedicines 2023, 11, 3323. https://doi.org/10.3390/biomedicines11123323
Nagy A, Májer R, Boczán J, Sipka S Jr., Szabó A, Enyedi EE, Tatai O, Fagyas M, Papp Z, Csiba L, et al. Enalapril Is Superior to Lisinopril in Improving Endothelial Function without a Difference in Blood–Pressure–Lowering Effects in Newly Diagnosed Hypertensives. Biomedicines. 2023; 11(12):3323. https://doi.org/10.3390/biomedicines11123323
Chicago/Turabian StyleNagy, Attila, Réka Májer, Judit Boczán, Sándor Sipka, Jr., Attila Szabó, Enikő Edit Enyedi, Ottó Tatai, Miklós Fagyas, Zoltán Papp, László Csiba, and et al. 2023. "Enalapril Is Superior to Lisinopril in Improving Endothelial Function without a Difference in Blood–Pressure–Lowering Effects in Newly Diagnosed Hypertensives" Biomedicines 11, no. 12: 3323. https://doi.org/10.3390/biomedicines11123323