
Detection Rate and Clinical Impact of PET/CT with 18F-FACBC in Patients with Biochemical Recurrence of Prostate Cancer: A Retrospective Bicentric Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
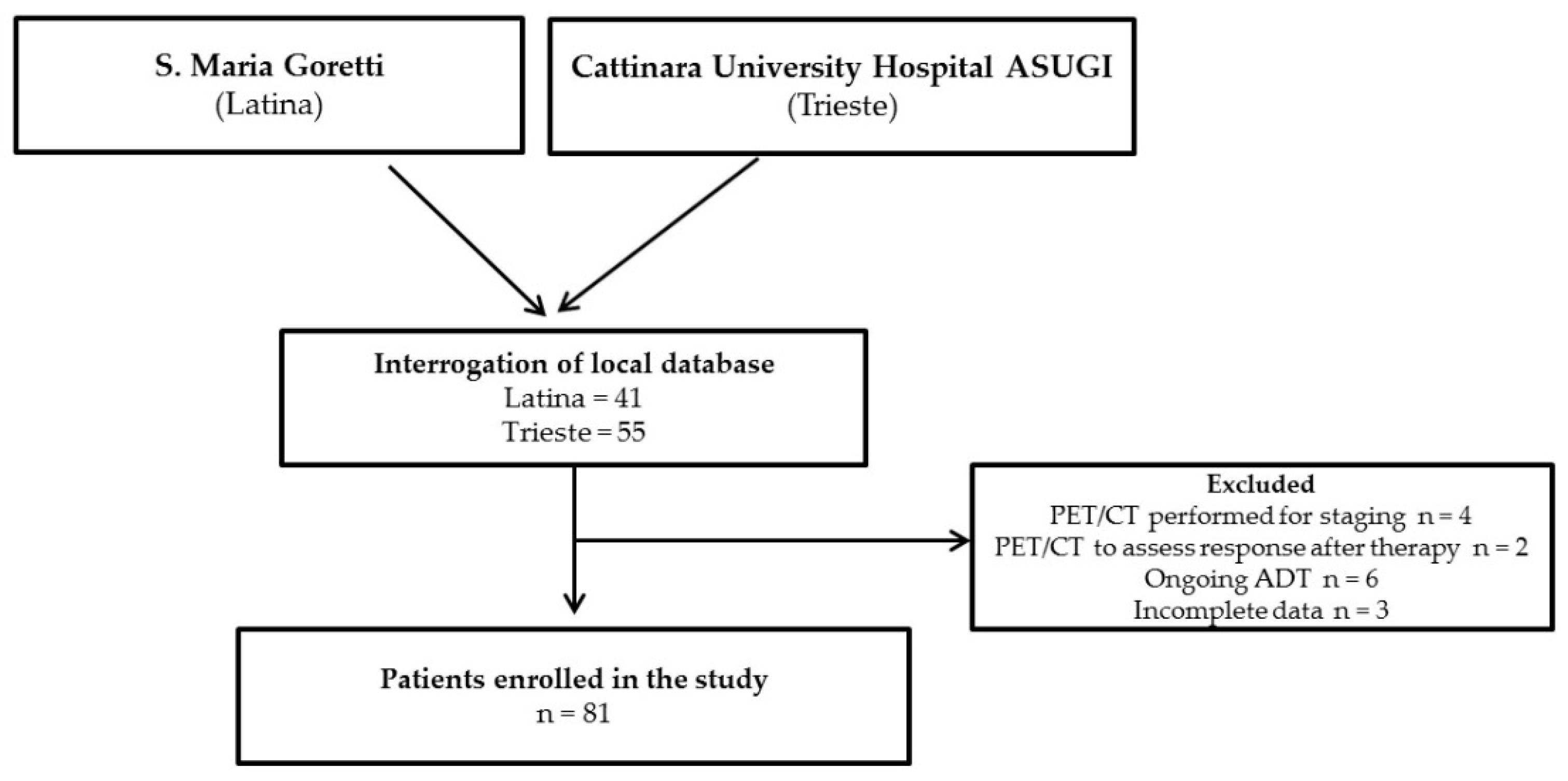
2.1. Study Design
2.2. 18F-FACBC PET/CT
2.3. Statistical Analysis
3. Results
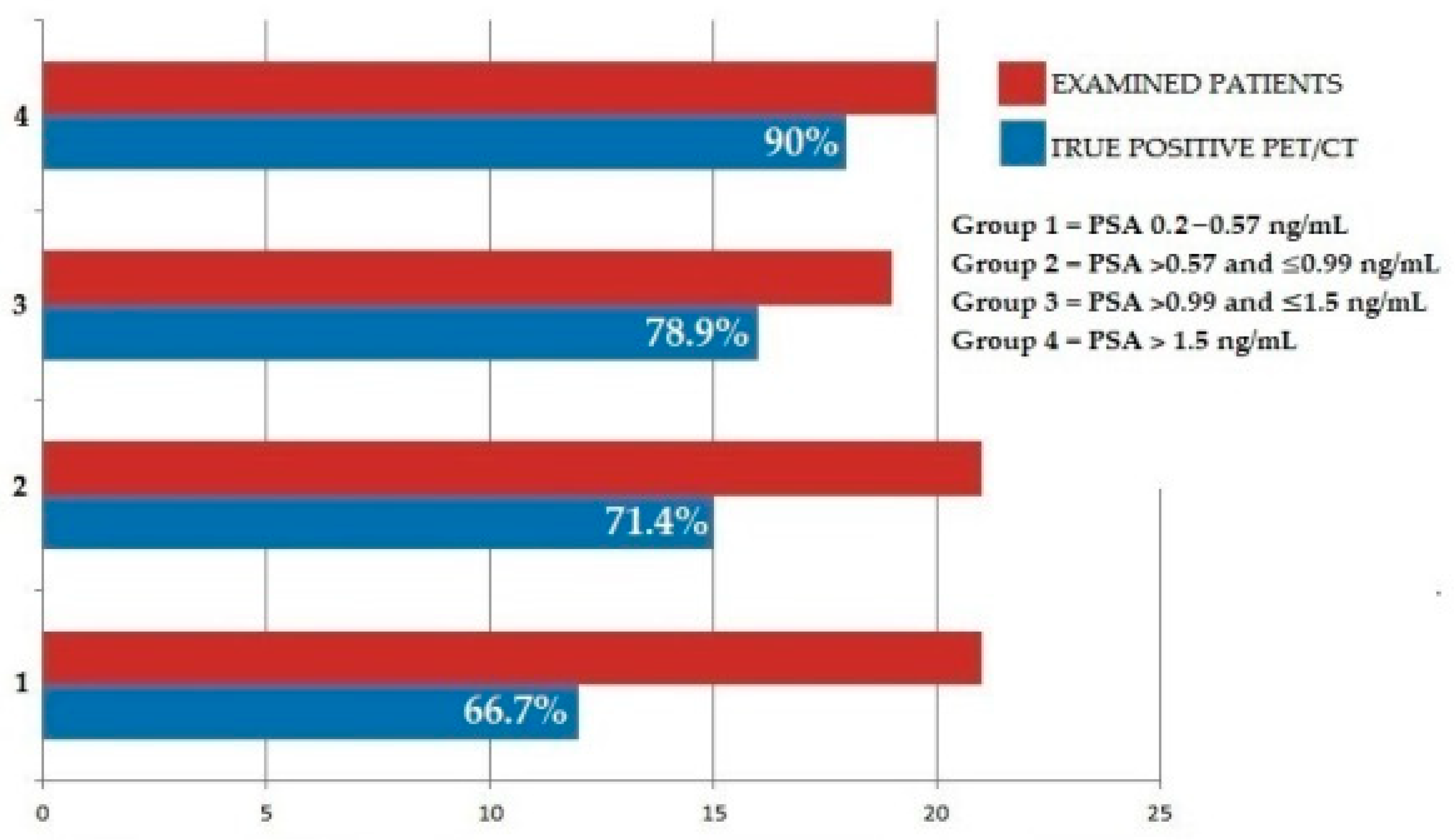
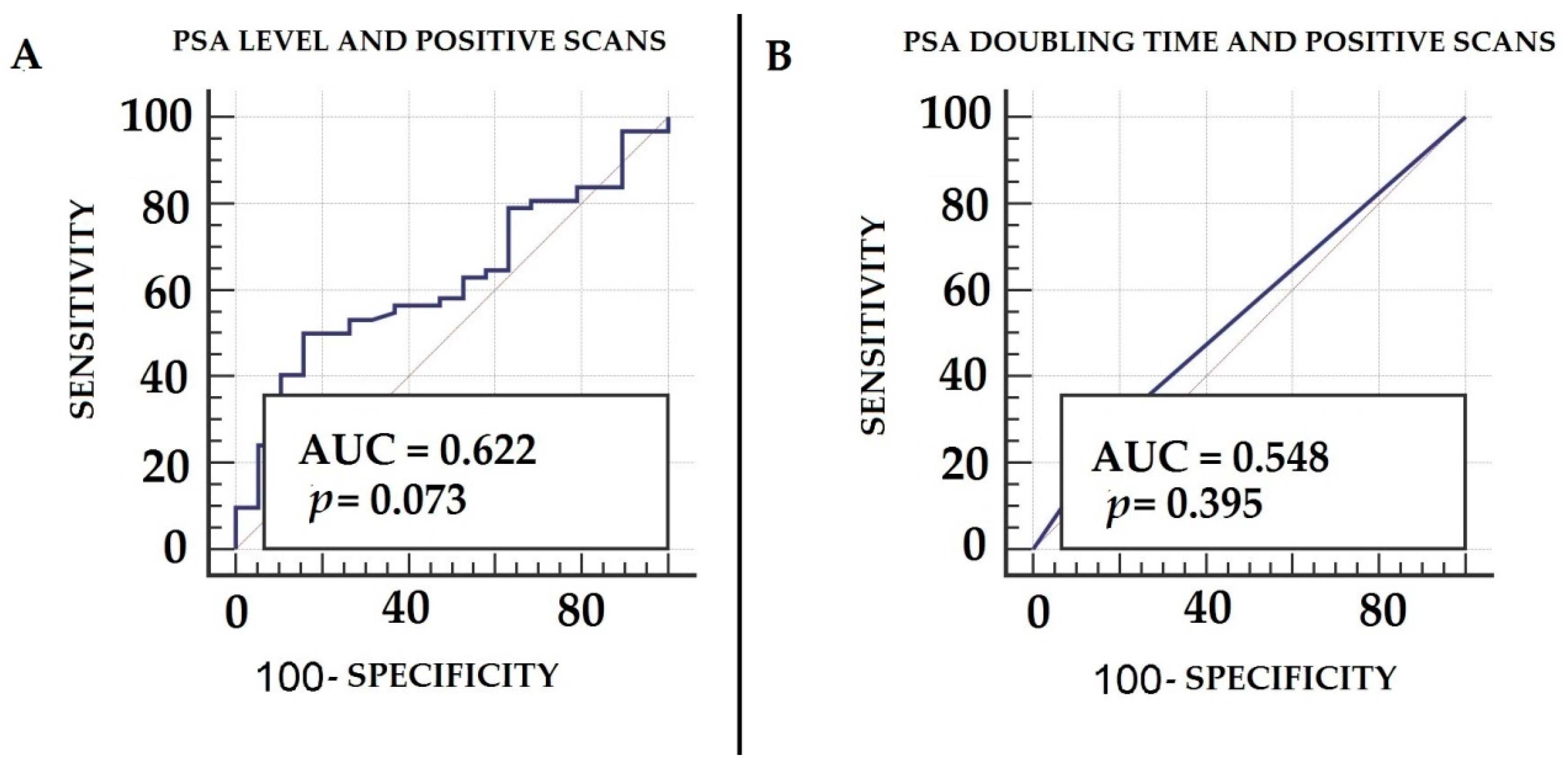
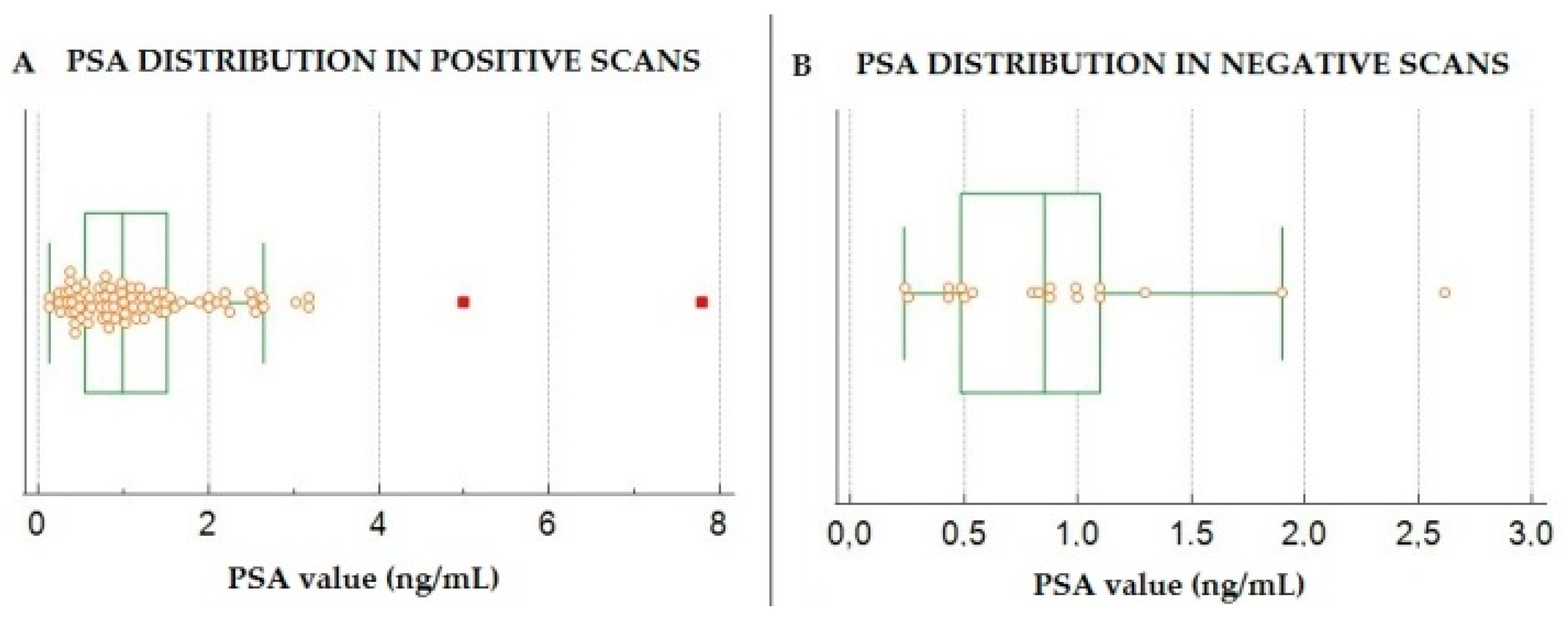
3.1. Diagnostic Performance of 18F-FACBC PET/CT in Enrolled Patients
3.2. Classification of 18F-FACBC PET/CT’s Results According to PROMISE
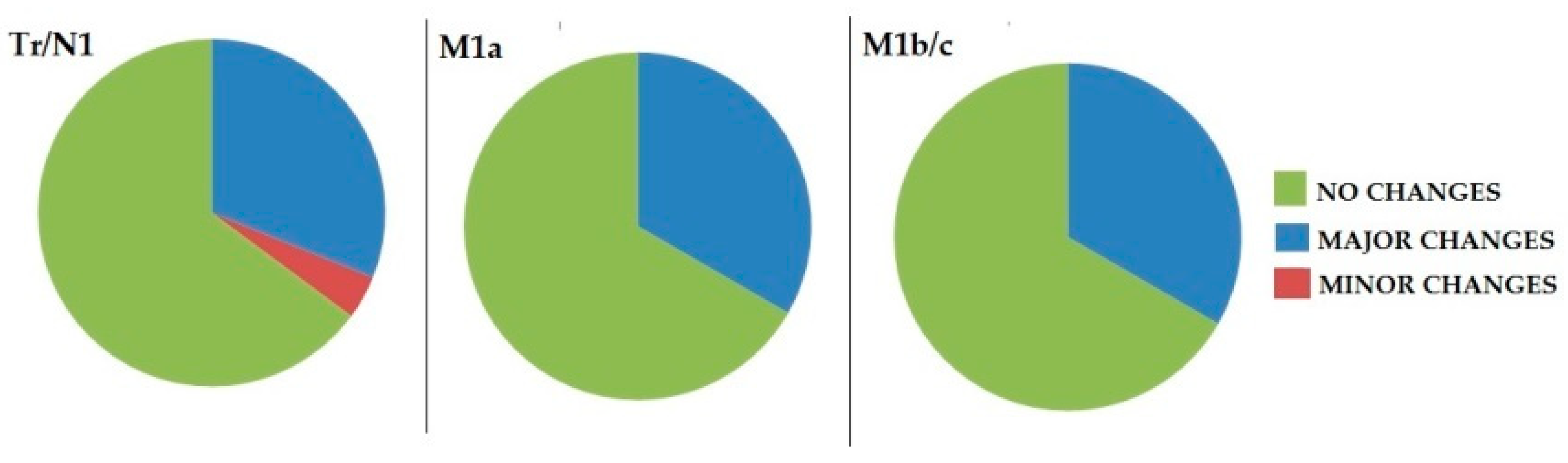
3.3. Impact of 18F-FACBC PET/CT on Clinical Management
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Tourinho-Barbosa, R.; Srougi, V.; Nunes-Silva, I.; Baghdadi, M.; Rembeyo, G.; Eiffel, S.S.; Barret, E.; Rozet, F.; Galiano, M.; Cathelineau, X.; et al. Biochemical Recurrence after Radical Prostatectomy: What Does It Mean? Int. Braz. J. Urol. 2018, 44, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, A.J.; Kattan, M.W.; Eastham, J.A.; Dotan, Z.A.; Bianco, F.J.; Lilja, H.; Scardino, P.T. Defining Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy: A Proposal for a Standardized Definition. J. Clin. Oncol. 2006, 24, 3973–3978. [Google Scholar] [CrossRef] [PubMed]
- Matteucci, F.; Paganelli, G.; Martinelli, G.; Cerchione, C. PET/CT in Multiple Myeloma: Beyond FDG. Front. Oncol. 2021, 10, 622501. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Schillaci, O.; Bagni, O. Recent Advances in PET Probes for Hepatocellular Carcinoma Characterization. Expert Rev. Med. Devices 2019, 16, 341–350. [Google Scholar] [CrossRef]
- Castellucci, P.; Fuccio, C.; Rubello, D.; Schiavina, R.; Santi, I.; Nanni, C.; Allegri, V.; Montini, G.C.; Ambrosini, V.; Boschi, S.; et al. Is There a Role for 11C-Choline PET/CT in the Early Detection of Metastatic Disease in Surgically Treated Prostate Cancer Patients with a Mild PSA Increase <1.5 Ng/ML? Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Crawford, E.D.; Koo, P.J.; Shore, N.; Slovin, S.F.; Concepcion, R.S.; Freedland, S.J.; Gomella, L.G.; Karsh, L.; Keane, T.E.; Maroni, P.; et al. A Clinician’s Guide to Next Generation Imaging in Patients With Advanced Prostate Cancer (RADAR III). J. Urol. 2019, 201, 682–692. [Google Scholar] [CrossRef]
- García Garzón, J.R.; de Arcocha Torres, M.; Delgado-Bolton, R.; Ceci, F.; Alvarez Ruiz, S.; Orcajo Rincón, J.; Caresia Aróztegui, A.P.; García Velloso, M.J.; García Vicente, A.M. La PET/TC con 68Ga-PSMA en el cáncer de próstata. Rev. Española Med. Nucl. Imagen Mol. 2018, 37, 130–138. [Google Scholar] [CrossRef]
- Liu, A.; Han, J.; Nakano, A.; Konno, H.; Moriwaki, H.; Abe, H.; Izawa, K.; Soloshonok, V.A. New Pharmaceuticals Approved by FDA in 2020: Small-molecule Drugs Derived from Amino Acids and Related Compounds. Chirality 2021, 34, 86–103. [Google Scholar] [CrossRef]
- Uprimny, C.; Kroiss, A.S.; Decristoforo, C.; Fritz, J.; Warwitz, B.; Scarpa, L.; Roig, L.G.; Kendler, D.; von Guggenberg, E.; Bektic, J.; et al. Early Dynamic Imaging in 68Ga- PSMA-11 PET/CT Allows Discrimination of Urinary Bladder Activity and Prostate Cancer Lesions. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 765–775. [Google Scholar] [CrossRef]
- Biscontini, G.; Romagnolo, C.; Cottignoli, C.; Palucci, A.; Fringuelli, F.M.; Caldarella, C.; Ceci, F.; Burroni, L. 18F-Fluciclovine Positron Emission Tomography in Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis. Diagnostics 2021, 11, 304. [Google Scholar] [CrossRef]
- Wang, Y.; Chow, D.Z.; Ebert, E.; Tajmir, S.; Scott, J.A.; Palmer, E.L. Utility of 18F-Fluciclovine PET/CT for Detecting Prostate Cancer Recurrence in Patients With Low (<1 Ng/ML) or Very Low (<0.3 Ng/ML) Prostate-Specific Antigen Levels. Am. J. Roentgenol. 2020, 215, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.; Abiodun-Ojo, O.A.; Jani, A.B.; Schuster, D.M. Clinical Utility of 18F-Fluciclovine PET/CT in Recurrent Prostate Cancer with Very Low (≤0.3 Ng/ML) Prostate-Specific Antigen Levels. Am. J. Nucl. Med. Mol. Imaging 2021, 11, 406–414. [Google Scholar] [PubMed]
- Abiodun-Ojo, O.A.; Jani, A.B.; Akintayo, A.A.; Akin-Akintayo, O.O.; Odewole, O.A.; Tade, F.I.; Joshi, S.S.; Master, V.A.; Fielder, B.; Halkar, R.K.; et al. Salvage Radiotherapy Management Decisions in Postprostatectomy Patients with Recurrent Prostate Cancer Based on 18F-Fluciclovine PET/CT Guidance. J. Nucl. Med. 2021, 62, 1089–1096. [Google Scholar] [CrossRef]
- Roach, M.; Hanks, G.; Thames, H.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining Biochemical Failure Following Radiotherapy with or without Hormonal Therapy in Men with Clinically Localized Prostate Cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Biol. 2006, 65, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Nanni, C.; Zanoni, L.; Bach-Gansmo, T.; Minn, H.; Willoch, F.; Bogsrud, T.V.; Edward, E.P.; Savir-Baruch, B.; Teoh, E.; Ingram, F.; et al. [18F]Fluciclovine PET/CT: Joint EANM and SNMMI Procedure Guideline for Prostate Cancer Imaging—Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed MiTNM Classification for the Interpretation of PSMA-Ligand PET/CT. J. Nucl. Med. 2018, 59, 469–478. [Google Scholar] [CrossRef] [Green Version]
- Laudicella, R.; Albano, D.; Alongi, P.; Argiroffi, G.; Bauckneht, M.; Baldari, S.; Bertagna, F.; Boero, M.; De Vincentis, G.; Sole, A.D.; et al. 18F-Facbc in Prostate Cancer: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarsbrook, A.F.; Bottomley, D.; Teoh, E.J.; Bradley, K.M.; Payne, H.; Afaq, A.; Bomanji, J.; van As, N.; Chua, S.; Hoskin, P.; et al. Effect of 18F-Fluciclovine Positron Emission Tomography on the Management of Patients With Recurrence of Prostate Cancer: Results From the FALCON Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 316–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andriole, G.L.; Kostakoglu, L.; Chau, A.; Duan, F.; Mahmood, U.; Mankoff, D.A.; Schuster, D.M.; Siegel, B.A.; Adler, L.P.; Belkoff, L.H.; et al. The Impact of Positron Emission Tomography with 18F-Fluciclovine on the Treatment of Biochemical Recurrence of Prostate Cancer: Results from the LOCATE Trial. J. Urol. 2019, 201, 322–331. [Google Scholar] [CrossRef]
- Bach-Gansmo, T.; Nanni, C.; Nieh, P.T.; Zanoni, L.; Bogsrud, T.V.; Sletten, H.; Korsan, K.A.; Kieboom, J.; Tade, F.I.; Odewole, O.; et al. Multisite Experience of the Safety, Detection Rate and Diagnostic Performance of Fluciclovine (18F) Positron Emission Tomography/Computerized Tomography Imaging in the Staging of Biochemically Recurrent Prostate Cancer. J. Urol. 2017, 197, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, J.M.; Martin, C.R.; Dechet, C.; Morton, K.; Evans, D.; Ambrose, J.; Maughan, B.L.; O’Neil, B.; Lowrance, W. 18F-Fluciclovine PET CT Detection of Biochemical Recurrent Prostate Cancer at Specific PSA Thresholds after Definitive Treatment. Oncol. Semin. Orig. 2020, 38, 636.e1–636.e6. [Google Scholar] [CrossRef]
- Marcus, C.; Butler, P.; Bagrodia, A.; Cole, S.; Subramaniam, R.M. Fluorine-18-Labeled Fluciclovine PET/CT in Primary and Biochemical Recurrent Prostate Cancer Management. Am. J. Roentgenol. 2020, 215, 267–276. [Google Scholar] [CrossRef]
- Parent, E.E. Letter Regarding 18F-Fluciclovine PET/CT Performance in Biochemical Recurrence of Prostate Cancer: A Systematic Review. Prostate Cancer Prostatic Dis. 2021, 24, 944–945. [Google Scholar] [CrossRef]
- Knipper, S.; Ascalone, L.; Ziegler, B.; Hohenhorst, J.L.; Simon, R.; Berliner, C.; van Leeuwen, F.W.B.; van der Poel, H.; Giesel, F.; Graefen, M.; et al. Salvage Surgery in Patients with Local Recurrence After Radical Prostatectomy. Eur. Urol. 2021, 79, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Alberts, I.; Hünermund, J.-N.; Sachpekidis, C.; Mingels, C.; Fech, V.; Bohn, K.P.; Rominger, A.; Afshar-Oromieh, A. The Influence of Digital PET/CT on Diagnostic Certainty and Interrater Reliability in [68Ga]Ga-PSMA-11 PET/CT for Recurrent Prostate Cancer. Eur. Radiol. 2021, 31, 8030–8039. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Schillaci, O. Digital PET and Detection of Recurrent Prostate Cancer: What Have We Gained, and What Is Still Missing? Expert Rev. Med. Devices 2021, 18, 1107–1110. [Google Scholar] [CrossRef] [PubMed]
- Fendler, W.P.; Ferdinandus, J.; Czernin, J.; Eiber, M.; Flavell, R.R.; Behr, S.C.; Wu, I.-W.K.; Lawhn-Heath, C.; Pampaloni, M.H.; Reiter, R.E.; et al. Impact of 68Ga-PSMA-11 PET on the Management of Recurrent Prostate Cancer in a Prospective Single-Arm Clinical Trial. J. Nucl. Med. 2020, 61, 1793–1799. [Google Scholar] [CrossRef] [PubMed]
- Salavati, A.; Gencturk, M.; Koksel, Y.; Schik, A.N.; Carroll, P.R.; Feng, F.Y.; Rowe, S.P.; Lawhn-Heath, C.; Hope, T.A.; Froelich, J.W. A Bicentric Retrospective Analysis of Clinical Utility of 18F-Fluciclovine PET in Biochemically Recurrent Prostate Cancer Following Primary Radiation Therapy: Is It Helpful in Patients with a PSA Rise Less than the Phoenix Criteria? Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4463–4471. [Google Scholar] [CrossRef]
- Alberts, I.; Niklas-Hünermund, J.; Sachpekidis, C.; Zacho, H.D.; Mingels, C.; Dijkstra, L.; Bohn, K.P.; Läppchen, T.; Gourni, E.; Rominger, A.; et al. Combination of Forced Diuresis with Additional Late Imaging in 68Ga-PSMA-11 PET/CT: Effects on Lesion Visibility and Radiotracer Uptake. J. Nucl. Med. 2021, 62, 1252–1257. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Shen, G.; Huang, M.; Tian, R. The Diagnostic Role of 18F-Choline, 18F-Fluciclovine and 18F-PSMA PET/CT in the Detection of Prostate Cancer With Biochemical Recurrence: A Meta-Analysis. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | - | |
| median | 74 | |
| mean ± SD | 73.2 ± 6.9 | |
| Initial Therapy | n | % |
| Surgery only | 45 | 55.5 |
| Radiation therapy only | 20 | 24.7 |
| Surgery + radiation therapy | 14 | 17.3 |
| Brachytherapy | 2 | 2.4 |
| ISUP | n | % |
| ISUP 1 | 8 | 9.9 |
| ISUP 2 | 8 | 9.9 |
| ISUP 3 | 27 | 33.3 |
| ISUP 4 | 33 | 40.7 |
| ISUP 5 | 5 | 6.2 |
| Time from Diagnosis to Relapse (y) | ||
| median | 7 | |
| mean ± SD | 7 ± 4.3 | |
| PSA prior to PET/CT | ||
| median | 0.99 | |
| mean ± SD | 1.27 ± 1.1 | |
| PSA doubling time | n | % |
| <6 months | 23 | 28.4 |
| >6 months | 58 | 71.6 |
| Final Classification | TNM |
|---|---|
| Local relapse (Tr/N1) n = 48 (59.3%) | TrN0M0, n = 25 (30.8%) |
| T0N1M0, n = 16 (19.8%) | |
| TrN1M0, n = 7 (8.7%) | |
| Distant Lymph nodes (M1a) n = 8 (9.9%) | T0N0M1a, n = 3 (3.8%) |
| TrN0M1a, n = 1 (1.2%) | |
| T0N1M1a, n = 3 (3.8%) | |
| TrN1M1a, n = 1 (1.2%) | |
| Bone/visceral metastases (M1b/C) n = 6 (7.4%) | TrN0M1b, n = 4 (4.9%) |
| T0N0M1b, n = 1 (1.2%) | |
| M1c, n= 1 (1.2%) | |
| Negative n = 19 (23.4%) | T0N0M0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filippi, L.; Bagni, O.; Crisafulli, C.; Cerio, I.; Brunotti, G.; Chiaravalloti, A.; Schillaci, O.; Dore, F. Detection Rate and Clinical Impact of PET/CT with 18F-FACBC in Patients with Biochemical Recurrence of Prostate Cancer: A Retrospective Bicentric Study. Biomedicines 2022, 10, 177. https://doi.org/10.3390/biomedicines10010177
Filippi L, Bagni O, Crisafulli C, Cerio I, Brunotti G, Chiaravalloti A, Schillaci O, Dore F. Detection Rate and Clinical Impact of PET/CT with 18F-FACBC in Patients with Biochemical Recurrence of Prostate Cancer: A Retrospective Bicentric Study. Biomedicines. 2022; 10(1):177. https://doi.org/10.3390/biomedicines10010177
Chicago/Turabian StyleFilippi, Luca, Oreste Bagni, Carmelo Crisafulli, Ivan Cerio, Gabriele Brunotti, Agostino Chiaravalloti, Orazio Schillaci, and Franca Dore. 2022. "Detection Rate and Clinical Impact of PET/CT with 18F-FACBC in Patients with Biochemical Recurrence of Prostate Cancer: A Retrospective Bicentric Study" Biomedicines 10, no. 1: 177. https://doi.org/10.3390/biomedicines10010177