
Divergent Survival Outcomes Associated with Elevated Branched-Chain Amino Acid Levels among Older Adults with or without Hypertension and Diabetes: A Validated, Prospective, Longitudinal Follow-Up Study

 , , , , , , , , , and
, , , , , , , , , and 
Abstract
:1. Introduction
2. Methods
2.1. Study Cohort
2.2. Definitions of Hypertension, Diabetes Mellitus, Frailty, and Estimated Glomerular Filtration Rate
2.3. Phlebotomy, Serum Processing, and Sample Storage
2.4. Quantification of Serum Concentration of Branched-Chain Amino Acids and Creatinine
2.5. Ascertainment of Deaths
2.6. Data and Statistical Analysis
3. Results
3.1. Baseline Characteristics of Longitudinal Study Cohort
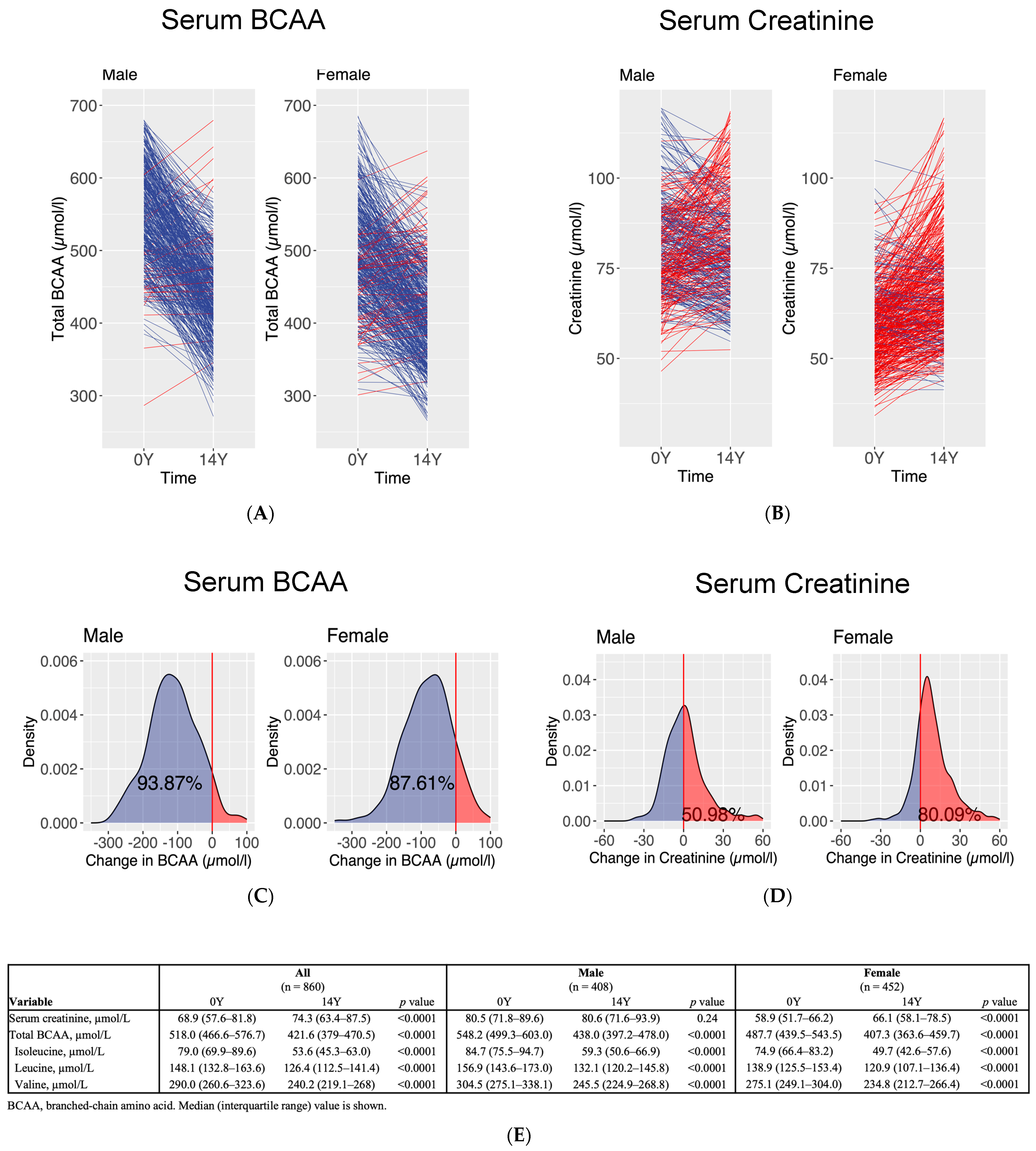
3.2. Interval Measurements of Serum Concentration of Branched-Chain Amino Acids and Creatinine at Baseline and at 14 Years
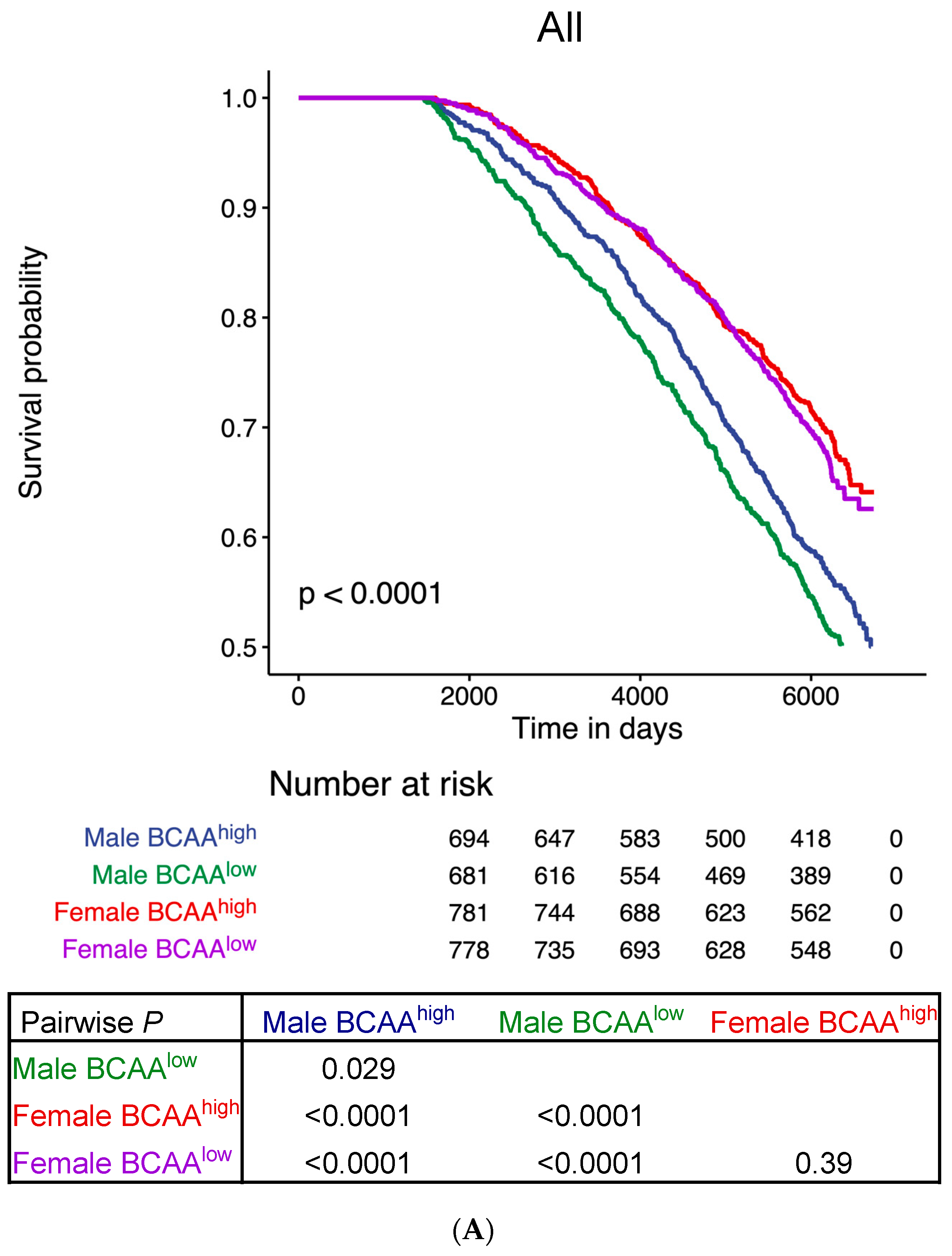
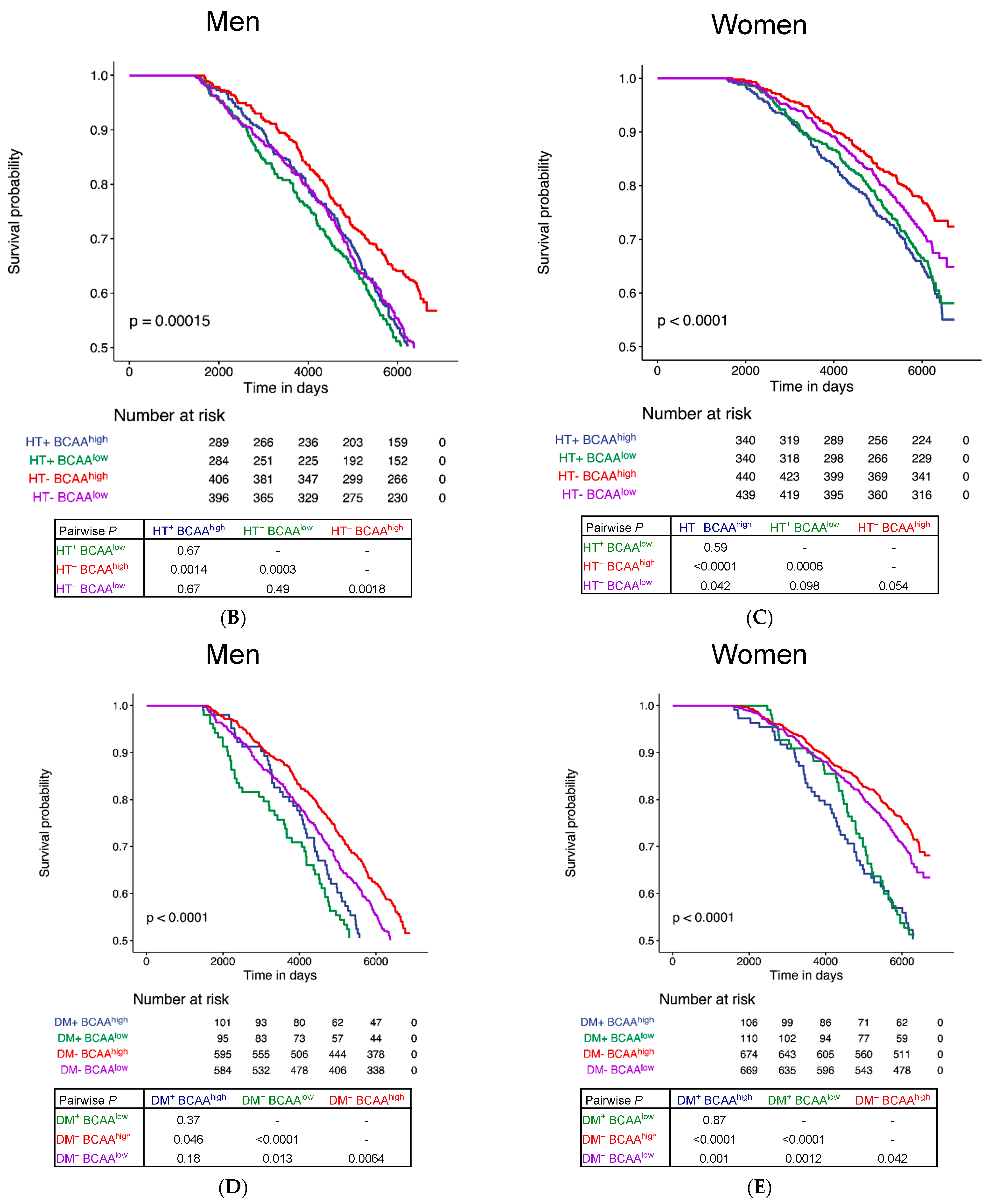
3.3. Survival Analysis during a Median Follow-Up of 17 Years
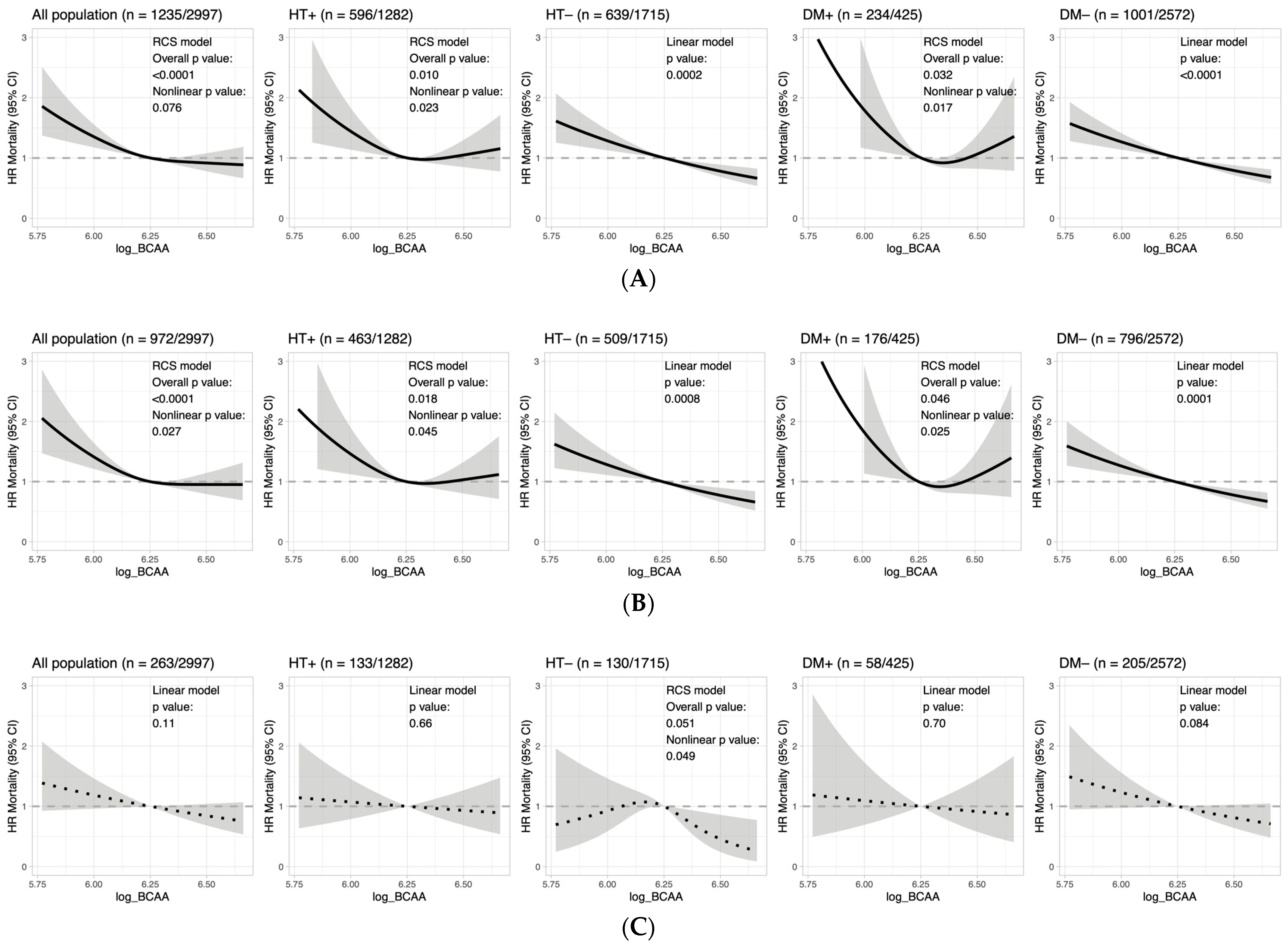
3.4. Mortality Hazard and Nonlinearity of BCAA Effects in Cardiometabolic Disease
3.5. Serum BCAA Levels at Baseline and Year 14 Can Predict Future Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Available online: https://www.un.org/en/global-issues/ageing (accessed on 29 April 2023).
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222, Erratum in Lancet 2020, 396, 1562. [Google Scholar] [CrossRef]
- Hambleton, I.R.; Caixeta, R.; Jeyaseelan, S.M.; Luciani, S.; Hennis, A.J.M. The rising burden of non-communicable diseases in the Americas and the impact of population aging: A secondary analysis of available data. Lancet Reg. Health Am. 2023, 21, 100483. [Google Scholar] [CrossRef]
- Ford, E.S. Trends in mortality from all causes and cardiovascular disease among hypertensive and nonhypertensive adults in the United States. Circulation 2011, 123, 1737–1744. [Google Scholar] [CrossRef]
- Rapsomaniki, E.; Timmis, A.; George, J.; Pujades-Rodriguez, M.; Shah, A.D.; Denaxas, S.; White, I.R.; Caulfield, M.J.; Deanfield, J.E.; Smeeth, L.; et al. Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people. Lancet 2014, 383, 1899–1911. [Google Scholar] [CrossRef]
- Bozkurt, B.; Aguilar, D.; Deswal, A.; Dunbar, S.B.; Francis, G.S.; Horwich, T.; Jessup, M.; Kosiborod, M.; Pritchett, A.M.; Ramasubbu, K.; et al. Contributory Risk and Management of Comorbidities of Hypertension, Obesity, Diabetes Mellitus, Hyperlipidemia, and Metabolic Syndrome in Chronic Heart Failure: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e535–e578. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2021, 183, 109119. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- McGarrah, R.W.; White, P.J. Branched-chain amino acids in cardiovascular disease. Nat. Rev. Cardiol. 2023, 20, 77–89. [Google Scholar] [CrossRef]
- Lynch, C.J.; Adams, S.H. Branched-chain amino acids in metabolic signalling and insulin resistance. Nat. Rev. Endocrinol. 2014, 10, 723–736. [Google Scholar] [CrossRef]
- Zhang, Z.Y.; Monleon, D.; Verhamme, P.; Staessen, J.A. Branched-Chain Amino Acids as Critical Switches in Health and Disease. Hypertension 2018, 72, 1012–1022. [Google Scholar] [CrossRef]
- Flores-Guerrero, J.L.; Groothof, D.; Connelly, M.A.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F. Concentration of Branched-Chain Amino Acids Is a Strong Risk Marker for Incident Hypertension. Hypertension 2019, 74, 1428–1435. [Google Scholar] [CrossRef]
- Sun, H.; Olson, K.C.; Gao, C.; Prosdocimo, D.A.; Zhou, M.; Wang, Z.; Jeyaraj, D.; Youn, J.Y.; Ren, S.; Liu, Y.; et al. Catabolic Defect of Branched-Chain Amino Acids Promotes Heart Failure. Circulation 2016, 133, 2038–2049. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.L.; Lau, E.S.H.; Fung, E.; Lee, H.M.; Ma, R.C.W.; Tam, C.H.T.; Wong, W.K.K.; Ng, A.C.W.; Chow, E.; Luk, A.O.Y.; et al. Circulating branched-chain amino acids and incident heart failure in type 2 diabetes: The Hong Kong Diabetes Register. Diabetes Metab. Res. Rev. 2020, 36, e3253. [Google Scholar] [CrossRef]
- Du, X.; Li, Y.; Wang, Y.; You, H.; Hui, P.; Zheng, Y.; Du, J. Increased branched-chain amino acid levels are associated with long-term adverse cardiovascular events in patients with STEMI and acute heart failure. Life Sci. 2018, 209, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; You, H.; Li, Y.; Wang, Y.; Hui, P.; Qiao, B.; Lu, J.; Zhang, W.; Zhou, S.; Zheng, Y.; et al. Relationships between circulating branched chain amino acid concentrations and risk of adverse cardiovascular events in patients with STEMI treated with PCI. Sci. Rep. 2018, 8, 15809. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Lawler, P.R.; Harada, P.H.; Demler, O.V.; Ridker, P.M.; Manson, J.E.; Cheng, S.; Mora, S. Circulating Branched-Chain Amino Acids and Incident Cardiovascular Disease in a Prospective Cohort of US Women. Circ. Genom. Precis. Med. 2018, 11, e002157. [Google Scholar] [CrossRef]
- Solon-Biet, S.M.; Cogger, V.C.; Pulpitel, T.; Wahl, D.; Clark, X.; Bagley, E.; Gregoriou, G.C.; Senior, A.M.; Wang, Q.P.; Brandon, A.E.; et al. Branched chain amino acids impact health and lifespan indirectly via amino acid balance and appetite control. Nat. Metab. 2019, 1, 532–545. [Google Scholar] [CrossRef]
- Zhang, Z.Y.; Marrachelli, V.G.; Yang, W.Y.; Trenson, S.; Huang, Q.F.; Wei, F.F.; Thijs, L.; Van Keer, J.; Monleon, D.; Verhamme, P.; et al. Diastolic left ventricular function in relation to circulating metabolic biomarkers in a population study. Eur. J. Prev. Cardiol. 2019, 26, 22–32. [Google Scholar] [CrossRef]
- Tanada, Y.; Shioi, T.; Kato, T.; Kawamoto, A.; Okuda, J.; Kimura, T. Branched-chain amino acids ameliorate heart failure with cardiac cachexia in rats. Life Sci. 2015, 137, 20–27. [Google Scholar] [CrossRef]
- D’Antona, G.; Ragni, M.; Cardile, A.; Tedesco, L.; Dossena, M.; Bruttini, F.; Caliaro, F.; Corsetti, G.; Bottinelli, R.; Carruba, M.O.; et al. Branched-chain amino acid supplementation promotes survival and supports cardiac and skeletal muscle mitochondrial biogenesis in middle-aged mice. Cell Metab. 2010, 12, 362–372. [Google Scholar] [CrossRef]
- Cheng, S.; Rhee, E.P.; Larson, M.G.; Lewis, G.D.; McCabe, E.L.; Shen, D.; Palma, M.J.; Roberts, L.D.; Dejam, A.; Souza, A.L.; et al. Metabolite profiling identifies pathways associated with metabolic risk in humans. Circulation 2012, 125, 2222–2231. [Google Scholar] [CrossRef]
- Magnusson, M.; Lewis, G.D.; Ericson, U.; Orho-Melander, M.; Hedblad, B.; Engström, G.; Ostling, G.; Clish, C.; Wang, T.J.; Gerszten, R.E.; et al. A diabetes-predictive amino acid score and future cardiovascular disease. Eur. Heart J. 2013, 34, 1982–1989. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Hu, C.; Yang, R.; Lv, Y.; Yuan, H.; Liang, Q.; He, B.; Pang, G.; Jiang, M.; Dong, J.; et al. Association of circulating branched-chain amino acids with cardiometabolic traits differs between adults and the oldest-old. Oncotarget 2017, 8, 88882–88893. [Google Scholar] [CrossRef] [PubMed]
- Hamaya, R.; Mora, S.; Lawler, P.R.; Cook, N.R.; Ridker, P.M.; Buring, J.E.; Lee, I.M.; Manson, J.E.; Tobias, D.K. Association of Plasma Branched-Chain Amino Acid With Biomarkers of Inflammation and Lipid Metabolism in Women. Circ. Genom. Precis. Med. 2021, 14, e003330. [Google Scholar] [CrossRef] [PubMed]
- Le Couteur, D.G.; Ribeiro, R.; Senior, A.; Hsu, B.; Hirani, V.; Blyth, F.M.; Waite, L.M.; Simpson, S.J.; Naganathan, V.; Cumming, R.G.; et al. Branched Chain Amino Acids, Cardiometabolic Risk Factors and Outcomes in Older Men: The Concord Health and Ageing in Men Project. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1805–1810. [Google Scholar] [CrossRef]
- Ni, M.Y.; Canudas-Romo, V.; Shi, J.; Flores, F.P.; Chow, M.S.C.; Yao, X.I.; Ho, S.Y.; Lam, T.H.; Schooling, C.M.; Lopez, A.D.; et al. Understanding longevity in Hong Kong: A comparative study with long-living, high-income countries. Lancet Public Health 2021, 6, e919–e931. [Google Scholar] [CrossRef]
- Woo, J.; Leung, J.C.; Wong, S.Y. Impact of childhood experience of famine on late life health. J. Nutr. Health Aging 2010, 14, 91–95. [Google Scholar] [CrossRef]
- Kin, C.F.; Shan, W.S.; Shun, L.J.; Chung, L.P.; Jean, W. Experience of famine and bone health in post-menopausal women. Int. J. Epidemiol. 2007, 36, 1143–1150. [Google Scholar] [CrossRef]
- Centre for Health Protection. Hypertension; Department of Health, The Government of the Hong Kong Special Administrative Region: Hong Kong, China, 2023. Available online: https://www.chp.gov.hk/en/healthtopics/content/25/35390.html (accessed on 6 May 2023).
- World Health Organization. HEARTS D: Diagnosis and Management of Type 2 Diabetes (HEARTS-D); World Health Organization: Geneva, Switzerland, 2020; (WHO/UCN/NCD/20.1); Available online: https://apps.who.int/iris/rest/bitstreams/1274478/retrieve (accessed on 6 May 2023).
- Rockwood, K.; Andrew, M.; Mitnitski, A. A comparison of two approaches to measuring frailty in elderly people. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 738–743. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612, Erratum in Ann. Intern. Med. 2011, 155, 408. [Google Scholar] [CrossRef]
- Su, Y.; Elshorbagy, A.; Turner, C.; Refsum, H.; Chan, R.; Kwok, T. Circulating amino acids are associated with bone mineral density decline and ten-year major osteoporotic fracture risk in older community-dwelling adults. Bone 2019, 129, 115082. [Google Scholar] [CrossRef]
- Soininen, P.; Kangas, A.J.; Würtz, P.; Suna, T.; Ala-Korpela, M. Quantitative serum nuclear magnetic resonance metabolomics in cardiovascular epidemiology and genetics. Circ. Cardiovasc. Genet. 2015, 8, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Bhinderwala, F.; Wase, N.; DiRusso, C.; Powers, R. Combining Mass Spectrometry and NMR Improves Metabolite Detection and Annotation. J. Proteome Res. 2018, 17, 4017–4022. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, S.C.; Surendran, P.; Karthikeyan, S.; Lambert, S.A.; Bolton, T.; Pennells, L.; Danesh, J.; Di Angelantonio, E.; Butterworth, A.S.; Inouye, M. Quality control and removal of technical variation of NMR metabolic biomarker data in ~120,000 UK Biobank participants. Sci. Data 2023, 10, 64. [Google Scholar] [CrossRef] [PubMed]
- Pansini, A.; Lombardi, A.; Morgante, M.; Frullone, S.; Marro, A.; Rizzo, M.; Martinelli, G.; Boccalone, E.; De Luca, A.; Santulli, G.; et al. Hyperglycemia and Physical Impairment in Frail Hypertensive Older Adults. Front. Endocrinol. 2022, 13, 831556. [Google Scholar] [CrossRef]
- Mone, P.; Gambardella, J.; Lombardi, A.; Pansini, A.; De Gennaro, S.; Leo, A.L.; Famiglietti, M.; Marro, A.; Morgante, M.; Frullone, S.; et al. Correlation of physical and cognitive impairment in diabetic and hypertensive frail older adults. Cardiovasc. Diabetol. 2022, 21, 10. [Google Scholar] [CrossRef]
- Fung, E.; Lui, L.T.; Huang, L.; Cheng, K.F.; Lau, G.H.W.; Chung, Y.T.; Ahmadabadi, B.N.; Xie, S.; Lee, J.S.W.; Hui, E.; et al. Characterising frailty, metrics of continuous glucose monitoring, and mortality hazards in older adults with type 2 diabetes on insulin therapy (HARE): A prospective, observational cohort study. Lancet Healthy Longev. 2021, 2, e724–e735. [Google Scholar] [CrossRef]
- Shah, S.H.; Sun, J.L.; Stevens, R.D.; Bain, J.R.; Muehlbauer, M.J.; Pieper, K.S.; Haynes, C.; Hauser, E.R.; Kraus, W.E.; Granger, C.B.; et al. Baseline metabolomic profiles predict cardiovascular events in patients at risk for coronary artery disease. Am. Heart J. 2012, 163, 844–850.e1. [Google Scholar] [CrossRef]
- Moissl, A.P.; Lorkowski, S.; Meinitzer, A.; Pilz, S.; Scharnagl, H.; Delgado, G.E.; Kleber, M.E.; Krämer, B.K.; Pieske, B.; Grübler, M.R.; et al. Association of branched-chain amino acids with mortality-the Ludwigshafen Risk and Cardiovascular Health (LURIC) study. iScience 2023, 26, 106459. [Google Scholar] [CrossRef]
- Reisinger, A.C.; Posch, F.; Hackl, G.; Marsche, G.; Sourij, H.; Bourgeois, B.; Eller, K.; Madl, T.; Eller, P. Branched-Chain Amino Acids Can Predict Mortality in ICU Sepsis Patients. Nutrients 2021, 13, 3106. [Google Scholar] [CrossRef]
- Luo, S.; Surapaneni, A.; Rebholz, C.M.; Appel, L.J.; Coresh, J.; Grams, M.E. Circulating Banched-Chain Amino Acids, Incident Cardiovascular Disease, and Mortality in the African American Study of Kidney Disease and Hypertension. Circ Genom Precis Med 2023, 16, e003729. [Google Scholar] [CrossRef] [PubMed]
- Vanweert, F.; Neinast, M.; Tapia, E.E.; van de Weijer, T.; Hoeks, J.; Schrauwen-Hinderling, V.B.; Blair, M.C.; Bornstein, M.R.; Hesselink, M.K.C.; Schrauwen, P.; et al. A randomized placebo-controlled clinical trial for pharmacological activation of BCAA catabolism in patients with type 2 diabetes. Nat. Commun. 2022, 13, 3508. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Li, Y.; Zeng, X.; Wang, H.; Yin, P.; Wang, L.; Liu, Y.; Liu, J.; Qi, J.; Ran, S.; et al. Burden of cardiovascular diseases in China, 1990–2016: Findings from the 2016 Global Burden of Disease Study. JAMA Cardiol 2019, 4, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Li, J.J.; Liu, H.H.; Li, S. Landscape of cardiometabolic risk factors in Chinese population: A narrative review. Cardiovasc. Diabetol. 2022, 21, 113. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart disease and stroke statistics—2022 update: A report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar]
- Yap, I.K.; Brown, I.J.; Chan, Q.; Wijeyesekera, A.; Garcia-Perez, I.; Bictash, M.; Loo, R.L.; Chadeau-Hyam, M.; Ebbels, T.; De Iorio, M.; et al. Metabolome-wide association study identifies multiple biomarkers that discriminate north and south Chinese populations at differing risks of cardiovascular disease: INTERMAP study. J. Proteome Res. 2010, 9, 6647–6654. [Google Scholar] [CrossRef]
- Wang, F.H.; Liu, J.; Deng, Q.J.; Qi, Y.; Wang, M.; Wang, Y.; Zhang, X.G.; Zhao, D. Association between plasma essential amino acids and atherogenic lipid profile in a Chinese population: A cross-sectional study. Atherosclerosis 2019, 286, 7–13. [Google Scholar] [CrossRef]
- Fukushima, K.; Harada, S.; Takeuchi, A.; Kurihara, A.; Iida, M.; Fukai, K.; Kuwabara, K.; Kato, S.; Matsumoto, M.; Hirata, A.; et al. Association between dyslipidemia and plasma levels of branched-chain amino acids in the Japanese population without diabetes mellitus. J. Clin. Lipidol. 2019, 13, 932–939.e2. [Google Scholar] [CrossRef]
- Gojda, J.; Cahova, M. Gut Microbiota as the Link between Elevated BCAA Serum Levels and Insulin Resistance. Biomolecules 2021, 11, 1414. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall | HT | No HT | p Value | DM | No DM | p Value |
|---|---|---|---|---|---|---|---|
| N | 2997 (100%) | 1282 (42.8%) | 1715 (57.2%) | - | 425 (14.2%) | 2572 (85.8%) | - |
| Age, years | 71 (68–75) | 72 (68–75) | 71 (68–75) | <0.0001 | 71 (68–76) | 71 (68–75) | 0.11 |
| Sex, male | 1424 (47.5%) | 594 (46.3%) | 830 (48.4%) | 0.26 | 206 (48.5%) | 1218 (47.3%) | 0.67 |
| Body weight, kg | 58 (51.9–65) | 59.8 (53.6–66.5) | 56.7 (50.8–63.7) | <0.0001 | 59.9 (53.9–66.8) | 57.7 (51.6–64.5) | <0.0001 |
| BMI, kg/m2 | 23.6 (21.7–25.8) | 24.4 (22.4–26.4) | 23 (21.2–25.3) | <0.0001 | 24.3 (22.4–26.4) | 23.5 (21.5–25.6) | <0.0001 |
| eGFR, mL/min/1.73 m2 | 90 (77.8–95.4) | 86.8 (73.2–94.4) | 91.7 (81.6–96) | <0.0001 | 89.6 (75.8–95.8) | 90.1 (78.1–95.3) | 0.52 |
| Frailty index | 0.11 (0.04–0.15) | 0.13 (0.11–0.19) | 0.06 (0.04–0.11) | <0.0001 | 0.17 (0.11–0.21) | 0.09 (0.04–0.13) | <0.0001 |
| PASE | 85.6 (65.3–112.6) | 84.7 (62.2–110.4) | 86.3 (67.6–115.3) | 0.0016 | 85.4 (65.4–111.3) | 85.6 (65.3–112.6) | 0.94 |
| Smoking | |||||||
| Never | 1979 (66%) | 868 (67.7%) | 1111 (64.7%) | 0.094 | 282 (66.4%) | 1697 (66%) | 0.88 |
| Past | 840 (28%) | 371 (28.9%) | 469 (27.3%) | 0.34 | 125 (29.4%) | 715 (27.8%) | 0.49 |
| Current | 178 (5.9%) | 43 (3.4%) | 135 (7.9%) | <0.0001 | 18 (4.2%) | 160 (6.2%) | 0.11 |
| Comorbidities | |||||||
| Myocardial infarction | 277 (9.2%) | 172 (13.4%) | 105 (6.1%) | <0.0001 | 63 (14.8%) | 214 (8.3%) | <0.0001 |
| Angina pectoris | 241 (8.0%) | 139 (10.8%) | 102 (6.0%) | <0.0001 | 45 (10.6%) | 196 (7.6%) | 0.037 |
| Stroke | 117 (3.9%) | 82 (6.4%) | 35 (2.0%) | <0.0001 | 25 (5.9%) | 92 (3.6%) | 0.023 |
| Heart failure | 115 (3.8%) | 73 (5.7%) | 42 (2.4%) | <0.0001 | 25 (5.9%) | 90 (3.5%) | 0.018 |
| COPD | 218 (7.3%) | 87 (6.8%) | 131 (7.6%) | 0.37 | 26 (6.1%) | 192 (7.5%) | 0.32 |
| CKD (eGFR < 60) | 189 (6.3%) | 127 (9.9%) | 62 (3.6%) | <0.0001 | 28 (6.6%) | 161 (6.3%) | 0.80 |
| Cardiovascular drugs | |||||||
| CCB | 548 (18.3%) | 509 (39.7%) | 39 (2.3%) | <0.0001 | 131 (30.8%) | 417 (16.2%) | <0.0001 |
| β-blocker | 489 (16.3%) | 430 (33.5%) | 59 (3.4%) | <0.0001 | 108 (25.4%) | 381 (14.8%) | <0.0001 |
| ACEI/ARB | 342 (1.4%) | 314 (24.5%) | 28 (1.6%) | <0.0001 | 111 (26.1%) | 231 (9.0%) | <0.0001 |
| Aspirin | 322 (10.7%) | 216 (16.8%) | 106 (6.2%) | <0.0001 | 85 (20.0%) | 237 (9.2%) | <0.0001 |
| Diuretic | 293 (9.8%) | 267 (20.8%) | 26 (1.5%) | <0.0001 | 56 (13.2%) | 237 (9.2%) | 0.011 |
| Statin | 188 (6.3%) | 133 (10.4%) | 55 (3.2%) | <0.0001 | 49 (11.5%) | 139 (5.4%) | <0.0001 |
| α-blocker | 184 (6.1%) | 110 (8.6%) | 74 (4.3%) | <0.0001 | 31 (7.3%) | 153 (5.9%) | 0.29 |
| Nitrate | 182 (6.1%) | 125 (9.8%) | 57 (3.3%) | <0.0001 | 43 (10.1%) | 139 (5.4%) | 0.0002 |
| Digoxin | 16 (0.5%) | 5 (0.4%) | 11 (0.6%) | 0.35 | 1 (0.2%) | 15 (0.6%) | 0.36 |
| Warfarin | 12 (0.4%) | 5 (0.4%) | 7 (0.4%) | 0.94 | 4 (0.9%) | 8 (0.3%) | 0.57 |
| Antihypertensive drugs * | 1177 (39.3%) | 990 (77.2%) | 187 (10.9%) | <0.0001 | 258 (60.7%) | 919 (35.7%) | <0.0001 |
| Hypoglycaemic drugs | 319 (10.6%) | 223 (17.4%) | 96 (5.6%) | <0.0001 | 311 (73.2%) | 8 (0.3%) | <0.0001 |
| Metformin | 98 (3.3%) | 67 (5.2%) | 31 (1.8%) | <0.0001 | 97 (22.8%) | 1 (0.04%) | <0.0001 |
| Glibenclamide | 61 (2.0%) | 38 (3.0%) | 23 (1.3%) | 0.0019 | 61 (14.4%) | 0 (0%) | <0.0001 |
| Gliclazide | 86 (2.9%) | 58 (4.5%) | 28 (1.6%) | <0.0001 | 83 (19.5%) | 3 (0.1%) | <0.0001 |
| Glipizide | 16 (0.5%) | 11 (0.9%) | 5 (0.3%) | 0.035 | 16 (3.8%) | 0 (0%) | <0.0001 |
| Acarbose | 5 (0.2%) | 5 (0.4%) | 0 (0%) | 0.0097 | 5 (1.2%) | 0 (0%) | <0.0001 |
| Insulin | 3 (0.1%) | 3 (0.2%) | 0 (0%) | 0.045 | 3 (0.7%) | 0 (0%) | <0.0001 |
| Tolbutamide | 2 (0.1%) | 2 (0.2%) | 0 (0%) | 0.102 | 2 (0.5%) | 0 (0%) | 0.0005 |
| 0Y | |||||||
| Variable | Overall (n = 2997) | HT (n = 1282) | No HT (n = 1715) | p Value | DM (n = 425) | No DM (n = 2572) | p Value |
| Age, years | 71 (68–75) | 72 (68–75) | 71 (68–75) | <0.0001 | 71 (68–76) | 71 (68–75) | 0.11 |
| Sex, male | 1424 (47.5%) | 594 (46.3%) | 830 (48.4%) | 0.26 | 206 (48.5%) | 1218 (47.3%) | 0.67 |
| Serum creatinine, µmol/L | 70.3 (58.2–84.3) | 72.8 (60.7–87.8) | 68.4 (57.1–81.2) | <0.0001 | 70.7 (59.1–84.5) | 70.3 (58.2–84.3) | 0.66 |
| Total BCAA, µmol/L | 514.3 (463.2–574.6) | 525.3 (474.6–592.8) | 507 (455–560.9) | <0.0001 | 558.6 (501.9–616.1) | 509 (457.7–565.5) | <0.0001 |
| Isoleucine, µmol/L | 78.9 (69.6–89.3) | 80.3 (72.1–92.4) | 77.2 (68.2–87.0) | <0.0001 | 86.1 (76.3–98.6) | 77.7 (68.7–87.5) | <0.0001 |
| Leucine, µmol/L | 146.9 (131.3–164.2) | 150 (134.9–169.1) | 144.5 (129.0–160.9) | <0.0001 | 159.8 (143.4–177.8) | 144.9 (129.5–161.7) | <0.0001 |
| Valine, µmol/L | 288.9 (259.2–323.0) | 295.2 (265.0–331.1) | 284.8 (255.7–316.1) | <0.0001 | 310.7 (283.0–340.4) | 285.6 (256.5–318.9) | <0.0001 |
| 14Y | |||||||
| Variable | Overall (n = 860) | HT at 0Y (n = 339) | No HT at 0Y (n = 521) | pvalue | DM at 0Y (n = 104) | No DM at 0Y (n = 756) | pvalue |
| Age, years | 83 (81–86) | 84 (81–87) | 83 (80–86) | 0.0005 | 83 (81–85) | 83 (81–86) | 0.94 |
| Sex, male | 408 (47.4%) | 165 (48.7%) | 243 (46.6%) | 0.56 | 50 (48.1%) | 358 (47.4%) | 0.89 |
| Serum creatinine, µmol/L | 74.3 (63.4–87.5) | 78.2 (65.8–93.9) | 71.5 (62.0–83.6) | <0.0001 | 81 (68.0–98.2) | 73 (62.8–85.7) | <0.0001 |
| Total BCAA, µmol/L | 421.6 (379.0–470.5) | 433.5 (392.5–477.9) | 413 (370.2–466.7) | 0.0002 | 469.1 (406.1–507.4) | 417.8 (374.9–464.7) | <0.0001 |
| Isoleucine, µmol/L | 53.6 (45.3–63.0) | 56.8 (48.5–64.5) | 51.8 (44.3–60.9) | <0.0001 | 62.8 (52.5–71.8) | 52.9 (44.7–61.5) | <0.0001 |
| Leucine, µmol/L | 126.4 (112.5–141.4) | 130.3 (115.9–143.9) | 123.6 (110.0–139.6) | 0.0002 | 140.1 (125.9–152.6) | 124.4 (111.4–139.3) | <0.0001 |
| Valine, µmol/L | 240.2 (219.1–268.0) | 243.3 (225.8–273.5) | 237.3 (213.9–263.9) | 0.0029 | 257.1 (231.3–281.1) | 239 (215.8–265.1) | <0.0001 |
| Variable | HT+ (Deaths, n = 596/1282) | HT− (Deaths, n = 639/1715) | DM+ (Deaths, n = 234/425) | DM− (Deaths, n = 1001/2572) | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 1.09 (1.07–1.11) | <0.0001 | 1.11 (1.09–1.13) | <0.0001 | 1.1 (1.07–1.13) | <0.0001 | 1.1 (1.09–1.11) | <0.0001 |
| Sex | 1.44 (1.16–1.78) | 0.0008 | 1.66 (1.35–2.04) | <0.0001 | 1.41 (1.01–1.98) | 0.043 | 1.62 (1.37–1.91) | <0.0001 |
| BMI | 1 (0.97–1.03) | 0.88 | 0.98 (0.95–1) | 0.085 | 0.93 (0.88–0.97) | 0.0025 | 1 (0.98–1.02) | 0.97 |
| Previous smoking | 1.32 (1.07–1.62) | 0.0086 | 1.29 (1.06–1.57) | 0.011 | 1.17 (0.84–1.63) | 0.34 | 1.34 (1.14–1.57) | 0.0003 |
| Active smoking | 2.4 (1.65–3.49) | <0.0001 | 1.85 (1.4–2.45) | <0.0001 | 1.99 (1.07–3.68) | 0.029 | 2.09 (1.65–2.65) | <0.0001 |
| Frailty index | 3.43 (0.97–12.16) | 0.057 | 3.69 (0.89–15.3) | 0.072 | 3 (0.39–22.84) | 0.29 | 3.5 (1.21–10.11) | 0.021 |
| PASE | 1 (1–1) | 0.31 | 1 (1–1) | 0.21 | 1 (0.99–1) | 0.096 | 1 (1–1) | 0.18 |
| Egfr | 0.99 (0.98–0.99) | <0.0001 | 0.99 (0.99–1) | 0.014 | 0.99 (0.98–1) | 0.0052 | 0.99 (0.98–0.99) | <0.0001 |
| log(BCAA) ‡ | 0.55 (0.3–1.02) | 0.057 | 0.43 (0.25–0.75) | 0.0029 | 0.98 (0.37–2.58) | 0.97 | 0.39 (0.25–0.61) | <0.0001 |
| Antihypertensive drugs * | 1.12 (0.91–1.38) | 0.29 | 1.3 (1.02–1.66) | 0.033 | 1.15 (0.84–1.57) | 0.39 | 1.2 (1.04–1.39) | 0.015 |
| Hypoglycaemic drugs † | 1.69 (1.36–2.08) | <0.0001 | 1.61 (1.17–2.22) | 0.0039 | 1.13 (0.83–1.54) | 0.45 | 1.73 (0.77–3.9) | 0.18 |
| Variable | Model 1 a | Model 2 b | Model 3 c | Model 4 d | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Baseline (0Y) | ||||||||
| Age | 1.10 (1.09–1.11) | <0.0001 | 1.10 (1.09–1.11) | <0.0001 | 1.10 (1.09–1.11) | <0.0001 | 1.10 (1.09–1.11) | <0.0001 |
| Sex | 1.56 (1.35–1.80) | <0.0001 | 1.55 (1.34–1.79) | <0.0001 | 1.52 (1.32–1.76) | <0.0001 | 1.57 (1.36–1.81) | <0.0001 |
| BMI | 0.99 (0.97–1.01) | 0.31 | 0.99 (0.97–1.01) | 0.21 | 0.99 (0.97–1.01) | 0.25 | 0.99 (0.97–1.01) | 0.32 |
| Previous smoking | 1.30 (1.13–1.49) | 0.0003 | 1.30 (1.13–1.50) | 0.0003 | 1.30 (1.13–1.50) | 0.0003 | 1.31 (1.13–1.50) | 0.0002 |
| Active smoking | 1.98 (1.59–2.47) | <0.0001 | 2.05 (1.64–2.56) | <0.0001 | 2.04 (1.64–2.54) | <0.0001 | 2.01 (1.61–2.51) | <0.0001 |
| Frailty index | 14.48 (6.79–30.89) | <0.0001 | 5.28 (2.16–12.92) | 0.0003 | 7.95 (3.31–19.12) | <0.0001 | 6.99 (3.12–15.66) | <0.0001 |
| eGFR | 0.99 (0.99–0.99) | <0.0001 | 0.99 (0.98–0.99) | <0.0001 | 0.99 (0.99–0.99) | <0.0001 | 0.99 (0.98–0.99) | <0.0001 |
| log(BCAA) † | 0.58 (0.39–0.87) | 0.0090 | 0.47 (0.31–0.70) | 0.0002 | 0.58 (0.39–0.87) | 0.0078 | 0.47 (0.32–0.71) | 0.0003 |
| HT | - | - | 1.08 (0.95–1.24) | 0.23 | - | - | - | - |
| DM | - | - | 1.61 (1.38–1.89) | <0.0001 | - | - | - | - |
| Antihypertensive drugs | - | - | - | - | 1.21 (1.06–1.38) | 0.0056 | - | - |
| Hypoglycaemic drugs | - | - | - | - | - | - | 1.67 (1.4–1.99) | <0.0001 |
| 14Y | ||||||||
| Age | 1.10 (1.04–1.15) | 0.0002 | 1.10 (1.04–1.15) | 0.0002 | 1.10 (1.05–1.15) | 0.0002 | 1.10 (1.04–1.15) | 0.0002 |
| Sex | 1.70 (1.03–2.79) | 0.037 | 1.62 (0.98–2.67) | 0.058 | 1.61 (0.98–2.65) | 0.061 | 1.69 (1.03–2.78) | 0.038 |
| BMI (baseline) | 0.95 (0.88–1.02) | 0.15 | 0.95 (0.88–1.02) | 0.14 | 0.95 (0.88–1.02) | 0.19 | 0.95 (0.88–1.02) | 0.15 |
| Previous smoking (baseline) | 1.22 (0.74–2.00) | 0.43 | 1.25 (0.76–2.05) | 0.38 | 1.22 (0.75–2.01) | 0.42 | 1.23 (0.75–2.01) | 0.42 |
| Active smoking (baseline) | 2.46 (1.12–5.38) | 0.025 | 2.67 (1.21–5.91) | 0.015 | 2.68 (1.21–5.90) | 0.015 | 2.45 (1.12–5.37) | 0.025 |
| Frailty index (baseline) | 8.42 (0.37–189.70) | 0.18 | 2.56 (0.06–105.63) | 0.62 | 1.71 (0.04–69.51) | 0.78 | 7.52 (0.29–196.15) | 0.23 |
| eGFR | 0.97 (0.96–0.99) | <0.0001 | 0.98 (0.96–0.99) | 0.0002 | 0.98 (0.96–0.99) | 0.0001 | 0.97 (0.96–0.99) | 0.0001 |
| log(BCAA) † | 0.16 (0.04–0.61) | 0.0069 | 0.15 (0.04–0.58) | 0.0057 | 0.15 (0.04–0.56) | 0.0047 | 0.16 (0.04–0.60) | 0.0067 |
| HT (baseline) | - | - | 1.41 (0.88–2.25) | 0.15 | - | - | - | - |
| DM (baseline) | - | - | 1.01 (0.53–1.93) | 0.97 | - | - | - | - |
| Antihypertensive drugs (baseline) | - | - | - | - | 1.51 (0.94–2.43) | 0.092 | - | - |
| Hypoglycaemic drugs (baseline) | - | - | - | - | - | - | 1.09 (0.55–2.16) | 0.81 |
| Variable | Model 1 a | Model 2 b | Model 3 c | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Baseline (0Y) | ||||||
| Age | 1.10 (1.09–1.11) | <0.0001 | 1.1 (1.09–1.11) | <0.0001 | 1.1 (1.09–1.11) | <0.0001 |
| Sex | 1.56 (1.35–1.80) | <0.0001 | 1.56 (1.35–1.8) | <0.0001 | 1.53 (1.32–1.76) | <0.0001 |
| BMI | 0.99 (0.97–1.01) | 0.31 | 0.99 (0.97–1.01) | 0.27 | 0.99 (0.97–1.01) | 0.19 |
| Previous smoking | 1.30 (1.13–1.49) | 0.0003 | 1.3 (1.13–1.5) | 0.0003 | 1.31 (1.14–1.51) | 0.0002 |
| Active smoking | 1.98 (1.59–2.47) | <0.0001 | 2.03 (1.63–2.53) | <0.0001 | 2.09 (1.68–2.61) | <0.0001 |
| Frailty index | 14.48 (6.79–30.89) | <0.0001 | 5.34 (2.19–13.05) | 0.0002 | 3.86 (1.53–9.75) | 0.0043 |
| eGFR | 0.99 (0.99–0.99) | <0.0001 | 0.99 (0.98–0.99) | <0.0001 | 0.99 (0.99–0.99) | <0.0001 |
| log(BCAA)† | 0.58 (0.39–0.87) | 0.0090 | 0.47 (0.31–0.7) | 0.0003 | 0.46 (0.31–0.7) | 0.0002 |
| HT and antihypertensive drugs | - | - | 1.12 (0.98–1.28) | 0.10 | - | - |
| DM and hypoglycaemic drugs | - | - | 1.65 (1.38–1.96) | <0.0001 | - | - |
| HT or antihypertensive drugs | - | - | - | - | 1.17 (1.02–1.34) | 0.024 |
| DM or hypoglycaemic drugs | - | - | - | - | 1.62 (1.39–1.9) | <0.0001 |
| 14Y | ||||||
| Age | 1.10 (1.04–1.15) | 0.0002 | 1.1 (1.05–1.15) | 0.0002 | 1.1 (1.04–1.15) | 0.0002 |
| Sex | 1.70 (1.03–2.79) | 0.037 | 1.63 (0.99–2.68) | 0.053 | 1.61 (0.97–2.66) | 0.065 |
| BMI (baseline) | 0.95 (0.88–1.02) | 0.15 | 0.95 (0.88–1.02) | 0.18 | 0.95 (0.88–1.02) | 0.15 |
| Previous smoking (baseline) | 1.22 (0.74–2.00) | 0.43 | 1.26 (0.77–2.06) | 0.37 | 1.23 (0.75–2.02) | 0.42 |
| Active smoking (baseline) | 2.46 (1.12–5.38) | 0.025 | 2.67 (1.21–5.87) | 0.015 | 2.67 (1.2–5.92) | 0.016 |
| Frailty index (baseline) | 8.42 (0.37–189.70) | 0.18 | 1.61 (0.04–65.75) | 0.80 | 2.5 (0.05–120.87) | 0.65 |
| eGFR | 0.97 (0.96–0.99) | <0.0001 | 0.98 (0.96–0.99) | 0.0002 | 0.97 (0.96–0.99) | 0.0001 |
| log(BCAA) † | 0.16 (0.04–0.61) | 0.0069 | 0.15 (0.04–0.55) | 0.0045 | 0.15 (0.04–0.58) | 0.0056 |
| HT and antihypertensive drugs (baseline) | - | - | 1.6 (1–2.55) | 0.049 | - | - |
| DM and hypoglycaemic drugs (baseline) | - | - | 1.06 (0.53–2.11) | 0.87 | - | - |
| HT or antihypertensive drugs (baseline) | - | - | - | - | 1.35 (0.83–2.21) | 0.21 |
| DM or hypoglycaemic drugs (baseline) | - | - | - | - | 1.01 (0.53–1.92) | 0.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fung, E.; Ng, K.H.; Kwok, T.; Lui, L.-T.; Palaniswamy, S.; Chan, Q.; Lim, L.-L.; Wiklund, P.; Xie, S.; Turner, C.; et al. Divergent Survival Outcomes Associated with Elevated Branched-Chain Amino Acid Levels among Older Adults with or without Hypertension and Diabetes: A Validated, Prospective, Longitudinal Follow-Up Study. Biomolecules 2023, 13, 1252. https://doi.org/10.3390/biom13081252
Fung E, Ng KH, Kwok T, Lui L-T, Palaniswamy S, Chan Q, Lim L-L, Wiklund P, Xie S, Turner C, et al. Divergent Survival Outcomes Associated with Elevated Branched-Chain Amino Acid Levels among Older Adults with or without Hypertension and Diabetes: A Validated, Prospective, Longitudinal Follow-Up Study. Biomolecules. 2023; 13(8):1252. https://doi.org/10.3390/biom13081252
Chicago/Turabian StyleFung, Erik, Kwan Hung Ng, Timothy Kwok, Leong-Ting Lui, Saranya Palaniswamy, Queenie Chan, Lee-Ling Lim, Petri Wiklund, Suyi Xie, Cheryl Turner, and et al. 2023. "Divergent Survival Outcomes Associated with Elevated Branched-Chain Amino Acid Levels among Older Adults with or without Hypertension and Diabetes: A Validated, Prospective, Longitudinal Follow-Up Study" Biomolecules 13, no. 8: 1252. https://doi.org/10.3390/biom13081252