
Emergent Inflammatory Markers and Echocardiographic Indices in Patients with Bronchial Asthma
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Intervention
2.3. Blood Samples
2.4. Statistical Analysis
3. Results
3.1. Baseline Clinical and Laboratory Characteristics
3.2. Cardiac Findings (Electrocardiogram and Echocardiogram)
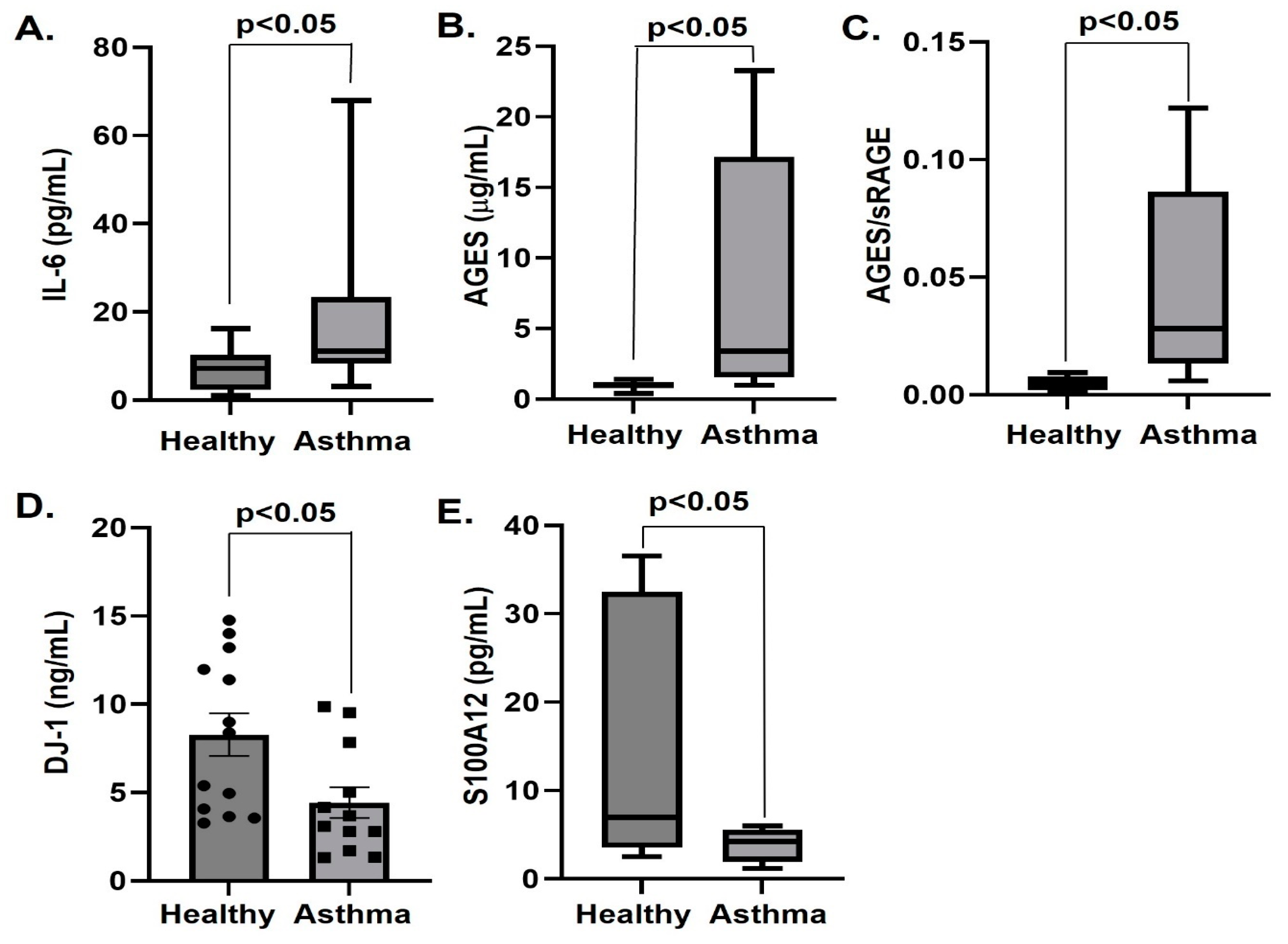
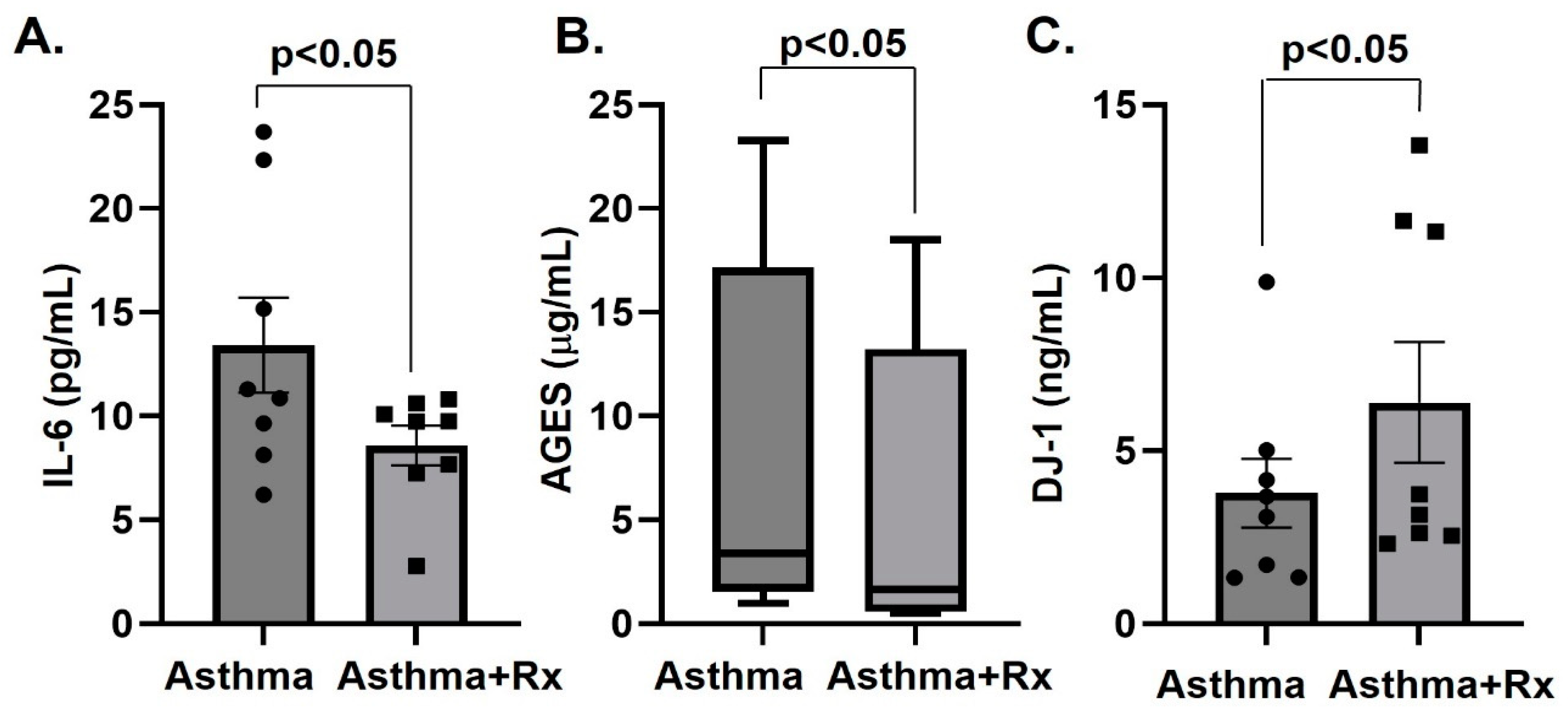
3.3. Serum Levels of IL-6, IL-1β, RAGE Ligands and DJ-1
3.4. Correlations of Inflammatory Markers and Spirometry Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gans, M.D.; Gavrilova, T. Understanding the immunology of asthma: Pathophysiology, biomarkers, and treatments for asthma endotypes. Paediatr. Respir. Rev. 2020, 36, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Cowan, D.C. Obesity, Inflammation, and Severe Asthma: An Update. Curr. Allergy Asthma Rep. 2021, 21, 46. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Dinarello, C.A.; Molgora, M.; Garlanda, C. Interleukin-1 and Related Cytokines in the Regulation of Inflammation and Immunity. Immunity 2019, 50, 778–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, J.; Li, Y.; Zhong, W.; Gao, P.; Hu, C. Recent developments in the role of reactive oxygen species in allergic asthma. J. Thorac. Dis. 2017, 9, E32–E43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudson, B.I.; Lippman, M.E. Targeting RAGE Signaling in Inflammatory Disease. Annu. Rev. Med. 2018, 69, 349–364. [Google Scholar] [CrossRef]
- Gorroño, L.E.; López-Díez, R.; Yepuri, G.; Ramirez, L.S.; Reverdatto, S.; Gugger, P.; Shekhtman, A.; Ramasamy, R.; Schmidt, A.M. Receptor for Advanced Glycation End Products (RAGE) and Mechanisms and Therapeutic Opportunities in Diabetes and Cardiovascular Disease: Insights from Human Subjects and Animal Models. Front. Cardiovasc. Med. 2020, 7, 37. [Google Scholar] [CrossRef]
- Schmidt, A.M. Soluble RAGEs—Prospects for treating & tracking metabolic and inflammatory disease. Vasc. Pharmacol. 2015, 72, 1–8. [Google Scholar]
- Rai, V.; Touré, F.; Chitayat, S.; Pei, R.; Song, F.; Li, Q.; Zhang, J.; Rosario, R.; Ramasamy, R.; Chazin, W.J.; et al. Lysophosphatidic acid targets vascular and oncogenic pathways via RAGE signaling. J. Exp. Med. 2012, 209, 2339–2350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, K.; Sakai, S.; Tsuyama, J.; Nakamura, A.; Otani, K.; Kurabayashi, K.; Yogiashi, Y.; Masai, H.; Shichita, T. Extracellular DJ-1 induces sterile inflammation in the ischemic brain. PLoS Biol. 2021, 19, e3000939. [Google Scholar] [CrossRef] [PubMed]
- Perkins, T.N.; Oury, T.D. The perplexing role of RAGE in pulmonary fibrosis: Causality or casualty? Ther. Adv. Respir. Dis. 2021, 15, 17534666211016071. [Google Scholar] [CrossRef]
- Lyu, Y.; Zhao, H.; Ye, Y.; Liu, L.; Zhu, S.; Xia, Y.; Zou, F.; Cai, S. Decreased soluble RAGE in neutrophilic asthma is correlated with disease severity and RAGE G82S variants. Mol. Med. Rep. 2018, 17, 4131–4137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, T.; Asai, K.; Fujimoto, H.; Tanaka, H.; Kanazawa, H.; Hirata, K. Increased levels of HMGB-1 and endogenous secretory RAGE in induced sputum from asthmatic patients. Respir. Med. 2011, 105, 519–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukkar, M.B.; Wood, L.G.; Tooze, M.; Simpson, J.L.; McDonald, V.M.; Gibson, P.G.; Wark, P.A.B. Soluble RAGE is deficient in neutrophilic asthma and COPD. Eur. Respir. J. 2012, 39, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Jiang, Y.-Q.; Wang, W.-X.; Zhou, Z.-X.; Wang, Y.-G.; Yang, L.; Ji, Y.-L. HMGB1 and RAGE levels in induced sputum correlate with asthma severity and neutrophil percentage. Hum. Immunol. 2012, 73, 1171–1174. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, M.C.; Barnet, J.H.; Korcarz, C.E.; Hagen, E.W.; Peppard, P.E.; Stein, J.H. Late-onset asthma predicts cardiovascular disease events: The Wisconsin sleep cohort. J. Am. Heart Assoc. 2016, 5, e003448. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, M.; Konishi, M.; Akiyama, E.; Morita, Y.; Fukutomi, Y.; Nakayama, N.; Takamura, T.; Tamura, K.; Kimura, K. Prognostic role of bronchial asthma in patients with heart failure. Heart Vessel. 2020, 35, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.Y.; Lu, L.; Wang, Y.N.; Jin, C.; Zhang, R.Y.; Zhang, Q.; Chen, Q.J.; Shen, W.F. Association of increased S100B, S100A6 and S100P in serum levels with acute coronary syndrome and also with the severity of myocardial infarction in cardiac tissue of rat models with ischemia-reperfusion injury. Atherosclerosis 2011, 217, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, R.; Schmidt, A.M. Receptor for Advanced Glycation End Products (RAGE) and Implications for the Pathophysiology of Heart Failure. Curr. Heart Fail. Rep. 2012, 9, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Larsen, H.G.; Yndigegn, T.; Marinković, G.; Grufman, H.; Mares, R.; Nilsson, J.; Goncalves, I.; Schiopu, A. The soluble receptor for advanced glycation end-products (sRAGE) has a dual phase-dependent association with residual cardiovascular risk after an acute coronary event. Atherosclerosis 2019, 287, 16–23. [Google Scholar] [CrossRef]
- Haahtela, T.; Burbach, G.J.; Bachert, C.; Bindslev-Jensen, C.; Bonini, S.; Bousquet, J.; Bousquet-Rouanet, L.; Bousquet, P.J.; Bresciani, M.; Bruno, A.; et al. Clinical relevance is associated with allergen-specific wheal size in skin prick testing. Clin. Exp. Allergy 2013, 44, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Karrasch, S.; Linde, K.; Rücker, G.; Sommer, H.; Karsch-Völk, M.; Kleijnen, J.; Jörres, R.A.; Schneider, A. Accuracy of FeNO for diagnosing asthma: A systematic review. Thorax 2017, 72, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otterstad, J.E. Measuring left ventricular volume and ejection fraction with the biplane Simpson’s method. Heart 2002, 88, 559–560. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K. Is there any evidence that AGE/sRAGE is a universal biomarker/risk marker for diseases? Mol. Cell Biochem. 2019, 451, 139–144. [Google Scholar] [CrossRef]
- Perkins, T.N.; Donnell, M.L.; Oury, T.D. The axis of the receptor for advanced glycation endproducts in asthma and allergic airway disease. Allergy 2021, 76, 1350–1366. [Google Scholar] [CrossRef] [PubMed]
- Perkins, T.N.; Oczypok, E.A.; Dutz, R.E.; Donnell, M.L.; Myerburg, M.M.; Oury, T.D. The receptor for advanced glycation end products is a critical mediator of type 2 cytokine signaling in the lungs. J. Allergy Clin. Immunol. 2019, 144, 796–808.e12. [Google Scholar] [CrossRef] [Green Version]
- Elseify, M.; Fouda, E.; Nabih, E.S. Serum Level of Soluble Receptor for Advanced Glycation End Products in Asthmatic Children and its Correlation to Severity and Pulmonary Functions. Clin. Lab. 2014, 60, 957–962. [Google Scholar] [PubMed]
- Li, Y.; Wu, R.; Tian, Y.; Bao, T.; Tian, Z. Fraction of exhaled nitric oxide and soluble receptors for advanced glycation end products are negatively correlated in children with recurrent wheezing. Asian Pac. J. Allergy Immunol. 2017, 35, 33–37. [Google Scholar]
- Sharma, A.; Kaur, S.; Sarkar, M.; Sarin, B.C.; Changotra, H. The AGE-RAGE Axis and RAGE Genetics in Chronic Obstructive Pulmonary Disease. Clin. Rev. Allergy Immunol. 2021, 60, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-H.; Chang, H.S.; Bae, D.-J.; Song, H.J.; Kim, M.-S.; Park, J.S.; Jun, J.A.; Lee, S.Y.; Uh, S.T.; Kim, S.H.; et al. Role of S100A9 in the development of neutrophilic inflammation in asthmatics and in a murine model. Clin. Immunol. 2017, 183, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-H.; Jang, A.-S.; Park, J.-S.; Kim, T.-H.; Choi, Y.S.; Shin, H.-R.; Park, S.-W.; Uh, S.-T.; Choi, J.-S.; Kim, Y.H.; et al. Elevation of S100 calcium binding protein A9 in sputum of neutrophilic inflammation in severe uncontrolled asthma. Ann. Allergy Asthma Immunol. 2013, 111, 268–275.e1. [Google Scholar] [CrossRef]
- Wu, J.; Kobayashi, M.; Sousa, E.A.; Liu, W.; Cai, J.; Goldman, S.J.; Dorner, A.J.; Projan, S.J.; Kavuru, M.S.; Qiu, Y.; et al. Differential Proteomic Analysis of Bronchoalveolar Lavage Fluid in Asthmatics following Segmental Antigen Challenge. Mol. Cell. Proteom. 2005, 4, 1251–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozinovski, S.; Cross, M.; Vlahos, R.; Jones, J.E.; Hsuu, K.; Tessier, P.A.; Reynolds, E.C.; Hume, D.A.; Hamilton, J.A.; Geczy, C.L.; et al. S100A8 Chemotactic Protein Is Abundantly Increased, but Only a Minor Contributor to LPS-Induced, Steroid Resistant Neutrophilic Lung Inflammation in Vivo. J. Proteome Res. 2005, 4, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Greenlee, K.J.; Corry, D.B.; Engler, D.A.; Matsunami, R.K.; Tessier, P.; Cook, R.G.; Werb, Z.; Kheradmand, F. Proteomic Identification of In Vivo Substrates for Matrix Metalloproteinases 2 and 9 Reveals a Mechanism for Resolution of Inflammation. J. Immunol. 2006, 177, 7312–7321. [Google Scholar] [CrossRef] [Green Version]
- Gharib, S.A.; Nguyen, E.V.; Lai, Y.; Plampin, J.D.; Goodlett, D.R.; Hallstrand, T.S. Induced sputum proteome in healthy subjects and asthmatic patients. J. Allergy Clin. Immunol. 2011, 128, 1176–1184.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camoretti-Mercado, B.; Karrar, E.; Nuñez, L.; Bowman, M.A.H. S100A12 and the airway smooth muscle: Beyond inflammation and constriction. J. Allergy Ther. 2012, 3 (Suppl. S1), S1–S7. [Google Scholar] [PubMed]
- Bowler, R.P.; Mishra, V.; Banga, J.; Silveyra, P. Oxidative stress and cellular pathways of asthma and inflammation: Therapeutic strategies and pharmacological targets. Pharmacol. Ther. 2018, 181, 169–182. [Google Scholar]
- Kim, D.K.; Kim, H.S.; Kim, A.-R.; Kim, J.H.; Kim, B.; Noh, G.; Kim, H.S.; Beaven, M.A.; Kim, Y.M.; Choi, W.S. DJ-1 regulates mast cell activation and IgE-mediated allergic responses. J. Allergy Clin. Immunol. 2012, 131, 1653–1662.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahle, P.J.; Oh, S.E.; Mouradian, M.M. Cytoprotective mechanisms of DJ-1 against oxidative stress through modulating ERK1/2 and ASK1 signal transduction. Redox Biol. 2018, 14, 211–217. [Google Scholar]
- Neves, M.; Grãos, M.; Anjo, S.I.; Manadas, B. Modulation of signaling pathways by DJ-1: An updated overview. Redox Biol. 2022, 51, 102283. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, J.; Wang, J.; Yang, B.; He, Q.; Weng, Q. Role of DJ-1 in Immune and Inflammatory Diseases. Front. Immunol. 2020, 11, 994. [Google Scholar] [CrossRef]
- Kaur, S.; Bansal, Y.; Kumar, R.; Bansal, G. A panoramic review of IL-6: Structure, pathophysiological roles and inhibitors. Bioorg. Med. Chem. 2020, 28, 115327. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Healthy | Asthmatics | p | |
|---|---|---|---|
| n | 12 | 13 | N.S. |
| Age (years) | 35 ± 3.5 | 37 + 5.8 | N.S. |
| Sex (Female) | 4 | 5 | N.S. |
| BMI (Kg/m2) | 22.1 ± 6.4 | 24.33 ± 3.03 | N.S. |
| E (m/s) | 0.86 ± 0.15 | 0.77 ± 0.13 | N.S. |
| A (m/s) | 0.45 (0.44, 0.46) | 0.51 (0.48, 0.56) | N.S. |
| E/A | 1.7 ± 0.3 | 1.5 ± 0.2 | N.S. |
| RVD(4CHmid) (mm) | 29.3 ± 2.5 | 30.1 ± 4.2 | N.S. |
| LVESD (mm) | 44.3 ± 3.2 | 45.3 ± 5.6 | N.S. |
| LVEDD (mm) | 26.7 ± 2.1 | 30.1 ± 4.1 | N.S. |
| Left atrium (mL) | 32.1 ± 2.1 | 33.5 ± 4.3 | N.S. |
| PASP (mmHg) | 14.2 ± 2.8 | 19.1 ± 6.2 | N.S. |
| Right atrium (mL) | 27.6 ± 5.8 | 30.75 ± 6.57 | N.S. |
| SRV (cm/s) | 14.3 ± 2.5 | 13.8 ± 2.1 | N.S. |
| TAPSE (mm) | 26.7 ± 2.7 | 24.3 ± 2.8 | N.S. |
| tIgE (IU/L) | 155.2 ± 61.4 | 173.4 ± 73.2 | N.S. |
| FeNO (ppb) | 0 (0, 30.5) | 19.7 (0, 134.9) | N.S. |
| FEV1″ (L) | 4.0 ± 0.8 | 3.3 ± 0.6 | N.S. |
| FEV1″ (%) | 99.5 ± 9.9 | 96.0 ± 11.4 | N.S. |
| FVC (L) | 5.2 ± 1.1 | 4.7 ± 0.9 | N.S. |
| FVC (%) | 108.0 ± 7.2 | 113.4 ± 14.3 | N.S. |
| MEF (%) | 75.7 ± 28.6 | 55.8 ± 11.1 | N.S. |
| EF (%) | 65.1 ± 3.5 | 62.8 ± 3.6 | N.S. |
| Healthy | Asthmatics | p | |
|---|---|---|---|
| n | 12 | 13 | |
| DJ-1 (ng/mL) | 8.4 (3.9, 12.6) | 3.4 (1.9, 7.1) | <0.05 |
| S100A12 (ng/mL) | 6.9 (3.6, 32.5) | 4.3 (1.9, 5.6) | <0.05 |
| IL-1β (pg/mL) | 5.1 (3.1, 49.4) | 4.1 (3.1, 8.4) | N.S. |
| IL-6 (pg/mL) | 7.2 (2.4, 10.3) | 11.1 (8.3, 23.4) | <0.05 |
| AGE (μg/mL) | 1.0 (0.8, 1.2) | 3.4 (1.6, 17.2) | <0.05 |
| Ratio AGE/sRAGE (%) | 0.005 (0.002, 0.008) | 0.028 (0.013, 0.086) | <0.05 |
| S100A8/A9 (ng/mL) | 1324.7 (171.8, 1884.2) | 559.1 (288.3, 1599.7) | N.S. |
| S100B (pg/mL) | 181.1 ± 38.6 | 216.7 ± 135.9 | N.S. |
| sRAGE (pg/mL) | 209.8 (120.7, 621.5) | 156.4 (94.2, 304.7) | N.S. |
| Pre-Rx | Post-Rx | p | |
|---|---|---|---|
| n | 8 | 8 | |
| DJ-1 (ng/mL) | 3.8 + 0.9 | 6.4 + 1.7 | <0.05 |
| S100A12 (ng/mL) | 5.2 (2.4, 5.6) | 2.4 (1.9, 6.0) | N.S. |
| IL-1β (pg/mL) | 3.9 (3.1, 7.3) | 3.2 (2.9, 6.1) | N.S. |
| IL-6 (pg/mL) | 13.4 + 2.3 | 8.6 + 2.7 | <0.05 |
| AGE (μg/mL) | 3.4 (1.6, 17.2) | 1.7 (0.6, 13.2) | <0.05 |
| Ratio AGE/sRAGE (%) | 0.044 + 0.015 | 0.036 + 0.017 | N.S. |
| S100A8/A9 (ng/mL) | 2362.9 + 1294.2 | 3654.6 + 1793.3 | N.S. |
| S100B (pg/mL) | 225.4 + 56.7 | 150.7 + 36.2 | N.S. |
| sRAGE (pg/mL) | 189.7 + 58.4 | 170.1 + 46.4 | N.S. |
| FEV1″(Post Rx) r | p | FEV1″/FVC (Post Rx) r | p | MEF75–25 (Post Rx) r | p | sRAGE r | p | |
|---|---|---|---|---|---|---|---|---|
| S100B | −0.737 | <0.05 | ||||||
| S100A8/A9 | −0.762 | <0.05 | −0.712 | <0.05 | 0.403 | <0.05 | ||
| DJ-1 | −0.787 | <0.05 | 0.833 | <0.05 | ||||
| IL-6 | 0.714 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkavogiannakis, N.A.; Tsoporis, J.N.; Drosatos, I.-A.; Tsirebolos, G.; Izhar, S.; Sakadakis, E.; Triantafyllis, A.S.; Parker, T.G.; Kalogiros, L.A.; Leong-Poi, H.; et al. Emergent Inflammatory Markers and Echocardiographic Indices in Patients with Bronchial Asthma. Biomolecules 2023, 13, 955. https://doi.org/10.3390/biom13060955
Gkavogiannakis NA, Tsoporis JN, Drosatos I-A, Tsirebolos G, Izhar S, Sakadakis E, Triantafyllis AS, Parker TG, Kalogiros LA, Leong-Poi H, et al. Emergent Inflammatory Markers and Echocardiographic Indices in Patients with Bronchial Asthma. Biomolecules. 2023; 13(6):955. https://doi.org/10.3390/biom13060955
Chicago/Turabian StyleGkavogiannakis, Nikolaos A., James N. Tsoporis, Ioannis-Alexandros Drosatos, George Tsirebolos, Shehla Izhar, Eleftherios Sakadakis, Andreas S. Triantafyllis, Thomas G. Parker, Lampros A. Kalogiros, Howard Leong-Poi, and et al. 2023. "Emergent Inflammatory Markers and Echocardiographic Indices in Patients with Bronchial Asthma" Biomolecules 13, no. 6: 955. https://doi.org/10.3390/biom13060955