Arginine Metabolites as Biomarkers of Myocardial Ischaemia, Assessed with Cardiac Magnetic Resonance Imaging in Chronic Kidney Disease

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Serum Biochemistry
2.3. CMR Protocol
2.4. CMR Analysis
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Arginine Metabolite Concentrations in Normal Volunteers and CKD Patients
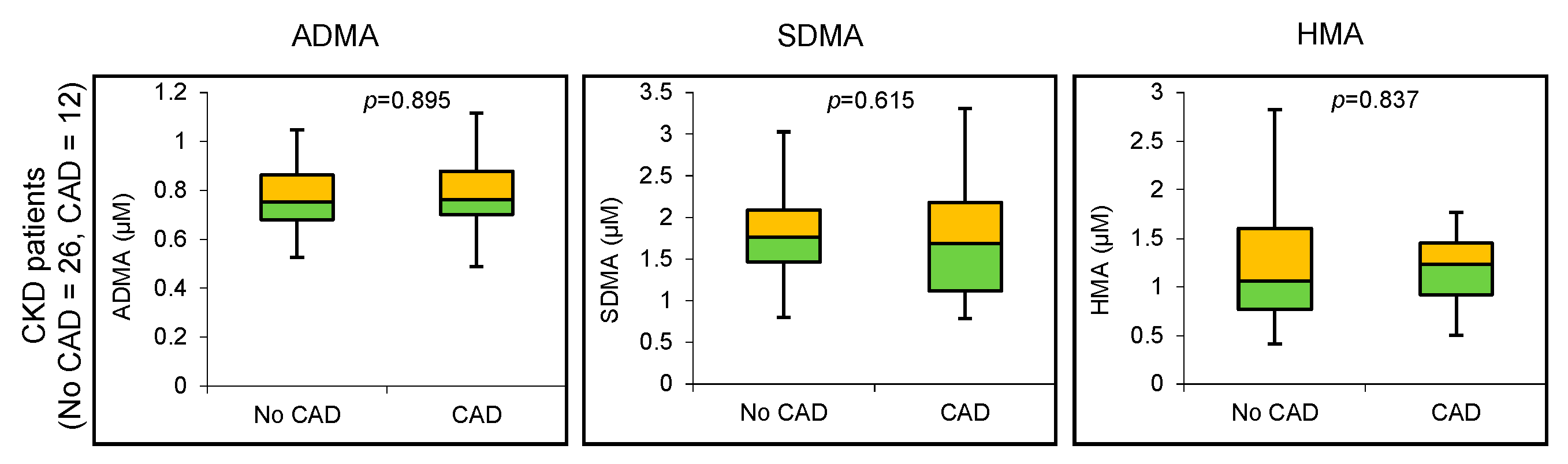
3.3. Arginine Metabolite Concentrations in CKD Patients with and without CAD
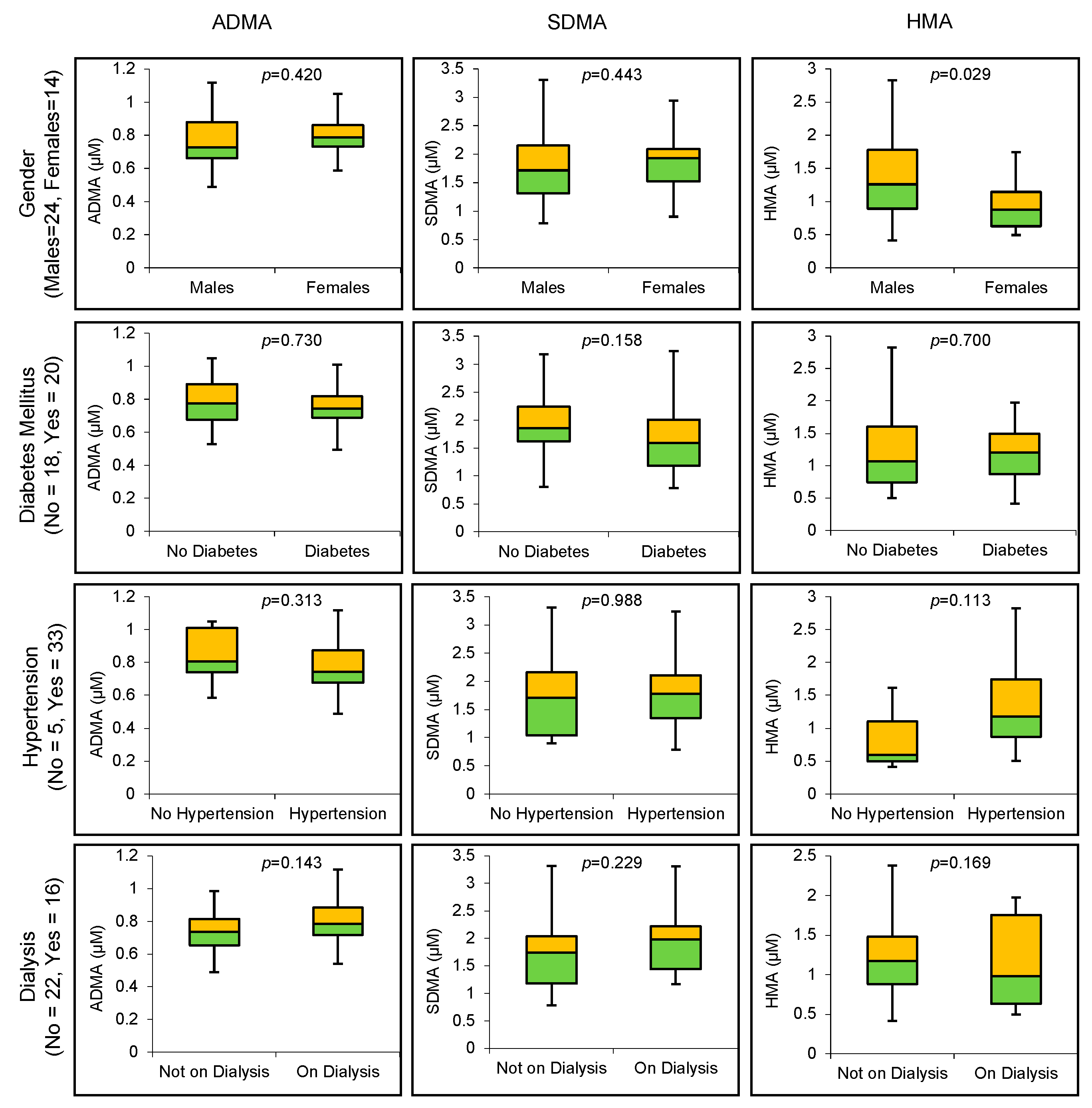
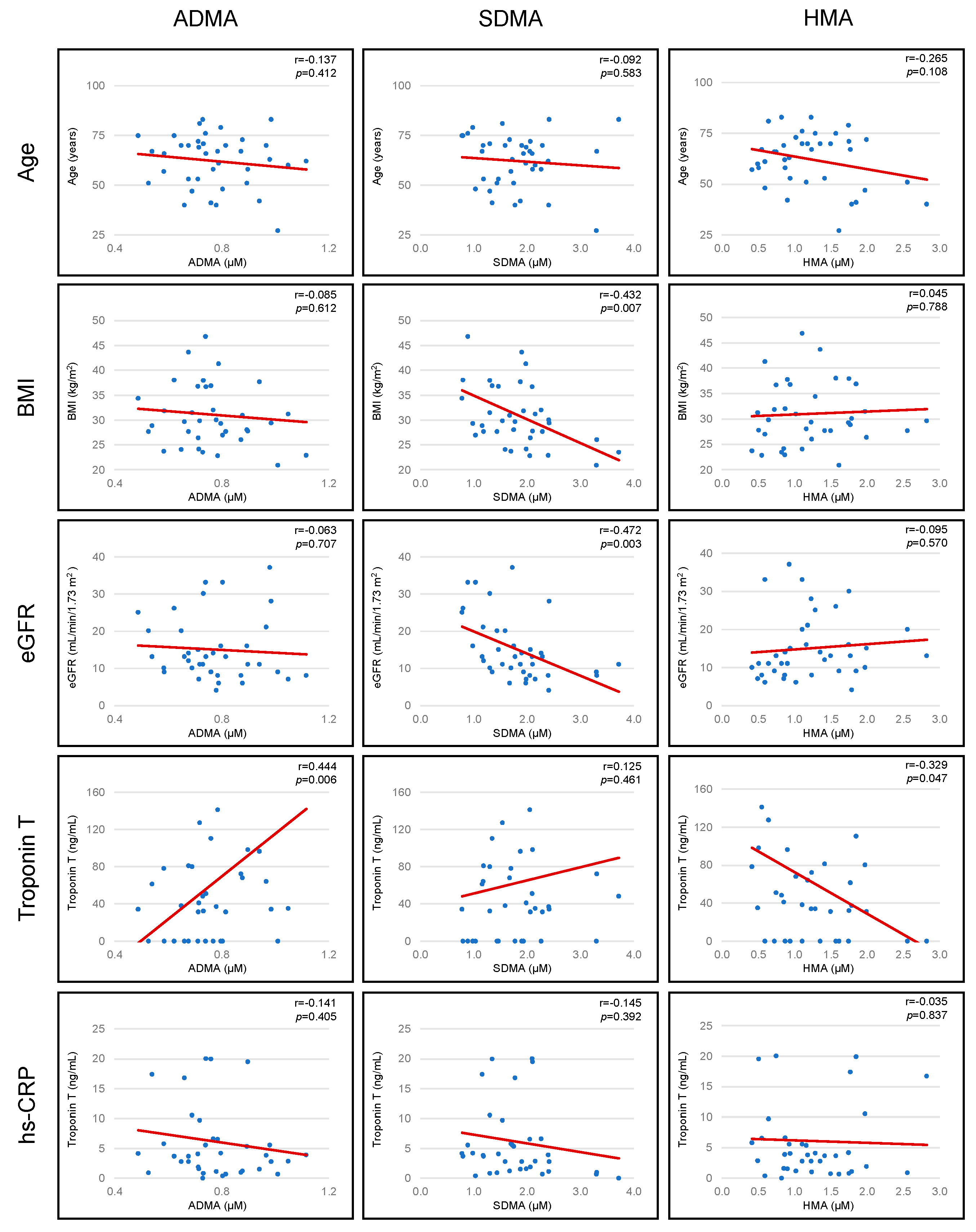
3.4. Association between Arginine Metabolites and Patient Baseline Characteristics: Age, Gender, BMI, Renal Function (eGFR), Diabetes Mellitus, Hypertension, Dialysis, Troponin T (TnT) and hs-CRP
3.5. Association between Arginine Metabolites and CMR Derived Parameters: Left Ventricular Ejection Fraction (LVEF), Indexed Left Ventricular Mass (LVMi), Stress OS-CMR and Stress T1 Mapping
3.6. Adjusted Partial Correlations between Biochemical Markers of Endothelial Dysfunction (Arginine Metabolites) and Myocardial Oxygenation (Δ OS-CMR SI) and Perfusion Response to Stress (Δ T1)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iimori, S.; Naito, S.; Noda, Y.; Nishida, H.; Kihira, H.; Yui, N.; Okado, T.; Sasaki, S.; Uchida, S.; Rai, T. Anaemia management and mortality risk in newly visiting patients with chronic kidney disease in Japan: The CKD-ROUTE study. Nephrology 2015, 20, 601–608. [Google Scholar] [CrossRef]
- Ritchie, J.; Rainone, F.; Green, D.; Alderson, H.; Chiu, D.; Middleton, R.; O’Donoghue, D.; Kalra, P.A. Extreme Elevations in Blood Pressure and All-Cause Mortality in a Referred CKD Population: Results from the CRISIS Study. Int. J. Hypertens. 2013, 2013, 597906. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.; Matthews, G.J.; Shah, R.Y.; McLaughlin, C.; Chen, J.; Wolman, M.; Master, S.R.; Chai, B.; Xie, D.; Rader, D.J.; et al. Serum Fractalkine (CX3CL1) and Cardiovascular Outcomes and Diabetes: Findings From the Chronic Renal Insufficiency Cohort (CRIC) Study. Am. J. Kidney Dis. 2015, 66, 266–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 2003, 42, 1050–1065. [Google Scholar] [CrossRef] [PubMed]
- Kielstein, J.T.; Zoccali, C. Asymmetric dimethylarginine: A novel marker of risk and a potential target for therapy in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2008, 17, 609–615. [Google Scholar] [CrossRef]
- Schwedhelm, E.; Boger, R.H. The role of asymmetric and symmetric dimethylarginines in renal disease. Nat. Rev. Nephrol. 2011, 7, 275–285. [Google Scholar] [CrossRef]
- Baylis, C. Nitric oxide deficiency in chronic kidney disease. Am. J. Physiol. Renal. Physiol. 2008, 294, F1–F9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furchgott, R.F.; Zawadzki, J.V. The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nature 1980, 288, 373–376. [Google Scholar] [CrossRef]
- Forstermann, U.; Closs, E.I.; Pollock, J.S.; Nakane, M.; Schwarz, P.; Gath, I.; Kleinert, H. Nitric oxide synthase isozymes. Characterization, purification, molecular cloning, and functions. Hypertension 1994, 23, 1121–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marz, W.; Meinitzer, A.; Drechsler, C.; Pilz, S.; Krane, V.; Kleber, M.E.; Fischer, J.; Winkelmann, B.R.; Bohm, B.O.; Ritz, E.; et al. Homoarginine, cardiovascular risk, and mortality. Circulation 2010, 122, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Ravani, P.; Maas, R.; Malberti, F.; Pecchini, P.; Mieth, M.; Quinn, R.; Tripepi, G.; Mallamaci, F.; Zoccali, C. Homoarginine and mortality in pre-dialysis chronic kidney disease (CKD) patients. PLoS ONE 2013, 8, e72694. [Google Scholar] [CrossRef]
- Drechsler, C.; Meinitzer, A.; Pilz, S.; Krane, V.; Tomaschitz, A.; Ritz, E.; Marz, W.; Wanner, C. Homoarginine, heart failure, and sudden cardiac death in haemodialysis patients. Eur. J. Heart Fail. 2011, 13, 852–859. [Google Scholar] [CrossRef]
- Lu, T.M.; Ding, Y.A.; Lin, S.J.; Lee, W.S.; Tai, H.C. Plasma levels of asymmetrical dimethylarginine and adverse cardiovascular events after percutaneous coronary intervention. Eur. Heart J. 2003, 24, 1912–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valkonen, V.P.; Paiva, H.; Salonen, J.T.; Lakka, T.A.; Lehtimaki, T.; Laakso, J.; Laaksonen, R. Risk of acute coronary events and serum concentration of asymmetrical dimethylarginine. Lancet 2001, 358, 2127–2128. [Google Scholar] [CrossRef]
- Meinitzer, A.; Seelhorst, U.; Wellnitz, B.; Halwachs-Baumann, G.; Boehm, B.O.; Winkelmann, B.R.; Marz, W. Asymmetrical dimethylarginine independently predicts total and cardiovascular mortality in individuals with angiographic coronary artery disease (the Ludwigshafen Risk and Cardiovascular Health study). Clin. Chem. 2007, 53, 273–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bode-Boger, S.M.; Scalera, F.; Kielstein, J.T.; Martens-Lobenhoffer, J.; Breithardt, G.; Fobker, M.; Reinecke, H. Symmetrical dimethylarginine: A new combined parameter for renal function and extent of coronary artery disease. J. Am. Soc. Nephrol. 2006, 17, 1128–1134. [Google Scholar] [CrossRef]
- Pernow, J.; Jung, C. Arginase as a potential target in the treatment of cardiovascular disease: Reversal of arginine steal? Cardiovasc. Res. 2013, 98, 334–343. [Google Scholar] [CrossRef] [Green Version]
- Durante, W.; Johnson, F.K.; Johnson, R.A. Arginase: A critical regulator of nitric oxide synthesis and vascular function. Clin. Exp. Pharmacol. Physiol. 2007, 34, 906–911. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, R.B.; Toque, H.A.; Narayanan, S.P.; Caldwell, R.W. Arginase: An old enzyme with new tricks. Trends Pharmacol. Sci. 2015, 36, 395–405. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.; Parnham, S.; Liang, Z.; Perry, R.; Bradbrook, C.; Smith, E.; Faull, R.; Woodman, R.J.; Nucifora, G.; Gleadle, J.M.; et al. Prognostic Utility of Oxygen-Sensitive Cardiac Magnetic Resonance Imaging in Diabetic and Nondiabetic Chronic Kidney Disease Patients With No Known Coronary Artery Disease. JACC Cardiovasc. Imaging 2019, 12, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Sree Raman, K.; Walls, A.; Woodman, R.J.; Faull, R.; Gleadle, J.M.; Selvanayagam, J.B. Gadolinium-Free Cardiovascular Magnetic Resonance Stress T1 Mapping in Patients With Chronic Kidney Disease. JACC Cardiovasc. Imaging 2019, 12, 2083–2085. [Google Scholar] [CrossRef] [PubMed]
- Karamitsos, T.D.; Leccisotti, L.; Arnold, J.R.; Recio-Mayoral, A.; Bhamra-Ariza, P.; Howells, R.K.; Searle, N.; Robson, M.D.; Rimoldi, O.E.; Camici, P.G.; et al. Relationship between regional myocardial oxygenation and perfusion in patients with coronary artery disease: Insights from cardiovascular magnetic resonance and positron emission tomography. Circ. Cardiovasc. Imaging 2010, 3, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muntner, P.; He, J.; Astor, B.C.; Folsom, A.R.; Coresh, J. Traditional and nontraditional risk factors predict coronary heart disease in chronic kidney disease: Results from the atherosclerosis risk in communities study. J. Am. Soc. Nephrol. 2005, 16, 529–538. [Google Scholar] [CrossRef] [Green Version]
- Menon, V.; Greene, T.; Wang, X.; Pereira, A.A.; Marcovina, S.M.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Sarnak, M.J. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005, 68, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Kestenbaum, B.; Sampson, J.N.; Rudser, K.D.; Patterson, D.J.; Seliger, S.L.; Young, B.; Sherrard, D.J.; Andress, D.L. Serum phosphate levels and mortality risk among people with chronic kidney disease. J. Am. Soc. Nephrol. 2005, 16, 520–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham-Brown, M.P.; March, D.S.; Churchward, D.R.; Stensel, D.J.; Singh, A.; Arnold, R.; Burton, J.O.; McCann, G.P. Novel cardiac nuclear magnetic resonance method for noninvasive assessment of myocardial fibrosis in hemodialysis patients. Kidney Int. 2016, 90, 835–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutherford, E.; Talle, M.A.; Mangion, K.; Bell, E.; Rauhalammi, S.M.; Roditi, G.; McComb, C.; Radjenovic, A.; Welsh, P.; Woodward, R.; et al. Defining myocardial tissue abnormalities in end-stage renal failure with cardiac magnetic resonance imaging using native T1 mapping. Kidney Int. 2016, 90, 845–852. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, M.G.; Karamitsos, T.D. Oxygenation-sensitive cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2013, 15, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallavollita, J.A.; Malm, B.J.; Canty, J.M., Jr. Hibernating myocardium retains metabolic and contractile reserve despite regional reductions in flow, function, and oxygen consumption at rest. Circ. Res. 2003, 92, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Fliser, D.; Kronenberg, F.; Kielstein, J.T.; Morath, C.; Bode-Boger, S.M.; Haller, H.; Ritz, E. Asymmetric dimethylarginine and progression of chronic kidney disease: The mild to moderate kidney disease study. J. Am. Soc. Nephrol. 2005, 16, 2456–2461. [Google Scholar] [CrossRef] [Green Version]
- Ravani, P.; Tripepi, G.; Malberti, F.; Testa, S.; Mallamaci, F.; Zoccali, C. Asymmetrical dimethylarginine predicts progression to dialysis and death in patients with chronic kidney disease: A competing risks modeling approach. J. Am. Soc. Nephrol. 2005, 16, 2449–2455. [Google Scholar] [CrossRef] [PubMed]
- Hanai, K.; Babazono, T.; Nyumura, I.; Toya, K.; Tanaka, N.; Tanaka, M.; Ishii, A.; Iwamoto, Y. Asymmetric dimethylarginine is closely associated with the development and progression of nephropathy in patients with type 2 diabetes. Nephrol. Dial. Transplant. 2009, 24, 1884–1888. [Google Scholar] [CrossRef] [Green Version]
- Kielstein, J.T.; Boger, R.H.; Bode-Boger, S.M.; Frolich, J.C.; Haller, H.; Ritz, E.; Fliser, D. Marked increase of asymmetric dimethylarginine in patients with incipient primary chronic renal disease. J. Am. Soc. Nephrol. 2002, 13, 170–176. [Google Scholar] [PubMed]
- Zoccali, C.; Bode-Boger, S.; Mallamaci, F.; Benedetto, F.; Tripepi, G.; Malatino, L.; Cataliotti, A.; Bellanuova, I.; Fermo, I.; Frolich, J.; et al. Plasma concentration of asymmetrical dimethylarginine and mortality in patients with end-stage renal disease: A prospective study. Lancet 2001, 358, 2113–2117. [Google Scholar] [CrossRef]
- Shafi, T.; Hostetter, T.H.; Meyer, T.W.; Hwang, S.; Hai, X.; Melamed, M.L.; Banerjee, T.; Coresh, J.; Powe, N.R. Serum Asymmetric and Symmetric Dimethylarginine and Morbidity and Mortality in Hemodialysis Patients. Am. J. Kidney Dis. 2017, 70, 48–58. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analyte | RT (min) | MSE Channel | Ion | m/z1 | Int Std | QClow 2 %CV | QChigh 2 %CV |
|---|---|---|---|---|---|---|---|
| ADMA | 11.93 | 1 | Parent | 203.16 | d6-ADMA | 6.4 | 7.1 |
| L-ARG | 11.06 | 1 | Parent | 175.13 | d4-HMA | 9.0 | 10.0 |
| CIT | 9.34 | 1 | Fragment | 159.09 | d7-CIT | 6.1 | 4.0 |
| HMA | 11.15 | 1 | Parent | 189.15 | d4-HMA | 1.6 | 1.4 |
| L-NMMA | 11.38 | 1 | Parent | 189.15 | d4-HMA | 8.6 | 14.4 |
| ORNITHINE | 11.38 | 1 | Parent | 133.11 | d6-ORN | 5.1 | 3.5 |
| SDMA | 11.75 | 1 | Parent | 203.16 | d6-SDMA | 4.2 | 4.3 |
| CKD Patients (n = 38) | |
|---|---|
| Age (years) | 62.2 ± 13.5 |
| Male sex | 24 (63.2) |
| BMI (kg/m2) | 31.1 ± 7.4 |
| eGFR (mL/min/1.73 m2) | 15.1 ± 8.5 |
| Dialysis | 16 (42.1) |
| Diabetes Mellitus | 20 (52.6) |
| LVEF (%) | 62.3 ± 11.7 |
| LVMi (g/m2) | 61.7 ± 18.6 |
| Dyslipidemia | 12 (31.6) |
| Smoking History | 8 (21.1) |
| Anti-platelet Agent | 15 (39.5) |
| Beta blocker | 16 (42.1) |
| ACE inhibitor | 10 (26.3) |
| Angiotensin Receptor Blocker | 10 (26.3) |
| Calcium channel blocker | 19 (50.0) |
| Statin | 23 (60.5) |
| Analyte | Normal Volunteers (Pooled Plasma of 5 Healthy Volunteers) | CKD Patients (n = 38) | p-Value 1 |
|---|---|---|---|
| ADMA (µM) | 0.505 | 0.780 ± 0.149 | <0.001 |
| L-ARG (µM) | 213.8 | 182.7 ± 39.6 | <0.001 |
| CIT (µM) | 42.6 | 96.7 ± 29.0 | <0.001 |
| HMA (µM) | 2.40 | 1.28 ± 0.61 | <0.001 |
| L-NMMA (µM) | 0.115 | 0.101 ± 0.041 | 0.042 |
| ORN (µM) | 71.1 | 84.7 ± 22.5 | 0.001 |
| SDMA (µM) | 0.505 | 1.784 ± 0.669 | <0.001 |
| Analyte | OS-CMR (n = 38) | T1 Mapping (n = 30) | ||
|---|---|---|---|---|
| r-Value | p-Value | r-Value | p-Value | |
| ADMA (µM) | −0.106 | 0.558 | −0.419 | 0.037 |
| L-ARG (µM) | −0.183 | 0.308 | −0.338 | 0.098 |
| CIT (µM) | −0.102 | 0.573 | −0.444 | 0.026 |
| HMA (µM) | −0.164 | 0.362 | 0.000 | 0.999 |
| L-NMMA (µM) | 0.078 | 0.666 | −0.002 | 0.992 |
| ORN (µM) | −0.156 | 0.387 | −0.460 | 0.021 |
| SDMA (µM) | −0.226 | 0.206 | −0.080 | 0.702 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, R.J.; Tommasi, S.; Faull, R.; Gleadle, J.M.; Mangoni, A.A.; Selvanayagam, J.B. Arginine Metabolites as Biomarkers of Myocardial Ischaemia, Assessed with Cardiac Magnetic Resonance Imaging in Chronic Kidney Disease. Biomolecules 2021, 11, 416. https://doi.org/10.3390/biom11030416
Shah RJ, Tommasi S, Faull R, Gleadle JM, Mangoni AA, Selvanayagam JB. Arginine Metabolites as Biomarkers of Myocardial Ischaemia, Assessed with Cardiac Magnetic Resonance Imaging in Chronic Kidney Disease. Biomolecules. 2021; 11(3):416. https://doi.org/10.3390/biom11030416
Chicago/Turabian StyleShah, Ranjit J., Sara Tommasi, Randall Faull, Jonathan M. Gleadle, Arduino A. Mangoni, and Joseph B. Selvanayagam. 2021. "Arginine Metabolites as Biomarkers of Myocardial Ischaemia, Assessed with Cardiac Magnetic Resonance Imaging in Chronic Kidney Disease" Biomolecules 11, no. 3: 416. https://doi.org/10.3390/biom11030416