
Association between Thyroid Function and Ocular Parameters

 ,
,  , , , and
, , , and
Abstract
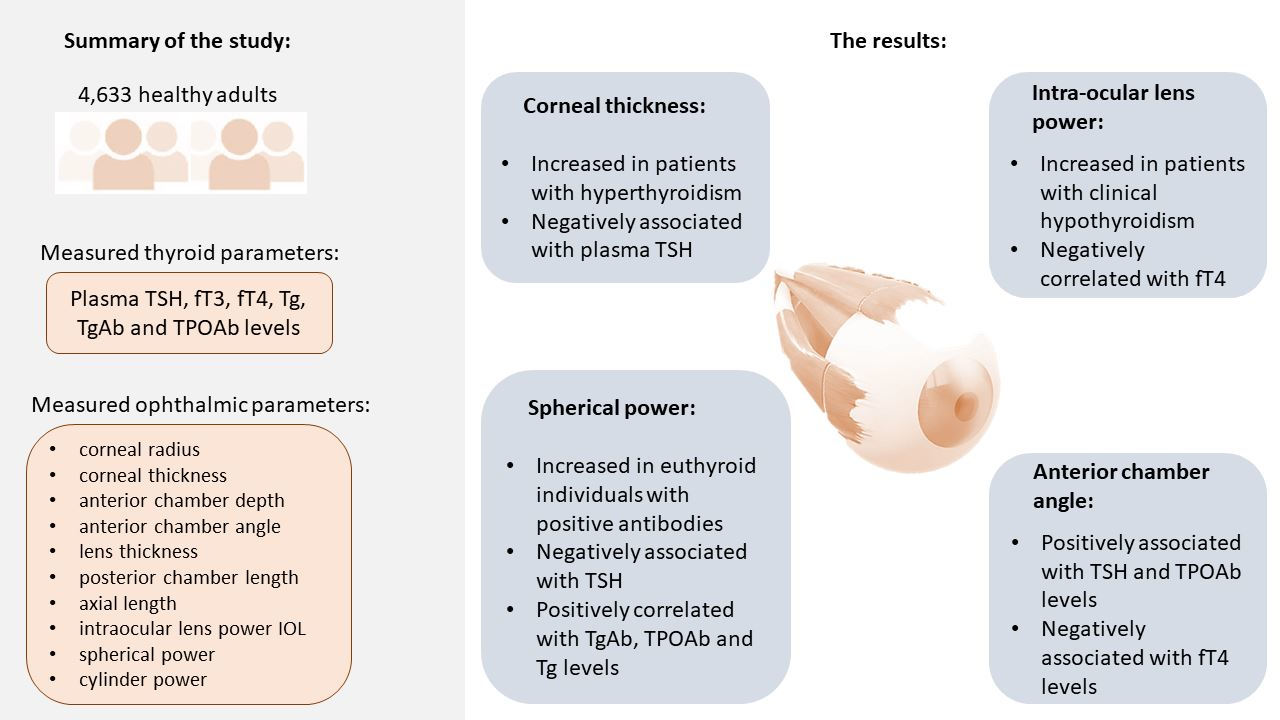
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Biochemical Measurements
2.3. Measurement of Ocular Parameters
2.4. Definitions
2.5. Statistical Analyses
3. Results
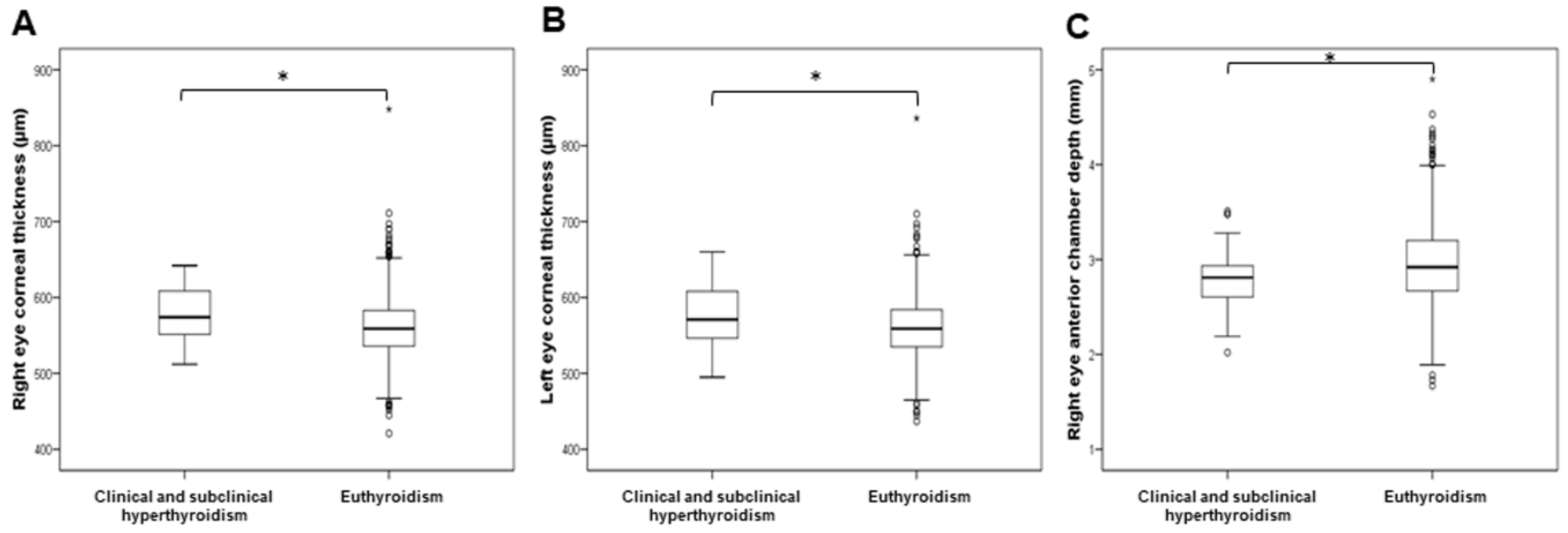
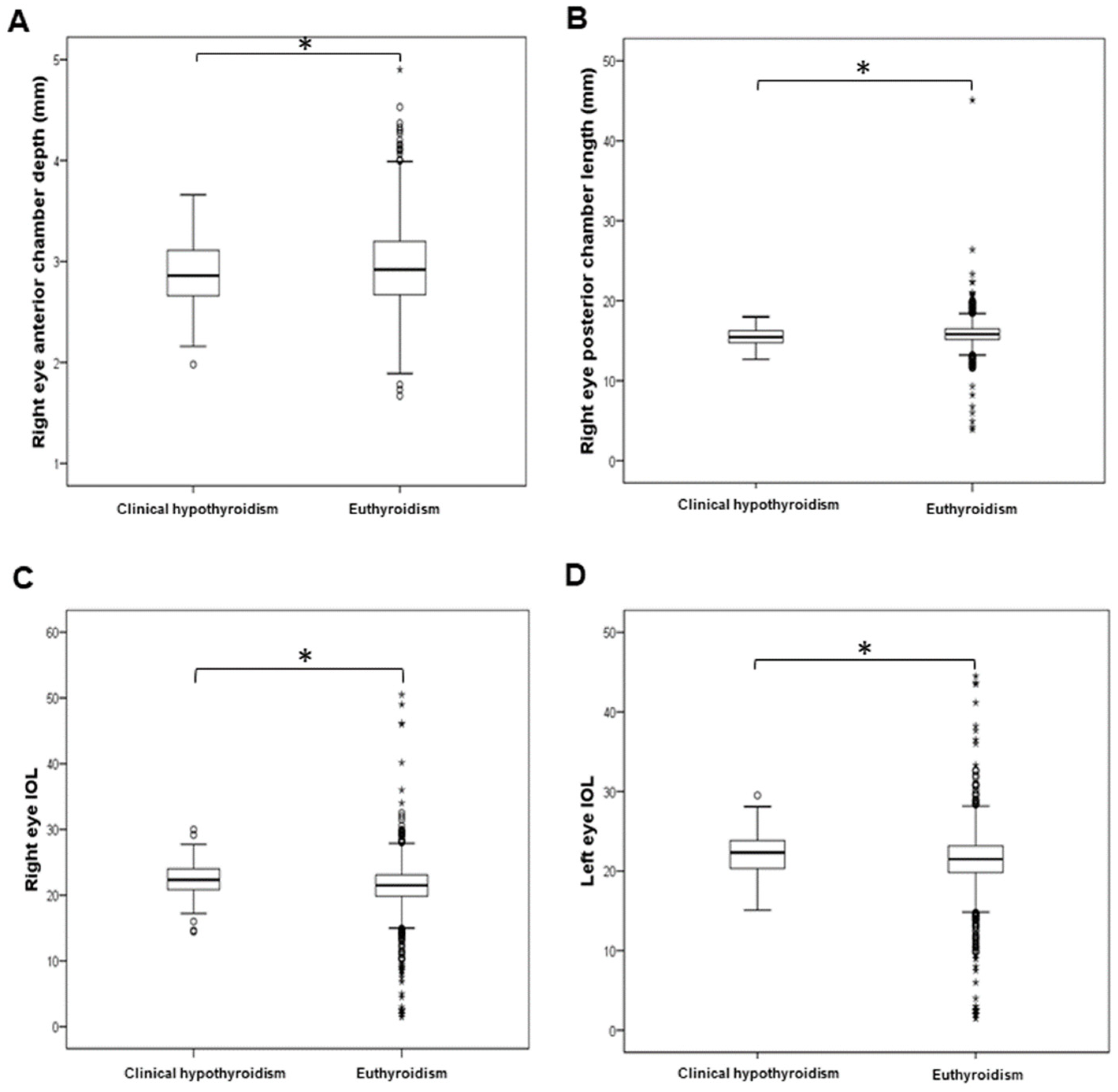
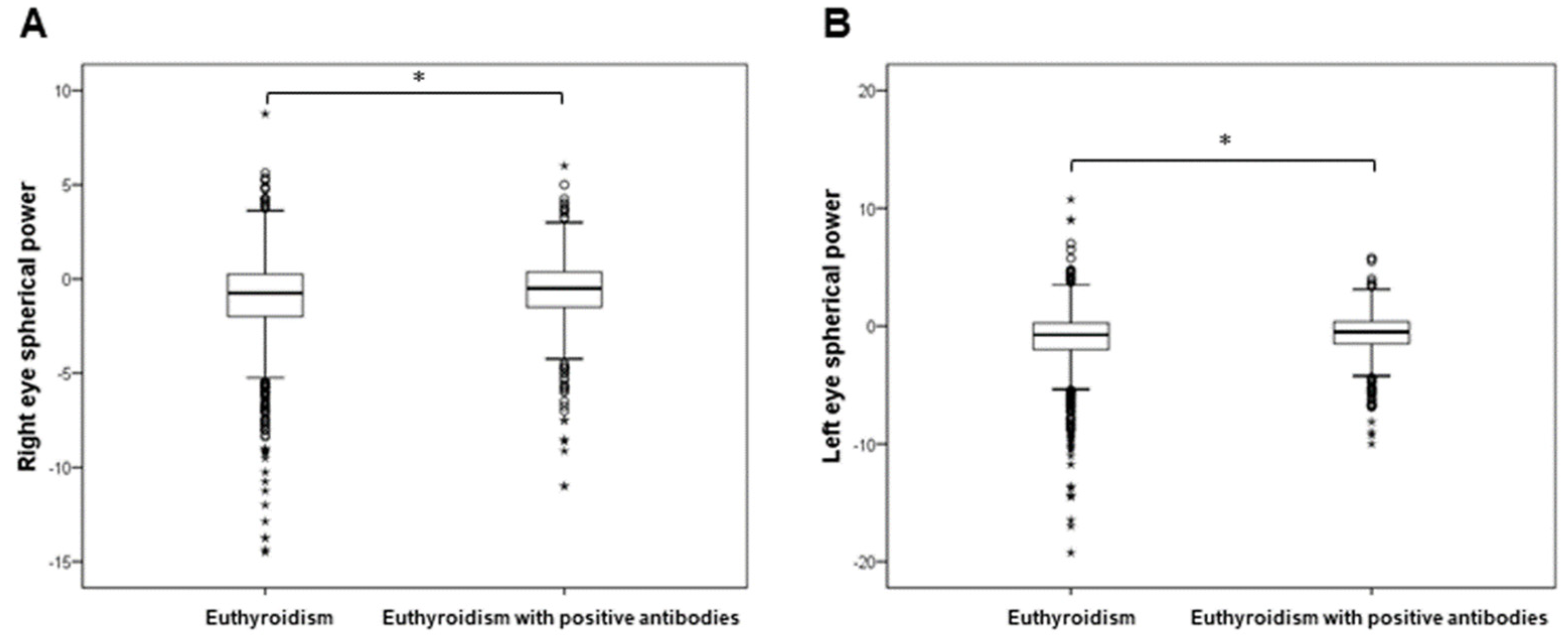
3.1. Comparison of Ocular Parameters between Individuals with Euthyroidism and Individuals with Altered Thyroid Function
3.2. Principal Component Analysis of Ocular Parameters
3.3. The Effect of TSH, Thyroid Hormones, Tg, TgAb, and TPOAb on the Eye
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Williams, G.R. Neurodevelopmental and neurophysiological actions of thyroid hormone. J. Neuroendocrinol. 2008, 20, 784–794. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J. Thyroid Hormones in Brain Development and Function. Endotext; Feingold, K., Anawalt, B., Boyce, A., Sur, I., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2022. [Google Scholar]
- Ludwig, P.E.; Lopez, M.J.; Czyz, C.N. Embryology, Eye Malformations; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- McNerney, C.; Johnston, R.J. Thyroid hormone signaling specifies cone photoreceptor subtypes during eye development: Insights from model organisms and human stem cell-derived retinal organoids. Vitam. Horm. 2021, 116, 51–90. [Google Scholar] [CrossRef] [PubMed]
- Bahn, R.S. Graves’ Ophthalmopathy. N. Engl. J. Med. 2010, 362, 726–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thvilum, M.; Brandt, F.; Brix, T.H.; Hegedüs, L. The interrelation between hypothyroidism and glaucoma: A critical review and meta-analyses. Acta Ophthalmol. 2017, 95, 759–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozturk, B.T.; Kerimoglu, H.; Dikbas, O.; Pekel, H.; Gonen, M.S. Ocular changes in primary hypothyroidism. BMC Res. Notes 2009, 2, 266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.; Tevaarwerk, G.; Allen, L. An ocular dynamic study supporting the hypothesis that hypothyroidism is a treatable cause of secondary open-angle glaucoma. Can. J. Ophthalmol. 1992, 27, 341–344. [Google Scholar] [PubMed]
- Kan, E.; Kiliçkan, E.; Ecemiş, G.; Beyazyildiz, E.; Çolak, R. Presence of Dry Eye in Patients with Hashimoto’s Thyroiditis. J. Ophthalmol. 2014, 2014, 754923. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Baek, S. Dry eye syndrome in thyroid eye disease patients: The role of increased incomplete blinking and Meibomian gland loss. Acta Ophthalmol. 2019, 97, e800–e806. [Google Scholar] [CrossRef]
- Rudan, I.; Marušić, A.; Janković, S.; Rotim, K.; Boban, M.; Lauc, G.; Grković, I.; Dogaš, Z.; Zemunik, T.; Vatavuk, Z.; et al. “10 001 Dalmatians”: Croatia Launches Its National Biobank. Croat. Med. J. 2009, 50, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Paharia, N.; Arora, I.; Agrawal, N.; Mathur, A.; Agrawal, S. Comparative Clinicopathological Evaluation of the Ocular Surface in Newly Diagnosed Patients of Hyperthyroidism and Hypothyroidism Compared to Healthy Subjects. Cureus 2022, 14, e23890. [Google Scholar] [CrossRef]
- Kanellopoulos, A.J.; Asimellis, G. In vivo 3-dimensional corneal epithelial thickness mapping as an indicator of dry eye: Preliminary clinical assessment. Am. J. Ophthalmol. 2014, 157, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Abou Shousha, M.; Wang, J.; Kontadakis, G.; Feuer, W.; Canto, A.P.; Hoffmann, R.; Perez, V.L. Corneal epithelial thickness profile in dry-eye disease. Eye 2019, 34, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Karabulut, G.O.; Kaynak, P.; Altan, C.; Ozturker, C.; Aksoy, E.F.; Demirok, A.; Yilmaz, O.F. Corneal biomechanical properties in thyroid eye disease. Kaohsiung J. Med. Sci. 2014, 30, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Moghimi, S.; Safizadeh, M.; Mazloumi, M.; Hosseini, H.; Vahedian, Z.; Rajabi, M.T. Evaluation of Corneal Biomechanical Properties in Patients With Thyroid Eye Disease Using Ocular Response Analyzer. J. Glaucoma 2016, 25, 269–273. [Google Scholar] [CrossRef]
- Kırgız, A.; Çabuk, K.Ş.; Yetmis, M.; Atalay, K. Corneal biomechanical properties in patients with Hashimoto’s thyroiditis. Adv. Clin. Exp. Med. 2019, 28, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Okan Olcaysü, O.; Karasu, B.; Olcaysü, E.; Çayır, A.; Rıza Cenk Çelebi, A. Alterations of Neuroretinal and Corneal Thickness in Hashimoto’s Thyroiditis. Acıbadem Üniversitesi Sağlık Bilim. Derg. 2022, 13, 234–240. [Google Scholar] [CrossRef]
- Bahceci, U.A.; Ozdek, S.; Pehlivanli, Z.; Yetkin, I.; Onol, M. Changes in intraocular pressure and corneal and retinal nerve fiber layer thicknesses in hypothyroidism. Eur. J. Ophthalmol. 2005, 15, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Roszkowska, A.M.; Alessandrello, F.; Waśniewska, M.; Tropeano, A.; Gargano, R.; Aragona, P. Is keratoconus associated to thyroid diseases? Assessment of the corneal parameters in patients with congenital hypothyroidism. Eur. J. Ophthalmol. 2022, 32, 31–35. [Google Scholar] [CrossRef]
- Bassiouny, R.M.; Awad, E.A.; Gaafar, W.; Kyrillos, F.A.; Samra, W.A.A.; Abdelhameed, A.G. Corneal Tomographic Analysis Among Patients With Thyroid Gland Dysfunction. J. Refract. Surg. 2021, 37, 192–197. [Google Scholar] [CrossRef]
- Villani, E.; Viola, F.; Sala, R.; Salvi, M.; Mapelli, C.; Currò, N.; Vannucchi, G.; Beck-Peccoz, P.; Ratiglia, R. Corneal Involvement in Graves’ Orbitopathy: An In Vivo Confocal Study. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4574–4578. [Google Scholar] [CrossRef]
- Allam, I.Y.; Lazreg, S.; Shaheen, M.S.; Doheim, M.F.; Mohammed, M.A. Ocular Surface Changes in Patients with Thyroid Eye Disease: An Observational Clinical Study. Clin. Ophthalmol. 2021, 15, 2481–2488. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Wu, D.; Yu, F.; Hong, S.; Ye, J.; Wang, C.; Li, Y.; Du, M.; Xiao, H.; Wan, P. Corneal Endothelium: A Promising Quantitative Index for Graves Ophthalmopathy Activity Evaluation. Am. J. Ophthalmol. 2021, 230, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Seyrek, F.N.C.; Başer, H.; Uğurlu, N.; Yülek, F.; Ersoy, R.; Çağil, N.; Çakir, B. Evaluation of the central corneal thickness, retinal thickness and intraocular pressure in patients with euthyroid Hashimoto’s thyroiditis. Gulhane Med. J. 2019, 61, 41–45. [Google Scholar] [CrossRef]
- Costantini, E.; Touzeau, O.; Gaujoux, T.; Basli, E.; Kopito, R.; Borderie, V.M.; Laroche, L. Age-Related Changes in Central and Peripheral Corneal Thickness. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5107. [Google Scholar]
- Rieth, S.; Engel, F.; Bühner, E.; Uhlmann, S.; Wiedemann, P.; Foja, C. Comparison of data from the rostock cornea module of the heidelberg retina tomograph, the oculus pentacam, and the endothelial cell microscope. Cornea 2010, 29, 314–320. [Google Scholar] [CrossRef]
- Galgauskas, S.; Juodkaite, G.; Tutkuviene, J. Age-related changes in central corneal thickness in normal eyes among the adult Lithuanian population. Clin. Interv. Aging 2014, 9, 1145. [Google Scholar] [CrossRef] [Green Version]
- Vitályos, G.; Kolozsvári, B.L.; Németh, G.; Losonczy, G.; Hassan, Z.; Pásztor, D.; Fodor, M. Effects of aging on corneal parameters measured with Pentacam in healthy subjects. Sci. Rep. 2019, 9, 3419. [Google Scholar] [CrossRef] [Green Version]
- Colakoglu, A.; Cosar, C.B. Age-Related Changes in Corneal Epithelial Thickness Measured with an Ultrasound Pachymeter. Clin. Interv. Aging 2022, 17, 1461–1470. [Google Scholar] [CrossRef]
- Kiely, P.M.; Carney, L.G.; Smith, G. Menstrual cycle variations of corneal topography and thickness. Am. J. Optom. Physiol. Opt. 1983, 60, 822–829. [Google Scholar] [CrossRef] [Green Version]
- Tabibian, D.; de Tejada, B.M.; Gatzioufas, Z.; Kling, S.; Meiss, V.S.; Boldi, M.O.; Othenin-Girard, V.; Chilin, A.; Lambiel, J.; Hoogewoud, F.; et al. Pregnancy-induced Changes in Corneal Biomechanics and Topography Are Thyroid Hormone Related. Am. J. Ophthalmol. 2017, 184, 129–136. [Google Scholar] [CrossRef]
- Tripathy, D.; Rao, A.; Banerjee, A.; Padhy, D. Case Report: Aqueous misdirection in thyroid eye disease. BMJ Case Rep. 2014, 2014, bcr2014205824. [Google Scholar] [CrossRef] [PubMed]
- Senthilkumar, V.A.; Pradhan, C.; Dosapati, S.; Krishnadas, R. Unilateral acute secondary angle-closure glaucoma in active thyroid eye disease. Indian J. Ophthalmol.—Case Rep. 2021, 1, 505. [Google Scholar] [CrossRef]
- Lam, C.C.; Chong, K.K. Spontaneous intercalated corneal epithelial folds in thyroid eye disease: A case report. Hong Kong J. Ophthalmol. 2020, 24, 60–62. [Google Scholar] [CrossRef]
- Lee, J.S.; Yeom, D.J.; Nah, S.K.; Kim, B.Y.; Jang, S.Y. Changes in the Ocular Parameters of Patients with Graves’ Disease after Antithyroid Drug Treatment. Medicina 2021, 57, 414. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD or Median (25–75th Percentile) | Number of Participants |
|---|---|---|
| Age | 55 (42–66) | 4578 |
| TSH (mIU/L) | 1.6 (1.1–2.5) | 4420 |
| fT4 (pmol/L) | 12.9 (11.9–14.1) | 4424 |
| fT3 (pmol/L) | 4.4 (4.2–4.8) | 4395 |
| Tg (ng/mL) | 10.1 (5.5–16.8) | 3491 |
| TgAb (IU/mL) | 8.5 (5–19.2) | 4427 |
| TPOAb (IU/mL) | 4.4 (1.7–11.6) | 4426 |
| Right eye: posterior chamber length (mm) | 15.8 (15.2–16.5) | 3931 |
| Right eye: axial length (mm) | 23.1 ± 1.3 | 3933 |
| Right eye: IOL (D) | 21.5 (19.8–23.1) | 3887 |
| Right eye: corneal thickness (µm) | 560.1 ± 36.2 | 3919 |
| Right eye: lens thickness (mm) | 4.4 ± 0.5 | 3903 |
| Right eye: cylinder power (°) | −0.284 ± 0.922 | 3910 |
| Right eye: spherical power (D) | −0.620 (−1.750–0.250) | 3902 |
| Right eye: anterior chamber angle (°) | 88.5 ± 57.1 | 3331 |
| Right eye: anterior chamber depth (mm) | 2.9 ± 0.4 | 3933 |
| Right eye: corneal radius (mm) | 7.8 ± 0.3 | 2257 |
| Left eye: posterior chamber length (mm) | 15.9 ± 1.2 | 3921 |
| Left eye: axial length (mm) | 23.1 (22.4–23.7) | 3929 |
| Left eye: IOL (D) | 21.6 (19.8–23.2) | 3891 |
| Left eye: corneal thickness (µm) | 560.4 ± 36.2 | 3908 |
| Left eye: lens thickness (mm) | 4.4 ± 0.4 | 3904 |
| Left eye: cylinder power (°) | −0.294 ± 1.291 | 3916 |
| Left eye: spherical power (D) | −0.620 (−1.870–0.250) | 3916 |
| Left eye: anterior chamber angle (°) | 89.1 ± 58.6 | 3329 |
| Left eye: anterior chamber depth (mm) | 2.9 ± 0.4 | 3929 |
| Left eye: corneal radius (mm) | 7.8 (7.6–8) | 2272 |
| Factors | Ocular Parameters (Factor Loadings) |
|---|---|
| Factor 1 | Right eye: posterior chamber length (0.636), right eye: axial length (0.736), right eye: IOL (−0.746), left eye: posterior chamber length (0.710), left eye: axial length (0.715), left eye: IOL (−0.744) |
| Factor 2 | Right eye: corneal thickness (0.939), left eye: corneal thickness (0.944) |
| Factor 3 | Right eye: lens thickness (0.712), left eye: lens thickness (0.695) |
| Factor 4 | Right eye: cylinder power (0.702), left eye: cylinder power (0.654) |
| Factor 5 | Right eye: spherical power (0.542), left eye: spherical power (0.578) |
| Factor 6 | Right eye: anterior chamber depth (0.512), left eye: anterior chamber depth (0.575) |
| Factor 7 | Right eye: anterior chamber angle (0.672), left eye: anterior chamber angle (0.726) |
| Factor 2—Corneal Thickness | Factor 3—Lens Thickness | Factor 7—Anterior Chamber Angle | |
|---|---|---|---|
| TSH | β = −0.043 * | β = 0.042 * | |
| fT4 | β = −0.035 * | ||
| Tg | β = 0.050 ** | ||
| TPOAb | β = 0.038 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babić Leko, M.; Pleić, N.; Lešin, M.; Gunjača, I.; Torlak, V.; Škunca Herman, J.; Vatavuk, Z.; Punda, A.; Polašek, O.; Hayward, C.; et al. Association between Thyroid Function and Ocular Parameters. Biology 2022, 11, 1847. https://doi.org/10.3390/biology11121847
Babić Leko M, Pleić N, Lešin M, Gunjača I, Torlak V, Škunca Herman J, Vatavuk Z, Punda A, Polašek O, Hayward C, et al. Association between Thyroid Function and Ocular Parameters. Biology. 2022; 11(12):1847. https://doi.org/10.3390/biology11121847
Chicago/Turabian StyleBabić Leko, Mirjana, Nikolina Pleić, Mladen Lešin, Ivana Gunjača, Vesela Torlak, Jelena Škunca Herman, Zoran Vatavuk, Ante Punda, Ozren Polašek, Caroline Hayward, and et al. 2022. "Association between Thyroid Function and Ocular Parameters" Biology 11, no. 12: 1847. https://doi.org/10.3390/biology11121847