
Ambient PM2.5 and Daily Hospital Admissions for Acute Respiratory Infections: Effect Modification by Weight Status of Child

 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Materials and Methods
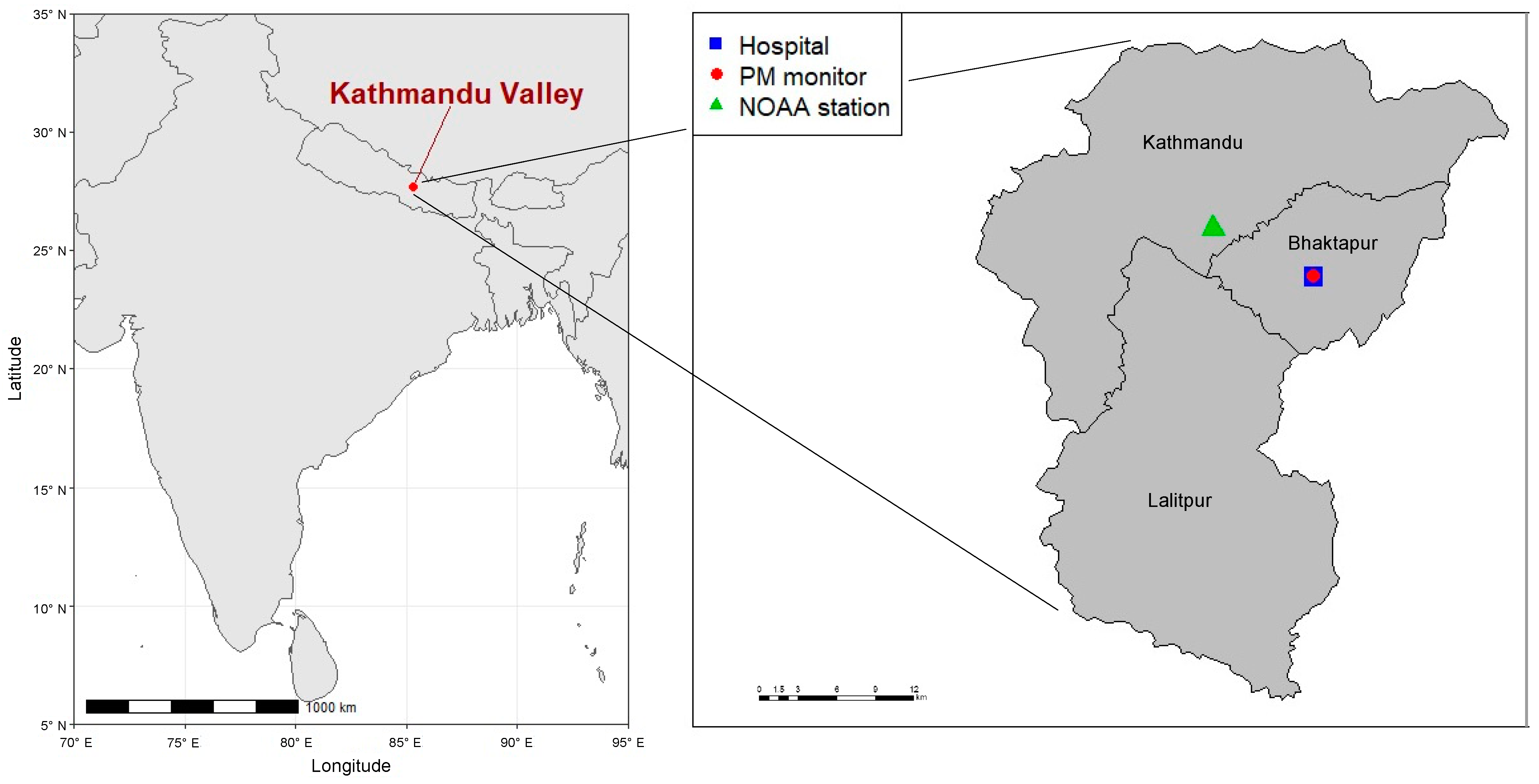
2.1. Study Site
2.2. Study Design
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Descriptive Summary
3.2. Main Results
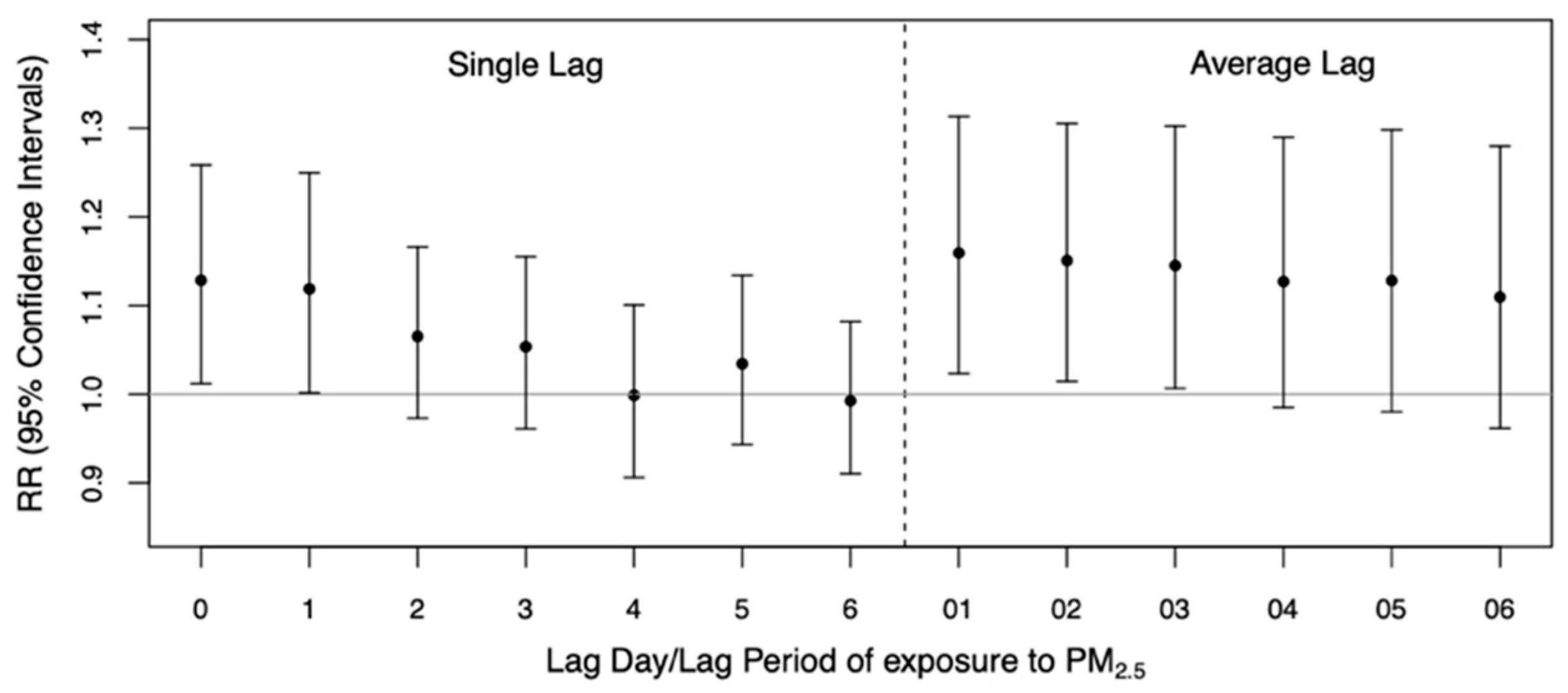
3.2.1. Results for All ARI Admissions
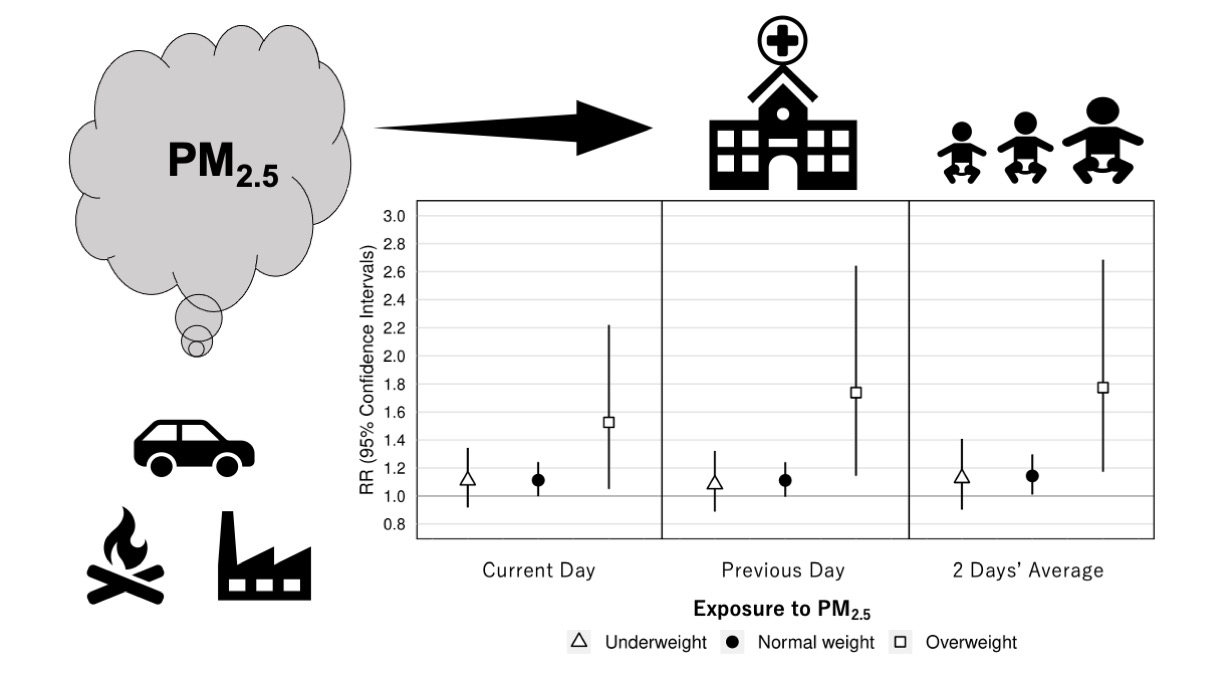
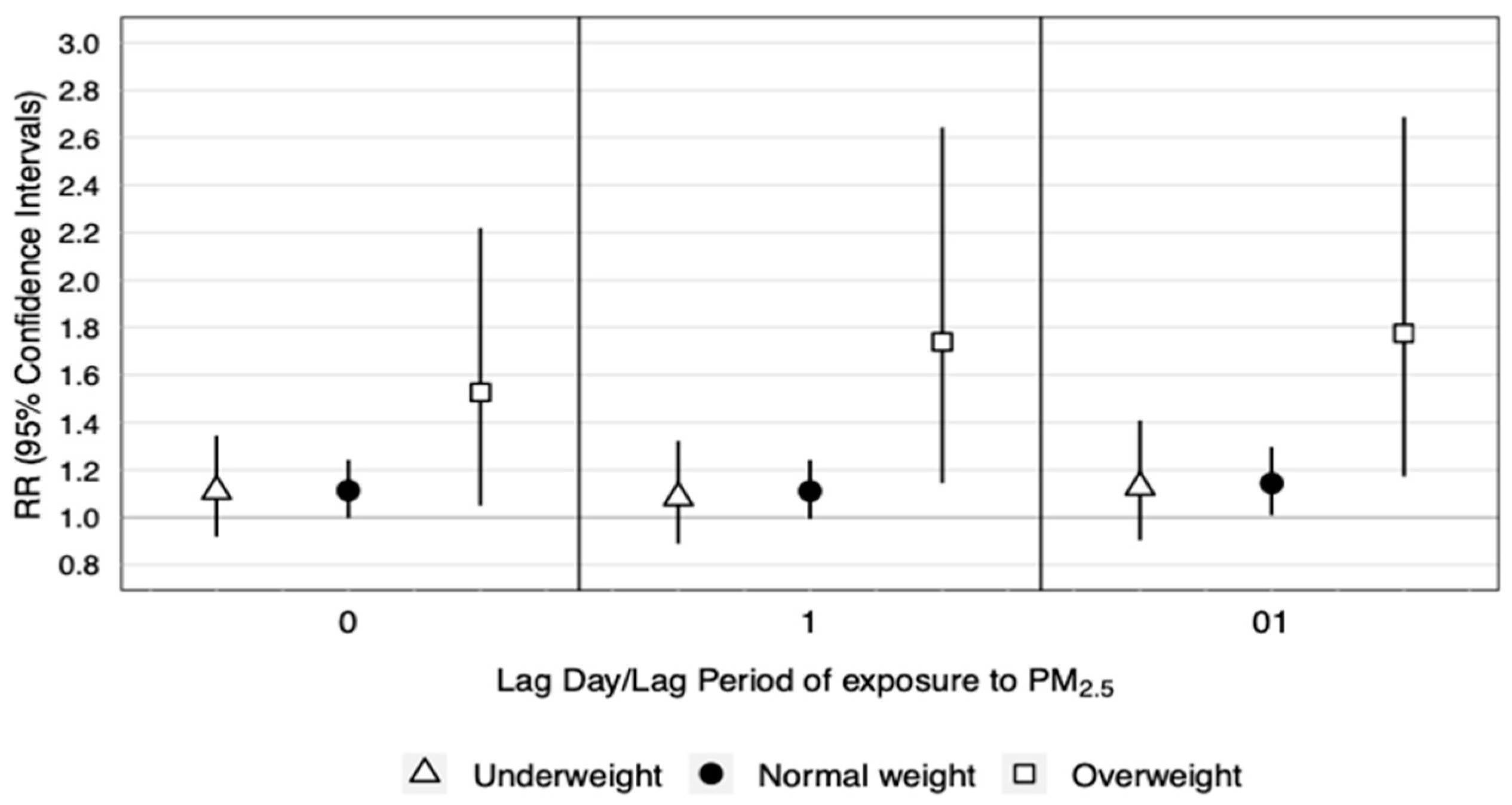
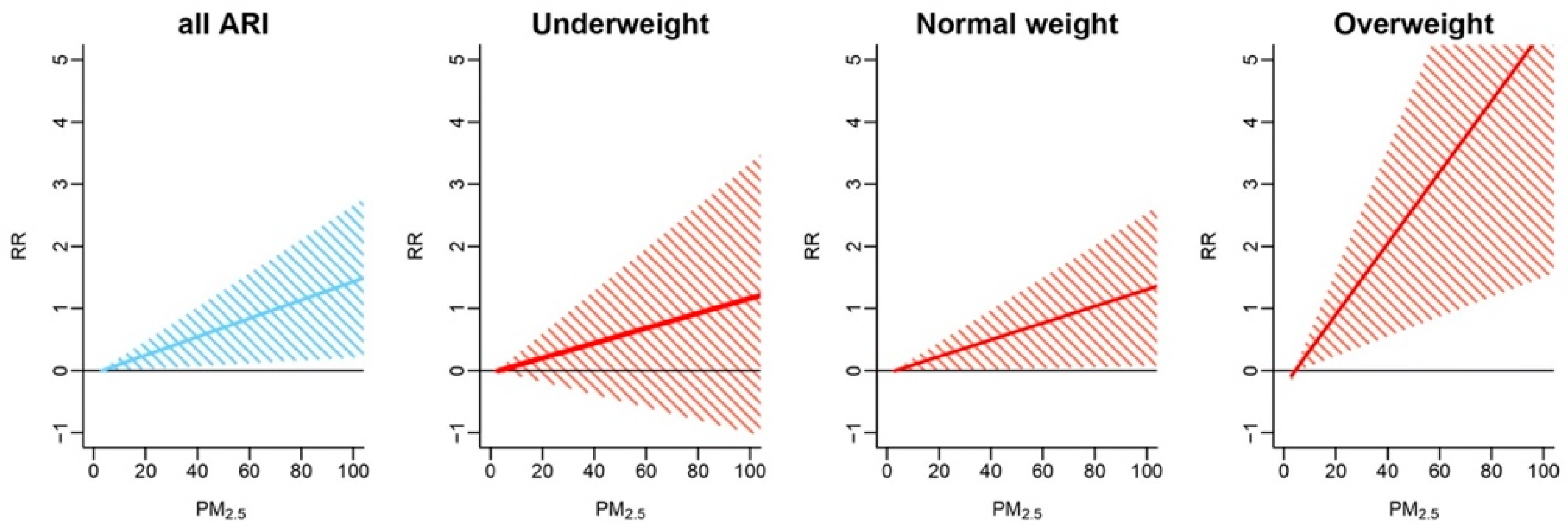
3.2.2. Results by Weight Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide—Global Update 2005; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Gurung, A.; Bell, M.L. The state of scientific evidence on air pollution and human health in Nepal. Environ. Res. 2013, 124, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Peng, R.D.; Bell, M.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, A.; Dockery, D.; Muller, J.E.; Mittleman, M. Increased particulate air pollution and the triggering of myocardial infarction. Circulation 2001, 103, 2810–2815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, C.A.; Muhlestein, J.B.; May, H.T.; Renlund, D.G.; Anderson, J.L.; Horne, B.D. Ischemic heart disease events triggered by short-term exposure to fine particulate air pollution. Circulation 2006, 114, 2443–2448. [Google Scholar] [CrossRef] [Green Version]
- Gurung, A.; Bell, M.L. Exposure to airborne particulate matter in Kathmandu Valley, Nepal. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 235–242. [Google Scholar] [CrossRef]
- UNEP. Young and Old, Air Pollution Affects the Most Vulnerable; UN Environment Programme: Nairobi, Kenya, 2018; Available online: www.unenvironment.org/news-and-stories/blogpost/young-and-old-air-pollution-affects-most-vulnerable (accessed on 4 August 2021).
- WHO. World Health Statistics 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Nascimento, A.P.; Santos, J.M.; Mill, J.G.; de Souza, J.B.; Reis, N.C.J.; Reisen, V.A. Association between the concentration of fine particles in the atmosphere and acute respiratory diseases in children. Rev. Saúde Pública 2017, 51, 3. [Google Scholar] [CrossRef] [Green Version]
- Horne, B.D.; Joy, E.A.; Hofmann, M.G.; Gesteland, P.H.; Cannon, J.B.; Lefler, J.; Blagev, D.P.; Korgenski, E.K.; Torosyan, N.; Hansen, G.I.; et al. Short-term elevation of fine particulate matter air pollution and acute lower respiratory infection. Am. J. Respir. Crit. Care Med. 2018, 198, 759–766. [Google Scholar] [CrossRef]
- IHME. GBD Country Profile Compare—Nepal; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2017; Available online: www.healthdata.org/nepal (accessed on 4 August 2021).
- Ministry of Health, Nepal; New ERA; ICF. Nepal Demographic and Health Survey 2016; Ministry of Health, Nepal: Kathmandu, Nepal, 2017.
- Bates, M.N.; Chandyo, R.K.; Valentiner-Branth, P.; Pokhrel, A.K.; Mathisen, M.; Basnet, S.; Shrestha, P.S.; Strand, T.A.; Smith, K.R. Acute lower respiratory infection in childhood and household fuel use in Bhaktapur, Nepal. Environ. Health Perspect. 2013, 121, 637–642. [Google Scholar] [CrossRef] [Green Version]
- Levy, D.; Lumley, T.; Sheppard, L.; Kaufman, J.; Checkoway, H. Referent selection in case-crossover analyses of acute health effects of air pollution. Epidemiology 2001, 12, 186–192. [Google Scholar] [CrossRef]
- Lumley, T.; Levy, D. Bias in the case-crossover design: Implications for studies of air pollution. Environmetrics 2000, 11, 689–704. [Google Scholar] [CrossRef]
- Carracedo-Martínez, E.; Taracido, M.; Tobías, A.; Saez, M.; Figueiras, A. Case-crossover analysis of air pollution health effects: A systematic review of methodology and application. Environ. Health Perspect. 2010, 118, 1173–1182. [Google Scholar] [CrossRef]
- Levy, D.; Sheppard, L.; Checkoway, H.; Kaufman, J.; Lumley, T.; Koenig, J.; Siscovick, D. A case-crossover analysis of particulate matter air pollution and out-of-hospital primary cardiac arrest. Epidemiology 2001, 12, 193–199. [Google Scholar] [CrossRef]
- Schwartz, J. The effects of particulate air pollution on daily deaths: A multi-city case crossover analysis. Occup. Environ. Med. 2004, 61, 956–961. [Google Scholar] [CrossRef] [Green Version]
- Szyszkowicz, M.; Kousha, T.; Castner, J. Air pollution and emergency department visits for conjunctivitis: A case-crossover study. Int. J. Occup. Med. Environ. Health 2016, 29, 381–393. [Google Scholar] [CrossRef]
- Maclure, M. The case-crossover design: A method for studying transient effects on the risk of acute events. Am. J. Epidemiol. 1991, 133, 144–153. [Google Scholar] [CrossRef]
- Janes, H.; Sheppard, L.; Lumley, T. Case-crossover analyses of air pollution exposure data: Referent selection strategies and their implications for bias. Epidemiology 2005, 16, 717–726. [Google Scholar] [CrossRef]
- WHO. Growth Reference Data for 5–19 Years; World Health Organization: Geneva, Switzerland, 2007; Available online: www.who.int/growthref/en/ (accessed on 4 August 2021).
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Mei, Z.G.; Grummer-Strawn, L.M. Standard deviation of anthropometric Z-scores as a data quality assessment tool using the 2006 WHO growth standards: A cross country analysis. Bull. World Health Organ. 2007, 85, 441–448. [Google Scholar] [CrossRef]
- Karki, K.B.; Dhakal, P.; Shrestha, S.L.; Joshi, H.D.; Aryal, K.K.; Poudyal, A.; Puri, S.; Verma, S.C.; Pokhrel, A.; Lohani, G.R.; et al. Situation Analysis of Ambient Air Pollution and Respiratory Effects in Kathmandu Valley, 2015; Nepal Health Research Council: Kathmandu, Nepal, 2016. [Google Scholar]
- Armstrong, B.G.; Gasparrini, A.; Tobías, A. Conditional Poisson models: A flexible alternative to conditional logistic case cross-over analysis. BMC Med. Res. Methodol. 2014, 14, 122. [Google Scholar] [CrossRef] [Green Version]
- Alessandrini, E.R.; Faustini, A.; Chiusolo, M.; Stafoggia, M.; Gandini, M.; DeMaria, M.; Antonelli, A.; Arena, P.; Biggeri, A.; Canova, C.; et al. Air pollution and mortality in twenty-five Italian cities: Results of the EpiAir2 project. Epidemiol. Prev. 2013, 37, 220–229. [Google Scholar]
- Baccini, M.; Biggeri, A.; Accetta, G.; Kosatsky, T.; Katsouyanni, K.; Analitis, A.; Anderson, H.R.; Bisanti, L.; D’Ippoliti, D.; Danova, J.; et al. Heat effects on mortality in 15 European cities. Epidemiology 2008, 19, 711–719. [Google Scholar] [CrossRef]
- Ye, X.; Wolff, R.; Yu, W.; Vaneckova, P.; Pan, X.; Tong, S. Ambient temperature and morbidity: A review of epidemiological evidence. Environ. Health Perspect. 2012, 120, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Lessler, J.; Brookmeyer, R.; Reich, N.G.; Nelson, K.E.; Cummings, D.A.T.; Perl, T.M. Identifying the probable timing and setting of respiratory virus infections. Infect. Control. Hosp. Epidemiol. 2010, 31, 809–815. [Google Scholar] [CrossRef]
- Pudpong, N.; Hajat, S. High temperature effects on out-patient visits and hospital admissions in Chiang Mai, Thailand. Sci. Total. Environ. 2011, 409, 5260–5267. [Google Scholar] [CrossRef]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, M.F.; Hod, R.; Nawi, A.M.; Sahani, M. Association between ambient air pollution and childhood respiratory diseases in low- and middle-income Asian countries: A systematic review. Atmos. Environ. 2021, 256, 118422. [Google Scholar] [CrossRef]
- Liu, J.Y.; Li, Y.F.; Li, J.; Liu, Y.; Tao, N.N.; Song, W.M.; Cui, L.L.; Li, H.C. Association between ambient PM2.5 and children’s hospital admissions for respiratory diseases in Jinan, China. Environ. Sci. Pollut. Res. 2019, 26, 24112–24120. [Google Scholar] [CrossRef]
- Karr, C.; Kaufman, J.; Lumley, T.; Davis, R.; Shepherd, K.; Ritz, B.; Larson, T. Effect of ambient air pollution on infant bronchiolitis. Epidemiology 2004, 15, S31–S32. [Google Scholar] [CrossRef]
- Karr, C.; Lumley, T.; Shepherd, K.; Davis, R.; Larson, T.; Ritz, B.; Kaufman, J. A case-crossover study of wintertime ambient air pollution and infant bronchiolitis. Environ. Health Perspect. 2006, 114, 277–281. [Google Scholar] [CrossRef]
- Lu, K.D.; Breysse, P.N.; Diette, G.B.; Curtin-Brosnan, J.; Aloe, C.; Williams, D.L.; Peng, R.D.; McCormack, M.C.; Matsui, E.C. Being overweight increases susceptibility to indoor pollutants among urban children with asthma. J. Allergy Clin. Immunol. 2013, 131, 1017–1023. [Google Scholar] [CrossRef] [Green Version]
- Romieu, I.; Castro-Giner, F.; Künzli, N.; Sunyer, J. Air pollution, oxidative stress and dietary supplementation: A review. Eur. Respir. J. 2008, 31, 179–197. [Google Scholar] [CrossRef]
- Bowler, R.P.; Crapo, J.D. Oxidative stress in allergic respiratory diseases. J. Allergy Clin. Immunol. 2002, 110, 349–356. [Google Scholar] [CrossRef]
- Holguin, F.; Fitzpatrick, A. Obesity, asthma, and oxidative stress. J. Appl. Physiol. 2010, 108, 754–759. [Google Scholar] [CrossRef]
- Keaney, J.F.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.F.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J. Obesity and systemic oxidative stress—Clinical correlates of oxidative stress in the Framingham study. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limaye, S.; Salvi, S. Obesity and asthma: The role of environmental pollutants. Immunol. Allergy Clin. 2014, 34, 839–855. [Google Scholar] [CrossRef]
- Graham, D.R.; Chamberlain, M.J.; Hutton, L.; King, M.; Morgan, W.K. Inhaled particle deposition and body habitus. Occup. Environ. Med. 1990, 47, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Shore, S.A.; Rivera-Sanchez, Y.M.; Schwartzman, I.N.; Johnston, R. Responses to ozone are increased in obese mice. J. Appl. Physiol. 2003, 95, 938–945. [Google Scholar] [CrossRef] [PubMed]
- O’Lenick, C.; Winquist, A.; Mulholland, J.; Friberg, M.D.; Chang, H.H.; Kramer, M.; Darrow, L.; Sarnat, S.E. Assessment of neighbourhood-level socioeconomic status as a modifier of air pollution–asthma associations among children in Atlanta. J. Epidemiol. Community Health 2016, 71, 129–136. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency (n = 258) | |||
|---|---|---|---|---|
| n | (%) | |||
| Sex | Male | 181 | (70.2) | |
| Female | 77 | (29.8) | ||
| Age (years) | Infant (≤1) | 132 | (51.2) | |
| Underweight | 16 | (12.1) | ||
| Normal weight | 109 | (82.6) | ||
| Overweight | 7 | (5.3) | ||
| Toddler (2–5) | 114 | (44.2) | ||
| Underweight | 17 | (14.9) | ||
| Normal weight | 94 | (82.5) | ||
| Overweight | 3 | (2.6) | ||
| Child (6–10) | 12 | (4.7) | ||
| Underweight | 4 | (33.3) | ||
| Normal weight | 8 | (66.7) | ||
| Overweight | 0 | (0.0) | ||
| Nutritional status a | Underweight | 37 | (14.3) | |
| Normal weight | 211 | (81.8) | ||
| Overweight | 10 | (3.9) | ||
| Min. | 25th Percentile | Median | 75th Percentile | Max. | Mean | SD | |
|---|---|---|---|---|---|---|---|
| ARI admissions | 0.0 | 0.0 | 0.0 | 1.0 | 5.0 | 0.7 | 0.9 |
| PM2.5 (μg/m3) | 2.0 | 11.6 | 41.0 | 63.6 | 213.7 | 43.5 | 35.9 |
| Temperature (°C) | 9.4 | 15.1 | 22.4 | 27.1 | 29.8 | 21.2 | 6.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, H.; Ng, C.F.S.; Madaniyazi, L.; Seposo, X.T.; Dhoubhadel, B.G.; Pokhrel, D.; Pokhrel, A.K.; Verma, S.C.; Shrestha, D.; Raya, G.B.; et al. Ambient PM2.5 and Daily Hospital Admissions for Acute Respiratory Infections: Effect Modification by Weight Status of Child. Atmosphere 2021, 12, 1009. https://doi.org/10.3390/atmos12081009
Nishikawa H, Ng CFS, Madaniyazi L, Seposo XT, Dhoubhadel BG, Pokhrel D, Pokhrel AK, Verma SC, Shrestha D, Raya GB, et al. Ambient PM2.5 and Daily Hospital Admissions for Acute Respiratory Infections: Effect Modification by Weight Status of Child. Atmosphere. 2021; 12(8):1009. https://doi.org/10.3390/atmos12081009
Chicago/Turabian StyleNishikawa, Hironori, Chris Fook Sheng Ng, Lina Madaniyazi, Xerxes Tesoro Seposo, Bhim Gopal Dhoubhadel, Dhiraj Pokhrel, Amod K. Pokhrel, Sharat Chandra Verma, Dhruba Shrestha, Ganendra Bhakta Raya, and et al. 2021. "Ambient PM2.5 and Daily Hospital Admissions for Acute Respiratory Infections: Effect Modification by Weight Status of Child" Atmosphere 12, no. 8: 1009. https://doi.org/10.3390/atmos12081009